
Abstract
Keywords
Introduction
Low back pain (LBP) has been reported to be a common musculoskeletal disorder with its underlying pathophysiology still not very clear. 1 The etiology of LBP is usually multifactorial ranging from degenerative changes, spinal stenosis, neoplasm, infection, trauma, and inflammatory or arthritic processes. 2 In an effort to better understand the etiology and pathogenesis of LBP, studies have focused on the intervertebral disc, facet joints, and vertebral end plates as potential sources of pain.3–5 Intervertebral disc diseases are among the leading cause of LBP. Various disc parameters and their correlation with LBP have been evaluated in the past and the outcome of these studies is still not able to shed light on the definitive association.6–14 Studies evaluating the etiology of low back pain have shown poor correlation between the MR imaging findings and LBP symptoms. There is still a lot to understand the disc structure and its association with LBP. Dural sac and nerve roots are in a direct anatomical relationship with the intervertebral disc. 15 Any change in disc morphology (herniation, degeneration, and content) is going to affect these vital neural structures and alter the normal biomechanics of the spine and thus may lead to LBP. 16 The objectives of the current study were (a) to evaluate the lumbar disc parameters (height, length, volume, and cross-sectional area) and their association with the development of LBP and (b) to find out whether these discs in LBP patients differ quantitatively in structure from the discs in healthy individuals.
Materials and methods
This prospective case–control study was conducted at a tertiary care center in the Department of Orthopaedics in collaboration with Department of Radiodiagnosis in Indian Population from March 2017 to March 2018. Fifty patients of either sex aged between 18 and 50 years with low back pain for a minimum 3 consecutive months duration and who give consent to participate in the study were enrolled as the study group (group A). Patients with gross deformity of spine such as scoliosis or spondylolisthesis, facet joint syndrome, sacroiliac joint dysfunction, fracture of spine, tumors and infections of spine, and history of hip or pelvic disorder were excluded from the study. Twenty-five healthy volunteers with no persistent LBP > 3 months and a history of medical attention for LBP and consenting to participate in the project were also enrolled randomly as the control group (group B).
Sample size was determined using the estimates of mean and standard deviation values from literature
17
using the formula
Approximate estimates:
80% power Type I error to be 5% Type II error to be 20% Population variance is assumed to be 5.25 MOE (margin of error) assumed as 1.5
Substituting the values,
Approximately 47–50 subjects/patients should complete the study at the endpoint follow-up.
Each patient and control participants were thoroughly examined clinically and were subjected to MRI. MRI was done free of cost in controls in the institution. MRI was done on 1.5 T machine (Phillips Intera) with patient lying supine comfortably with knees and hips extended. Multislice sagittal and transverse sections were taken with following MRI sequence:
T1 W Images:
Sagittal section Axial section TE – 8 TE – 8.5 TR – 400–600 TR – 500–600 Sagittal section Axial section TE – 100 TE – 115 TR – 3000–4000 TR – 2000–3000
T2 W Images:
A pilot parasagittal section on the MRI was used to define the vertebral levels. Measurement was done by using on-screen calipers using free open-source measurement software OsiriX (version 5.1.2, Pixmeo, Geneva, Switzerland) downloaded from http://www.osirix-viewer.com/.
18
Following parameters were measured at intervertebral disc level on each sagittal T2-image of MRI (Figures 1 and 2)
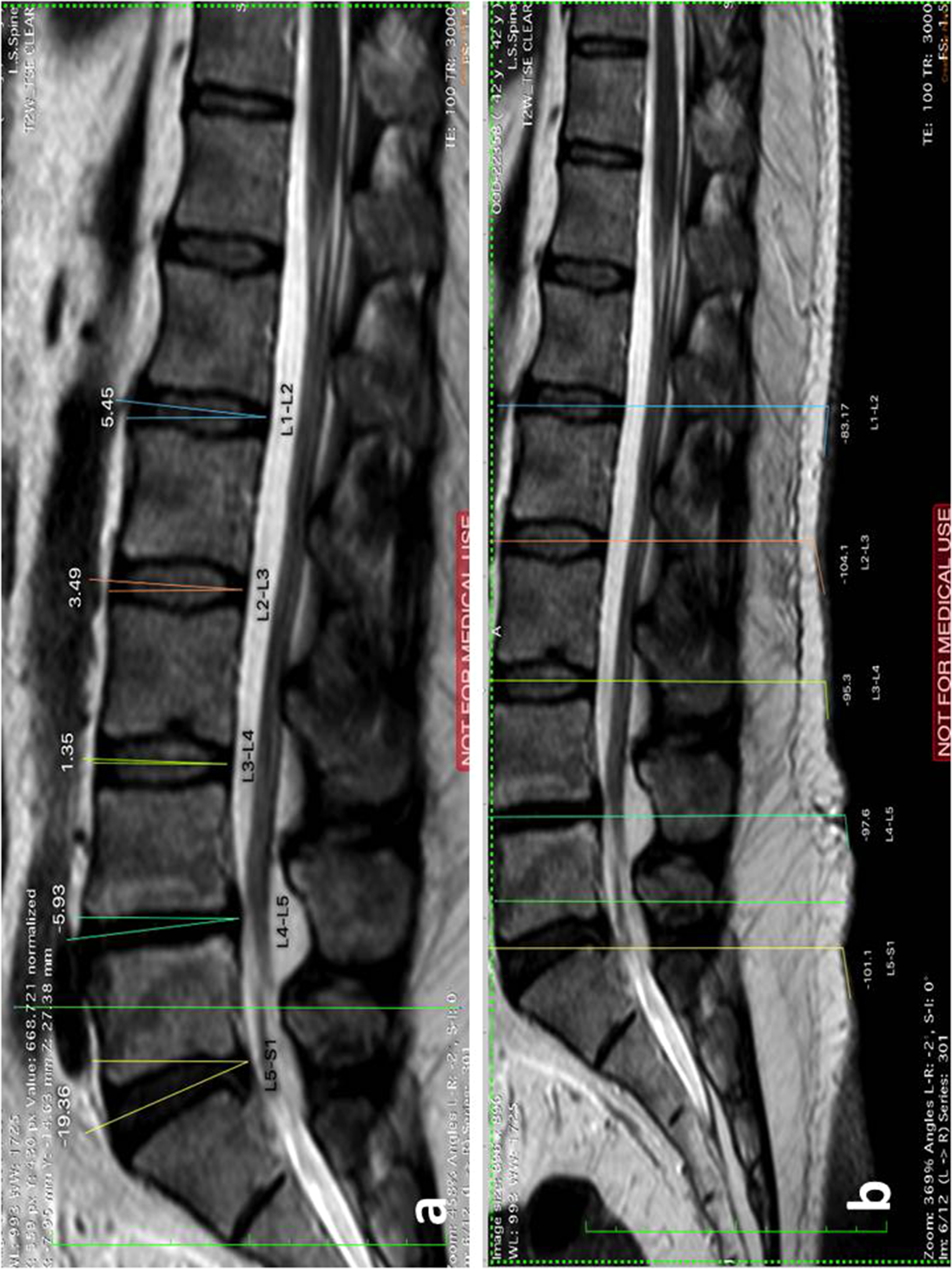
Measurement of the orientation of disc in vertebral column: disc angle (a) and skin angle (b) at each lumbar intervertebral disc level in a patient with L4-L5 disc herniation.
