
Abstract
Introduction:
The United States and the world are currently experiencing a tremendous growth in the elderly population. Moreover, individuals surpassing the ages of 80 and 90 are also continuing to increase. As this unique division of society expands, it is critical that the medical community best understands how to assess, diagnose, and treat this population. The purpose of this study was to analyze morbidity, mortality, and overall outcome of patients aged 90 years and older after orthopedic surgical fracture repair. Such knowledge will guide patients and their families in making decisions when surgery is required among nonagenarians.
Methods:
The trauma registry of our level I academic medical center was queried to identify potential study participants over the past decade. Two hundred and thirty-three surgical procedures among 227 patients were included and retrospectively assessed. Parameters of specific interest were injury type, mechanism of injury (including high energy vs low energy and height of falls), injury severity score, preoperative comorbidities, postoperative complications, length of hospital stay, discharge destination, and postoperative mortality rate.
Results:
Overall, 4.3% of the cohort died in the hospital following surgery. Of the patients who survived, 89.7% were discharged to a professionally supervised setting. The nonagenarian population displayed a considerable follow-up rate, as 82.8% of individuals returned for their first postoperative office visit.
Discussion:
Historically, surgical morbidity and mortality are highly associated with this age group. However, the number of nonagenarians in the United States is increasing, as are these surgical procedures. The epidemiologic and clinical findings of our study support this trend and add further insight into the matter.
Conclusion:
This investigation demonstrates that orthopedic surgery is an appropriate treatment in this population with an acceptable complication rate. Furthermore, nonagenarians have the potential to demonstrate a substantial follow-up rate, but postoperative discharge to a professionally supervised setting may be necessary.
Introduction
Over the past 30 years, the geriatric population in the United States has experienced a considerable increase in life expectancy. 1 According to Mather et al, by the year 2060, the number of Americans aged 65 and older is projected to more than double which is an approximate increase of 46 million to 98 million people. 2 Specifically, by 2050, it is predicted that there will be a 4-fold increase in adults aged 85 years and older. 3 Not only is this division of society expanding at a significant rate in the United States, but it is doing so internationally as well. 1
As the population ages, the incidence of patients experiencing fractures is expected to rise. 4 Lamb et al have specifically noted that the prevalence of “fragility fractures” is increasing (fragility fractures are defined as a fracture sustained from a standing height fall or less, or a fracture that presents without external evidence of trauma). 5 These low-energy events occur primarily in the geriatric population and are a good predictor of subsequent fractures later in life. As fracture occurrence increases with age for both males and females (the latter is especially prone 4 -8 ), this issue has the potential to become a staggering burden on the country’s health-care system. The creation of geriatric fracture treatment programs to address these and similar injuries has been shown to be beneficial. 5 However, further investigation is warranted to establish a standard of care that is reliable and can be adopted universally to alleviate these injuries efficiently and properly guide patients and their families in making a decision when surgery may be required.
To further assess orthopedic surgical fracture repair in this population and understand the associated outcomes, our institution’s trauma registry was queried to identify eligible study participants over the past 10 years. Parameters of specific interest included injury type, mechanism of injury and energy level of mechanism, injury severity score (ISS), pertinent preexisting conditions (including whether the patient was determined to have a functionally dependent health status and/or an advance directive limiting care on-file during their hospital stay), postoperative complications, length of hospital stay, discharge destination, follow-up rate, and postoperative mortality.
We hypothesized that orthopedic surgical fracture repair in nonagenarians is an appropriate treatment with acceptable complication rates. In an attempt to guide future statistical analysis in this population, we also explored factors outside advanced age that had an association with perioperative morbidity and mortality.
Methods
Institutional review board approval was obtained prior to initiation of the study. A retrospective chart review was conducted using the Trauma Registry at our level I trauma center. The authors identified all patients aged 90 and older who had a traumatic injury and as a result underwent orthopedic surgical fracture repair between January 2007 and March 2017. Two hundred and thirty three operative procedures performed on 227 patients with a mean age of 92.7 years (SD 2.6, range 90-103) were included in the investigation. Data parameters examined included the indications for surgery, injury type and body location, mechanism of injury and energy of mechanism, associated injuries, ISS, pertinent preexisting conditions (including whether the patient was determined to have a functionally dependent health status and/or an advance directive limiting care on-file during their hospital stay), postoperative complications, length of hospital stay, discharge destination, and postoperative mortality rate. Deceased patients either died during their postoperative hospital stay (as recorded by the Trauma Registry) or were confirmed dead by electronic medical record documentation after discharge. Available death certificates of these patients were reviewed in order to ascertain the cause of mortality.
