
Abstract
Keywords
Introduction
Trauma is a substantial cause of morbidity and mortality globally and is one of the leading causes of mortality in persons under 45 years 1 despite advances in technology and medical care. One of the determinants of outcome after a traumatic event is the patient's injury severity. 2 Trauma scoring systems were developed to quantify the injury severity and are categorised as physiologic scores, anatomic scores and combined scores. Trauma scoring systems facilitate an audit of trauma centres, triage patients in the event of a multiple casualty event, predict the survival probability after a traumatic event and document the epidemiology and magnitude of trauma as a cause of mortality and morbidity in a region.
The Injury Severity Score (ISS) was developed by Baker et al. in 1974. 3 It is an anatomic scoring system based on the Abbreviated Injury Scale (AIS). The latter was developed by the Committee on Medical Aspects of Automotive Safety of the American Medical Association in 1971. 4 The AIS has seen periodic revisions. The latest version divides the body into six regions, head and neck, face, thorax and abdomen, including the pelvis, extremities and external. Injuries in each region are ranked from one (minor) to six (fatal). 2 The ISS combines the sum of the squares of the three regions with the highest AIS scores and summarises a patient's injury. A score of six in any region automatically translates to an ISS of 75, the maximum score. 2 Studies have shown the ISS to predict mortality and morbidity accurately in trauma patients.5,6
However, the ISS is criticised for two main reasons. The first is that it does not weigh the injury peculiarity when assigning codes. For example, a unilateral flail chest with three or more fractured ribs and a type C pelvic fracture has an AIS score of 4 each, even though the flail chest is a potentially more severe injury than the fracture. Hence, identical ISS scores in different patients might represent different prognoses. The second is that it underestimates the injury severity in a patient with multiple injuries in one region. For example, a patient with bilateral femoral fractures, skin abrasion and lip laceration will have scores for one of the fractures in the extremity region, skin abrasion in the external and lip laceration in the face region. However, femoral fractures are more severe injuries than the latter injuries.
Osler et al. 7 in 1997 proposed the New Injury Severity Score (NISS) to address the second deficiency of the ISS. The NISS sums the squares of the three injuries with the highest AIS scores, regardless of the region of the body affected.7,8 Many studies have compared the predictive accuracies of these two scoring systems using different outcome parameters in diverse populations. Such parameters include mortality, length of hospital stay, ICU admission and post-traumatic complications. The different populations compared include blunt vs penetrating injuries, paediatric vs adult patients, different age categories, and region-specific injuries such as orthopaedic and head injuries. Results are conflicting; while some found the NISS is better in some or all outcome parameters,7,9–11 others found no significant difference between the two systems.12–15 This study compared these scoring systems in a tertiary orthopaedic and trauma centre in Nigeria. The authors hypothesised that the NISS would be a more accurate outcome predictor than the ISS in patients with musculoskeletal trauma.
Patients and methods
This study was a retrospective cohort analysis conducted at a tertiary hospital in Nigeria. The hospital is the regional trauma and orthopaedic centre receiving referrals for orthopaedic and trauma cases from the South-East, South-South and parts of North-Central Nigeria. The hospital's trauma database from January 2019 to December 2019 was used for the study. All patients admitted to the trauma unit within the study period and who stayed longer than 24 h were recruited. The inclusion criteria are patients with only orthopaedic injuries. We excluded patients with abdominal, head, thoracic and urogenital injuries as those patients are promptly referred to another tertiary hospital specialising in managing such injuries. Our hospital handles only orthopaedic injuries, burns, and plastic surgical cases. We also excluded patients with missing information in any listed variable of interest. The hospital's review board approved the study (IRB/S/313/517/21).
Information collected from the records included the patient's gender, age, injuries, injury mechanism and injury description. Two authors coded the patients’ injuries according to the AIS manual. Also, other information collected included if patients underwent surgical intervention, multiple surgeries, and received a preoperative blood transfusion. The hospital length of stay and whether the patient was discharged or died were recorded. The outcome parameters studied were the need for surgical intervention, multiple surgeries, allogeneic preoperative blood transfusion, length of hospital stay and mortality.
The authors divided the patients into two; discrepant and non-discrepant. The discrepant subjects have different ISS and NISS scores (NISS scores were greater than ISS scores), while the non-discrepant patients have the same ISS and NISS scores. The mean hospital length of stay was compared between the two groups using the student's independent t-test. The association between the groups and the need for surgeries, multiple surgeries and preoperative blood transfusions was analysed using the chi-square test of independence since they are categorical variables. Multiple surgeries are operations requiring more than one theatre session to address the same injury or injuries resulting from the same traumatic impact.
A receiver operator characteristic (ROC) curve was generated for each outcome parameter to test the predictive accuracy of the two scoring systems. The areas under the curves (AUC) for the two ROC curves were compared for each parameter using the non-parametric method described by Hanley & McNeil in 1982. 16 An AUC of 0.5 is no better than a chance occurrence, while a higher AUC signifies increasing accuracy. An AUC greater than 0.9 is an excellent discriminator, 0.8–0.7 is good, 0.7–0.6 is a fair discriminator, and less than 0.6 is poor. 17 The hospital length of stay was dichotomised into short (less than 14 days) and long (longer than 14 days) duration to allow the ROC generation for this continuous outcome. The authors chose 14 days as most uncomplicated orthopaedic injuries are managed and discharged within this period. Age was also arbitrarily categorised into young adults (18–44 years), middle-aged adults (45–64 years) and older adults (>65 years). The authors hypothesised that patients with discrepant scores would have a longer hospital stay, require multiple surgeries, and need more blood transfusions. They also hypothesised that the discrepant group would have a higher mortality rate. All the statistical analysis was done with the IBM software statistical package for social sciences (IBM SPSS Armonk, NY: IBM Corp) version 26.
