
Abstract
People with severe carpal tunnel syndrome with thenar muscle atrophy suffer from loss of dexterity of the affected hand, which hinders their daily lives. There are different options for opponensplasty. The more traditional option is Camitz operation combined with open carpal tunnel release (OCTR). Another option is to use the flexor digitorum superficialis of the ring finger (FDS4) for opponensplasty and to combine it with endoscopic carpal tunnel release (ECTR). In this study, we prospectively compared the surgical outcomes of these two methods. A total of 27 cases were recruited (13 Camitz
Introduction
Carpal tunnel syndrome is the most common peripheral entrapment neuropathy. 1 It affects 3.8% of the adult population worldwide.2,3 Those suffering from carpal tunnel syndrome have symptoms of tingling, pain, and numbness in the median nerve distribution. In severe cases, patients will have thenar muscle atrophy and loss of thumb opposition, resulting in the loss of dexterity of the affected hand. 4 Such reduction may affect their work performance and activities of daily living.
Opponensplasty is an essential surgical method to restore thumb opposition function. There are many different options for opponensplasty. The first opponensplasty was described by Steindler in 1917. 5 Camitz, in 1929 reported his method of opponensplasty using the palmaris longus (PL) tendon with the palmar aponeurosis. 6 Bunnel first described using the flexor digitorum superficialis (FDS) for transfer to restore thumb opposition in 1938. 7 Later, Royle, Thompson, and Brand et al. reported their modifications of this FDS transfer for opponensplasty.8–10 Huber described the use of the abductor digiti minimi as a method of opponensplasty for children with thumb hypoplasia in 1963. 11 Burkhalter et al. reported the use of extensor indicis proprius for opponensplasty in 1973. 12 This method is mainly used for high median nerve palsy cases and those with combined median and ulnar nerve palsies. Schneider, in 1969, suggested an alternative method of opponensplasty by using the extensor digiti minimi with good results. 13
Camitz procedure combined with open carpal tunnel release (OCTR) was first described by Littler in 1967. 14 Since then, Camitz procedure with OCTR has become a standard operative treatment for severe carpal tunnel syndrome with thenar wasting. 15 Its surgical outcomes had been reported to be satisfactory, 16 but this had also given rise to a couple of complications, related to the extensive dissection of the palm. 17
FDS of the ring finger (FDS4) opponensplasty, on the other hand, utilizes three small incisions to transfer the FDS4 to the abductor pollicis brevis (APB) to restore thumb opposition. With an addition of a fourth small incision, it can be combined with endoscopic carpal tunnel release (ECTR). It had been shown to have a good outcome with satisfactory improvement in thumb and hand function, as well as good sensory and motor recovery. 18
We hypothesized that FDS4 opponensplasty
Methods
This is a prospective comparative study. The study has received approval from the institutional ethical committee.
All patients with severe carpal tunnel syndrome and thenar muscle atrophy who received operations in our hospital from January 2015 to December 2021 were recruited. All patients were clinically diagnosed with carpal tunnel syndrome and electro-physiologically through nerve conduction studies. The symptoms include numbness, pain, and tingling sensation along the median nerve distribution. The clinical signs include positive Phalen's test and Durkan's test. Another critical clinical sign is muscle atrophy over the thenar eminence with the APB muscle power less than 2 out of 5. These patients were allocated to one of the study groups according to patients’ preference: (1) Camitz Procedure
Exclusion criteria include pediatric patients, patients with previous surgical treatment for carpal tunnel syndrome on the same limb and those who failed to complete the pre-operative or post-operative assessments.
For statistical analysis, sample size required was calculated using a 95% confidence interval, power of 0.8, and with reference to the post-operative pulp-pinch strength in Camitz
Surgical techniques
Camitz + OCTR
Before the operation, the presence of PL must be confirmed clinically by opposing the thumb to the little finger with the wrist slightly flexed. If the PL tendon is absent, the procedure is contraindicated. The surgery can be performed under general or local anesthesia.