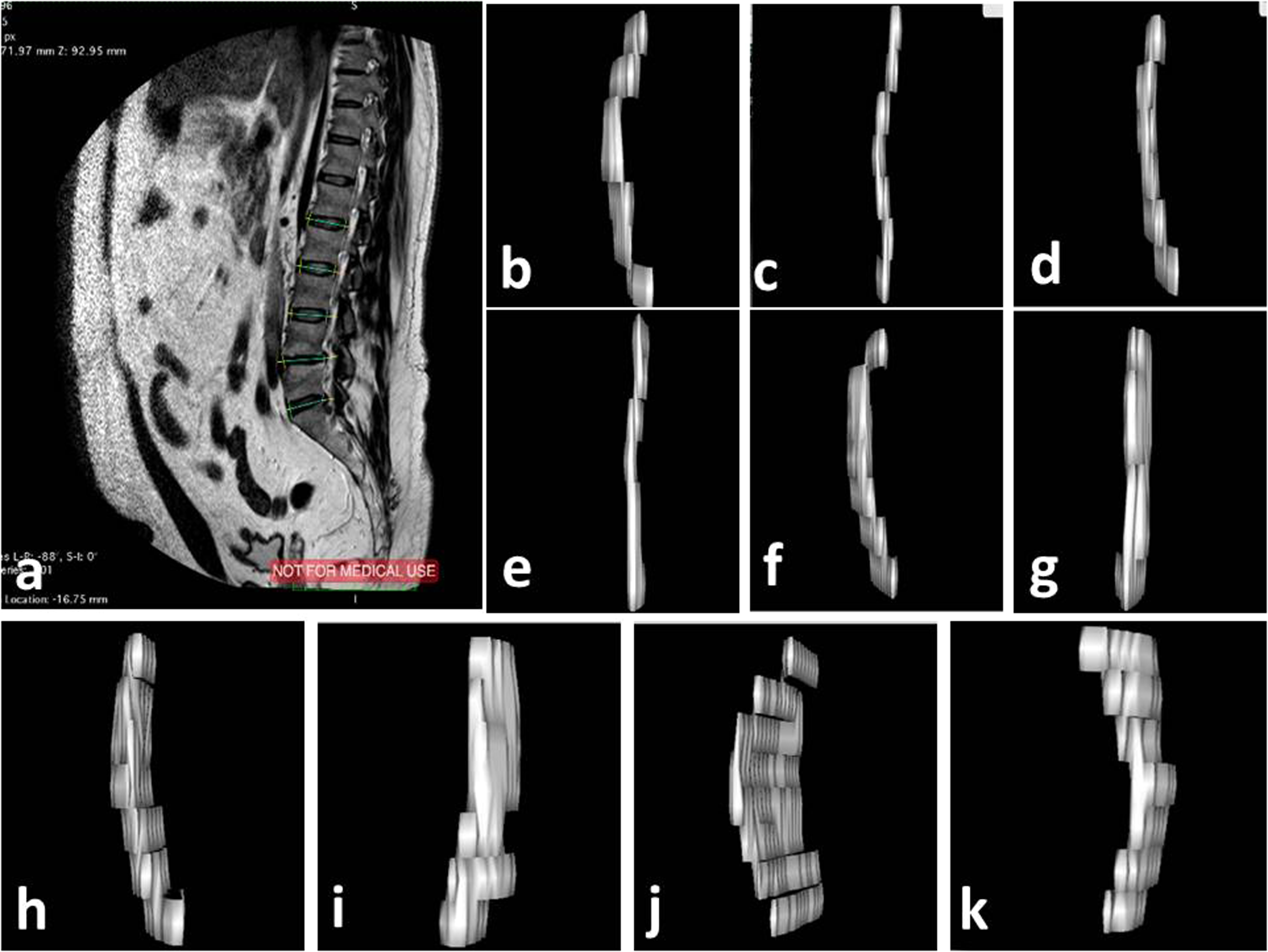
Measurement of disc parameters of anterior intervertebral height, posterior intervertebral height, anterior disc material, intervertebral disc, posterior disc material, and dural sac (a); (b) volume of anterior disc material (VADM) and (c) volume of posterior disc material (VPDM) at L1-L2 level; (d) VADM and (e) VPDM at L2-L3 level; (f) VADM and (g) VPDM at L3-L4 level; (h) VADM and (i) VPDM at L4-L5 level; (j) VADM and (k) VPDM at L5-S1 level on sagittal T2-image of MRI in the same patient.
