
Abstract
Introduction
Proximal phalangeal fracture is a commonly seen hand injury that constitutes up to 22% of hand fracture cases. 1 A stable, non-displaced fracture can be managed by conservative treatment with promising results. However, angulated, displaced fractures or patients requiring high demand of hand function will benefit from operative management. 2 Various treatment modalities for unstable proximal phalangeal fracture are available, including Kirschner-pin fixation, screw fixation, plating, external fixator, etc.2,3 Plating is a popular choice in the fixation of this fracture pattern. It allows anatomical reduction, and stable fixation allowing early mobilization and preferably maintaining tendon gliding for facilitating early rehabilitation in the majority of cases. 2 Usually, it is performed over the dorsal aspect of the proximal phalange as the standard method. Despite the excellent stability provided, complications including extensor tendon adhesion, and extension lag due to scarring developed around the extensor tendon. 4 It was hypothesized that the degree of soft tissue dissection, splitting of extensor tendon prior to fracture exposure, and plate fixation leads to scaring as well as adhesion due to their direct contact limiting the finger range of motion.5,6 On the other hand, lateral plating is gaining popularity as theoretically it can avoid adhesion of extensor tendon and prevent stiffness while at the same time being able to provide similar stability as evidenced by a cadaveric study. 7 Currently there is no consensus towards which approach can provide a more favorable outcome to patients.
Our study aims to compare the functional outcome of dorsal plating and lateral plating in a proximal phalangeal fracture in our local setting. We measure different objective functional parameters, and demographic data and record various post-operative complications for our analysis and comparison.
Materials and methods
Selection criteria and parameters measurement
We performed a retrospective study on patients suffering from a proximal phalangeal fracture of tri-phalangeal digits managed with plate fixation either with the method of dorsal plating or lateral plating. The research project had been approved and registered under Joint CUHK-NTEC Clinical Research Ethics Committee (reference number: CREC 2020.239) and strict confidentiality guidelines were followed.
Patients were identified through the Hospital Authority electronic medical record system in the period of the year April 2016 to January 2020. Patients with a proximal phalangeal fracture at tri-phalangeal digits who required open reduction and internal fixation with plating were included in this study with informed consent. Indication of operation included unstable fracture (pattern of fracture: spiral, long oblique, and comminuted fracture), severe initial displacement that required reduction, and re-displacement of fracture after reduction. Patients suffering from multiple proximal phalangeal fractures of the same hand were also included in this study. The exclusion criteria were as follows: open fracture, skeletal immature patients, patients who declined post-operative rehabilitation training, concomitant neurovascular bundle or tendon injury requiring repair.
Demographic data of the recruited patients were also recorded for facilitating data analysis. Age undergone operation, gender, dominant hand, smoking status, and whether the patient sustained an injury on duty were obtained as demographic data from medical records and interviews with the patient during clinic follow-up sessions or from occupational therapists' training session.
Our team also collected parameters reflecting the functional outcome including the range of motion of each joint in the injured digit (metacarpal-phalangeal joint, proximal, and distal inter-phalangeal joint), total active motion (TAM), which is the sum of the range of motion of the above-mentioned three joints, grip strength, and Belsky score 8 which is utilized for reflecting the functional outcome by grading (from excellent to poor) with reference to TAM, presence of deformity and symptoms. The range of motion and the grip strength of the contralateral normal side were also measured for comparison of the post-operative outcome. We aimed to utilize these objective parameters together with data of the contralateral hand as the baseline functional status to achieve a more comprehensive analysis of the post-operative functional outcome of our patients.
The ability of patients returning to work was also documented. It was defined as patients’ ability to return to work, either their own job or a new job, after the operation within our follow-up period.
Besides, post-operative complications including delayed union or non-union, wound infection, or aftercare operations such as tenolysis, and removal of the implant were reviewed and recorded as well.
Pre-operative and post-operative radiographs were reviewed by clinicians of our team based on AO classification for determination of fracture type and the presence of angular or rotational deformity. The post-operative radiographs provided information about the plating method, and fracture healing progress for analysis.
