
Abstract
We describe a novel technique for reconstructing a Leddy and Packer type Va flexor digitorum profundus avulsion using a K-wire to stabilize the extra-articular component and as a post for suture repair of the avulsed fragment.
Leddy and Packer type Va is an avulsion of the flexor digitorum profundus tendon from the distal phalanx, associated with an extra-articular fracture (Al-Qattan, 2001; Leddy and Packer, 1977). It is rare for the fragment to retract into the A4 pulley. A 48-year-old woman sustained this injury to her left little finger while playing rugby. It was a closed, isolated, neurovascularly intact, non-dominant injury (Figure 1). We present a novel technique for stabilizing the distal phalangeal fracture and suture repair of the avulsed fragment and attached tendon.
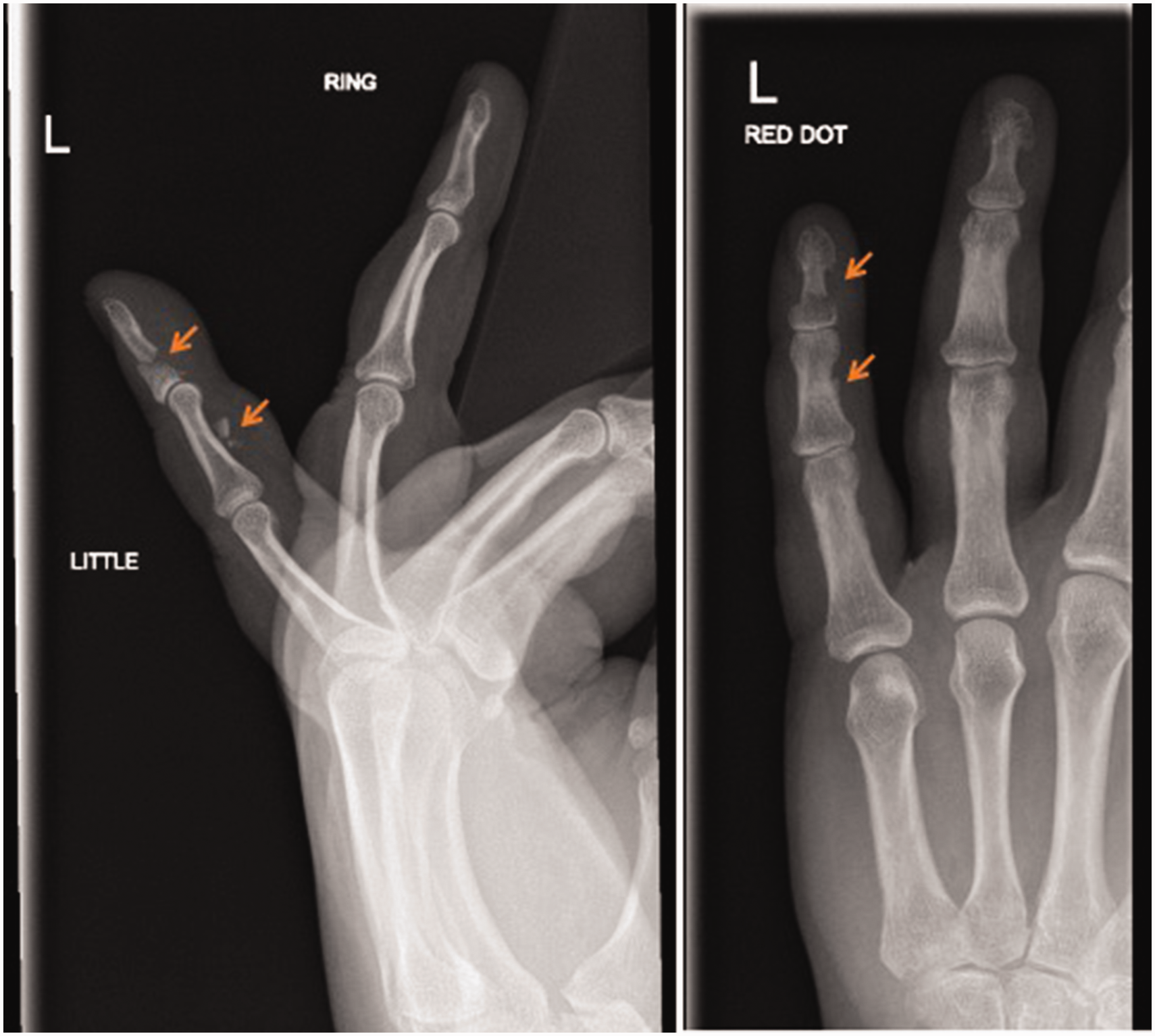
Pre-operative radiographs, (a) lateral and (b) anteroposterior, demonstrating the retracted FDP avulsion fracture of the left little finger (arrows indicating avulsed retracted fracture fragment and associated extra-articular fracture of the distal phalanx).