An incision is extended from the distal palmar crease to 2 cm proximal to the distal wrist crease. A 1.5- to 2-cm strip of palmar aponeurosis is elevated along the third and fourth fingers, taking care not to damage the underlying neurovascular structures. The sheet of palmar aponeurosis is rolled into a tubular structure and sutured with absorbable suture. Then the transverse carpal ligament is incised, and the carpal tunnel is released.
A second incision is made over the dorso-radial aspect of the thumb metacarpophalangeal joint. A subcutaneous tunnel is made between the thumb wound towards the wrist, along the axis of the APB muscle. The PL tendon is then transferred from the wrist to the thumb. The PL is weaved through the insertion of the APB tendon and the dorso-radial capsule with pulvertaft technique. All the wounds are closed with non-absorbable sutures (see Figures 1–3).

Pre-op clinical photo (to be put under surgical techniques: camitz + OCTR).
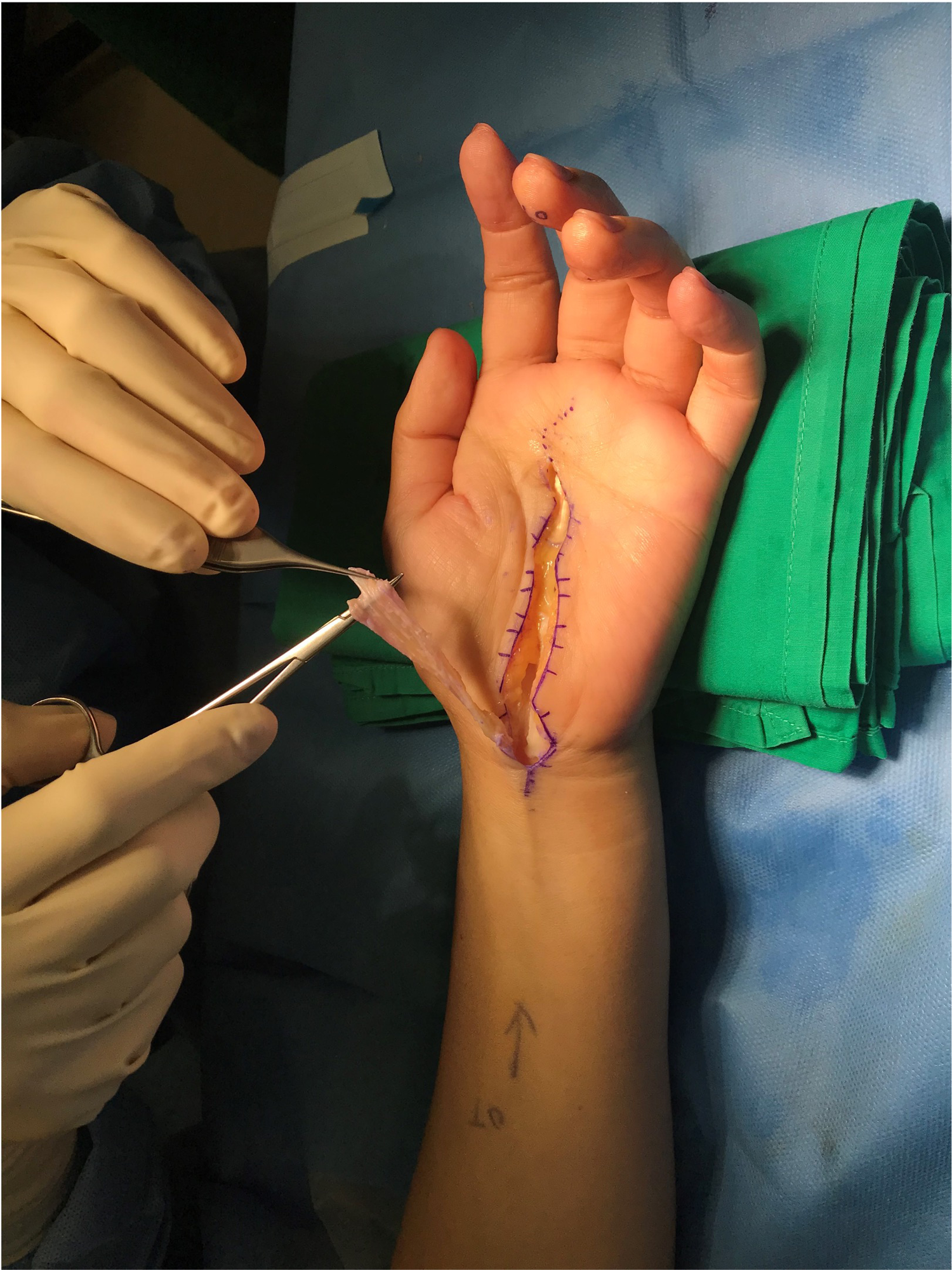
Intra-op clinical photo (to be put under surgical techniques: camitz + OCTR).