To determine whether each patient was present at the first follow-up appointment, the orthopedic department’s billing system was used to confirm that the office visit in question occurred. At our institution, these appointments typically take place at 2 weeks following the procedure. Categorical and continuous data were analyzed using descriptive statistics and univariate analysis.
Results
The Trauma Registry identified a total of 1351 patients aged 90 or older who were admitted for a traumatic injury between January 2007 and March 2017. Of the total nonagenarian trauma population, 507 (37.5%) received an orthopedic consult with 233 (46%) further undergoing surgical correction. Among those patients meeting inclusion criteria, 47 (20.2%) of 233 were male and 186 (79.8%) of 233 were female.
Ten (4.3%) of the 233 died in the hospital postoperatively, 5 (2.1%) of 233 were discharged to hospice, and 5 (2.1%) of 233 were confirmed dead before follow-up (2 had been discharged to hospice). The death certificates and causes of in-hospital death could only be attained for 5 patients. The causes of death included acute respiratory failure, nondescript respiratory failure, hypotension secondary to sepsis, pneumonia, and cardiac arrest. Twenty-three (9.9%) patients were discharged to a home setting, where they were originally living prior to their injury. Of these 23 patients, 22 returned for their first follow-up appointment (1 was lost to follow-up).
Demographic information of the study cohort is illustrated in Table 1. The first column displays all nonagenarians. The second column displays the patients who died in the hospital postoperatively (n = 10), those who were discharged to hospice (n = 5), and those who were confirmed dead before their first follow-up appointment (n = 5). The complete group is only comprised of 18 patients though because 2 patients discharged to hospice were confirmed dead before follow-up. The third column represents the nonagenarians who were discharged to an independent-living/home setting following their procedure (n = 23).
Demographic Characteristics and Outcomes of Nonagenarians with Comparison of 2 Subpopulations (Home Discharge vs Hospice Discharge/Early Mortality).