Results
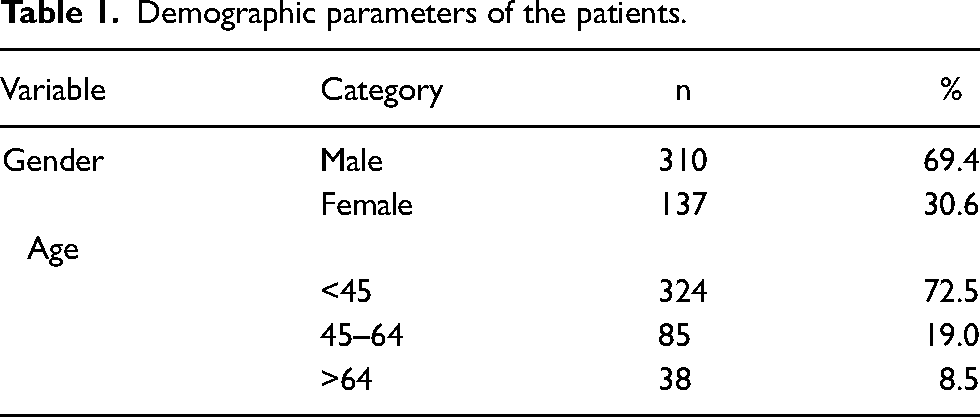
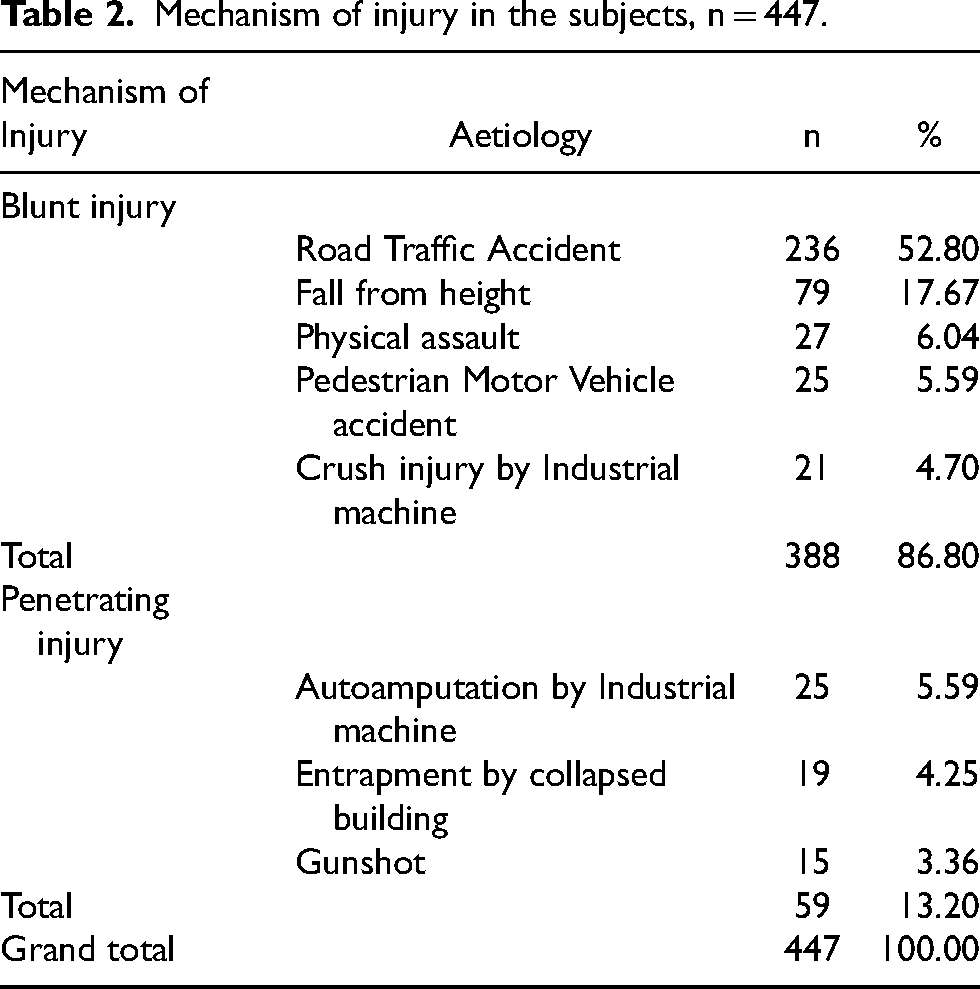
Five hundred and twenty-four patients presented to the hospital's trauma unit within the study period. However, 77 people were excluded for the reasons stated in the exclusion criteria, leaving a final sample size of 447 subjects with only musculoskeletal injuries. The patients’ average age was 34.78 years (SD = 18.67), with a range of one to 94 years, with most subjects younger than 45 years. There was no significant difference in the mean age of the discrepant and non-discrepant groups (35.90 vs 34.53 years, respectively, p = 0.550). Similarly, the Chi-square test of independence showed no significant association between gender and discrepant scores, p = .447. The proportion of males in the discrepant and non-discrepant groups was 65.9% and 70.1%, respectively, and 34.1% and 29.9% for females, respectively. Table 1 describes the study population, while Table 2 shows the mechanism of injury.
Demographic parameters of the patients.
Mechanism of injury in the subjects, n = 447.