Post-op clinical photo (to be put under surgical techniques: camitz + OCTR).
FDS4 + ECTR
Before the operation, the presence of FDS4 tendon is tested. This procedure should be avoided in cases with a previous ring finger injury. This procedure is performed under local anesthesia or BIER's block. First of all, ECTR with modified Chow's two-portal technique was performed. For the entry portal, a 1-cm incision is made ulnar to the PL tendon, along the proximal wrist crease. The exit portal is created at the intersection point between the thumb abducted line and along the line extended from the radial border of the ring finger. A 4.0-mm arthroscope was inserted to visualize the transverse carpal ligament, which is then released with a retrograde knife. After releasing the carpal tunnel, the wrist wound is extended ulnarly to around 2 cm in length and the FDS4 tendon is identified. Another incision at the level of the A1 pulley of the ring finger is incised. The A1 pulley is released and the FDS4 tendon is identified and transected just proximal to the chiasma. The FDS4 tendon is then delivered to the wrist wound, loop around the Flexor carpi ulnaris (FCU) tendon to create a better line of pull.
Similar to the Camitz procedure, a second incision is made over the dorsal–radial aspect of the thumb metacarpophalangeal joint. A subcutaneous tunnel is made between the thumb wound towards the wrist, along the axis of the APB muscle. The FDS4 tendon is then transferred from the wrist to the thumb. The FDS4 tendon is weaved through the insertion of the APB tendon and the dorso-radial capsule with pulvertaft technique. All the wounds are closed with non-absorbable sutures (see Figures 4–6).