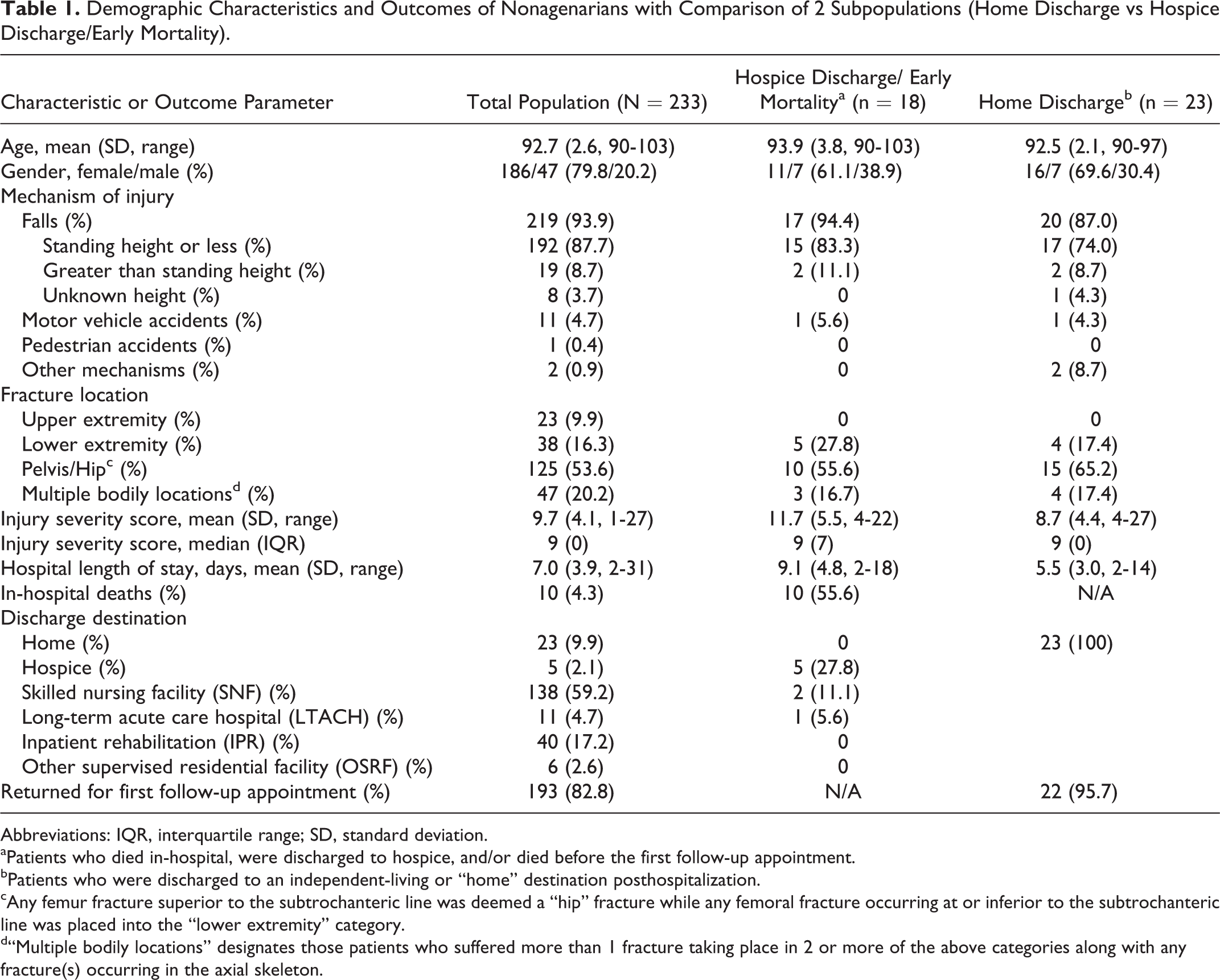
Abbreviations: IQR, interquartile range; SD, standard deviation.
aPatients who died in-hospital, were discharged to hospice, and/or died before the first follow-up appointment.
bPatients who were discharged to an independent-living or “home” destination posthospitalization.
cAny femur fracture superior to the subtrochanteric line was deemed a “hip” fracture while any femoral fracture occurring at or inferior to the subtrochanteric line was placed into the “lower extremity” category.
d“Multiple bodily locations” designates those patients who suffered more than 1 fracture taking place in 2 or more of the above categories along with any fracture(s) occurring in the axial skeleton.
Figure 1 shows the discharge disposition of all 233 patients in the study. It also elaborates on discharge destination specifically and presents the percentage of patients from each destination that returned for their first follow-up visit (at our institution, the first follow-up appointment took place approximately 2 weeks following the procedure). Twenty-five patients in the study had no record of returning to our clinic for follow-up. Without conclusive evidence of their follow-up disposition, these individuals were considered lost to follow-up. Overall, 82.8% of all patients were present at their first postoperative office appointment. Tables 2 and 3 display the prevalence of preexisting conditions at the time of surgery and the postoperative complications, respectively. The 3 most prevalent comorbidities among the entire population were hypertension (185/233, 79.4%), dementia (74/233, 31.8%), and thyroid disease (64/233, 27.5%). The 3 most prevalent comorbidities among the patients in the hospice discharge/early mortality group were hypertension (13/18, 72.2%), dementia (6/18, 33.3%), and coronary artery disease (5/18, 27.8%). The patients in the home discharge group resemble that of the entire population: hypertension (15/23, 65.2%), dementia (6/23, 26.1%), and thyroid disease (6/23, 26.1%).

Percentage of Patients by Discharge Disposition and Return for First Follow-Up Visits.
Prevalence of Pertinent Preexisting Conditions (PECs) among Nonagenarians.

