
Abstract
Background/Purpose
We aimed to investigate whether there is an interaction between life-space assessment (LSA) and movement control during one-leg standing on bone strength on the non-fractured side in patients with hip fracture.
Methods
Two-way analysis of variance (ANOVA) was applied for osteoporosis parameter to examine the interaction and main effects of LSA and movement control during one-leg standing.
Results
Two-way ANOVA revealed significant interaction and main effects of LSA and movement control during one-leg standing on bone mineral density (BMD) and Z-score. In parameters of hip structural analysis (HSA), the interaction and main effect of movement control during one-leg standing were detected only in cross-sectional area (CSA).
Conclusion
The results of this study suggest that both high LSA and good movement control during one-leg standing are necessary to maintain or improve some parameters of bone strength, such as BMD (neck and total hip), Z-score (neck and total hip), and CSA.
Keywords
Introduction
Elderly patients have a high risk of hip refracture.1,2 The cumulative incidence of second hip fracture reported by systematic review ranges from 2% to 20%, with an estimated average of 8.4%. 3 Hip refracture is associated with a worsened treatment outcome; compared with the first fractures, the number of complications and mortality are higher in the second hip fractures. 4 Hence, refracture prevention is a crucial issue in patients with hip fractures.
Osteoporosis is defined as a loss of bone strength and is one of the main causes of hip refracture. 5 Bone strength is determined by bone mineral density (BMD) and bone quality. BMD measurement and hip structural analysis (HSA) are the primary evaluation methods of bone strength.5,6 It is well known that old age and female sex are associated with lower femoral bone strength.7–10 However, these factors cannot be modified by interventions. Physical function and activity, which can be modified by interventions, are also associated with bone strength; short one-leg standing time, 11 decreased handgrip and knee extension strength, 12 and low activity 13 are associated with decreased bone strength. In a previous study, 14 we investigated factors associated with femoral BMD in patients who underwent surgery for a first hip fracture. Consequently, the Life-Space Assessment (LSA), which reflects the scope of activities, and movement control during one-leg standing were extracted; higher LSA and better movement control during one-leg standing were associated with higher BMD values. Bone formation occurs under loading conditions, whereas bone resorption occurs under unloading conditions, a phenomenon known as Wolff's Law. 15 Accordingly, in healthy individuals, mechanical loads on bones during daily activities promote bone formation and thus contribute to BMD. 16 The force applied to the proximal femur during one-leg standing varies greatly depending on the posture during unipedal stance 17 ; thus, it is reasonable to presume that movement control during one-leg standing is related to bone strength.
The total amount of the load on bone is determined by the product of its time and intensity. We speculate that there is an interaction between LSA (reflecting the time of the load) and movement control during one-leg standing (reflecting the intensity of the load) for bone strength. However, this possibility has not yet been examined. Clarifying the presence or absence of an interaction between LSA and movement control during one-leg standing will be useful information for developing treatment strategies.
In this study, we aimed to investigate whether there is an interaction between LSA and movement control during one-leg standing on bone strength on the non-fractured side in patients with hip fracture. We hypothesized that patients with higher activity levels and better movement control during one-leg standing would have higher bone strength. Validating this hypothesis will help to establish effective interventions for maintaining and increasing bone strength to prevent a second hip fracture.
Materials and methods
Study design
The present study was a cross-sectional study. This study did not require informed consent because it used past data. Designs of this study were approved by the ethics committees of Kure Kyosai Hospital (Hiroshima, Japan) [reference no. 2021-11] and Hiroshima International University (Hiroshima, Japan) [reference no. 21-003]. This study was performed following the STROBE (strengthening the reporting of observational studies in epidemiology) statement. The study was conducted according to the Helsinki Declaration.
Setting
This study was conducted in a hospital setting. Recruitment, follow-up, and data collection were performed between March 2019 and November 2020. Therapists in the rehabilitation departments recruited potential participants.