Pre-op clinical photo (to be put under surgical techniques: FDS4 + ECTR).

Intra-op clinical photo (to be put under surgical techniques: FDS4 + ECTR).
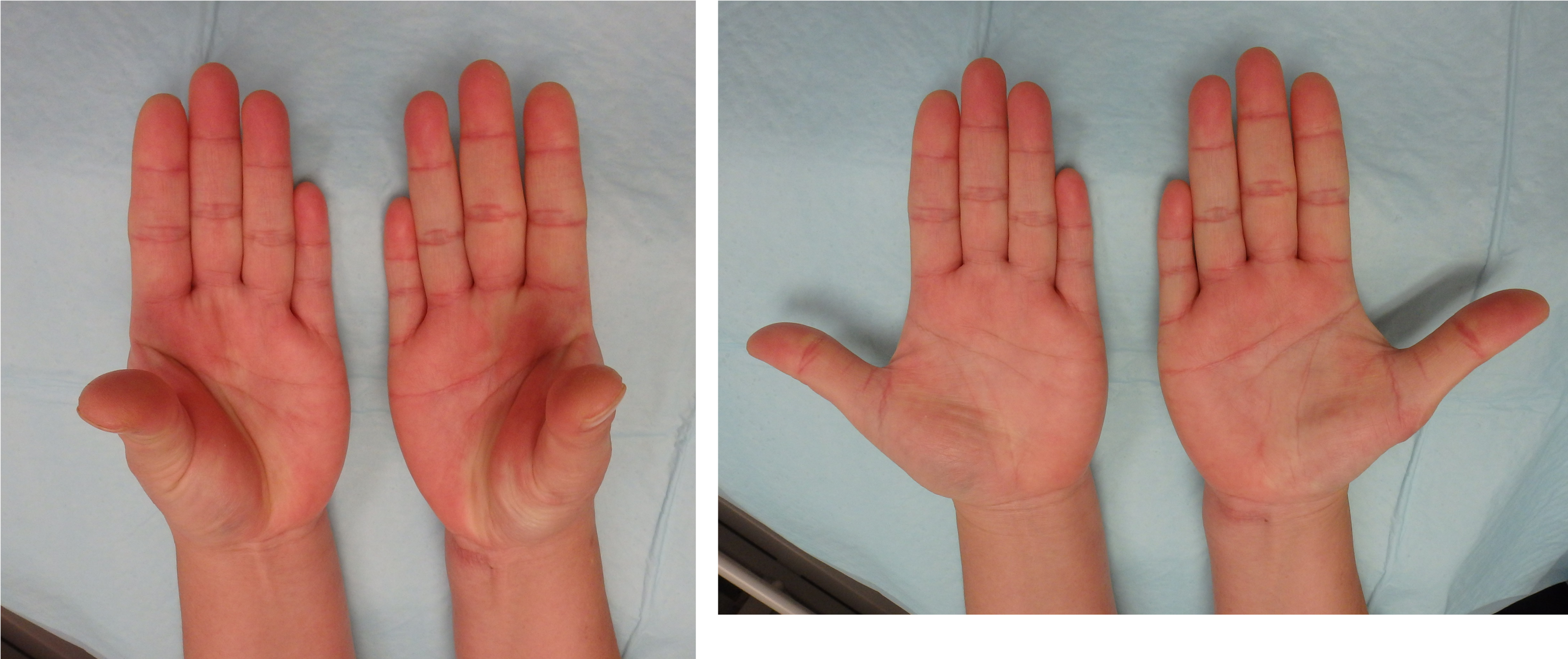
Post-op clinical photo (to be put under surgical techniques: FDS4 + ECTR).
Tension of transfer
During the transfer, the transferred tendon is slightly over-tensioned by putting the thumb in maximal abduction while the wrist is in neutral position.
Rehabilitation regime
The rehabilitation regime is the same for both groups of patients. A thumb spica cast is applied for three weeks. A thumb spica splint is given from week 3 to week 4, while the patient is allowed to make some gentle thumb motions out of the splint. Starting in week 5, the thumb spica splint is kept for another two weeks during night-time.
Results
A total of 28 cases were recruited in this study. Fourteen cases were allocated to Group 1 (Camitz
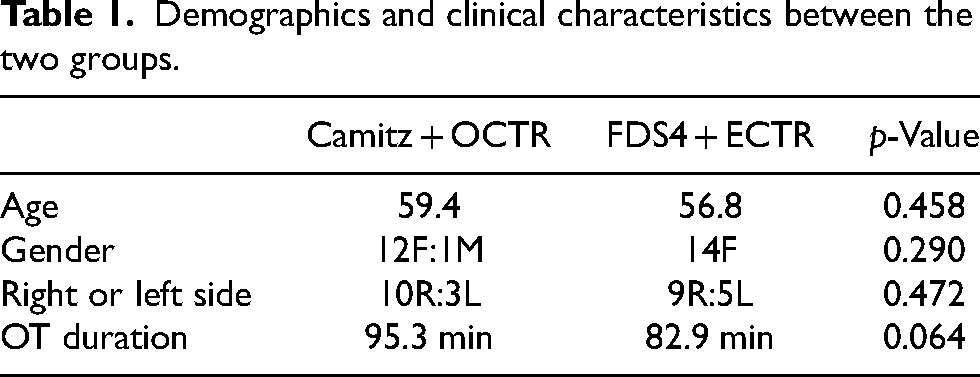
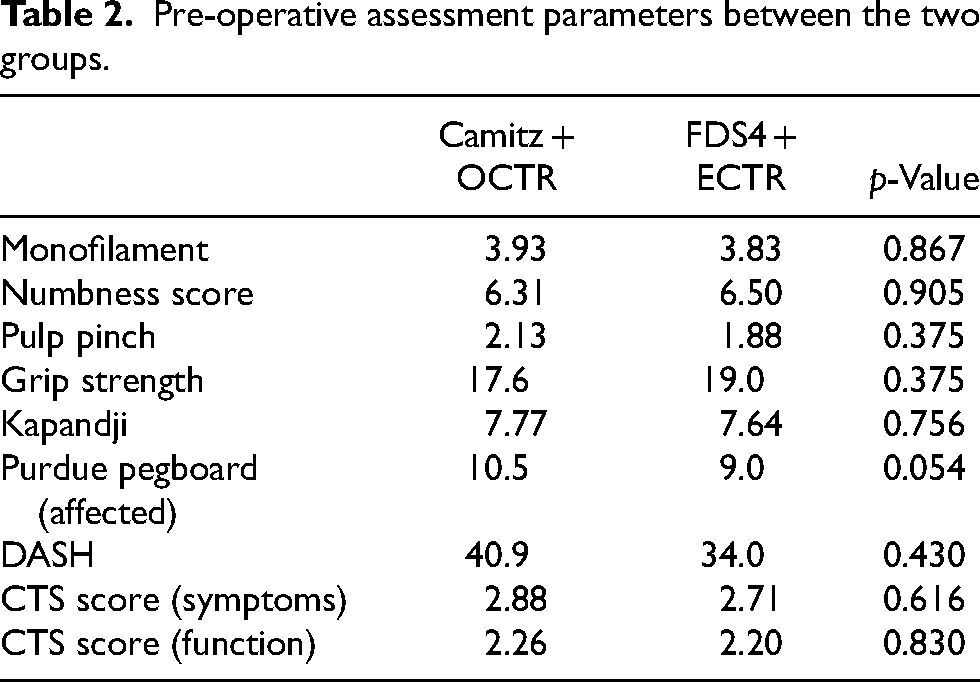
The two groups’ demographics and clinical characteristics were compared and summarized in Table 1. Both groups were comparable in age, gender, side of involvement, and operation time. The pre-operative assessment parameters were summarized and compared in Table 2. All pre-operative assessment parameters were comparable between the two groups.
Demographics and clinical characteristics between the two groups.
Pre-operative assessment parameters between the two groups.
Nine outcome assessment parameters were used to compare the changes within each of the study group. The results are summarized in Table 3. Each outcome assessment at post-op 3 months, 6 months and 12 months was compared with the pre-operative value. For the monofilament test, both Group 1 and Group 2 got statistically significant improvements at 3 months, 6 months, and 12 months. The subjective numbness score also showed a similar pattern of improvement. This suggested that both groups of patients achieved good sensory recovery after the surgery. For the pulp-pinch strength, Group 1 had a decrease in the pulp-pinch strength at 3 months, but this improved with time and got statistically significant improvement at 12 months. While in Group 2, the pulp-pinch strength showed gradual improvement over time. For the grip strength, both groups showed similar patterns, with an initial decrease in grip strength at 3 months but later improved and returned to pre-operative value at 6 months. For the Kapandji score, Group 2 performed better in terms of improvement in Kapandji score at 3 months, while Group 1 had a drop in the Kapandji score at 3 months, although not statistically significant. Both groups showed improvement in thumb dexterity, as shown by the perdue pegboard test (affected hand). Both groups showed similar improvement trends for the quick DASH Score, CTS questionnaire (symptoms score), and CTS questionnaire (function score).
Within group difference at four different time intervals: pre-op, 3 months, 6 months, and 12 months.
