
Abstract
Introduction
Nonunion is the inability of a fractured bone to heal. The most agreed-upon standard definition of nonunion made by the FDA is a fracture that persists for a minimum of 9 months without signs of healing for 3 months. 1 Nonunion is classified into four main categories—hypertrophic, atrophic, oligotrophic, and septic. Hypertrophic nonunion is demonstrated by the presence of adequate callus formation, however, there is a lack of bridging bone and the fracture ends are not united. This usually suggests adequate blood supply, evidenced by significant callus formation, however, there is a lack of stability. Atrophic nonunion is evidenced by radiographically absent callus formation, usually indicating poor blood supply. Oligotrophic nonunion is a balance between atrophic and hypertrophic nonunion, as these fractures demonstrate incomplete callus formation. Septic nonunion results in decreased bone formation due to the consumption of nutrition by organisms and consequently a decrease in nutrition supply towards healthy bone formation. 1
Thomas and Kehoe 1 suggest that blood supply could be one of the main factors predisposing to nonunion. Blood supply to the bone can be affected by many factors including the nature of the fracture, treatment options, energy of the injury (high vs. low), lifestyle habits, and metabolic abnormalities. Past medical history including cardiovascular disease, peripheral vascular disease, and lifestyle habits such as smoking can restrict osseous blood supply. In one systematic review, smokers were found to have an adjusted odds ratio of 2.32 (CI: −1.76 – 3.06, p < 0.001) of developing nonunion compared with the nonsmoking group, and overall risk of long-bone fracture nonunion was 12% higher in smokers. 2 Metabolic predispositions of diabetes, renal insufficiency, or vitamin D deficiency can also contribute to nonunion. 1 Vitamin D has been perhaps the most studied of the metabolic derangements affecting bone healing. The primary effect of vitamin D is enhanced calcium absorption in the small intestine. 3 A secondary effect of vitamin D is stimulating osteoblast plasma membrane expression of RANKL, which in turn activates a cascade culminating in the conversion of preosteoclasts to osteoclasts. 4 This conversion aids in metabolizing calcium stores from the bones into circulation to maintain physiologic levels. Over extended periods of time, vitamin D insufficiency has been associated with bone loss leading to increased fracture risk.4,5
It is clear that nonunion may occur due to various reasons including surgical technique (inadequate reduction, fixation, and stabilization), infection in the bone and surrounding tissues, or underlying metabolic or endocrinological abnormalities. Nonunion is a complex issue that requires multifactorial investigation to recommend the most appropriate therapeutic intervention. Generally, the first step in evaluating nonunion is ruling out hardware failure using radiographic evaluation. Once hardware failure is excluded, attention is turned to other common causes of nonunion such as infection, malnutrition, and lifestyle habits. Brinker et al. 6 suggested that patients who are experiencing nonunion despite adequate anatomical reduction and without other obvious etiologies should be evaluated for underlying metabolic abnormalities. This recommendation was supported by their findings which showed that 31/37 (83.8%) unexplained nonunion patients had at least one previously undiagnosed underlying metabolic abnormality. The most commonly identified disturbance was vitamin D deficiency. Other abnormalities included calcium imbalances, thyroid disorders, parathyroid disorders, and hypogonadism. More importantly, correcting these abnormalities resulted in bony union for 96% of the studied patients in an average of 9.6 months. Eight patients achieved bony union with medical treatment of their metabolic or endocrine disorders alone. Other sources have highlighted the importance of evaluating vitamin D in otherwise unexplained nonunion. Pourfeizi et al., 7 controlling for fracture location and severity, found statistically significant differences in vitamin D levels among patients with closed middle third tibial shaft fractures who achieved union versus nonunion.
Apart from vitamin D, there are other metabolic parameters that may have an impact on fracture union. The main objective of this study is to identify metabolic causes that would impact fracture union including calcium, vitamin D, thyroid hormone, thyroid stimulating hormone (TSH), testosterone, albumin, parathyroid hormone (PTH), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP). Our study aims to comprehensively evaluate fracture type, category of nonunion, and metabolic profile among a single institution's patients to determine whether there is a relationship between these variables that can highlight future interventions to reduce nonunion.