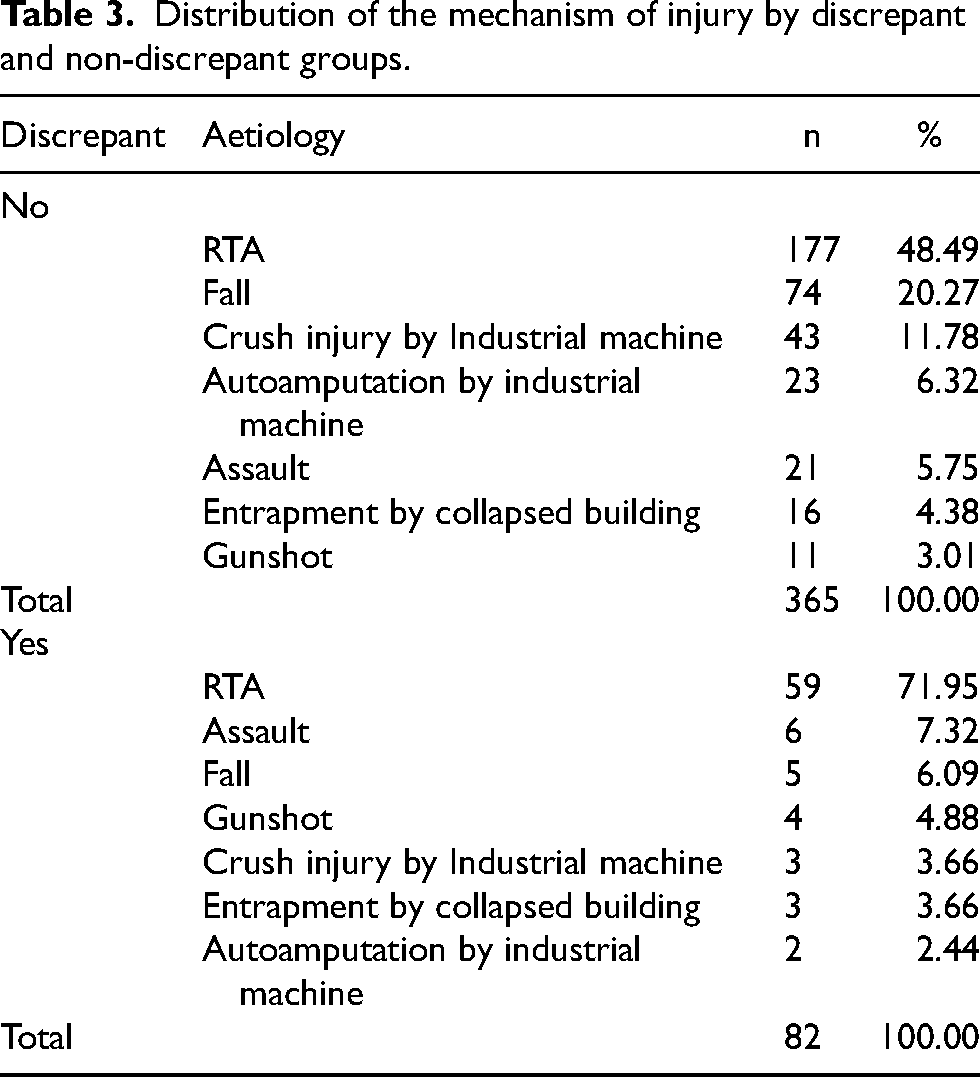
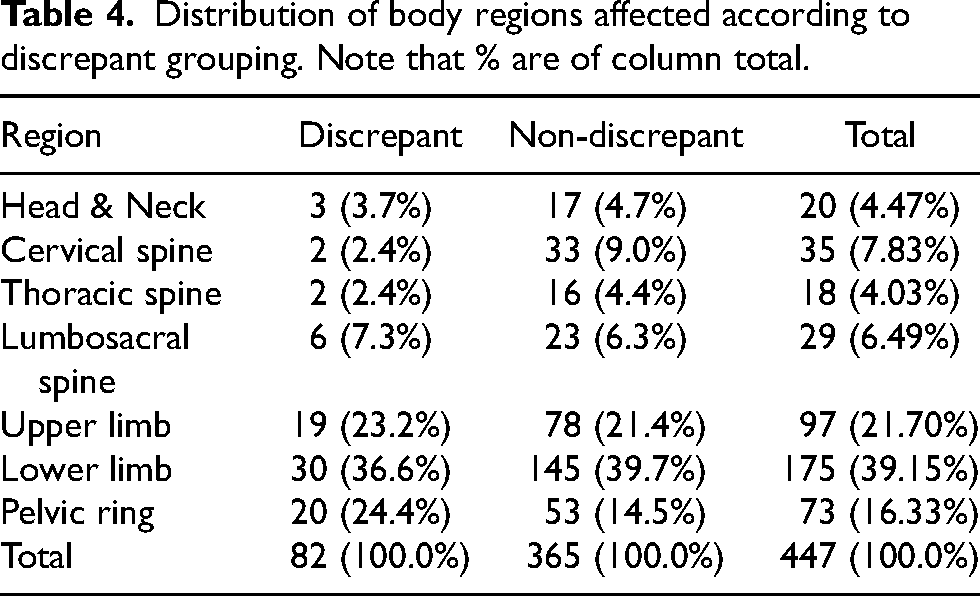
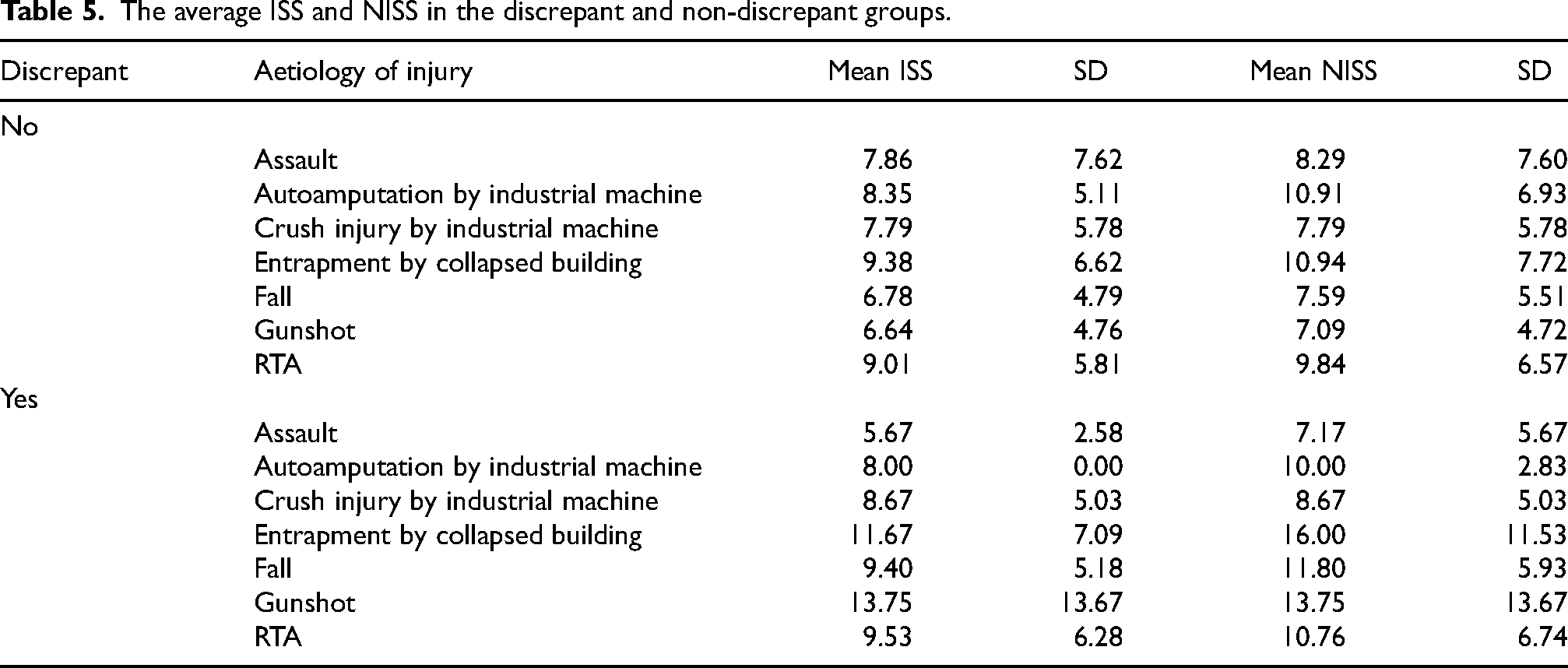
The mean ISS score for the study population was 8.5 (SD = 5.9), with a range of 4 to 34, while the average NISS was 9.4 (SD = 6.6), with the same range of 4 to 34. The NISS exceeded the ISS (discrepant) in 82 subjects (18.3%), while both scores were the same (non-discrepant) in 365 patients (81.7%). Table 3 shows the mechanism of injury by discrepant and non-discrepant groups, while Table 4 details the distribution of body regions affected in the subjects. A chi-square test of independence showed no significant difference in the mechanism of injury between the discrepant and non-discrepant groups, p = .713. Also, a chi-square test of independence showed that the body region affected did not significantly