Patients
This study included patients who satisfied the following inclusion criteria: (1) age of 65 years or older, (2) first hip fractures treated by surgery, (3) able to walk independently before the hip fractures, and (4) patients without lower limb deformation. The exclusion criteria for this study were (1) complications during hospitalization or (2) severe dementia, which was defined as a revised Hasegawa's dementia scale (HDS-R) score of ≤9. 18 Complications during hospitalization were defined as cases that required treatment, such as pneumonia, deep venous thrombosis, delirium, stroke, and infection after surgery. Parts of the data used in this study were also included in our previous study. 14
Basic and medical variables
Age, sex, body mass index (BMI), walking ability before hip fracture, residence (home or institution), cohabitating with family, presence or absence of smoking and drinking alcohol, and cognitive function were evaluated upon hospital admission and were included as basic information. Specific walking ability before hip fracture was classified as one of the following: walking without support, walking with a cane, or walking with a walker. Cognitive function was assessed using the HDS-R, and scores of 21–30, 15–20, 10–14, and ≤9 were considered as normal cognition, dementia doubt, light to moderate dementia, and severe dementia, respectively. 18
The LSA developed by Baker et al. 19 was used to evaluate life space. The timing of the LSA assessment was around 1 week after surgery, and LSA evaluated about life space during 4 weeks before hospitalization. The LSA is a validated questionnaire that measures community mobility on the basis of the frequency of travel to various locations, or “life-space levels,” and the need for assistance to reach those levels. The total score is 120 points, and high score indicates large life space level. The LSA consists of three components: life space, frequency, and with and without aids or independence. The life space is classified into six levels: within the bedroom, within the dwelling, very close to the living space, within 800 meters near the home, within the town between 800 meters and 16 kilometers, and outside the town more than 16 kilometers. Frequency is classified into four levels: 7 days in a week, 4 to 6 days, 1 to 3 days, and less than 1 day. With and without aids or independence is divided into three levels: activities performed independently without aids or assistance, activities performed with aids, and activities performed with aids or assistance. A previous study reported that LSA was significantly associated with the amount of daily activity measured by three-axis accelerometers in stroke survivors. 20 Thus, LSA is a clinically useful tool for assessing the amount of daily activity.
Fracture type, fracture side, operative type, previous medical history (chronic obstructive pulmonary disease, cardiovascular disease, cerebrovascular disease, cancer, hypertension, diabetes, chronic kidney disease, and rheumatism), geriatric nutritional risk index, and estimated glomerular filtration rate were assessed upon hospital admission and were included as medical information. The presence or absence of pharmacotherapy for osteoporosis (parathyroid hormone, anti-receptor activator of NF-κB ligand antibody, bisphosphonate, and selective estrogen receptor modulator, vitamin D) before hip fracture and the presence or absence of steroid in the past were recorded. Three metabolism markers (total P1NP, 25-hydroxyvitamin D, and TRACP-5b) were included as medical information on osteoporosis.
Physical function variables
Handgrip and isometric knee extension muscle strengths, pain, one-leg standing time, and movement control during one-leg standing were assessed 2 weeks after surgery as physical functions.
Handgrip strength (kg) was measured using a digital handgrip strength dynamometer (12B3X00030; Tsutsumi Works, Chiba, Japan). Patients were asked to squeeze the dynamometer with maximum effort over two trials for each hand. Thereafter, the maximum value (rounded to the nearest 0.1 kg) for either the left or right hand was used. 21
Isometric knee extension muscle strength was measured using a hand-held dynamometer (HHD) (Anima Corp., Tokyo, Japan) according to the methods described in a previous study. 22 Corrected muscle strength was determined using the following equation: muscle strength measured by HHD × lower leg length (nearly the moment arm) / body weight. Lower leg length was measured as the distance between the lateral femoral epicondyle and the lateral malleolus; the limb on the non-fractured side was measured.
Pain intensity of the hip joint on the operated side was assessed using the numerical rating scale (NRS), which is divided into 11 stages from 0 to 10, with 0 indicating no pain at all and 10 indicating the worst possible pain. The NRS was assessed at rest and during activity.
One-leg standing time was measured to evaluate standing balance. 23 The measured limb was on the non-fractured side.