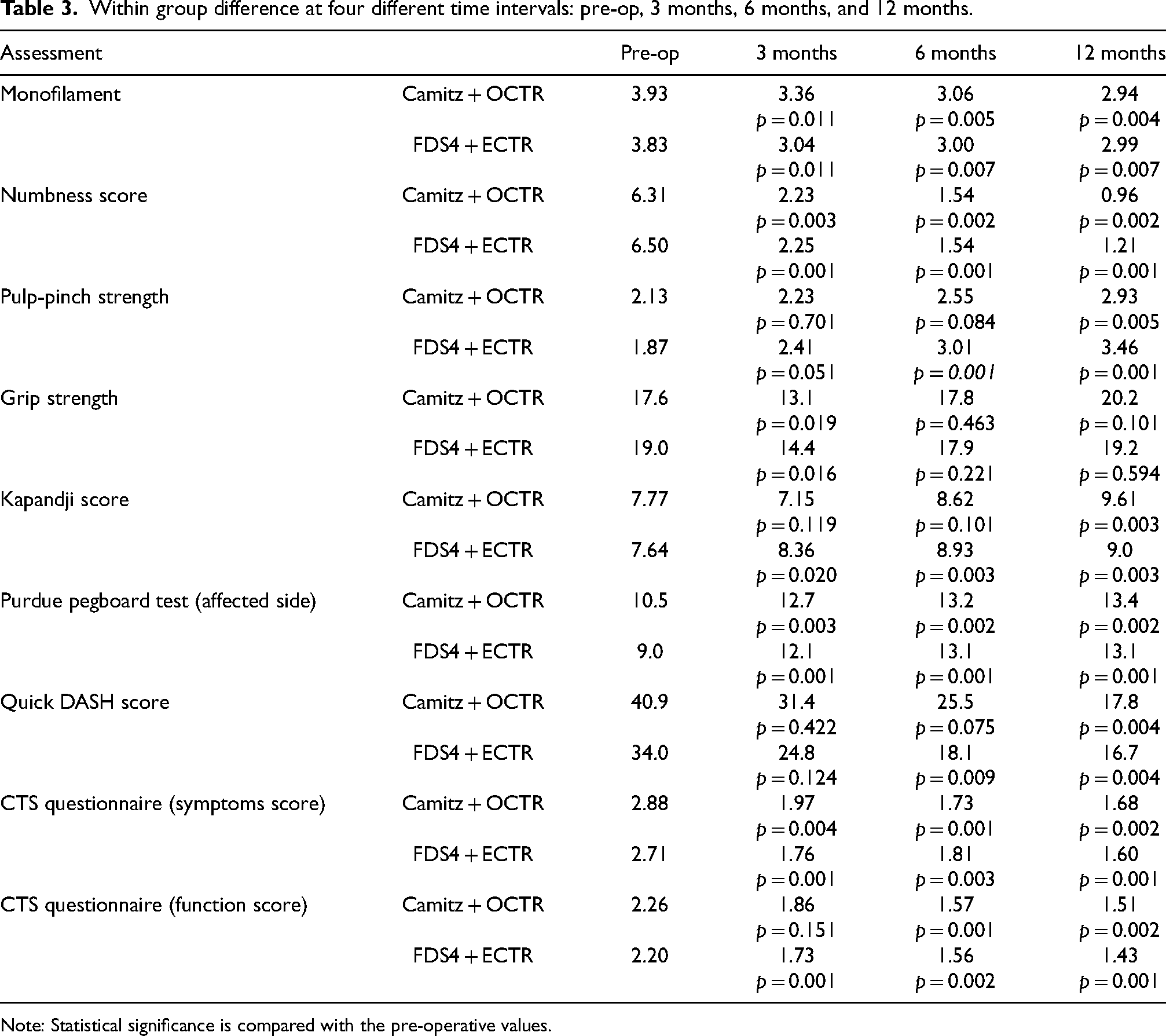
Note: Statistical significance is compared with the pre-operative values.