Operative technique
We performed the dorsal and lateral plating by our experienced specialist in a standard approach as described below to prevent variation in operative technique altering the outcome. For the dorsal approach, an incision was made at the direct dorsal side of the proximal phalanx and then the extensor tendon was split or dissected at the edge of the extensor to gain access to the fracture for fixation (Figures 1 and 2).

Photos demonstrating dorsal approach with fracture exposure and fixation.

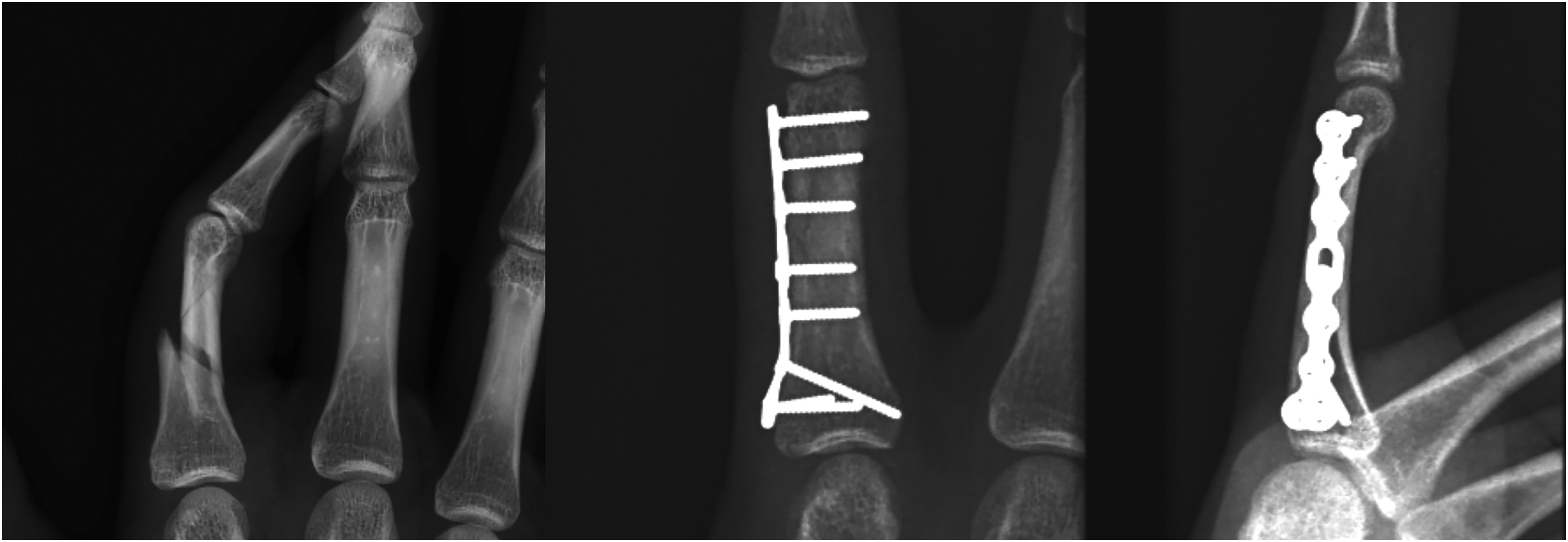
Radiographic images showing dorsal plating approach, before and after operation, respectively.
For the lateral approach, we started with a mid-axial incision at the dorsal extent of the lateral proximal phalanx, followed by dissection, identification, and protection of the neurovascular bundle. Once the above structures were protected, we opened the periosteum to perform fracture fixation. Locking plates were used for fracture fixation. 9 The plate needs to be bent in order to fit the contour of the lateral flank of the proximal phalanx base and leave space over the proximal phalanx to avoid compression to the collateral ligament causing proximal interphalangeal joint stiffness (Figures 3 and 4).

Photos demonstrating lateral approach with fracture exposure and reduction.
Radiographic images showing lateral plating approach, before and after operation, respectively.