Methodology
A retrospective chart review of patients diagnosed with nonunion after fracture fixation was performed from 1 January 2012 to 31 July 2021. Nonunion diagnosis in our study was assessed and determined by a fellowship-trained orthopedic trauma surgeon. We excluded patient data with inadequate follow-up or metabolic data. The study was approved by the local Committee for Research Involving Human Subjects.
Patient demographics including age, sex, height, weight, body mass index (BMI), smoking status, past medical history, and American Society of Anesthesiologists grade were recorded. Information regarding the fractured bone was recorded including the location (proximal, shaft, and distal). Details of the initial injury including whether the fracture was intra-articular versus extra-articular, open injury versus closed injury were recorded to further characterize the specific trauma. The type of nonunion was classified as hypertrophic, atrophic, or septic. Furthermore, the extent of operative intervention to treat each patient's nonunion was recorded by documenting any interim surgeries (e.g. irrigation and debridement, hardware removal, and revision open reduction internal fixation) performed either before or after diagnosis of nonunion. Metabolic profile was assessed within the period of 3 months pre- or post-nonunion diagnosis, using the closest serum laboratory values to the date of diagnosis of nonunion for each test. The serum values recorded included 25-hydroxy vitamin D, CRP, ESR, serum glucose, hemoglobin A1c (HbA1c), creatinine, albumin, TSH, T4, T3, PTH, pre-albumin, testosterone (free and total), white blood cell count (WBC), hemoglobin (Hgb), differential neutrophil percentage, and differential lymphocyte percentage.
Patients were followed from the date of initial surgery through the diagnosis of nonunion and the date of last follow-up with the surgeon. Our primary outcome was a radiographic interpretation of the union by the Orthopedic Surgeon. Our secondary outcomes included metabolic abnormalities, medical comorbidities, and a description of frequency and interim procedures following nonunion diagnosis. Eight out of 94 patients had procedures done prior to diagnosis of nonunion, specifically six patients had hardware removal due to pain and two patients had irrigation and debridement for superficial wound infections, all of which were performed by outside providers before nonunion diagnosis. All the remaining patients’ interim procedures were performed after a diagnosis of nonunion.
Results
Data were collected from 94 patients diagnosed with nonunion, the mean age of the cohort was 54.7 years and approximately 50% were men. The most common comorbidities were hypertension (50.4%), pulmonary disease (30.1%), diabetes (24.7%), and cardiac disease (23.7%). Around 47.3% of the patients with nonunion were obese (BMI > 30 kg/m2), and 60.8% were either current or former smokers (Table 1).