differ between the groups, p = .181. Sixty-nine subjects (15.4%) had an ISS greater than 15 (polytrauma), while the rest had a less severe trauma. Of the 69 polytraumatised patients, 18 (26.09%) belong to the discrepant group, while 51(73.91%) belong to the non-discrepant group. Table 5 shows the average ISS and NISS in the discrepant and non-discrepant groups, while Table 6 summarises the distribution of these outcomes in the study population.
Distribution of the mechanism of injury by discrepant and non-discrepant groups.
Distribution of body regions affected according to discrepant grouping. Note that % are of column total.
The average ISS and NISS in the discrepant and non-discrepant groups.
Distribution of the outcome parameters in the study population, n = 447.
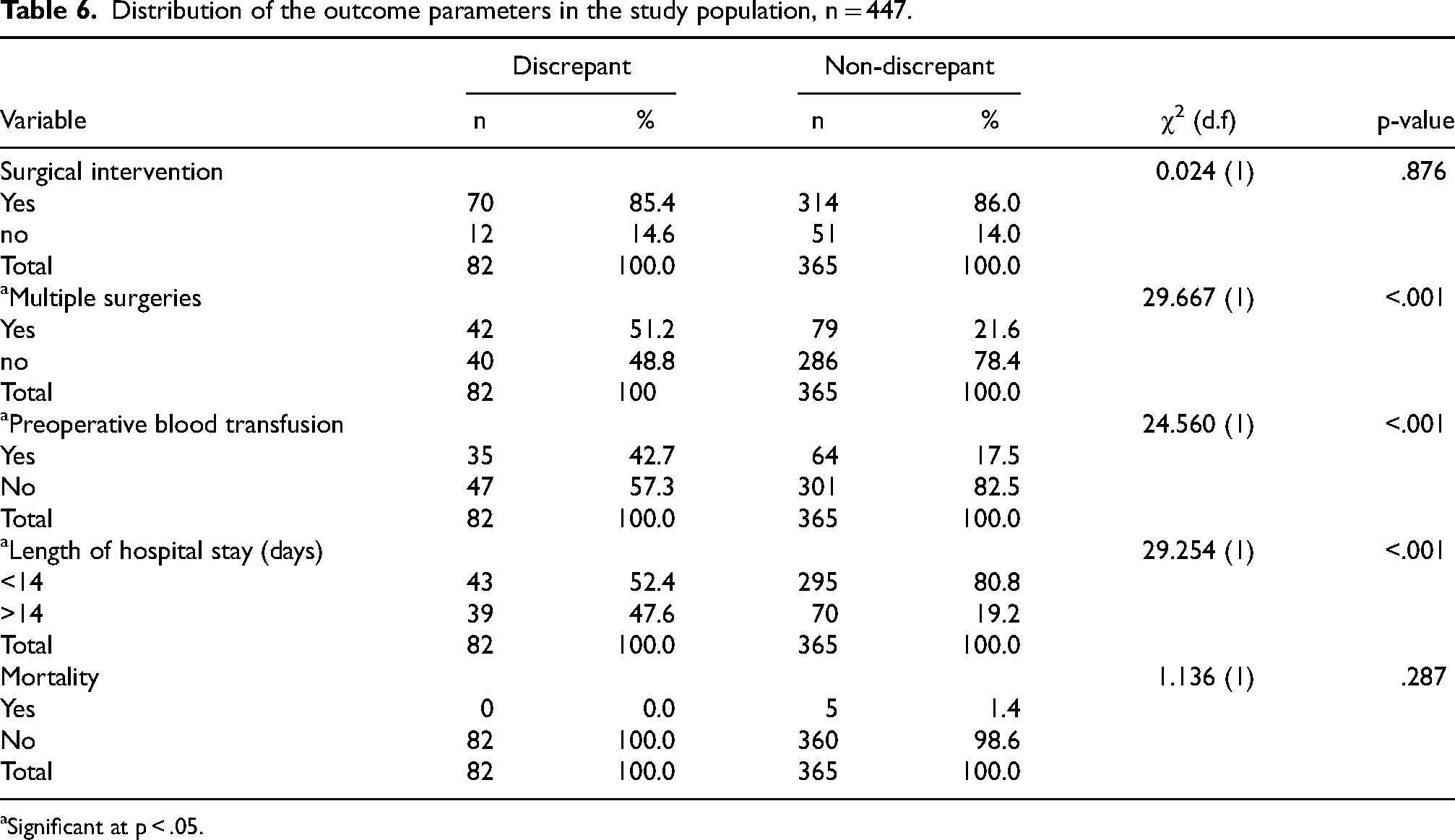
Significant at p < .05.