Standard post-operative rehabilitation protocol
Patients who received an operation were required to follow the same rehabilitation protocol. Active range of motion exercise was started from post-operative day 1 with edema control by Magnetopulse device (ASA Laser, Italy), while passive stretching exercise started at 4 weeks after the operation and strengthening exercise at 8 weeks onwards.
Statistical methods
Baseline demographic characteristics between the patients in the dorsal plating group and the lateral plating group were presented using mean and standard deviation (for numeric data) or N (%) (for categorical variables). They were compared using Student's t-test or chi-square test where appropriate. Baseline demographics included age at operation, sex, fracture location, operated side, operated finger, injury on duty (yes or no), and follow-up period in the number of months. The following clinical results were compared between the dorsal plating group and lateral plating group using Student's t-test for two-group comparison and analysis of variance for multiple group comparisons: (1) different kinds of range of motion, (2) TAM, contralateral TAM, and %TAM with normal side, (3) extension lag, (4) grip strength, (5) contralateral grip strength, (6) %grip strength with the contralateral side, (7) Belsky score, and (8) return to work. Spearman's correlation analyses were carried out relating TAM, contralateral TAM, and %TAM with normal side to (1) age at operation, (2) plate position, (3) fracture location, (4) grip strength, and (5) %grip strength with contralateral side. A two-sided p-value ≤ 0.05 was considered statistically significant. All statistical analyses were carried out using IBM SPSS Version 27.0 (Armonk, NY: IBM Corp).