Surgery was carried out 6 days after the injury under general anaesthesia, tourniquet and intravenous antibiotics. A mid-lateral radial incision was made and extended into the distal palmar pulp. The flexor sheath was exposed and the neurovascular bundles protected. A small rent was made in the flexor sheath between the C3 and A5 pulleys and the fracture site haematoma was removed. The retracted avulsed fragment with attached the FDP tendon was located within the A4 pulley, pulled distally and temporarily secured with a hypodermic needle. Owing to its friability, the A5 pulley was incised to aid repair. A 1.1 mm K-wire was then advanced from the fracture site through the distal fracture fragment and out of the fingertip (Figure 3(a)). The wire was then passed retrograde back through the distal and proximal fragments, stabilizing the extra-articular fracture and advanced to transfix the distal interphalangeal joint (DIPJ) (Figure 3(b)). The K-wire was left outside the skin for later removal. It was just visible in the fracture site but there was no space for a suture anchor to be inserted so the K-wire was used as a post for the suture repair, looping a 4–0 Ethibond suture (Ethicon Inc, Somerville, New Jersey, USA) around it and with a locked multiple grasping suture securing the avulsed fragment to the distal phalanx base (Figure 2). This grasping suture technique was used because it achieves an excellent secure hold in a delaminated tendon preserving its vascularity and allowing excursion into the A4 pulley. The hand was immobilized in a position of safe immobilisation for 2 weeks with slight wrist extension, 90° of metacarpophalangeal joint flexion and extension of the interphalangeal joints. Mobilization of all other joints was started and the K-wire was removed 6 weeks after the surgery to allow healing of the avulsed fragment. After 3 months of physiotherapy, active little finger flexion was 78° at the MCPJ, 78° at the proximal interphalangeal joint and 42° at the DIPJ with a full passive range of motion and adequate grip strength (left 24 kg vs. right 34 kg).
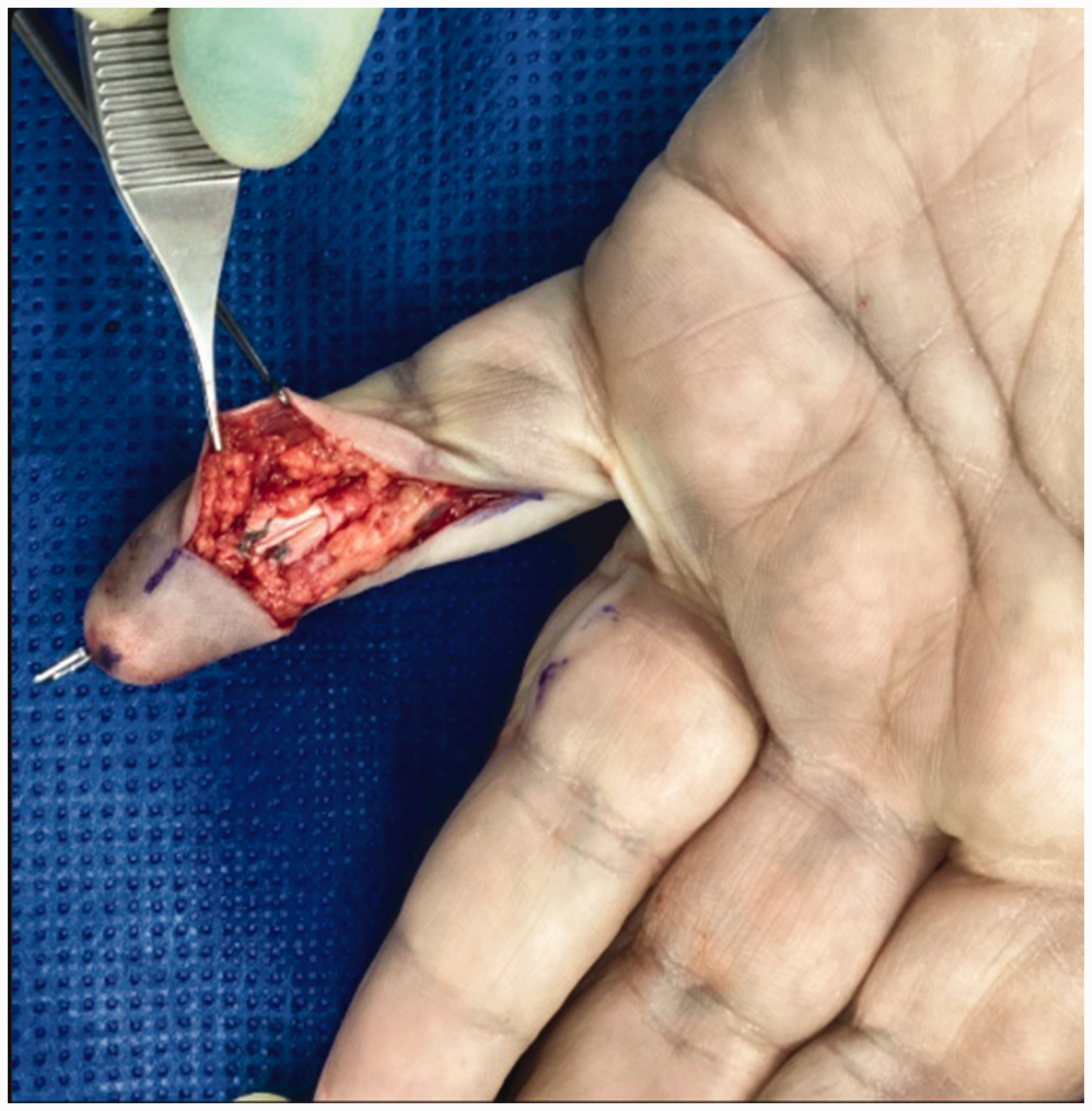
Intra-operative clinical photograph taken of the suture repair.