Baseline demographic and clinical outcomes in patients with fracture nonunion.
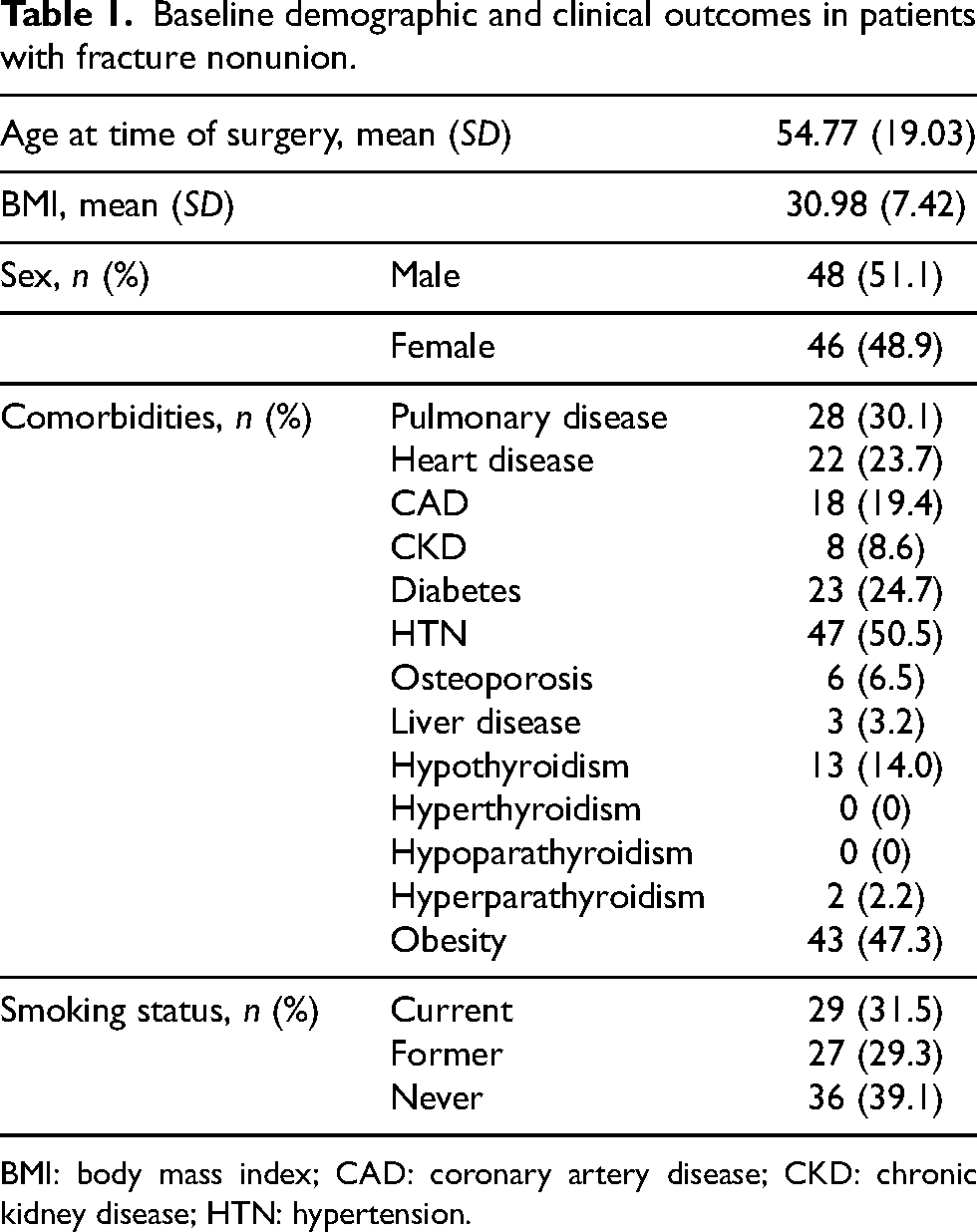
BMI: body mass index; CAD: coronary artery disease; CKD: chronic kidney disease; HTN: hypertension.
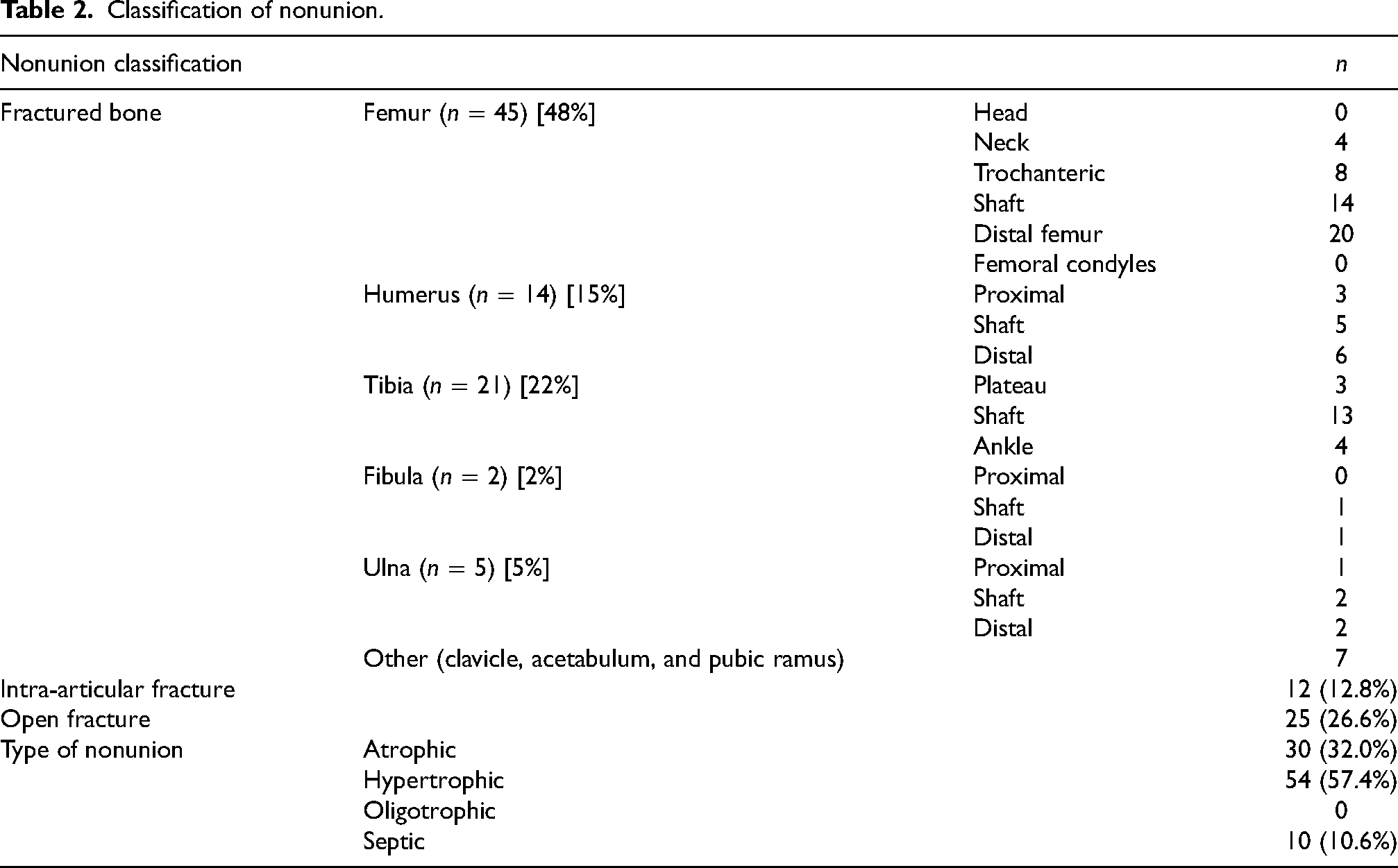
The most common nonunited bone was the femur (48% of the total cohort), followed by the tibia (22%), humerus (15%), ulna (5%), clavicle (3%), and fibula (2%) (Table 2). There were no cases of nonunion in radius fractures over the studied time period. More specifically by fracture location, distal femur nonunion was most prevalent making up 21% of the total cohort and 44% of all femoral nonunion. The femoral shaft was the second most common, comprising 15% of the cohort and 31% of femoral nonunion. The tibial shaft was the third most prevalent making up 14% of the cohort and 62% of tibial nonunion. These three fractures together accounted for 50% of the nonunion in this cohort. Thirteen percentof the fractures that went on to nonunion were intra-articular fractures, and about 27% were open injuries. The most common type of nonunion observed was hypertrophic (57%), followed by atrophic (32%), and septic (10%) (Table 2).
Classification of nonunion.