Results
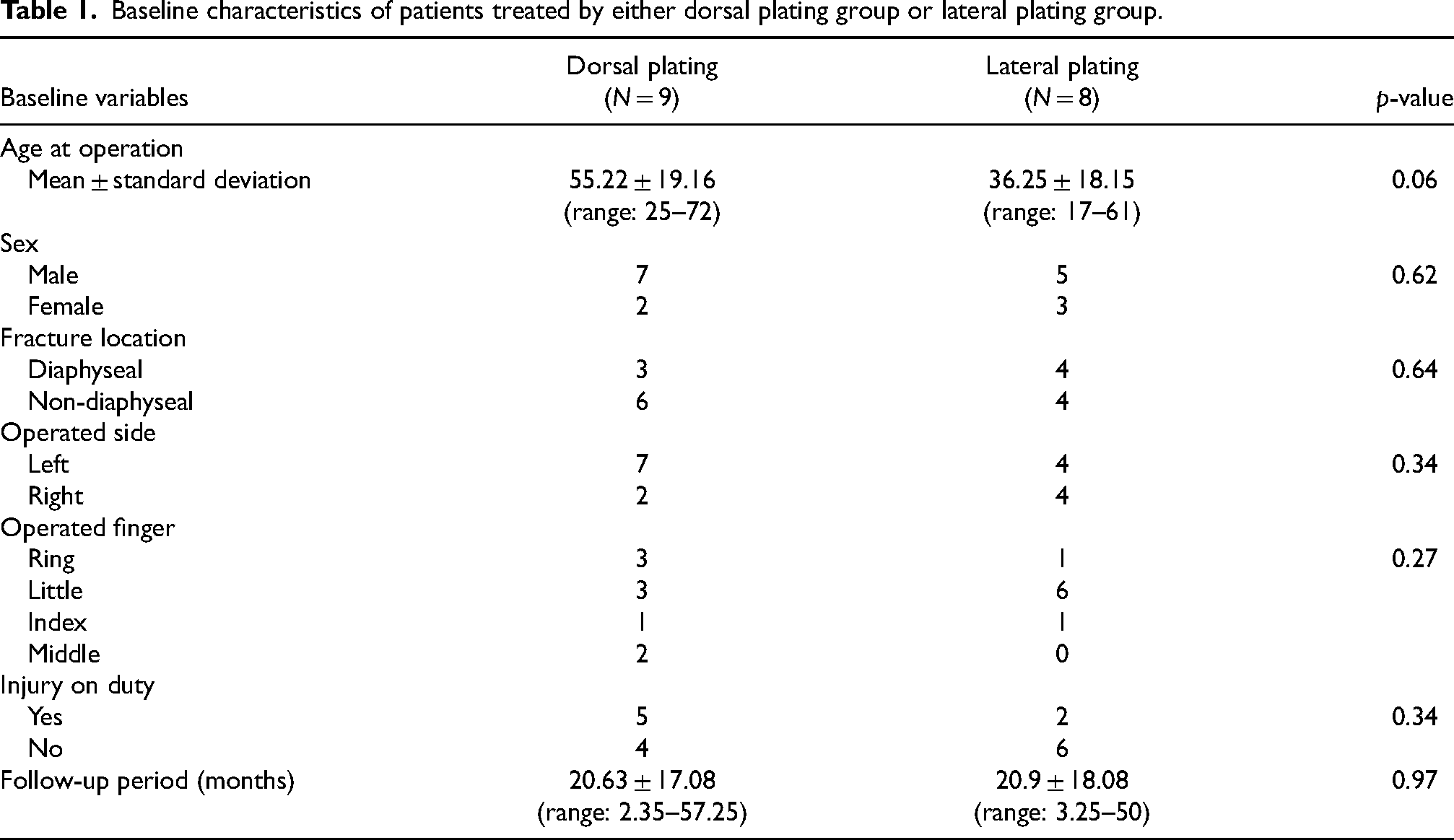
A total of 17 proximal phalangeal fractures from 14 patients fulfilling the selection criteria were included in our study (Table 1). The mean age of operation was 46.3 years old (range: 17–72), including nine males and five females. The mean follow-up period was 20.75 months (range: 2.35–57.25 months). The little finger was found to be the most commonly injured finger in our cohort, contributing nine cases, followed by the ring finger (n = 4), and the middle and index finger (n = 2). Nine cases were treated with dorsal plating while eight cases adopted the lateral plating method. We analyzed and compared the demographic data between the two study groups and no significant difference was found in those parameters.
Baseline characteristics of patients treated by either dorsal plating group or lateral plating group.
Total active motion
We combined the dorsal and lateral plating groups to look for any demographic parameters that would influence on the range of motion on the injured hand. We found that gender, diaphyseal or non-diaphyseal fracture, injured finger, and the right or left hand being operated on had no influence (i.e. p values > 0.05) on the total active motion or the percentage change in TAM of the injured side compared with normal side (Table 2). For the status of injury on duty (IOD), there was poorer TAM in the IOD group (p = 0.02). However, there was no significant difference in the percentage change of TAM regarding having IOD or not.