Dural sac length (DSL)
Cross-sectional area of dural sac (CDS) [Dural sac area]
Method used to calculate disc angle and skin angle had been described by Tracy et al. 19 Method used to calculate the disc and dural sac parameters had been described by Tunset et al. 17 and it had shown good intra- and inter-rater agreement as well as reliability.
The average disc height in the current study was calculated using the formula as described by Dabbs and Dabbs 20 (anterior intervertebral height + posterior intervertebral height)/2. The association between the dural sac area, average disc height, and cross-sectional area of disc (CIVD) was evaluated taking dural sac area as dependent variable and disc height and CIVD as an independent variable for univariate linear regression analyses. We presented the results from the regression analyses as beta coefficients with 95% CI and taking p-values of 0.05 or less as statistically significant.
Statistical analysis
All the measurements and data were analyzed using standard statistical tools. The measurements were entered in Microsoft excel spreadsheet. Statistical analysis was performed using the statistical software IBM SPSS for Windows ver. 25.0 (IBM Corp., Armonk, NY, USA). 21 Normally distributed variables were mentioned as means and standard deviation. For normally distributed data, t-test was employed for analysis. Mann–Whitney and Chi-square test was employed for categorical and ordinal data. Correlation between variables was assessed by Pearson's coefficient of correlation. Interobserver agreement of values between variables was assessed by kappa value (Cohen–Kappa).
Results
Both the groups were comparable demographically (p-value > 0.05). In group A, mean age, height, weight, and BMI were 36.24 ± 9.07 years, 1.65 ± 0.060 m, 68.04 ± 10.93 kg, 24.94 ± 3.2 kg/m2, respectively. In group B, mean age, height, weight, and BMI were 35.57 ± 8.87 years, 1.66 ± 0.069 m, 70.48 ± 9.39 kg, 24.60 ± 2.26 kg/m2, respectively. There was no significant difference with regard to age (p = 0.267), sex (p = 0.41), professions/occupation (p = 0.98), and BMI (p = 0.643). Table 1 shows the occupation-based comparison between two groups. 42% (n = 21) were smokers in group A and 36% (n = 9) were smokers in group B.
Occupation-based comparison between two groups.
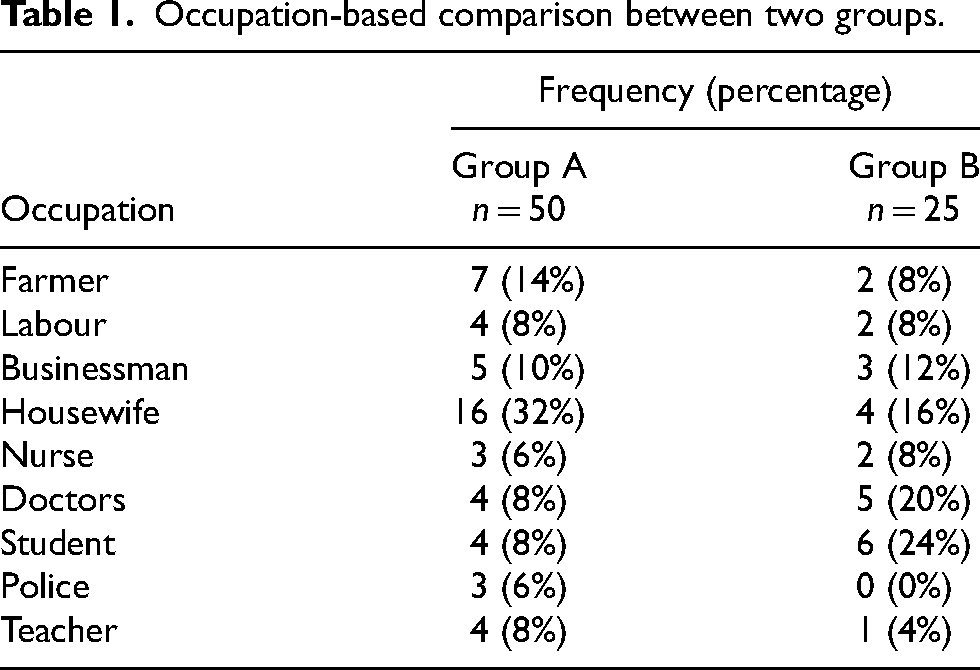
Table 2 shows comparison of disc angle and skin angle between study and control population. Statistically significant difference between the groups was present with regard to disc angle at L1-L2 (p = 0.01), L2-L3 (p = 0.05), and L3-L4 (p = 0.001) and skin angle at L2-L3 (p = 0.03) and L4-L5 (p = 0.05) levels. The disc angles were larger in group A and decreasing trend was seen from L1-L2 to L5-S1. Discs were more cranially angulated compared to group B.
MRI measurements and comparison of disc angle and skin angle at L1-L2, L2-L3, L3-L4, L4-L5, and L5-S1 disc level between group A and group B.