The metabolic laboratory values that were most frequently outside of normal limits were vitamin D (hypovitaminosis—44.3%), low testosterone (47%), and low hemoglobin (62%) (Table 3). Almost two-thirds (62%) of patients had an elevated neutrophil differential percentage. Among females, ESR was elevated in 52% of patients with a mean of 34.26 mm/h. Conversely among males, ESR was only elevated in 12.5% of patients. Metabolic profile data were further stratified by specific fracture location, selecting the three most commonly nonunited fractures, specifically the distal femur, femoral shaft, and tibial shaft. Patients with distal femur nonunion had mean vitamin D levels of 31.71 ng/mL, mean testosterone (female) of 27.58 ng/dL, mean testosterone (male) of 360.54 ng/dL, and mean neutrophil differential percentage of 61.05%. Patients with femoral shaft nonunion had mean vitamin D of 38.72 ng/mL, mean testosterone (female) of 13.5 ng/dL, mean testosterone (male) of 357.66 ng/dL, and mean neutrophil percentage of 61.72%. Patients with tibial shaft nonunion had mean vitamin D of 28.06 ng/mL, mean testosterone (female) of 247 ng/dL, mean testosterone (male) of 429.5 ng/dL, and mean neutrophil percentage of 55.97%.
Metabolic profile of patients diagnosed with nonunion within 3 months pre- or post-diagnosis.
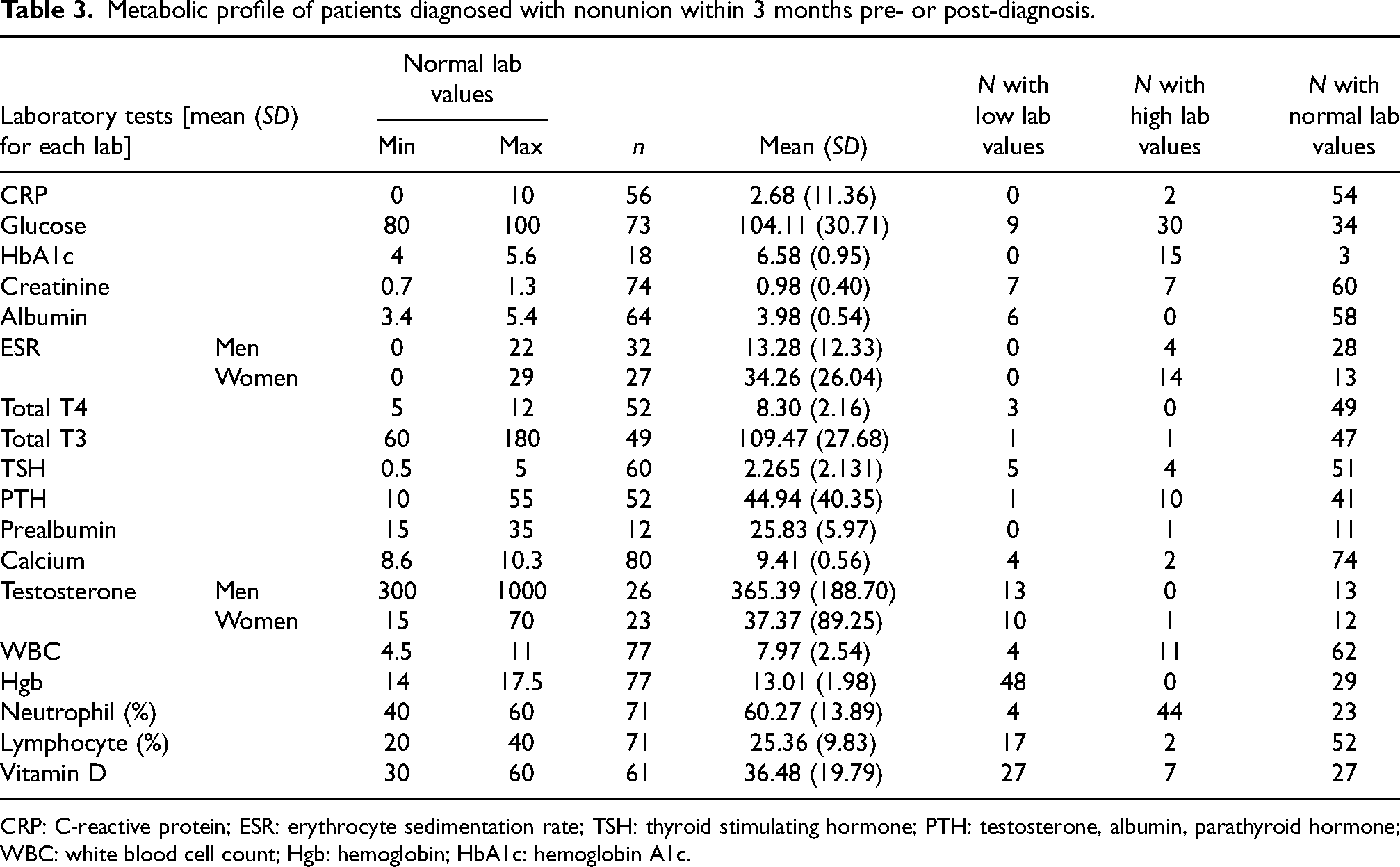
CRP: C-reactive protein; ESR: erythrocyte sedimentation rate; TSH: thyroid stimulating hormone; PTH: testosterone, albumin, parathyroid hormone; WBC: white blood cell count; Hgb: hemoglobin; HbA1c: hemoglobin A1c.