Effect of sex, fracture location, injury site (which finger), operated side, and injury on duty on total active motion (TAM) on the injured side, contralateral side, and %TAM.
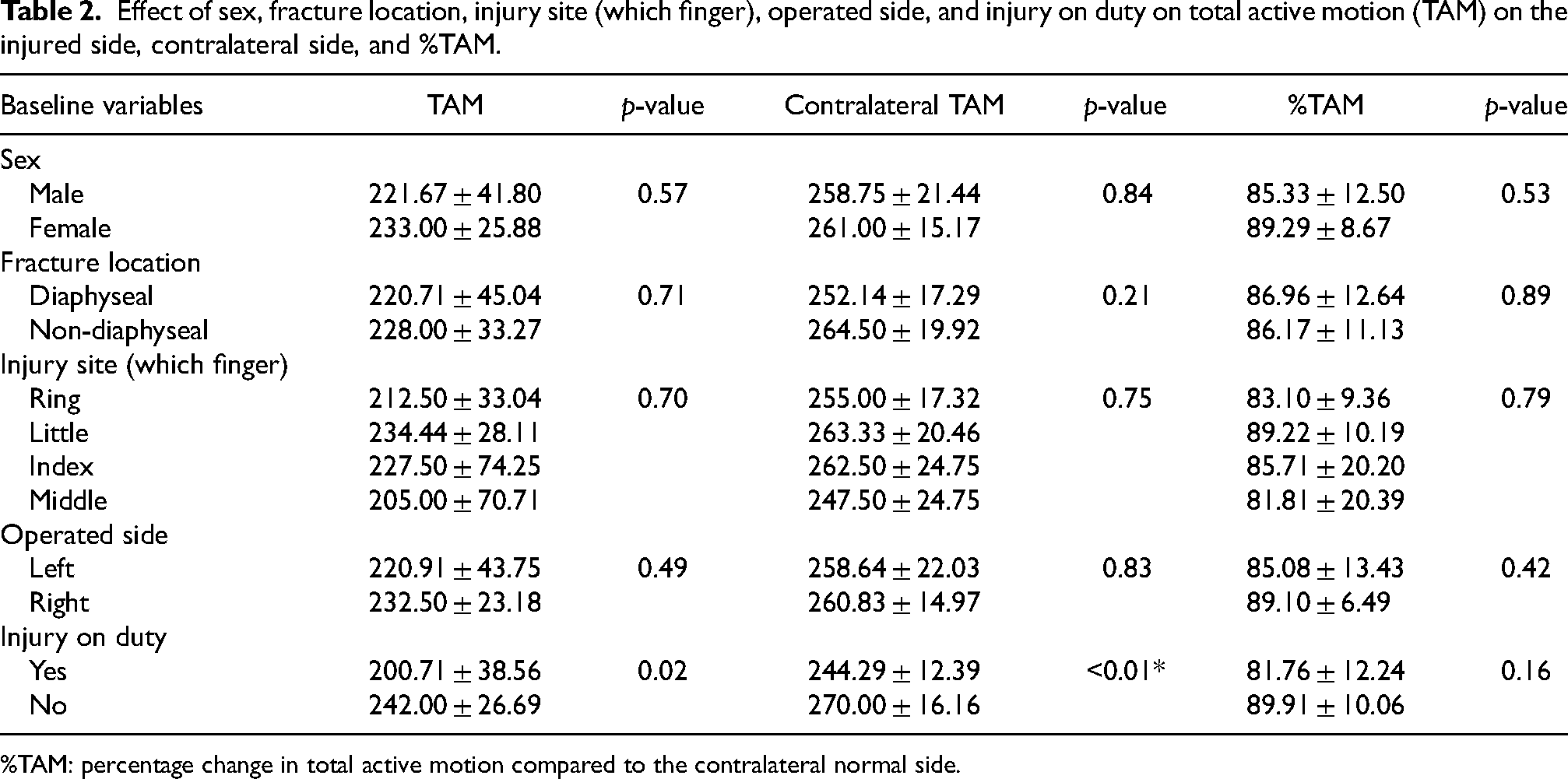
%TAM: percentage change in total active motion compared to the contralateral normal side.
By using Spearman's correlation model, we also found that age and TAM were inversely correlated which was statistically significant (Spearman's γ = −0.80, p < 0.01). In other words, with a younger age undergoing the operation, there was a better TAM outcome.
For comparison between the dorsal and lateral plating group, our team revealed statistically significant better TAM (dorsal plating (D): 203.9 ± 35.2 vs. lateral plating (L): 248.8 ± 23.7; p-value = 0.01) and percentage change in TAM (D: 79.41% ± 10.35, L: 94.47% ± 6.09; p-value < 0.01) in the lateral plating group (Table 3). As lateral plating can avoid direct contact between the metal plate and extensor tendon, it can likely prevent the formation of adhesion and preserve the gliding mechanism of extensor tendon leading to a better TAM and percentage change in TAM.
Correlation of TAM between dorsal plating group and lateral plating group.

TAM: total active motion.
%TAM: percentage change in total active motion compared to the contralateral normal side.