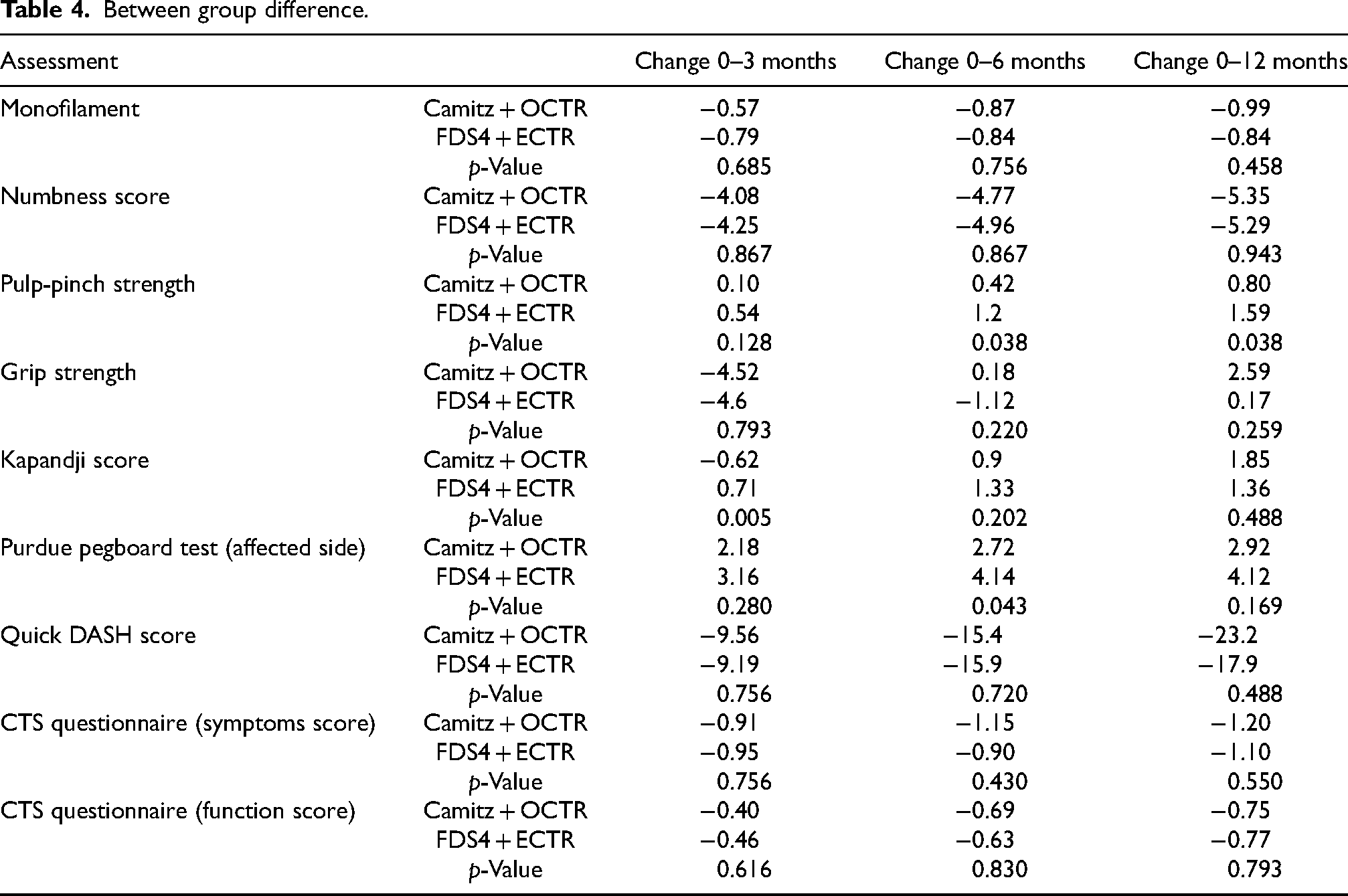
For the between-group comparison, the results are summarized in Table 4. The values were compared between the two groups at each time interval: (1) between pre-operation and 3 months; (2) between pre-operation and 6 months and (3) between pre-operation and 12 months. Group 2 patients had a better improvement in the pulp-pinch strength at 6 months and 12 months. Group 1 patients showed a significantly inferior score for the Kapandji score at 3 months post-operatively. However, this discrepancy between the two groups was no longer seen at 6 months and 12 months. Group 2 performed better in Purdue pegboard test (affected side) at 6 months, but this discrepancy was not observed at 3 months and 12 months.