Abbreviation: BMI, body mass index.
aPatients who died in-hospital, were discharged to hospice, and/or died before the first follow-up appointment.
bPatients who were discharged to an independent-living or “home” destination posthospitalization.
cPatients were determined to have a functionally dependent health status if before their injury, and as a result of cognitive or physical limitations relating to a preexisting medical condition, were partially dependent or completely dependent upon equipment, devices, or another person to complete some or all activities of daily living.
dPatients were deemed to have a mental/personality disorder if there was documentation in the medical record of diagnosis of preinjury depressive disorder, bipolar disorder, schizophrenia, borderline or antisocial personality disorder, and/or adjustment disorder/post-traumatic stress disorder.
Prevalence of In-Hospital Complications among Nonagenarians.

aPatients who died in-hospital, were discharged to hospice, and/or died before the first follow-up appointment.
bPatients who were discharged to an independent-living or “home” destination posthospitalization.
cThis row denotes the nonagenarians who were not noted to have any of the above complications following their procedure. It does not exclude the possibility of other postoperative occurrences which were not documented by our trauma registry.
Perhaps because of early death postoperatively, some members of the hospice discharge/early mortality group have no record of postoperative complications in-hospital. However, this group still collectively displayed several complications including cardiopulmonary arrest not resulting in death; deep vein thrombosis; gastrointestinal bleeding; iatrogenic damage to an organ, vessel, or nerve; iatrogenic pneumothorax; myocardial infarction; pulmonary embolism; stroke/cerebrovascular accident; unplanned admission to an intensive care unit; unplanned return to the operating room; and urinary tract infection not present upon admission.
Discussion
The elderly demographic is undergoing a tremendous expansion. 1 -3 In the United States alone, this population is predicted to grow between 2 to 4 times in size by 2060 with a considerable portion of those individuals being 80 and older. 1 -3 Orthopedic surgeons must pay particular attention to fracture occurrence among the elderly individuals as it is also rising at a significant rate. 4,5 This trend is most likely attributable to several reasons, although prior literature has stated that the rate will increase solely as a function of the surge in the elderly population (a demographic inherently more at risk for these injuries 4 ). Little work has been done solely assessing nonagenarian outcomes and complications following orthopedic surgical fracture repair, and although postoperative complications and mortality are noted to be higher among older individuals 9 -15 , we conducted this investigation to highlight potential factors that may contribute to this trend in a large nonagenarian cohort.
Epidemiologically, these data highlight 2 points that are consistent with current literature. The first is the large number of female patients (186/233, 79.8%) compared to males (47/233, 20.2%). This disparity is consistent with the work of several articles and reports. 7,8,16 Not only do females have a longer average life expectancy but within the US geriatric population they currently far outnumber males. 7,8,16 To compound the issue further, studies by Amin et al and Burge et al have stated that females are at an increased risk of fractures compared to males of the same age due to their higher incidence of osteoporosis. 4,6 Secondly, our study revealed that between 2007 and 2011, only 87 (37.3%) of the 233 procedures were performed, while 142 (60.9%) of the 233 procedures were done more recently from 2012 to 2016. January 2017 to March 2017 contained the remainder of the operations. This again agrees with prior literature 4 ; it appears that fracture incidence and/or operative treatment in this population is increasing with time.
One of the most definitive results of this study was how many injuries occurred because of falls (93.6%). One hundred and ninety-eight (85%) of the 218 total falls were from standing height or less. For all 18 patients who were discharged to hospice or suffered early mortality, there were 10 hip fractures, 5 lower extremity fractures, and 3 patients with fractures in multiple locations. Furthermore, of these 18 patients, 15 (83.3%) originally sustained falls from standing height or less. Per Lamb et al, fractures occurring as a result of this mechanism are considered “fragility fractures.” These injuries pose a serious threat to elderly individuals and are reliable indications of future fractures later in life. 5 These data further emphasize the potential benefit of fall prevention programs and treatment of osteoporosis.