Extension lag
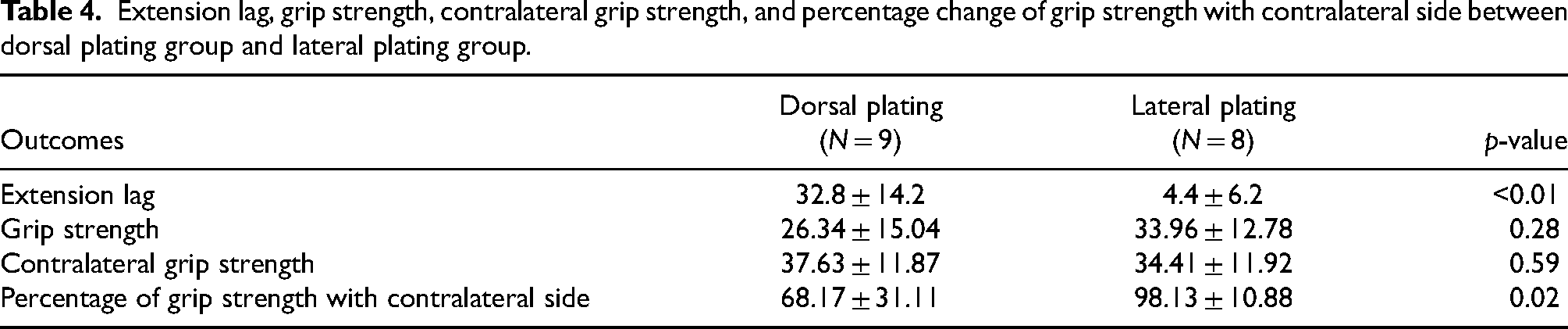
The extension deficits of each joint of the injured digit were measured. The sum of extension lag of the three finger joints was significantly larger in the dorsal group compared with the lateral group (D: 32.8 ± 14.2 vs. L: 4.4 ± 6.2, p < 0.01) which signifies a poorer range of motion in the dorsal group which also accountable by the formation of adhesion and disruption of tendon gliding mechanism (Table 4).
Extension lag, grip strength, contralateral grip strength, and percentage change of grip strength with contralateral side between dorsal plating group and lateral plating group.
Grip strength
We measured the grip strength of both hands and illustrated in terms of the percentage preserved after the operation compared with the normal side. The lateral plating group can achieve a better recovery of grip strength than the dorsal plating group as we have seen a statistically significant difference in percentage change of grip strength (D: 68.17% ± 31.11 vs. L: 98.13% ± 10.88, p = 0.02) when contralateral normal side was used as reference (Table 4). With better TAM and less extension lag, lateral plating should be able to provide better mobility for gripping and thus allow better performance in grip strength.
Belsky score and return to work
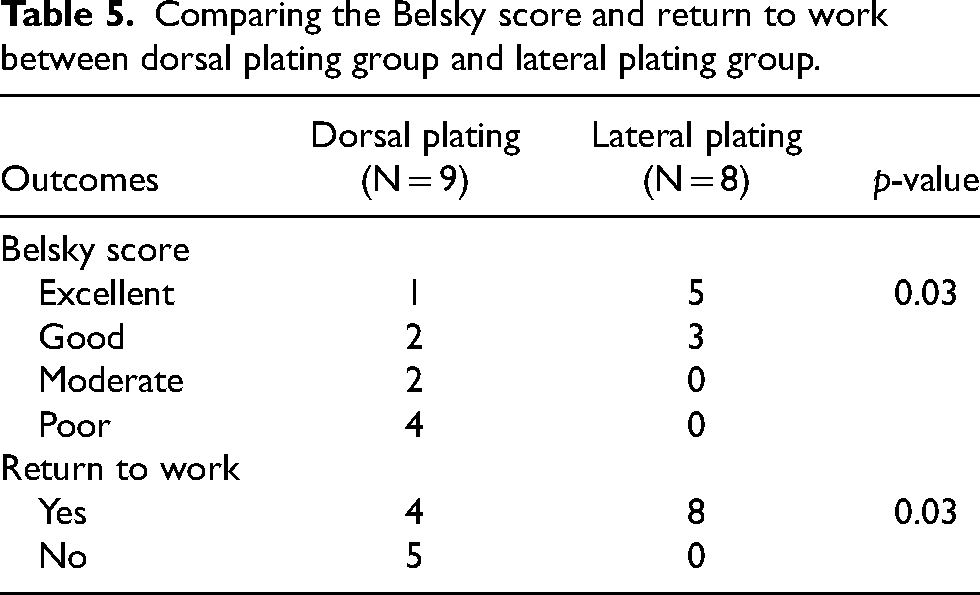
The Belsky score also showed statistically significantly better results in the lateral plating group (scored excellent: 83.3% vs. 16.7%, p = 0.03) reflecting better overall functional status in this group (Table 5). Regarding the ability to return to original work after operation, with the better functional status, the lateral plating group also showed notably better results with eight out of eight patients could return to work while only four out of nine patients are able to do so in the dorsal plating group (100% vs. 44.4%, p = 0.03) (Table 5).