Movement control during one-leg standing was assessed according to the criteria described by Lenzlinger-Asprion et al.. 24 Criteria 1 states that the hip joint should remain stable in the extension and intermediate position during rotation and abduction–adduction movements. The pelvis and upper body should not move from their initial position. Criteria 2 states that the vertical axis of the leg should remain straight, and varus or valgus should not occur. The patella should be directed to the third metatarsal. Criteria 3 states that a component was considered incorrect when intermittent support by the hand against the wall or the contralateral foot on the floor was necessary. If additional support was needed throughout the entire exercise, the component was considered to have >1 incorrect component. A three-point Likert scale was used for evaluation, where 2 points indicated that all criteria were correct, 1 point indicated that 1 criterion was incorrect, and 0 points indicated that >1 criterion was incorrect or false. The measured limb was on the non-fractured side. If movement control during one-leg standing is normal, the maximum principal stress values on the medial side of the femoral neck are 2.97 times of body weight. 17 However, if movement control during one-leg standing is abnormal, the maximum principal stress values on the medial side of the femoral neck are only 1.17 times of body weight. 17 Thus, movement control during one-leg standing is important to determine the intensity of the load on the proximal femur. In addition, the maximum principal stress values on the medial side of the femoral neck during one-leg standing are consistent with the average compressive stress during walking. 25 Therefore, movement control during one-leg standing will reflect the intensity of the load on the proximal femur during daily activity.
Osteoporosis parameter variables
Measurements of BMD and HSA using dual-energy X-ray absorptiometry (DXA) (PRODIGY Fuga: GE Healthcare Japan Int., Tokyo, Japan) are considered the best approach for diagnosing femoral osteoporosis. 5 The BMD and Z-score were measured in the femoral neck and total hip at 1 week after surgery. The Z-score is based on the standard deviation value of the BMD of a population of identical sex, race, and age of patients. If the patient is a 65-year-old Japanese woman, the Z-score is the relative value of the BMD to the mean of 65-year-old Japanese women. The high reliability of the DXA method has been previously reported. 26 On the basis of DXA data, the HSA of the proximal femur was assessed. Parameters calculated in the narrow neck region were used in the analysis. The cross-sectional area (CSA), cross-sectional moment of inertia (CSMI), section modulus (SM), and buckling ratio (BR) were calculated as strength parameters.27,28 CSA is the combined area of cortical and cancellous bone, excluding the marrow cavity. CSMI is a numerical value that represents the magnitude of structural stiffness, and higher values indicate greater stiffness. In other words, CSMI is an indicator of the resistance of an object to deformation. SM is a coefficient used to calculate the maximum stress for bending and torsional moments of a bone cross-sectional profile. In other words, SM is an index of bending strength, and higher values indicate stronger bending strength. BR is the relative cortical bone thickness. BR is an indicator of the phenomenon of bending and fracture under compressive force, and higher values indicate higher resistance to crush. Generally, patients with osteoporosis have low BMD, Z-score, CSA, CSMI, and SM values and high BR values.
Bias
To reduce selection bias, the outcomes of physical functions were selected on the basis of previous studies.21–24 To reduce the measurement bias, the first author (TU) was not involved in participant enrollment and data collection. Patients received explanations about the purpose of the study but were unaware of our hypothesis.
Statistical analysis
Patients were categorized based on LSA and movement control during one-leg standing. Patients with LSA scores lower or higher than the median were assigned to LSA low and high groups, respectively. Additionally, patients were classified into three groups on the basis of the point of movement control during one-leg standing (0, 1, and 2 points). Two-way analysis of variance (ANOVA) was applied for continuous variables to examine the interaction and main effects of LSA and movement control during one-leg standing. If significant main effects or interactions were detected, Bonferroni tests were performed post hoc to localize the effects. The χ2 test was applied for categorical variables. After performing sample size analysis using G × power 3.1.9, setting the alpha value at 0.05, power at 0.8, and effect size f2 to 0.4, a sample size of 86 cases were determined. Using SPSS version 27.0 for Windows (IBM Corp., Armonk, NY), statistical analyses were performed, with the significance level being set at P < 0.05.