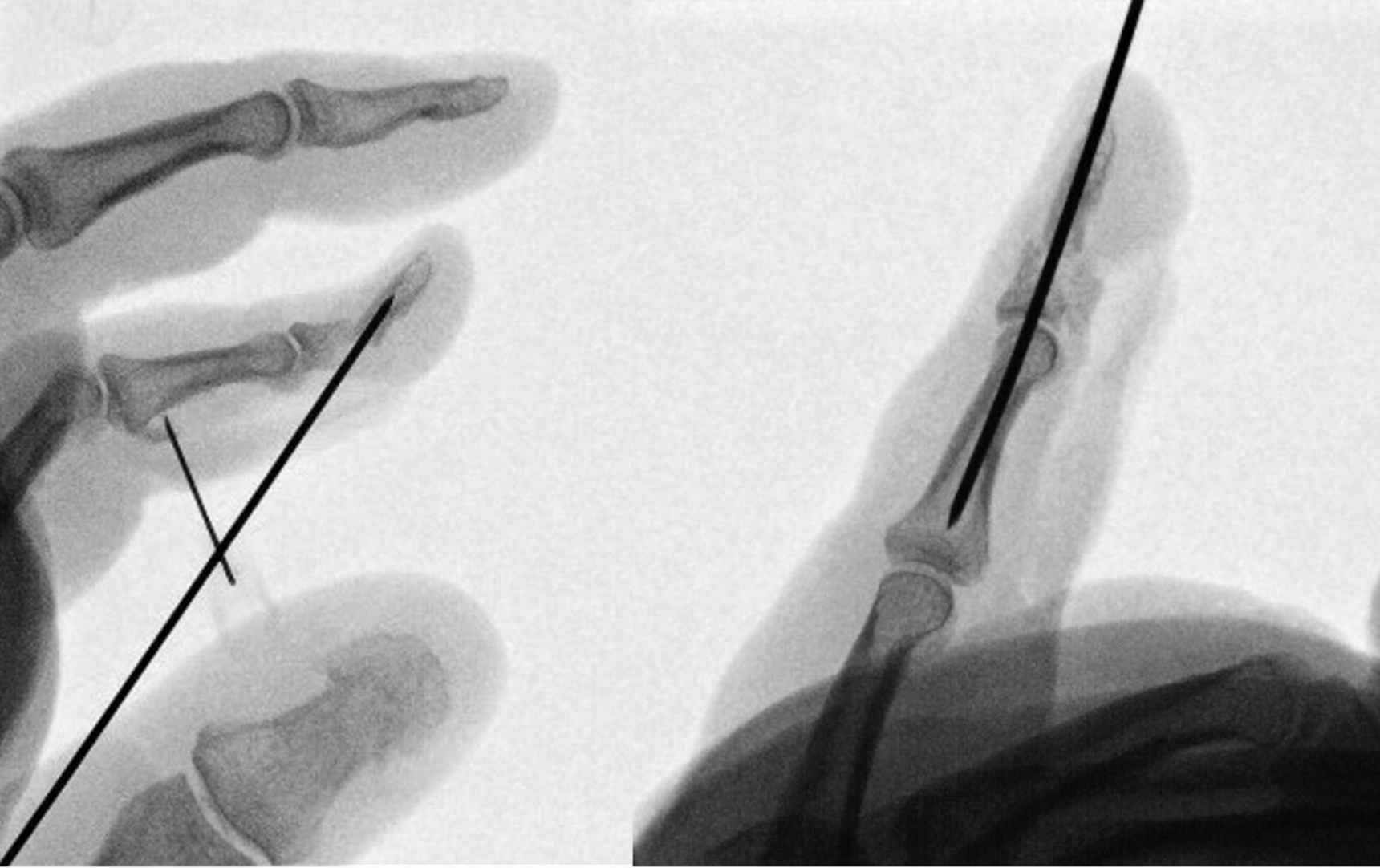
Intra-operative fluoroscopic images showing the wire passed antegrade through the fracture site (a) and then retrograde to stabilise the fracture transfix the joint (b).
The single pass K-wire stabilisation of the extra-articular distal phalangeal fracture preserves bone stock and reduces comminution and the risk of joint degeneration. The K-wire acts as a post for the suture repair of the avulsed fragment and attached FDP tendon. As the management of type Va Leddy and Packer FDP avulsions is difficult (Hoppe et al., 2024), we recommend our technique as an effective and safe reconstruction option.
Footnotes
Declaration of conflicting interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient for the publication of this technical tip.
Ethical approval
Ethics committee/IRB approval not required.