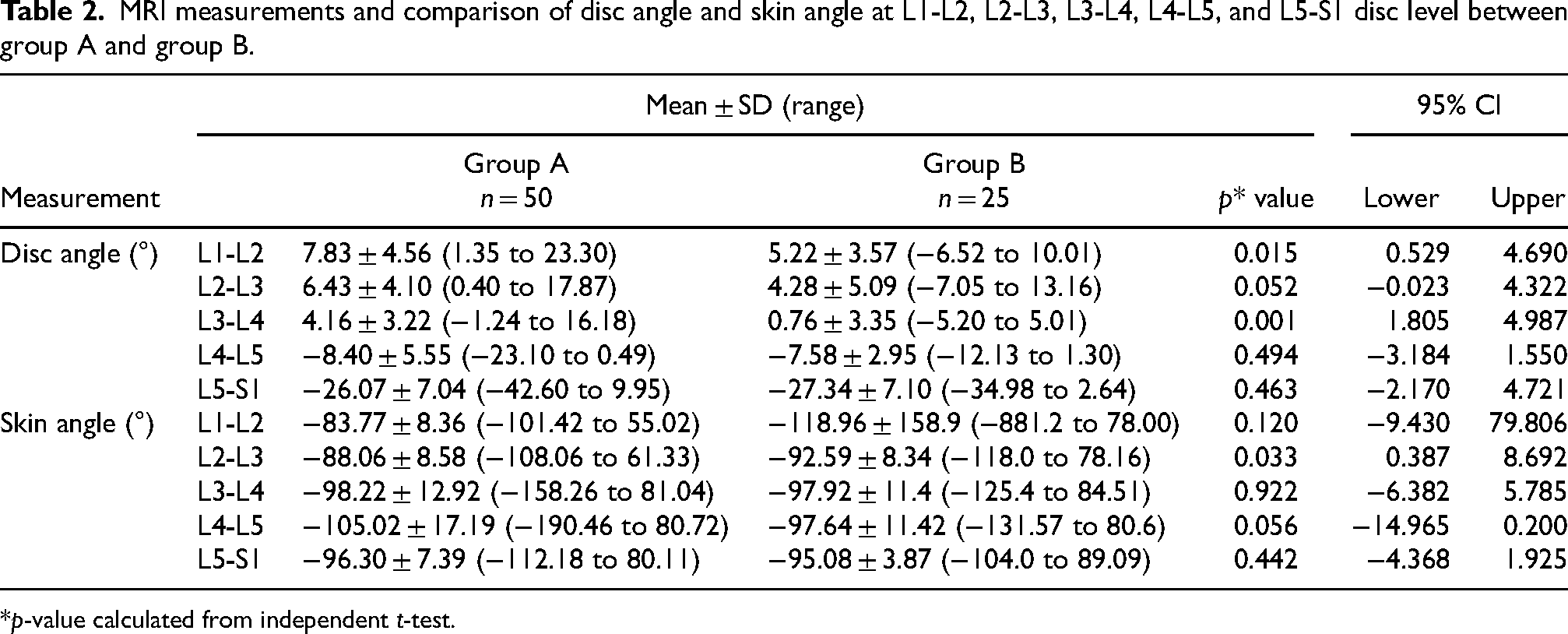
*p-value calculated from independent t-test.
Table 3 shows comparison of anterior intervertebral height (AIVH), posterior intervertebral height (PIVH), intervertebral disc length (IVDL), anterior disc material length (ADML), posterior disc material length (PDML), and antero-posterior dural sac length (ADSL) between study and control population. AIVH and PIVH were comparable except with regard to AIVH at L2-L3 (p = 0.05) and L5-S1 (p = 0.05) level, PIVH at L1-L2 (p = 0.03), and L5-S1 (p = 0.002) levels where it was statistically significant higher in group A. IVDL and ADML were also comparable (p > 0.05), except a significant difference with regard to IVDL at L4-L5 level (p = 0.03), ADML at L3-L4 (p = 0.002) and L5-S1 level (p = 0.001). PDML showed significant difference between group A and group B except at L3-L4 and L5-S1, where it was non-significant (p > 0.05). ADSL was significantly different between two groups at lower lumbar levels, that is, L3-L4 (p = 0.01), L4-L5 (p = 0.001), and L5-S1 level (p = 0.001).
MRI measurements and comparison of disc parameters (height and length) and anterior dural sac length at L1-L2, L2-L3, L3-L4, L4-L5, and L5-S1 disc level between group A and group B.
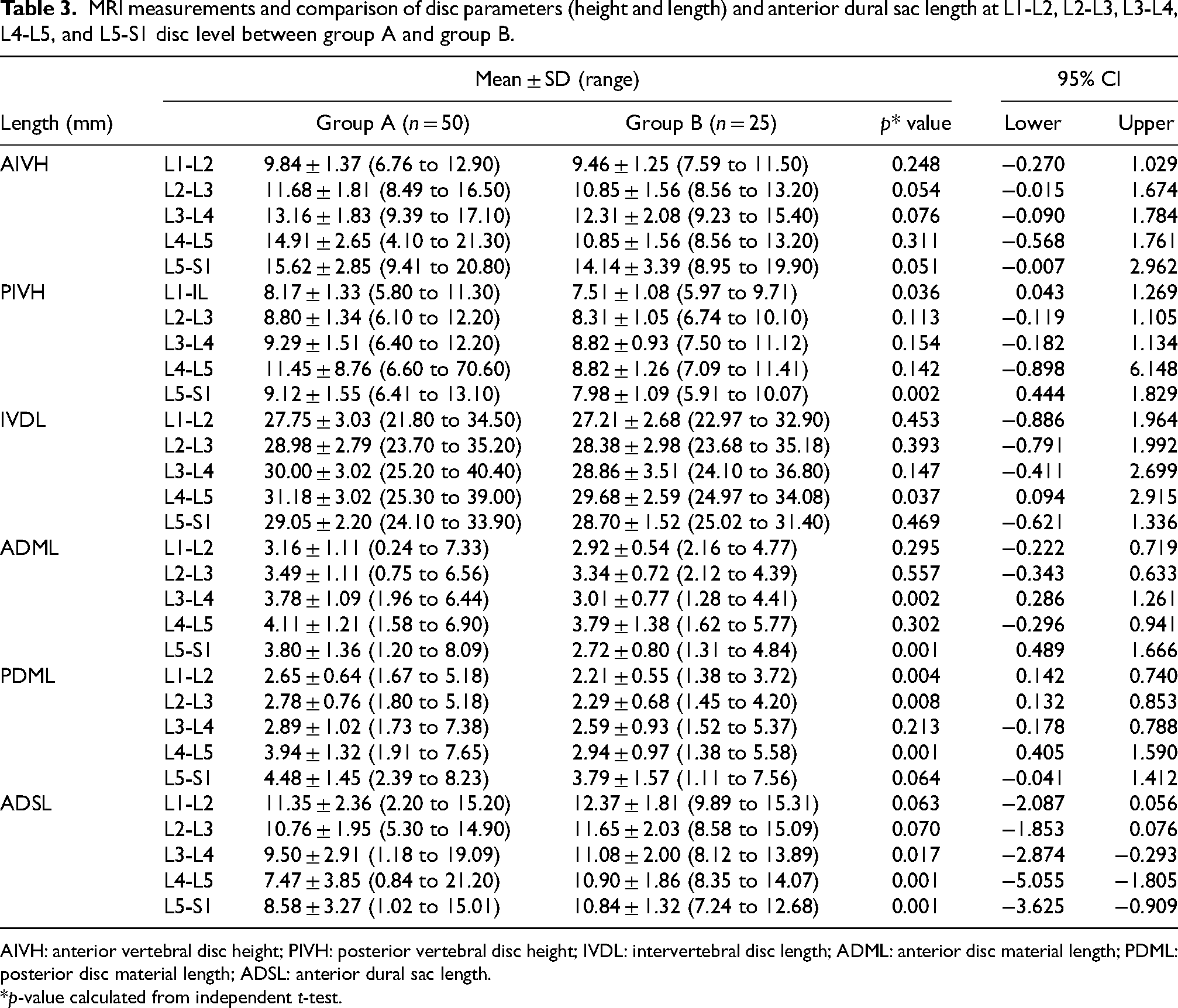
AIVH: anterior vertebral disc height; PIVH: posterior vertebral disc height; IVDL: intervertebral disc length; ADML: anterior disc material length; PDML: posterior disc material length; ADSL: anterior dural sac length.