The ISS and NISS predicted the need for surgery with good discrimination, with AUCs of .75 and .72, respectively (Figure 1). There was no significant difference between the two AUCs (p = .153). However, the NISS predicts the need for multiple surgeries better than the ISS (p = .028), with AUCs of .89 and .87, respectively (Figure 2). Also, NISS may better predict the possibility of preoperative transfusion, although statistical significance is not achieved in this study (p = .099) and a longer hospital stay (p = .030). The AUCs for blood transfusion were .91 and .89 (Figure 3), respectively, for NISS and ISS, while the length of hospital stay was .85 and .83 for the NISS and ISS (Figure 4). In contrast, the ISS predicts the probability of survival better than the NISS (p = <.001). The AUCs for hospital discharge (survival) were .88 and .85 for the ISS and NISS, respectively (Figure 5).
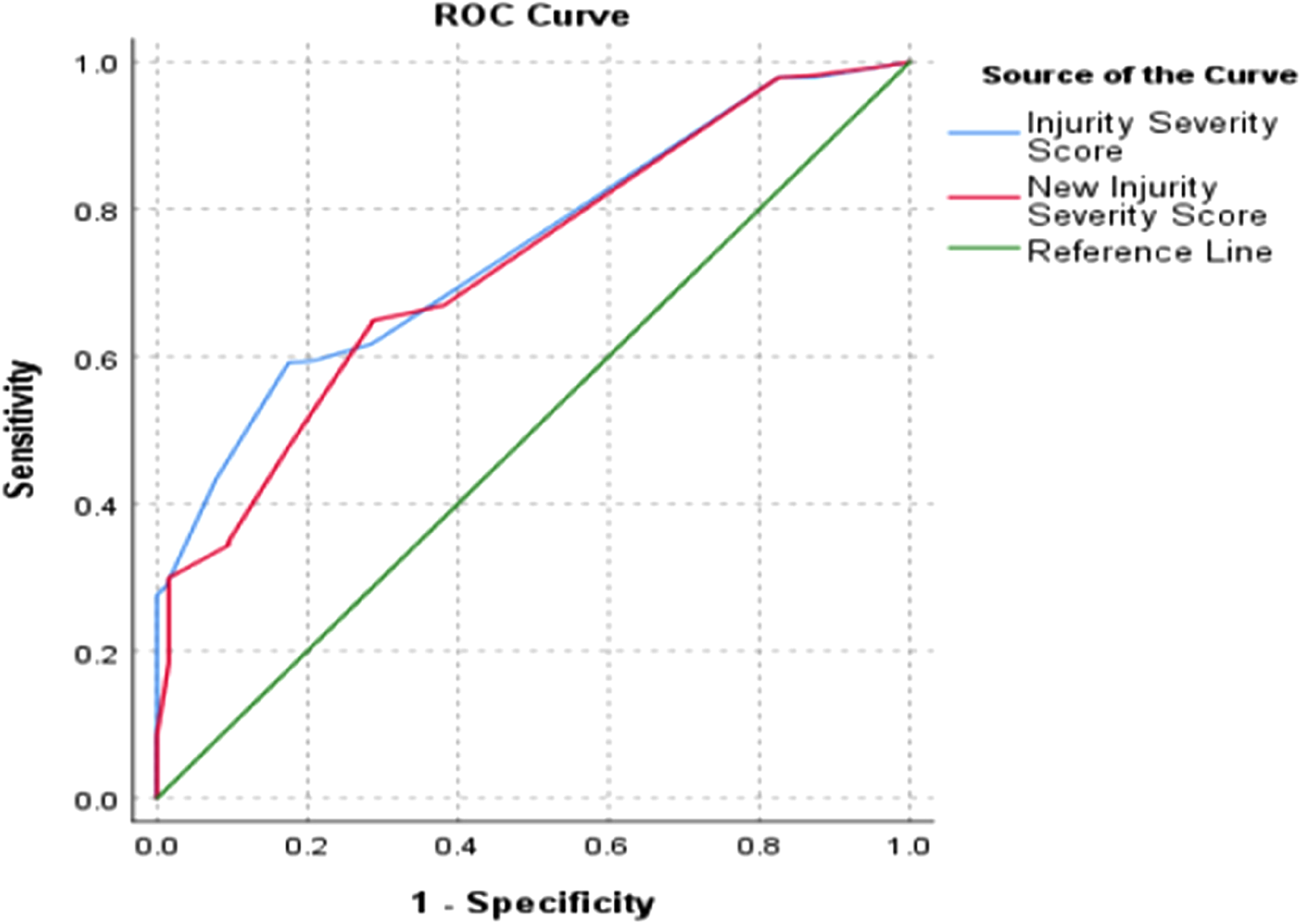
The ROC curves of the two scoring systems for the need for surgery. (ISS AUC = .75, NISS AUC = .72, p = .153).