Results
Patient characteristics
Among the 133 screened patients, seven who developed complications during hospitalization and 22 who had advanced dementia were excluded. Consequently, 104 patients (14 males and 90 females) with a mean age of 82.3 ± 7.5 years were included herein. Table 1 summarizes the main characteristics of the included patients. Both LSA low (>38 points) and high (≦38 points) groups included 52 patients. In the LSA low group, 26 (age: 82.5 ± 8.3 years; sex: 4 males and 22 females), 23 (age: 84.7 ± 6.5 years; sex: 1 male and 22 females), and 3 (age: 74.0 ± 4.0 years; sex: 1 male and 2 females) patients had 0, 1, and 2 points movement control during one-leg standing, respectively. In the LSA high group, 20 (age: 82.6 ± 8.2 years; sex: 3 males and 17 females), 24 (age: 81.9 ± 6.0 years; sex: 4 males and 20 females), and 8 (age: 75.8 ± 3.2 years; sex: 2 males and 6 females) patients had 0, 1, and 2 points movement control during one-leg standing, respectively.
Patient characteristics.
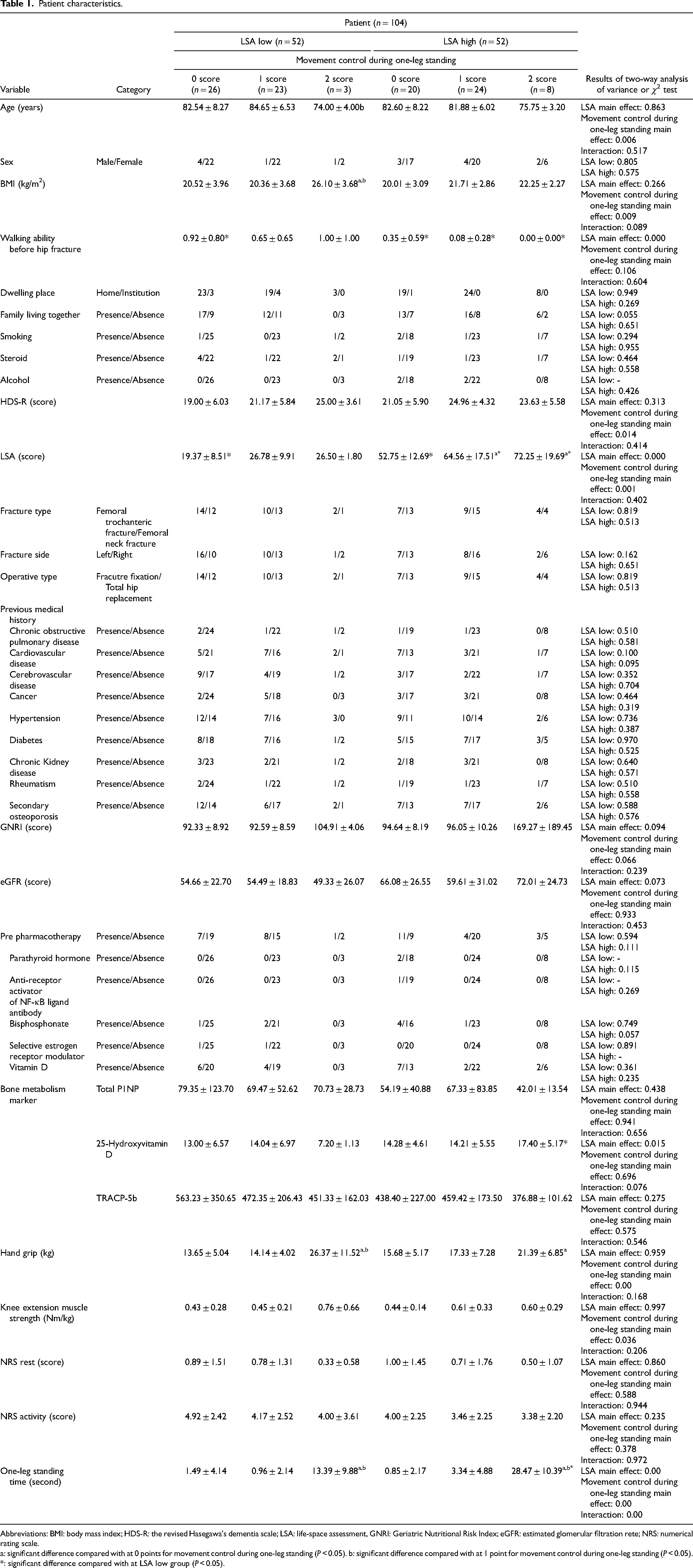
Abbreviations: BMI: body mass index; HDS-R: the revised Hasegawa's dementia scale; LSA: life-space assessment, GNRI: Geriatric Nutritional Risk Index; eGFR: estimated glomerular filtration rete; NRS: numerical rating scale.