The distal femur and tibial shaft had lower mean vitamin D levels than the total nonunion patient cohort (36.48 ng/mL). The distal femur and femoral shaft had lower mean testosterone levels in both men and women than the total cohort (men—365.4 ng/dL and women—37.4 ng/dL). The distal femur and femoral shaft had a higher mean neutrophil differential percentage than the total patient cohort (60.3%). In summary, distal femur nonunion had lower vitamin D and testosterone, and higher neutrophil differential percentage than the overall nonunion cohort. Femoral shaft nonunion had lower testosterone and higher neutrophil differential percentage than the total patient cohort. The tibial shaft nonunion had lower vitamin D levels than the total nonunion cohort (Table 3).
Metabolic profile was stratified by “Atrophic” nonunion, and no differences in metabolic profile were observed compared to the total cohort. Similarly, metabolic data were stratified by patients who required at least one interim procedure before definitive fixation as compared to those who did not require any interim procedures. Mean vitamin D among patients who required 1 + interim procedures, n = 31, were slightly lower (35.7 ng/mL) than mean vitamin D among patients who required no interim procedures, n = 63, (37 ng/mL). However again, no major differences in laboratory values or frequency of abnormal results were observed.
Discussion
The most commonly nonunited bones were the femur (48%), followed by the tibia (22%), and humerus (15%). The distal femur, femoral shaft, and tibial shaft made up 50% of the nonunion cohort. The intra-articular fracture was diagnosed in 13% of nonunions and open injuries in 27%. The most common metabolic abnormalities were low hemoglobin (62.3%), elevated neutrophil percentage (61.9%), elevated ESR in women (51.8%), low testosterone (46.9%), and hypovitaminosis D (44.3%).
While the incidence of fracture nonunion is debated,8,9 Mills et al. 9 published a prospective national database study that documents an incidence of nonunion per fracture of 1.9%. Notably, the overall rate was greater in men (2.3%) than in women (1.5%). They also showed nonunion rate per fracture was highest in the 30–44 years age group, 20 times greater than that in the 0–14 years old and 2.5 times higher than in those aged ≥ 75. 9 The patients from this cohort of nonunion fractures were older with a mean age of 54.7 years and there was an approximately even split between the two sexes (51% male). The average BMI of the patient cohort was 30.98, within the “obese” range. This coincides with existing literature supporting obesity to be associated with nonunion for the humerus, femur, and tibia. 10
In the patients presented in this article, the femur was the most commonly nonunited bone, accounting for 48% of the total cohort. Furthermore, three specific fracture locations of the distal femur, femoral shaft, and tibial shaft made up 50% of the nonunion cohort. This data is comparable to previously published information on nonunion incidence by anatomic location. 9 The highest risk of nonunion was in the lower leg (tibia/fibula)—9.1% in the 30–44 years age group, followed by the shoulder (scapula/clavicle)—8.0% in 30–44 years old, and then femur/pelvis—5.5% in this age group. Although femoral nonunion was more prevalent than lower leg (tibia and fibula) in this cohort, consistent with Mills et al., 9 nonunion in the femur and tibia are still more prevalent as compared to other long bones.