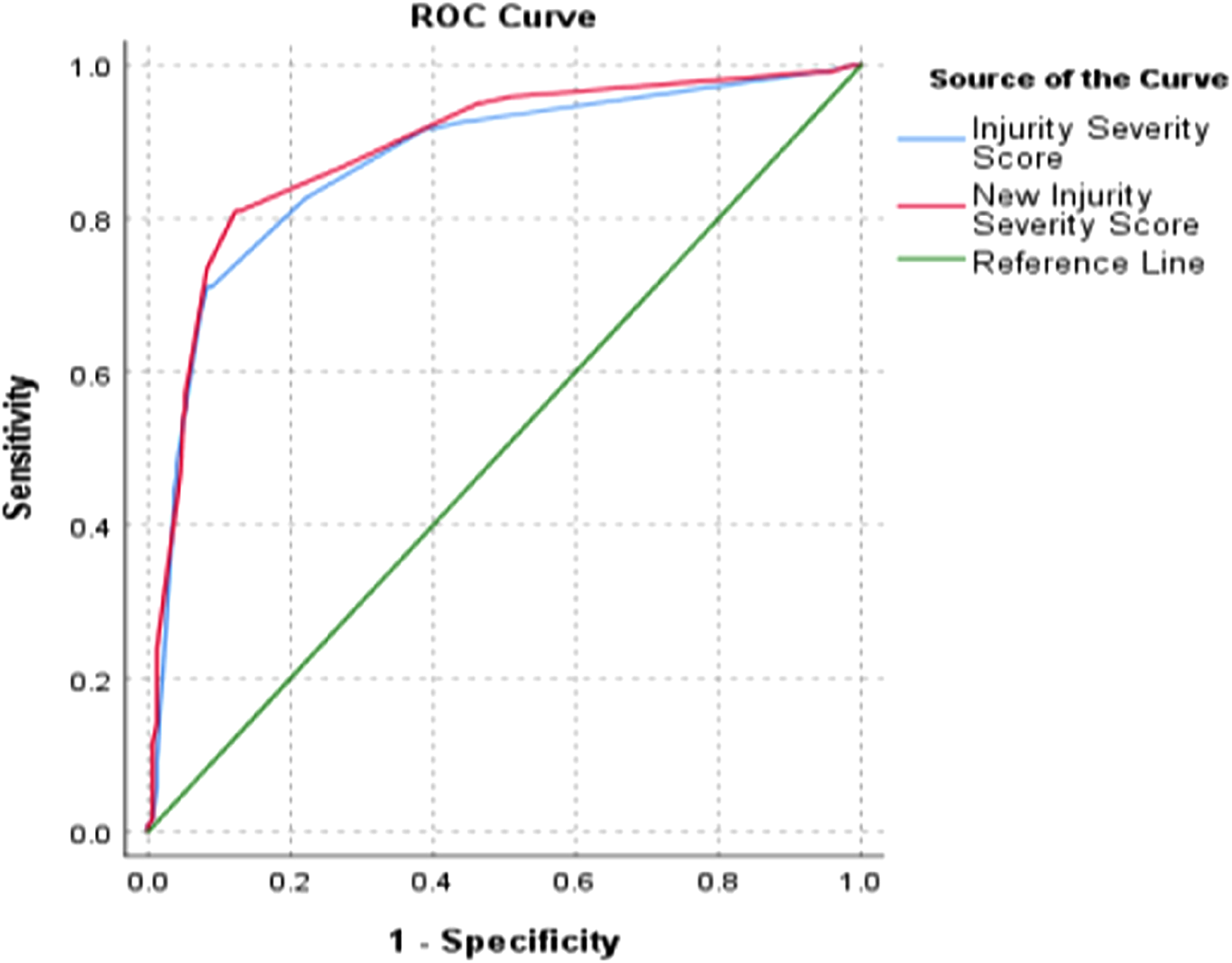
The ROC curves of the two scoring systems for the need for multiple surgeries. (ISS AUC = .87, NISS AUC = .89, p = .028).
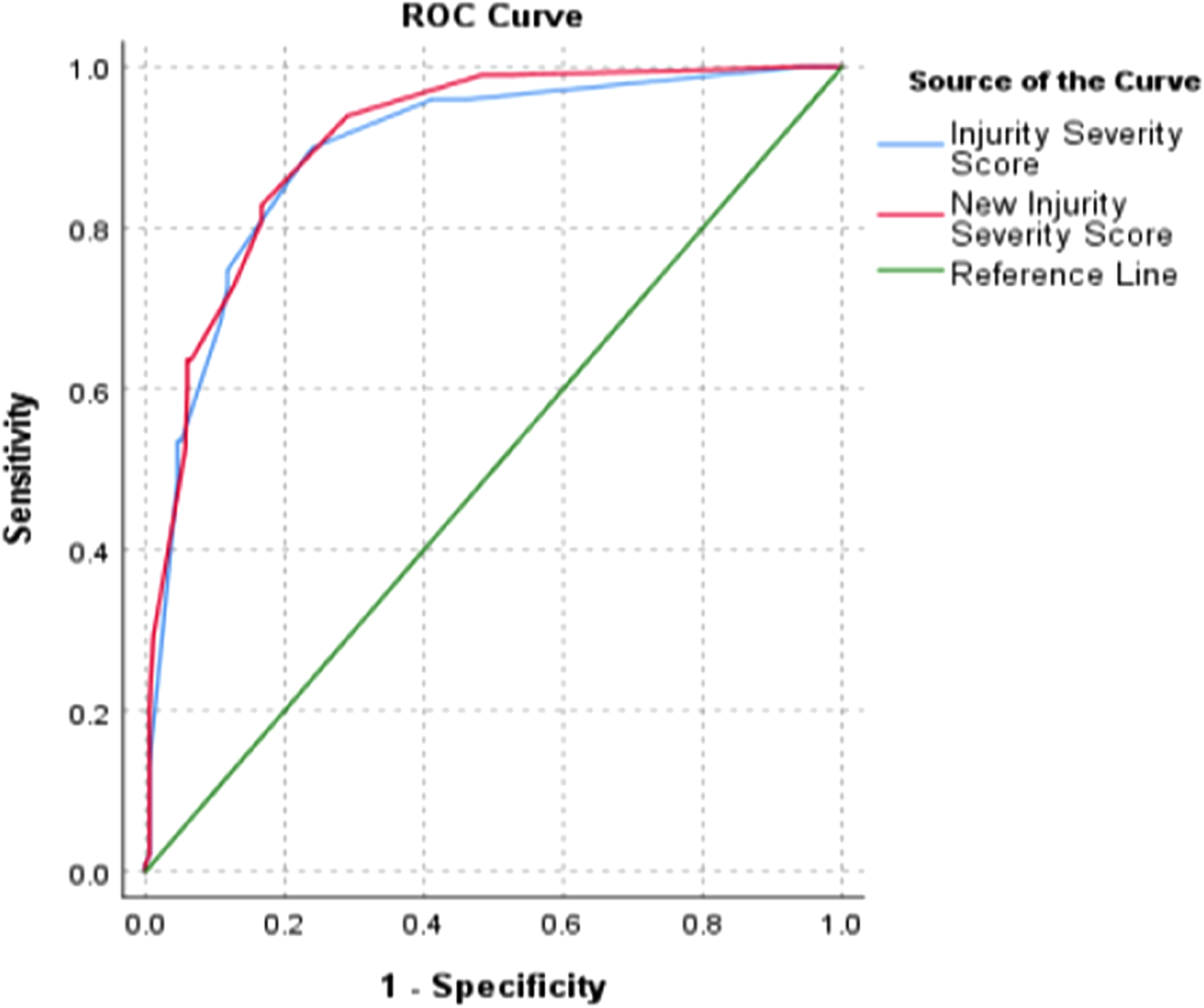
The ROC curves of the two scoring systems for the need for blood transfusion. (ISS AUC = .89, NISS AUC = .91, p = .099).