Comparing the Belsky score and return to work between dorsal plating group and lateral plating group.
Complications and aftercare operations
There was no post-operative wound infection, delayed union, or non-union noted in our series of cases. Both the dorsal and lateral plating groups had one patient who required tenolysis at 11 and 9 months after index operation, respectively, with TAM improvement of 15° and 10°. Three patients underwent removal of implant (two dorsal and one lateral plating) an average of 11 months after operations.
Discussion
The literature revealed multifactorial contributions to the development of adhesion and stiffness after phalangeal fracture with plate fixation. They believed that complications including stiffness were mainly contributed to increasing age, soft tissue handling technique, initial fracture severity, and plate interference with tendon excursion.5,10 With the severity of fracture already being determined at the moment of injury, the other two factors are controllable with operative technique and surgical approaches for plating.
Controversy presents regarding which approach of proximal phalanx fracture plating can provide a better outcome in terms of mobility and complication rate. Robinson et al. 11 described similar outcomes in a range of movements comparing dorsal and lateral plating patients in a retrospective study. While Page and Stern 12 revealed an unsatisfactory motion range in dorsal plating. A similar finding was also reported by Brei-Thoma et al. 13 regarding a high rate of extension lag and poor TAM value. Another study conducted by Omokawa et al. 14 demonstrated better results in maintaining the range of movement in the lateral approach. In our study, we reached a similar conclusion that lateral plating can achieve a better range of motion together with greater recovery of grip strength compared with the dorsal approach. It is believed that the dorsal approach required the splitting of the extensor tendon together with subsequent direct contact of plate and tendon which resulted in the formation of scar tissue and adhesion. 15 Scar formation and adhesion will be exacerbated when the skin incision is also planned directly above and parallel to the tendon-splitting line. These factors lead to ineffective extensor action and extension lag. Poor hand mobility may then further jeopardize grip strength and other hand functions.
The above deduction postulates the rationale of how the lateral approach provides a more promising operative outcome. However, this approach is regarded as more technically demanding. Careful soft tissue dissection and protection are of paramount importance as disruption of neurovascular structure is detrimental to the functional recovery of the injured finger. Damaging the digital nerve may lead to the formation of painful neuroma as well. In addition, we must be alert about the curved surface of the lateral proximal phalanx and bend the plate for better contouring to fit the curved surface of the bone in order to avoid mal-alignment or even further displacement of the fracture (Figures 2 and 5(a) and (b)). For fractures adjacent to the base or head of the proximal phalanx, special attention in plate contouring to prevent compression and impingement on the collateral ligament is required, as it will affect the motion range of the corresponding joint.