a: significant difference compared with at 0 points for movement control during one-leg standing (P < 0.05). b: significant difference compared with at 1 point for movement control during one-leg standing (P < 0.05). *: significant difference compared with at LSA low group (P < 0.05).
Osteoporosis parameters
Table 2 summarizes the osteoporosis parameter results. Two-way ANOVA revealed significant interaction and main effects of LSA and movement control during one-leg standing on BMD (neck and total hip) and Z-score (neck and total hip). In parameters of HSA, the interaction and main effect of movement control during one-leg standing were detected only in CSA. There were no significant interactions and main effects of LSA and movement control during one-leg standing in other parameters of HSA (CSMI, SM, and BR). In the LSA high group, post hoc analyses revealed that BMD (neck and total hip), Z-score (neck and total hip), and CSA were significantly higher at 1 and 2 points for movement control during one-leg standing than at 0 points. For the others, there were no significant differences.
Osteoporosis parameter.
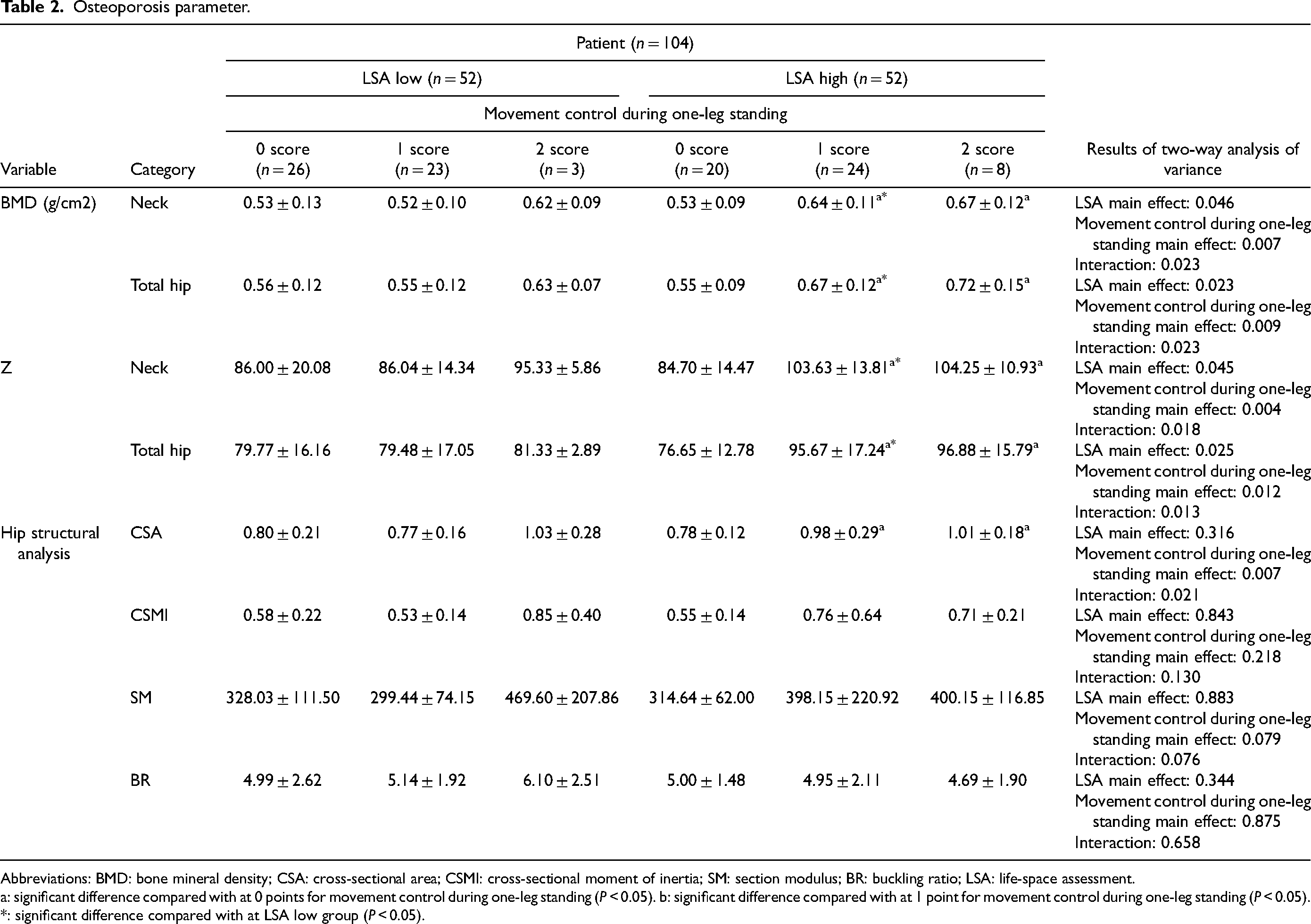
Abbreviations: BMD: bone mineral density; CSA: cross-sectional area; CSMI: cross-sectional moment of inertia; SM: section modulus; BR: buckling ratio; LSA: life-space assessment.
a: significant difference compared with at 0 points for movement control during one-leg standing (P < 0.05). b: significant difference compared with at 1 point for movement control during one-leg standing (P < 0.05). *: significant difference compared with at LSA low group (P < 0.05).
Discussion