The most common metabolic abnormalities were low hemoglobin, elevated neutrophil percentage, elevated ESR in women, low testosterone, and hypovitaminosis D. Vitamin D insufficiency and deficiency have been well documented in existing nonunion literature. 11 Average 25-hydroxyvitamin D across 652 trauma patients was 20.5 ng/mL with 86.2% of patients having some form of insufficiency (< 30 ng/mL). 11 Vitamin D was the only metabolic lab value that had an average value below the reference range across the 652 trauma patients. This manuscript reinforces the high prevalence of hypovitaminosis D among nonunion patients, but also showed a relatively high prevalence of low testosterone—a metabolic abnormality that is less researched in fracture nonunion. The data also showed a lower metabolic profile among the three subgroups of the distal femur, femoral shaft, and tibial shaft relative to the total cohort as mentioned above in the results. There were no major differences in metabolic profile between patients diagnosed with atrophic nonunion as compared to the total cohort. Similarly, Brinker et al. 6 found no difference in the likelihood of metabolic or endocrine abnormality by nonunion type. It is likely that metabolic abnormalities are prevalent in all nonunion patients, and not only selectively among those suffering atrophic nonunion. 12
Further research on metabolic abnormalities in patients with nonunion may help identify effective and preventive interventions to improve the quality of life in these patients and reduce overall costs. A number of studies have researched the effects of vitamin D and/or calcium supplementation on the incidence of fractures. The literature is conflicting, with several trials reporting a reduction in fracture incidence with Vitamin D alone,13–15 others reporting a reduction in fracture incidence only when Vitamin D is combined with calcium,16–18 and others still reporting no significant effect on incidence with either Vitamin D supplementation alone, 19 or in combination with calcium. 20 The discrepancies in outcomes have been suggested to be partly due to disagreement on the optimal dosing of vitamin D and calcium. Many existing controlled trials have used between 300 and 800 IU of vitamin D, which may not be an adequate dose to achieve clinical benefit. 3 Recent meta-analyses showed improved benefits with calcium doses of 1200 mg or more than with doses < 1200 mg (0.80 vs. 0.94; p = 0.006), and with vitamin D doses of 800 IU or more than with doses < 800 IU (0.84 vs. 0.87; p = 0.03). 21 In another meta-analysis that included 45 trials, combination therapy was superior to monotherapy as they found vitamin D alone was unlikely to be effective in preventing fracture, however, vitamin D with calcium was shown to reduce hip fractures (eight trials, 46,658 participants, RR 0.84, 95% CI: 0.73–0.96). 22 Furthermore, there is evidence that the clinical benefit of vitamin D and calcium supplementation is more effective in reducing the risk of fracture in patients who are in institutionalized care compared to individuals living independently in the community.16,22
Most of the available literature evaluates nutrition supplementation to reduce fracture incidence, but few studies have looked at nutrition supplementation for fracture nonunion. Studies investigating vitamin D supplementation for fracture nonunion also show conflicting results. Haines et al. 23 conducted a prospective randomized double-blind placebo-controlled trial on 100 patients with vitamin D insufficiency, administering a single 100,000 IU oral dose of vitamin D3 within 2 weeks of suffering a long bone fracture. Both the treatment and control groups had the same rate of nonunion (4%). The authors concluded that despite the high level of vitamin D insufficiency, the rate of union remained similar in both groups independent of vitamin D supplementation. 23 On the other hand, a case report detailing a patient with nonunion of the femoral shaft for 4 years after the initial injury and adequate fixation documented spontaneous healing and bony union after supplementation with vitamin D and correction of the underlying deficiency. 24 Similarly, Brinker et al. 6 identified 37 patients who met screening criteria of (1) unexplained nonunion despite adequate reduction, stabilization, and debridement in initially infected cases without obvious technical error, (2) history of multiple low-energy fractures with at least one progressing to nonunion, or (3) nonunion of a nondisplaced pubic ramus or sacral ala fracture. Of these, 31/37 (84%) had a new diagnosis of an underlying metabolic or endocrine abnormality, of which hypovitaminosis D was the most common (68%). Furthermore, eight patients achieved bony union without operative intervention after diagnosing and correcting the underlying metabolic or endocrine abnormality alone.