Between group difference.
Discussion
Our study has demonstrated that both groups of patients (Camitz procedure
Such outcomes are comparable with other studies on the Camitz procedure. 20 Nobuta et al. 21 reported improvement in CTS score (function and severity score) and pulp-pinch strength, while Park et al. demonstrated improvement in Kapandji score and numbness after the Camitz procedure. 22 Foucher et al. in 1991 reported that 91% of patients had good long-term results after the Camitz operation, and that 80% regained hand function. 23 Terrono et al. reported that 94% of their patients were satisfied with thumb function after the Camitz operation. 13
The procedure of FDS4 opponensplasty also showed promising clinical outcomes. This procedure has been gaining popularity recently 24 to treat severe carpal tunnel syndrome due to its potential advantages of smaller wounds, and hence less pain and better cosmesis, compared with traditional Camitz procedures. 25 A case series of ECTR combined with FDS4 opponensplasty was reported in 2019. They reported good improvement in thumb abduction and opposition, sensory and motor recovery, and early return to work in patients with severe CTS. 14
A recent study compared modified Camitz and FDS transfer for severe carpal tunnel syndrome patients. Both groups received OCTR. The outcomes were similar for both surgical techniques in terms of improvement in DASH score, Kapandji score, pulp pinch, key pinch and thumb pronation angle. They suggested that both methods have equal effectiveness and could be used interchangeably. 19 Our study echoed their results. However, both of their techniques involve OCTR, which permits internal neurolysis of the median nerve. While for ECTR, internal neurolysis is not possible. Curtis and Eversmann reported in 1973 that internal neurolysis was an effective surgical adjunct for the treatment of severe carpal tunnel syndrome with thenar atrophy. They suggested that internal neurolysis can increase the success of surgical treatment. 26 Gelberman, on the other hand, provided evidence that internal neurolysis is not necessary to provide good results in patients with severe carpal tunnel syndrome. 27 Hence, we can postulate that ECTR can achieve comparable results despite no internal neurolysis can be performed. Our study demonstrated that both groups of patients showed similar improvement in terms of sensory recovery, and hence, confirmed the theory that internal neurolysis is not necessary to provide good sensory recovery in cases of severe carpal tunnel syndrome.
Our study showed that there was better pulp-pinch strength with using the FDS4 opponenplasty. Previous studies have shown that the tension and excursion of the FDS are comparable to the APB muscle. 10 Therefore, the FDS4 muscle acts as a strong donor for opponensplasty and can provide reasonable restoration of pulp-pinch strength. 14
The FDS4 opponensplasty
Other potential drawbacks of the Camitz procedures were not observed in our series. These include injury to the palmar cutaneous branch of the median nerve and radial deviation of the transferred tendon. 7 While for FDS IV opponensplasty, possible drawbacks include flexion contracture of the proximal interphalangeal joint of the donor ring finger, limitation in ring finger extension, and deviation of the transferred tendon.28,29 These were also not observed in our cases.
Conclusion
This is the first study to compare the outcomes of Camitz procedure
Footnotes
Authors’ contribution
Both authors researched literature, conceived the study, were involved in protocol development, gaining ethical approval, patient recruitment, data analysis, writing draft and editing the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report these cases was obtained from Hospital Authority, Hong Kong with the reference number of KC/KE-20-0262/ER-2.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.
Trial registration
Hospital Authority, Hong Kong with the reference number of KC/KE-20-0262/ER-2.