We previously reported that LSA and movement control during one-leg standing were associated with BMD. 14 In the present study, two-way ANOVA revealed significant main effects of LSA and movement control during one-leg standing on BMD (neck and total hip) and Z-score (neck and total hip), and these results support the findings of our previous studies. The novelty of this study is that there was an interaction between LSA and movement control during one-leg standing on BMD (neck and total hip); patients with higher LSA and better movement control during one-leg standing had higher BMD (neck and total hip). To improve BMD in patients with femoral neck fractures, therefore, it would be more effective to improve both the intensity and time of loading on the bone rather than either of them alone.
BMD (neck and total hip) and Z-score (neck and total hip) in the LSA high group were significantly lower at 0 points for movement control during one-leg standing than at 1 and 2 points. In our previous study, 14 we calculated cutoff values for movement control during one-leg standing to divide the femoral neck and total hip BMD into above and below reference values. Consequently, the cutoff value of the movement control during one-leg standing was 1 point. Taken together, our previous study and the present study suggest that both high LSA and more than 1 point of movement control during one-leg standing were necessary to maintain or improve BMD. The 1 point for movement control during one-leg standing was reduced for any one of the following: hip and knee position and upper limb support. In patients with 1 point of movement control during one-leg standing, the deduction item was the upper extremity support in all cases (data not shown). To maintain or improve BMD (neck and total hip) and Z-score (neck and total hip), therefore, good hip and knee positioning during one-leg standing and walking may be important even if support by upper extremities is required.