*p-value calculated from independent t-test.
Table 4 shows comparison of CSA of anterior intervertebral height (CAIH), CSA of posterior intervertebral height (CPIH), CSA of intervertebral disc (CIVD), CSA of anterior disc material (CADM), CSA of posterior disc material (CPDM), and CSA of dural sac (CDS) between study and control population. CAIH and CPIH were mostly statistically significant (p < 0.05) higher at almost all lumbar disc level except CAIH at L3-L4 level (p = 0.07) in group A. CIVD and CADM were also mostly statistically significant (p < 0.05) higher at almost all lumbar disc level except CIVD at L1-L2 (p = 0.48) and L2-L3 (p = 0.27) levels, and CADM at L1-L2 (p = 0.32) and L4-L5 (p = 0.29) levels in group A. CPDM and CDS were again statistically significant (p < 0.05) higher at almost all lumbar disc level except CPDM at L1-L2 (p = 0.86) and L2-L3 (p = 0.18) levels and CDS at L3-L4 (p = 0.78) level in group A.
MRI measurements and comparison of cross-sectional area of disc and dural sac at L1-L2, L2-L3, L3-L4, L4-L5, and L5-S1 disc levels between group A and group B.
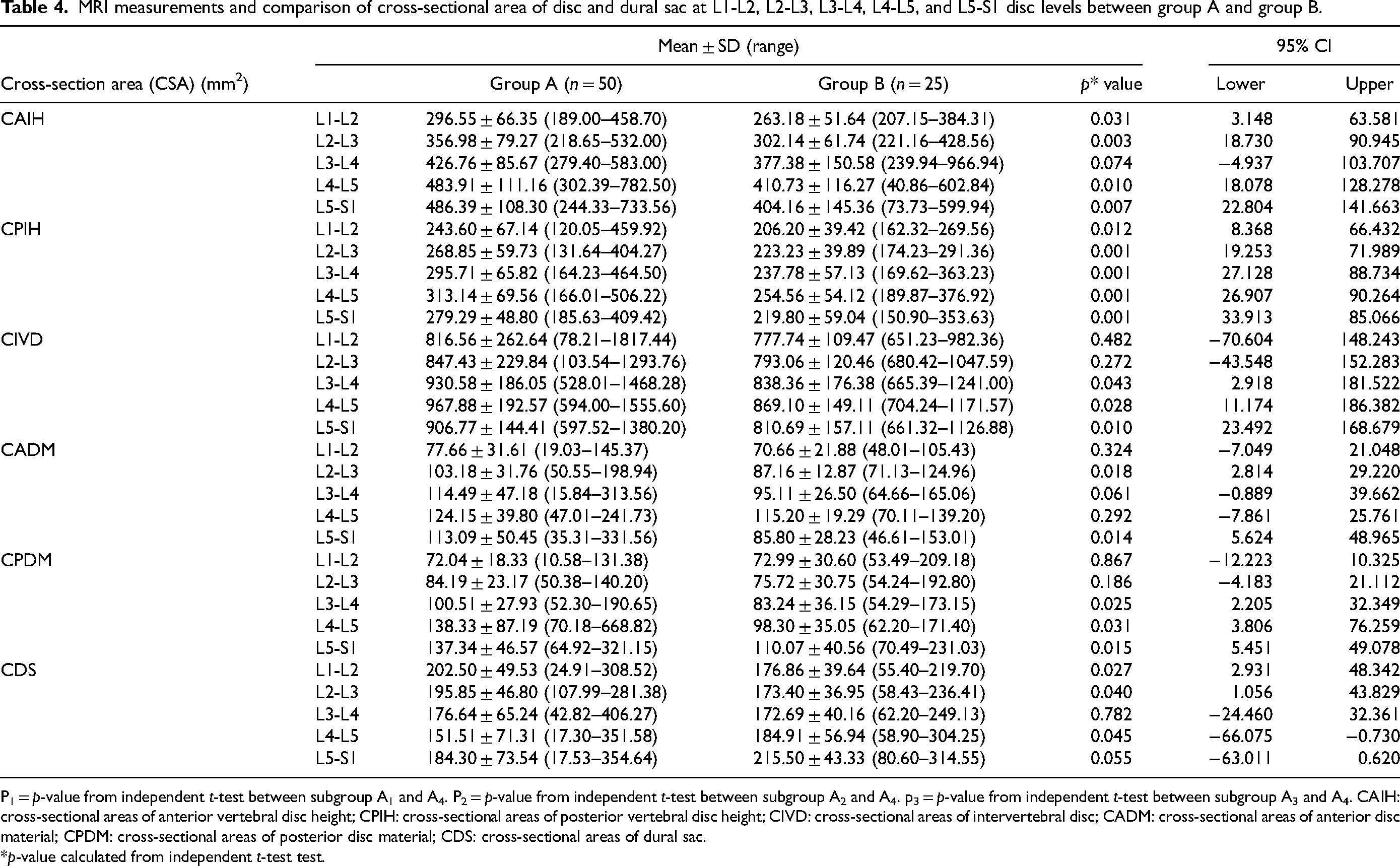
P1 = p-value from independent t-test between subgroup A1 and A4. P2 = p-value from independent t-test between subgroup A2 and A4. p3 = p-value from independent t-test between subgroup A3 and A4. CAIH: cross-sectional areas of anterior vertebral disc height; CPIH: cross-sectional areas of posterior vertebral disc height; CIVD: cross-sectional areas of intervertebral disc; CADM: cross-sectional areas of anterior disc material; CPDM: cross-sectional areas of posterior disc material; CDS: cross-sectional areas of dural sac.