In our investigation, there is little difference in the presence of preexisting conditions between the patients who were discharged home and those who were discharged to hospice or died shortly after surgery. However, having an advanced directive limiting care and ISS did stand out among the other parameters. The hospice discharge/early mortality group had 5 patients with advanced directives limiting care on file during their hospital stay compared to 2 advanced directives on file for patients discharged home. There have been multiple studies suggesting a prominent link between patients with a do-not-resuscitate (DNR) advanced directive and increased morbidity and mortality following surgery. 17 -19 Some authors have even inferred that the presence of a patient’s DNR advanced directive has a stronger correlation with postoperative mortality than does their age. 17 The mean ISS of the hospice discharge/early mortality group was 11.7 with a range of 4 to 22 compared to that of 8.7 (range of 4-27) for those patients discharged home. While these 2 subpopulations had an equivalent median ISS value of 9, the hospice discharge/early mortality group had a larger interquartile range (IQR) associated with the median, suggesting a larger spread toward higher scores. Although newer methods of injury scoring are being incorporated into trauma care, 20,21 the ISS has still been shown to accurately correlate with geriatric injury severity and mortality. 22 The results of our study also suggest that an increased ISS may still be a legitimate tool for predicting mortality among nonagenarians.
Perioperative morbidity and mortality are well established in older patients. 9 -15 In our study, urinary tract infection (3.9%), major dysrhythmia (3.4%), and pulmonary embolism (2.1%) were the most prevalent postoperative complications recorded by the trauma registry. Outside studies have also found that postoperative delirium is a common diagnosis among the elderly population following orthopedic surgery, specifically when preoperative dementia is present. 23,24 While our data did collect the frequency of preoperative dementia, postoperative delirium is not readily recorded by our medical center’s trauma database. Thus, the fact that delirium is not listed in Table 3 doesn’t rule out the possibility of its occurrence in our patients. The findings listed in Table 3 do suggest, however, that the use of surgical treatment on those of advanced age can be performed with acceptable outcome and complication rates. This is consistent with a study by Sieber and Barnett which found that among the elderly population, there are some practices that have reduced potential postsurgical complications with the use of quality measures and evidence-based strategies. 9
It is important to note that the majority (89.7%) of patients who survived their hospital stay were discharged to a professionally supervised setting. These included hospice, skilled nursing facilities, long-term acute care hospitals, rehabilitation centers, and other supervised residential facilities. Rehabilitation and return to ambulatory status have both been shown to improve mortality in the elderly following hip fractures. 15,25 Similar findings have been noted utilizing in-home rehabilitation programs with elderly patients who had proximal femur fractures. 26 In general, improving early functional status either before discharge or immediately afterward can decrease this population’s mortality rate following orthopedic surgical fracture repair. 15,25 -28 In our investigation, 85.1% of individuals discharged to a professionally supervised setting returned for follow-up (at our institution, the first follow-up appointment took place approximately 2 weeks following the procedure). These observations propose that nonagenarians may exhibit a high rate of discharge to professionally supervised settings following orthopedic surgical fracture repair. Medical professionals and patients’ families should prepare for this possibility when considering orthopedic surgical intervention in patients of this age group and understand the important role that proper rehabilitation may play in their recovery.
Limitations
The authors acknowledge that certain limitations are present. Retrospective study design and limited follow-up period are legitimate in this regard. Prospective studies are preferable in this type of investigation to attain uniformity across all parameters. Furthermore, longer average follow-up times may provide a clearer clinical picture of the overall functional outcome of these patients following fracture repair as well as a more accurate assessment of mortality. Finally, although there was a lack of powerful statistical analysis in this study, the investigation represents a diligent effort to assess a specific problem among nonagenarians without comparing them to a control group per the nature of our study design. This preliminary report serves to further understand a novel topic.
Conclusion
Orthopedic fractures are a growing issue among the elderly population. This investigation shows that orthopedic surgical fracture repair can be conducted on nonagenarians with an acceptable complication rate. Furthermore, this population has the potential to demonstrate a substantial follow-up rate, but postoperative discharge to a professionally supervised setting is usually necessary.
Footnotes
Authors’ Note
This data was presented at the New England Orthopedic Society’s Annual 2017 Fall Meeting, at the Massachusetts Medical Society, in Waltham, MA on 18 Nov 2017. This study has not been published elsewhere nor is it being considered for publication at any other entity.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.