In the parameters of HSA, significant interaction and main effect of movement control during one-leg standing were detected in CSA only. CSA in the LSA high group was significantly higher at 1 and 2 points for movement control during one-leg standing than at 0 points. This result may be explained by the amount of loading on the bone. Although the main effect of LSA was detected in BMD, it was not detected in CSA. This difference was explained by the difference in the calculation method. BMD was calculated by dividing the bone mineral mass by bone area, including marrow cavities, whereas CSA comprises a bone area without marrow cavities in the cross-section of the neck. In identical CSAs, a smaller bone area, including marrow cavities, induced higher BMD. However, the bone area, including marrow cavities, was not measured in this study, and further studies are required to elucidate the effects of bone size. Conversely, significant interaction and main effects of LSA and movement control during one-leg standing were not detected in other parameters of HSA (i.e. CSMI, SM, and BR). The CSMI and SM values in the LSA low group tended to be inversely proportional to age (e.g. 0–2 points: CSMI = 0.6 ± 0.2, 0.5 ± 0.1, 0.9 ± 0.4; age = 82.5 ± 8.3, 84.7 ± 6.5, and 74.0 ± 4.0 years). Thus, it is suggested that CSMI and SM in the LSA low group are more influenced by factors other than physical functions, such as age. The CSMI and SM values in the LSA high group tended to increase as the points of movement control during one-leg standing increased, although there were no significant differences. We cannot thus reject the possibility that movement control during one-leg standing partially influenced the CSMI and SM values in the LSA high group. BR is the relative cortical bone thickness and is calculated by dividing the radius of the bone by the cortical thickness. Theoretically, if the cortical thickness is the same, a larger bone radius would induce a larger BR. In both LSA low and high groups, BMI significantly increased or tended to increase when the point of movement control during one-leg standing increased. This result implies that patients who had a higher point of movement control during one-leg standing had a larger bone radius. This may explain why the main effect of movement control during one-leg standing was detected in CSA but not in BR.
There were significant interactions between LSA and movement control during one-leg standing in BMD, Z-score, and CSA. In the LSA high group, BMD (neck and total hip), Z-score (neck and total hip), and CSA at 1 and 2 points for movement control during one-leg standing were significantly higher than those at 0 points. These results suggest that both high LSA and good movement control during one-leg standing (≧1 point) are necessary to maintain or improve bone strength parameters including BMD, Z-score, and CSA. The maximum principal stress values on the medial side of the femoral neck during one-leg standing is higher in the normal standing position than in the abnormal standing position. 17 The maximum principal stress values on the medial side of the femoral neck during one-leg standing is consistent with the average compressive stress during walking. 25 Thus, movement control during one-leg standing will reflect the intensity of the load on the proximal femur during daily activity. LSA is positively correlated with the amount of daily activity measured by three-axis accelerometers in stroke survivors. 20 LSA will thus reflect the time of the load on the femur during daily activity. Because the total amount of the load on bone is determined by the product of its intensity and time, patients with high LSA and good movement control during one-leg standing will receive a high level of the load, which induces high bone strength parameters.
Our results suggest that good movement control during one-leg standing and high amount of activity are required to induce high bone strength and resulting to prevent secondary fracture. Specifically, in the LSA high group, bone strength was significantly higher at 1 and 2 points for movement control during one-leg standing than at 0 points. Low LSA indicates low activity level. Poor movement control during one-leg standing on the non-fractured side and low activity level should be targeted by therapeutic interventions to prevent secondary fractures.
This study has three limitations. First, this was a cross-sectional study. Hence, the causal relationship between the interaction of LSA and movement control during one-leg standing and bone strength is unclear. Longitudinal studies will be required in the future. Second, the causes of poor movement control during one-leg standing were unknown. Generally, it is considered that sufficient strength of hip abductors is required to control the posture during one-leg standing. 29 However, we did not assess the strength of hip abductors. If future studies can elucidate the cause of poor movement control during one-leg standing, therapeutic targets can be better defined. Third, we used LSA as a measure of activity. LSA represents the space of life. If patients actively moved in the home but did not go out, the LSA would be low. In the future, it will be necessary to investigate the amount of activity in more detail using three-axis accelerometers or other devices.
In conclusion, the results of this study suggest that both high LSA and good movement control during one-leg standing (≧1 point) are necessary to maintain or improve some parameters of bone strength, such as BMD (neck and total hip), Z-score (neck and total hip), and CSA.
Footnotes
Acknowledgments
The authors thank Nitta K, Matsumoto K, Masudome K, Matsuda N, Nakashima Y, Kinoshita Y, Tao Y, Higaki N, Yoneda S, Fujihara S (Kure Kyosai Hospital, Kure, Japan) for their support in data collection.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.