*p-value calculated from independent t-test test.
Table 5 shows comparison of volume of anterior disc material (VADM) and volume of posterior disc material (VPDM) between the two groups. We noted that VADM and VPDM at all lumbar disc levels were statistically significant (p < 0.005) more in group A.
MRI measurements and comparison of volume of anterior and posterior disc material volume at L1-L2, L2-L3, L3-L4, L4-L5, and L5-S1 disc level between group A and group B.
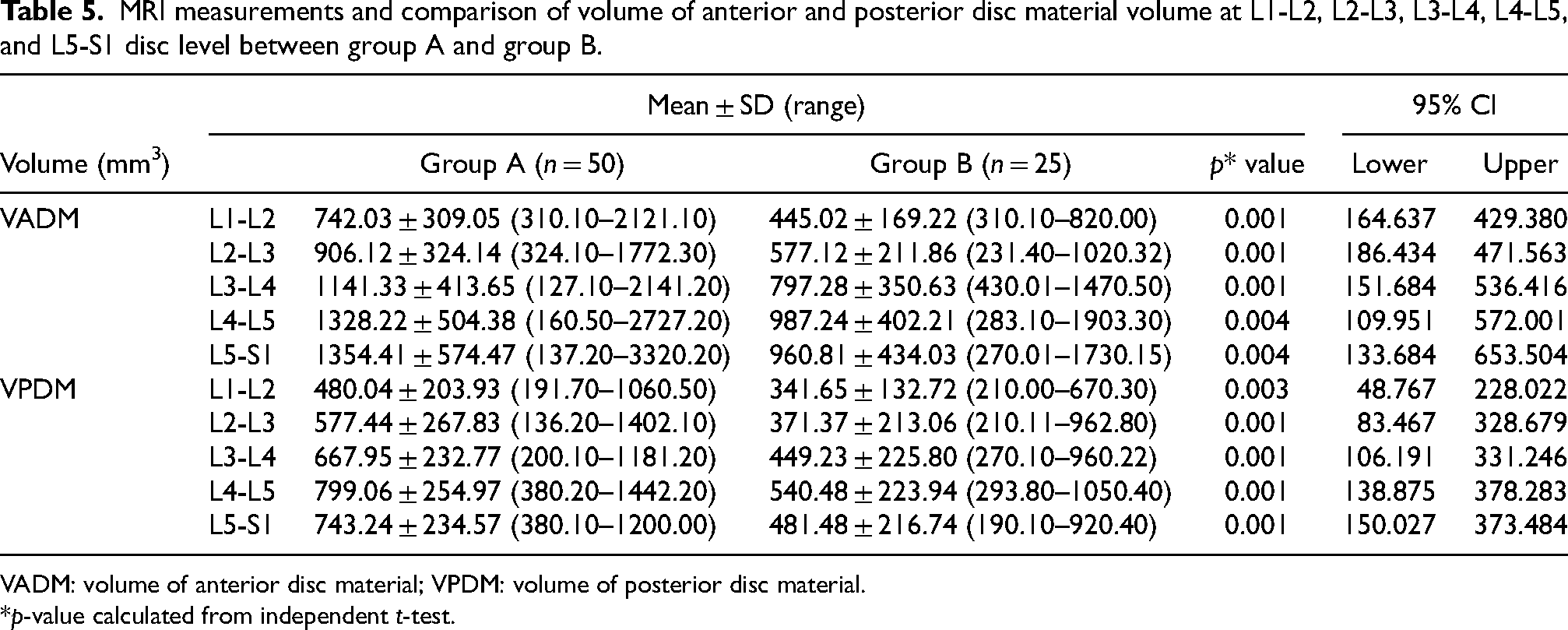
VADM: volume of anterior disc material; VPDM: volume of posterior disc material.
*p-value calculated from independent t-test.
Table 6 shows univariate linear regression analysis of association between dural sac area, average disc height, and cross-sectional area of intervertebral disc at different levels of lumbar spine. Statistical significant association was present between average disc height and dural sac area at L1-L2 (p-value = 0.039) and L5-S1 (p-value = 0.002) and cross-sectional area of the disc and dural sac area at L5-S1 (p-value = 0.049) in group A.
Analysis of the association between dural sac area, average disc height, and cross-sectional area of intervertebral disc at different levels of lumbar spine.