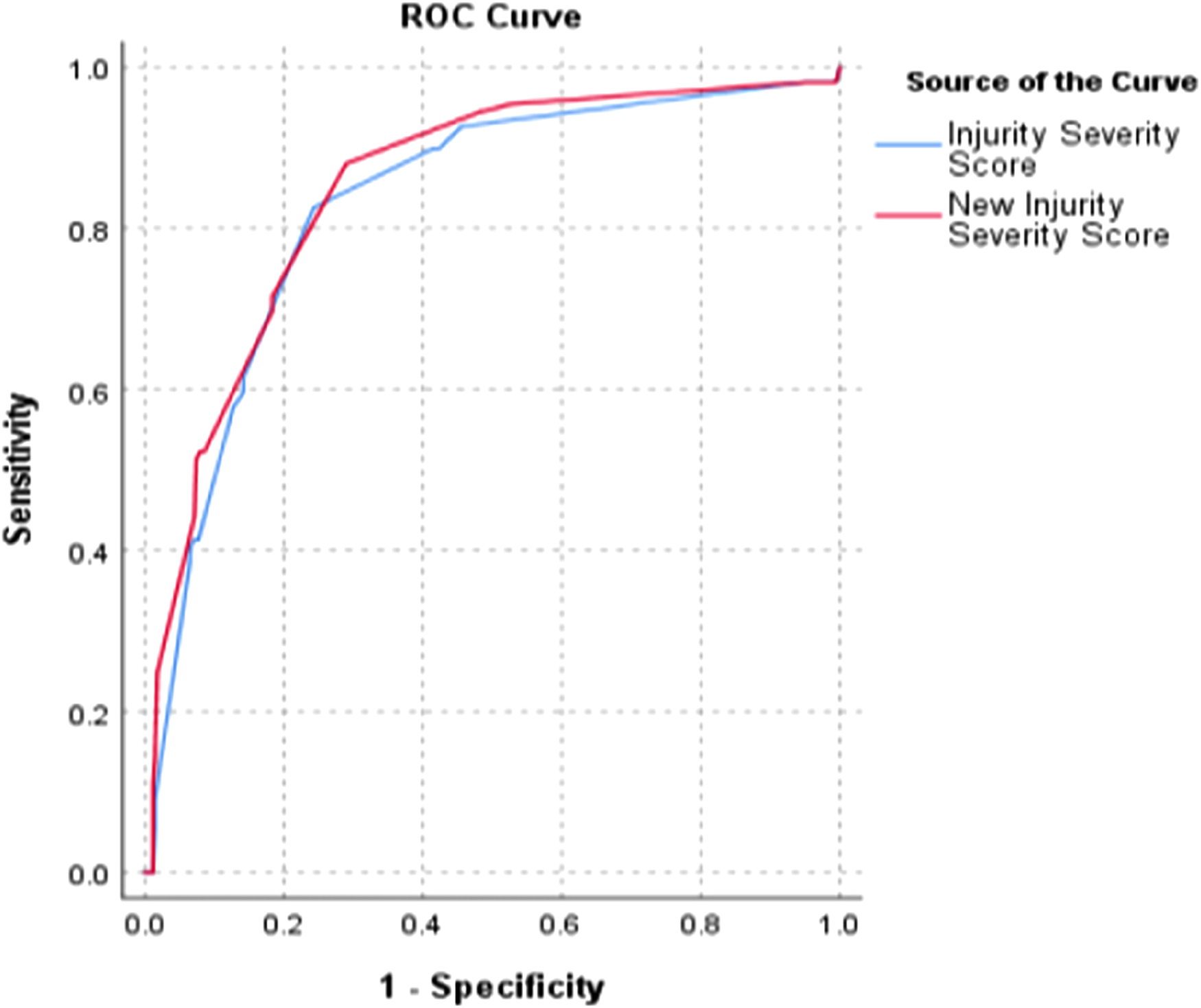
The ROC curves of the two scoring systems for the length of hospital stay. (ISS AUC = .83, NISS AUC = .85, p = .030).
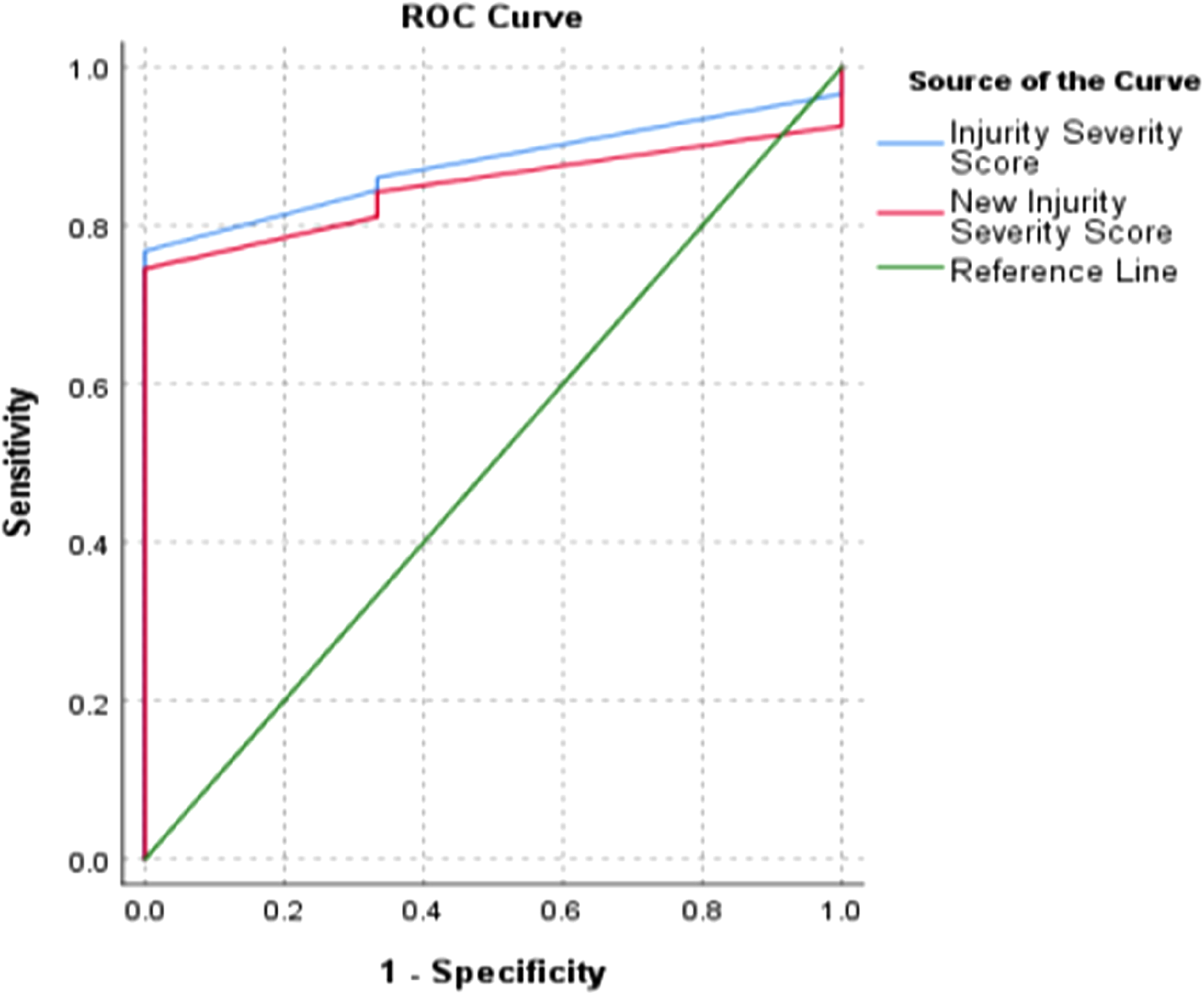
The ROC curves of the two scoring systems for predicting mortality. (ISS AUC = .88, NISS AUC = .85, p < .001).