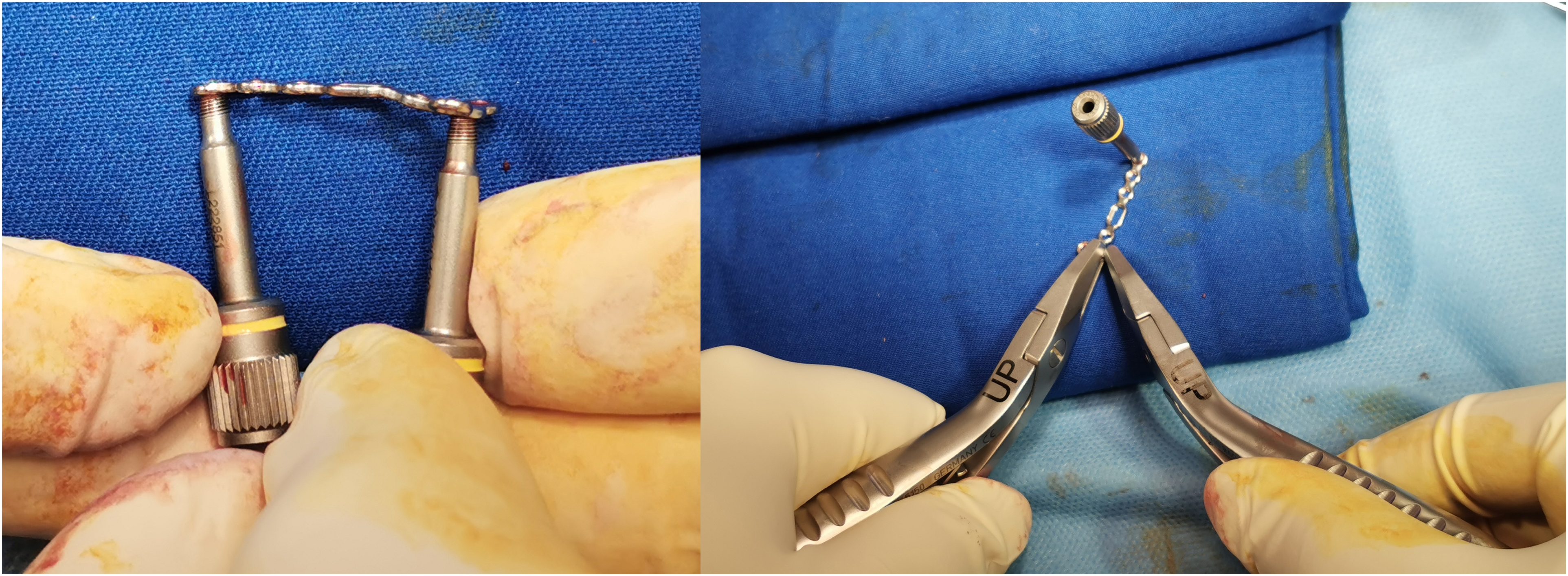
Photos demonstrating plate bending technique to ensure smooth contouring over lateral proximal phalanx to prevent mal-reduction of fracture, compression, or impingement of collateral ligaments which may cause stiffness.
Our study is a more focused study on the comparison of the two plate fixation approaches in the proximal phalanx in tri-phalangeal digits. We adopted multiple objective parameters including TAM, grip strength, and Belsky score to reflect the functional outcome after fracture fixation. These parameters can demonstrate the operative result in a more systemic and comparable manner. The mean follow-up time was 20.75 months which was reasonably long enough to demonstrate short- and long-term complications of fracture healing or soft tissue injury should it occur. Operations for our patients were mainly provided by experienced hand specialists of our center which can lower the variability of operative outcome due to surgeon's factor. Moreover, a standard rehabilitation program was adopted, and patients were ensured to follow the destinated plan by regular review of our occupational therapist team. This can guarantee our final analyzed results were not affected by variations in the rehabilitation plan which the effect could be significant.
Despite the above-mentioned characteristics, our study does have some limitations. First of all, we have a relatively small sample size which is more prone to Type II errors. Secondly, even though we have statistically comparable demographics between the two groups, a retrospective study is still unable to eliminate confounding factors as compared to a prospective controlled study. However, a prospective or randomized study may be difficult to conduct in this setting as operative decision, duration from injury to operation, and adoption of specific approach cannot be solely determined by randomization, multiple factors must be considered instead. And this decision-making process leads to another limitation: there may be a bias of inclining to a preferred approach in some specific fracture patterns or degree of severity which in turn altered the study outcome.
In summary, based on the result of our study, the lateral approach in plate fixation of proximal phalanx fracture provided a more favorable outcome in terms of the range of movement, grip strength, and Belsky score. There is also a low complication rate in our series of cases. Further efforts to expand the study size would be beneficial in conducting a more comprehensive comparison.
Footnotes
Declaration of conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by The Joint Chinese University of Hong Kong – New Territories East Cluster Clinical Research Ethics Committee (The Joint CUHK-NTEC CREC) with reference number CREC 2020.239 on 2 June 2020.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
There is no information in the submitted manuscript that can be used to identify patients.