Hypogonadism was also prevalent among patients in this nonunion cohort. Testosterone and androgens mediate their effects on bone by binding to the androgen receptor (AR) to launch transcription and expression of a genomic cascade required for bone formation and mineralization. 25 Testosterone also has nongenomic effects that affect bone regeneration by enhancing osteoblast proliferation and differentiation.25,26 A study evaluating the use of testosterone in healing segmental bone defects in mouse femurs showed testosterone to be as effective as bone morphogenetic protein-2 (BMP-2) at inducing callus formation and promoting the healing of critical-size segmental defects. 26 Furthermore, testosterone is much cheaper than BMP-2, and there are an increasing number of adverse effects associated with BMP-2 prompting research into alternative interventions. 26 While literature exists supporting the role of testosterone in promoting fracture repair, testosterone has not been used clinically to treat fractures, likely due to concern of hormonal disturbances, alteration of lipoprotein levels, and increasing levels of inflammatory and hypercoagulable metabolites such as CRP, homocysteine, and endothelin-1. 27
Fracture nonunion carries high patient morbidity as well as increased cost for the hospital and healthcare system. 28 A retrospective database analysis of 853 tibial shaft fractures showed an increased median total care cost of $25,556 in nonunion patients compared to $11,686 in normal union, p < 0.001. Nonunion tibial shaft fractures had increased costs associated with narcotic usage, as well as indirect costs from lost productivity due to the inability to return to work.28,29 Additionally, tibial shaft nonunion patients are more likely to be prescribed opioids for a longer duration for pain management, 29 which may increase the risk of drug dependence in these patients. A study by Childs et al. 30 aimed to evaluate whether reduced nonunion rates could justify the costs of supplementing every orthopedic trauma patient with calcium and vitamin D. They calculated the cost of nonunion, the cost of providing 1200 mg of calcium, and 1600 IU of vitamin D per day for 8 weeks, and assumed a 5% reduction in nonunion with supplementation. Using these values, they projected a reduction of 4.6 fewer nonunions per year at their institution after supplementation, saving $78,030 in treatment costs per year. The savings outweighed the $12,164 cost of supplementing all 2362 orthopedic trauma patients during the first 8 weeks of fracture healing, resulting in a net savings of $65,866 per year. 30 Therefore, further research characterizing the prevalence of metabolic abnormalities, as well as the efficacy of supplementation, can help identify opportunities for early intervention in order to improve quality of life and reduce healthcare costs.
Strengths and limitations
The strength of this retrospective chart review is that each patient was analyzed with a comprehensive metabolic panel that included lab values that are not routinely tested including vitamin D, testosterone, PTH, CRP, ESR, etc. This study also documents specific fracture locations, for example, distal femur, and tibial shaft, as opposed to simply listing the affected bone. Limitations of this study include the retrospective design, a small sample size, and patients from a single institution and single surgeon. Metabolic and endocrine data was collected as available across three electronic medical records, however, was incomplete for all patients. Another limitation was the metabolic data was not obtained directly at the time of nonunion diagnosis, but rather utilized the closest value to date within an absolute three-month limit.
Conclusion
Our study supports the higher prevalence of nonunion in the femur and tibia as compared to other long bones. More specifically, the distal femur, femoral shaft, and tibial shaft comprised 50% of the nonunion cohort. The prevalence of metabolic abnormalities among nonunion patients is high. The metabolic abnormalities were prevalent across all nonunion types, suggesting this is not unique to atrophic nonunion. The role of hypogonadism in nonunion is unclear, although early animal studies have shown promising results. With predicted higher morbidity and healthcare costs, future prospective studies are warranted to correctly define the prevalence of metabolic abnormalities among adult nonunion patients and identify effective preventive treatments in fracture patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.