Discussion
This study has found that both scoring systems perform similarly with no clear advantage over each other in all the outcome parameters studied. The NISS better predicts the need for multiple surgeries and hospital stay length, while the ISS better predicts the probability of survival. Both performed similarly on the other outcome parameters.
The ISS, NISS and other trauma scoring systems are classically used to predict mortality, length of hospital admission and the need for ICU admission after a traumatic event.8–15 This study introduced other important outcome variables that are indirectly associated with the severity of the injury. The need for surgical intervention likely indicates fractures or other injuries not amenable to conservative care. Multiple surgeries are likely in patients in extremis requiring damage control orthopaedics. At the same time, a preoperative blood transfusion might indicate two or more long bone fractures or an open-book pelvic injury with significant haemorrhage.
The ISS and NISS have similar abilities to classify trauma patients into those that will require surgery or not with a good classification score. Surgical intervention in musculoskeletal injuries implies significant trauma, especially in a developing country like ours, where the trend is towards a more conservative approach to fracture care as most patients are not insured and pay out-of-pocket. However, the NISS predicted patients requiring multiple surgeries better than the ISS.
Such patients usually have polytrauma and multiple fractures, making early total care inappropriate. 18 Patients requiring multiple surgeries had higher NISS scores than ISS cores (they were discrepant). Hence, such information should alert the surgeon to possibly a more seriously injured patient who may warrant damage control orthopaedics. A typical example would be a patient with a floating knee injury who sustained an ipsilateral femur and tibia fractures. The ISS will underestimate this injury, but the NISS would rightly capture the true nature of this severe orthopaedic condition.
Similarly, two scoring systems reliably classified blood transfusion in trauma patients. Traumatic blood loss requiring transfusion can lead to hypothermia, which with the resultant hypoxia and metabolic acidosis, sets up a vicious triad that increases mortality.18,19 Some authors have proposed specific transfusion prediction scores, such as the massive blood transfusion score and the traumatic bleeding severity score.19,20 These scores have not been compared to the ISS or NISS, but the latter scores have a good ability to classify trauma patients into those that will require blood transfusion or not. Future studies should build a regression model of these scores for predicting blood transfusion with a large sample size to establish which is more accurate.
Among the outcome parameters, multiple surgeries, preoperative blood transfusions, and hospitalisation duration differed significantly between the discrepant non-discrepant groups. While the three parameters were higher in the discrepant group, all mortality occurred in the non-discrepant group, although not statistically significant.
The NISS has a better classification rate for hospitalisation duration than the ISS. This finding agrees with Lavoie and colleagues, 8 who demonstrated that the NISS better predicts hospital stay length across all age categories of patients with head injuries. Also, Balogh et al. 21 found the NISS to predict hospitalisation duration better than ISS in a study of over 3000 trauma patients. Similarly, Harwood et al., 22 in a large prospective study of more than 10,000 patients with blunt orthopaedic injuries, concluded that NISS outperformed the ISS in predicting hospital stay length. In contrast, Tamim et al. 23 found that the ISS predicts hospital stay length better than the NISS, although the significance is lost when patients are stratified by age groups. However, the sample size was much smaller than the other studies that found a contrary result.
In terms of mortality or hospital discharge, there was no significant difference between the NISS and ISS. This finding agrees with Husum and Strada, 13 who found that both scoring systems have a similar predictive ability for mortality. Sullivan et al. 24 found that both scores perform similarly among paediatric trauma patients with less severe injuries, but that NISS outperforms ISS at higher injury severity. Stephenson et al., 15 in one of the largest studies involving more than 300,000 trauma patients for ten years, noted that the ISS slightly outperforms the NISS in predicting survival. However, several studies concluded that NISS is a better predictor of mortality than ISS.7–10 Osler et al. 7 proposed the NISS model and recommended replacing the ISS with it in grading injury severity.
Conclusion
Studies have not agreed on which scale is a better scoring system for predicting trauma-related mortality. However, the NISS better predicts the need for multiple surgeries and hospital stay length, while the ISS better predicts the mortality rate. Therefore, the authors found insufficient evidence to recommend replacing the ISS as an anatomic injury severity score with the NISS. However, since it uses the same parameters as the ISS and is easier to calculate than the ISS, it may be more practical to calculate in a busy trauma unit. These features could make it a more appealing scoring system than the ISS in trauma patients with musculoskeletal injuries.
Limitations
The study's limitations include its retrospective design which predisposed it to many problems, such as excluding many patients because of missing data. Also, it has limited external validity to other non-orthopaedic injuries, as only patients with musculoskeletal injuries were included. Similarly, since this is a tertiary trauma centre with the required staffing and expertise readily available, it is doubtful if the results could be replicated in a lower-tier hospital with less experience.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.