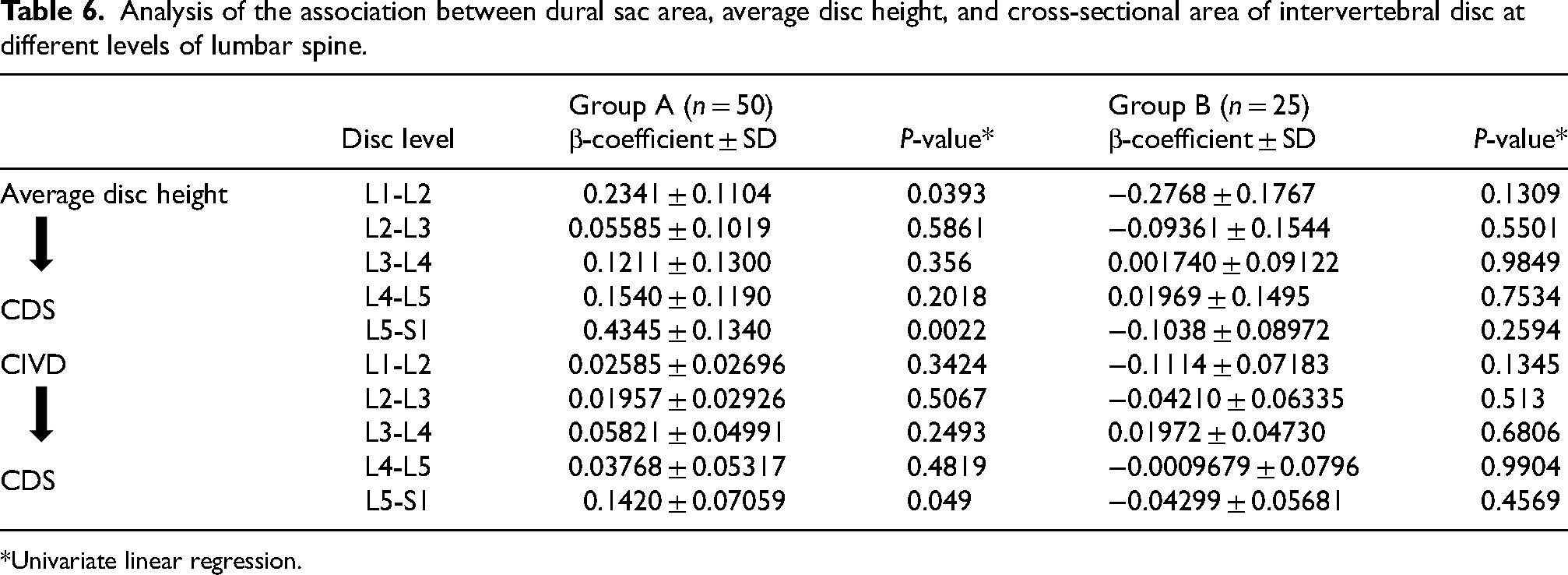
*Univariate linear regression.
Discussion
Disc parameters of CSA, orientation, and position had been reported to be sensitive methods in evaluating changes in physiopathological discs from a biomechanical point of view. 22 In the present study, the orientation of the disc in the vertebral column was evaluated by calculating disc and skin angles to find its correlation with low back pain.
We found a statistically significant difference between the two groups with regard to disc angles at L1-L2 (p = 0.01), L2-L3 (p = 0.05), and L3-L4 (p = 0.001); and skin angles at L2-L3 (p = 0.03) and L4-L5 (p = 0.05). The findings of the present study match with those reported by Tracy et al. 19 Singh et al. 16 also found a significant difference with regard to disc angles at L3-L4 (p = 0.005) and L4-L5 (p = 0.02) levels while comparing patients with CLBP and healthy volunteers. In the present study, discs in the patients with LBP (group A) were more cranially directed especially in proximal lumbar vertebrae (statistically significant p < 0.05), meaning by segmental hyperextension existed compared to healthy volunteers. It may be due to compensatory mechanism of the spine to degeneration. Literature also reports spine compensates by decrease of sacral slope, reduction of thoracic kyphosis or increase of lordosis in upper lumbar spine in the degenerative disorders of the spine.23–25 The significant normal variation in the sagittal alignment of the spine between asymptomatic people and back pain sufferers has also been noted in earlier research.16,23,24,26 According to Singh et al., a disc's abnormal orientation may render it more susceptible to degeneration. 26 We concur with the literature that pain does not necessarily associated with degenerative discs.14,26 However, it is possible that LBP is predisposed to the specific degeneration patterns and intensity linked to abnormal orientation. We are of the opinion that the orientation of the disc in the vertebral column plays a crucial role in transmission biomechanical forces and any alteration in it may predispose to back pain.
Tunset et al. 17 in their study measured parameters of disc length, area, and volume at L3-L4, L4-L5, and L5-S1 disc levels. The combined means at all measured levels (intra-rater measures agreements results) showed AIVH 14.7 ± 1.1 mm, PIVH = 9.5 ± 0.8 mm, IVDL = 31.1 ± 0.5 mm, ADML = 3.5 ± 0.6 mm, PDML = 3.6 ± 0.5 mm, ADSL = 8.5 ± 0.8 mm, CAIH = 512.6 ± 19.1 mm2, CPIH = 327.6 ± 11.7 mm2, CIVD = 1101.3 ± 10.2 mm2, CADM = 118.8 ± 12.2 mm2, CPDM = 121.8 ± 12.5 mm2, CDS = 267.9 ± 18.6 mm2, VADM = 2136.7 ± 246 mm3, and VPDM = 1314.8 ± 126 mm3. In the current study, we measured the length and volume parameters of the disc at all the lumbar levels, and the mean was measured at each level independently using the same method. However, in the present study the mean values of the disc parameters were lower as compared to the study done by Tunset et al. 17 This variance can be explained on the basis of the difference in the population under study Danish versus Asian.
Anterior disc material has its relevance to the back problems as it may be a causative factor for pain and other symptoms, especially anterior LDHs.27,28 The present study also substantiates these findings, as AIVH measurements were higher in patients with CLBP compared to controls at all levels; but at L2-L3 and L5-S1, it was significant(p = 0.05). Other disc parameters viz. PIVH, IVDL, ADML, and PDML were also higher in CLBP patients. There was statistically significant difference in PIVH at L1-L2 (p = 0.03) and L5-S1 (p = 0.002) level; in IVDL at L4-L5 (p = 0.03) level; in ADML at L3-L4 (p = 0.002) and L5-S1 (p = 0.001) level; and in PDML at L1-L2 (p = 0.004) level, L2-L3 (p = 0.008) level, and L4-L5 (p = 0.001) level.
ADSL was lower in patients with chronic LBP compared to controls at all levels; but was significant at L3-L4 (p = 0.01) level, L4-L5 (p = 0.001) level, and L5-S1 (p = 0.001). This result matches with the previous literature.6–9 Pneumaticos also reported in his study that patients with CLBP have smaller dural sac length as compared to the control population. 9
Hong et al. 29 in their study on 178 cases using picture archiving communication system (PACS) measured intervertebral space at three-level, that is, anterior disc space, middle disc space, and posterior disc space. They reported the mean distance of the intervertebral space of each segment of the lumbar vertebra. The mean distance of central portion of the intervertebral space at L1-L2, L2-L3, L3-L4, L4-L5, and L5-S1 was 7.97, 8.57, 9.64, 10.05, and 9.58 mm, respectively. Regarding the anterior intervertebral space, the mean distance at each lumbar level, that is, L1-L2, L2-L3, L3-L4, L4-L5, and L5-S1 was 6.73, 8.29, 9.88, 10.74, and 10.19 mm, respectively. Regarding the posterior intervertebral space, the mean distance at each lumbar level, that is, L1-L2, L2-L3, L3-L4, L4-L5, and L5-S1 was 5.01, 5.96, 6.63, 7.12, and 5.92 mm, respectively. In the present study, the AIVH at L1-L2, L2-L3, L3-L4, L4-L5, and L5-S1 was 9.84, 11.68, 13.16, 14.91, and 15.62 mm, respectively and PIVH was 8.17, 8.80, 9.29, 11.45, and 9.12 mm, respectively in the study (group A). In the healthy population (group B), the AIVH at L1-L2, L2-L3, L3-L4, L4-L5, and L5-S1 was 9.46, 10.85, 12.31, 10.85, and 14.41 mm, respectively and PIVH was 7.51, 8.31, 8.82, 8.82, and 7.98 mm, respectively.
Mirab et al. 30 measured normal intervertebral disc dimensions in the Iranian population. They reported that mean anterior, middle, and posterior disc heights at L4-L5 level were 18.14, 13.82, and 10.14 mm, respectively; and at the L5-S1 level the values were 18.71, 12.99, and 8.51 mm, respectively. Kizilgöz and Ulusoy 31 used lateral lumbar spine radiographies to measure the disc height in Turkish population. They reported the anterior, middle, and posterior disc heights 13.26, 11.20, and 8.44 mm, respectively at the L4-L5 level and 12.46, 9.50, and 5.89 mm, respectively at the L5-S1 level for non-degenerated discs. The findings by Hong et al., 29 Mirab et al., 30 and Kizilgöz and Ulusoy 31 did not match with the current finding. It might be due to differences in the methods for measurement of disc space and differences in the genetically different study population.
In the present study, we found that the measured values of CAIH, CPIH, CIVD, CADM, and CPDM were higher in group A (study) population than group B (control) population at all lumbar levels. Statistically significant differences between study and control population were observed for CAIH at L1-L2 (p = 0.03), L2-L3 (p = 0.003), L4-L5 (p = 0.01), L5-S1 (p = 0.007) level; for CPIH at L1-L2 (p = 0.01), L2-L3 (p = 0.001), L3-L4 (p = 0.001), L4-L5 (p = 0.001), L5-S1(p = 0.001); and for CIVD at L3-L4 (p = 0.04), L4-L5 (p = 0.02), L5-S1 (p = 0.01). Statistically significant differences for CADM at L2-L3 (p = 0.018), L5-S1 (p = 0.014) level; and for CPDM at L3-L4 (p = 0.02), L4-L5 (0.03), L5-S1 (p = 0.015) level were also observed. A significant finding of the current study was that CDS was significantly large in the upper lumbar spine: L1-L2 (p = 0.027), L2-L3 (p = 0.04); no difference at L3-L4 (0.782); and was significantly smaller at lower lumbar levels: L4-L5 (p = 0.04) and L5-S1 (p = 0.05) in CLBP patients. We are of the opinion that smaller dural sac area at lower lumbar may be one of the underlying cause for LBP, as also has been observed in the studies done in the past.9,32,33
Kjaer et al. 32 evaluated changes in and associations between the size of lumbar disc herniations, dural sac area, and disc height longitudinally over an 8-year period using MRI. Cross-sectional areas of dural sac area and disc height measurements at L3-L4, L4-L5, and L5-S1 levels were larger at presentation, four and eight years in patients with LDH than found in the present study. However, there is no study in the literature where a comparison of the CSA of the dural sac had been reported between CLBP and healthy population using the technique used in the current study and at all the lumbar levels. However, Pneumaticos et al. 9 also reported in their study using direct measurement on MRI that in patients with isolated leg pain secondary to intervertebral disc herniation CDS was smaller compared to the control population.
A statistically significant difference (p < 0.005) in disc parameters of VADM and VPDM was observed between the study and control population in the current study at all lumbar disc levels. VADM and VPDM were larger in group A (study) population than group B (control) population. However, there is no literature to compare these parameters using the measurement method used in the present study. However, Holodny et al. 33 reported volume of herniated material for all lumbar and lumbosacral levels with a mean of 503 ± 301 mm3. The average volume of all the intervertebral disc included in the study was 14,442 ± 4200 mm3 and of normal-appearing discs was 17,476 ± 2885 mm3. They also reported average height of all the discs and of normal-appearing disc was 10.1 ± 2.2 mm and 11.3 ± 1.3 mm, respectively.
We found a positive association between the dural sac area and average disc height at L1-L2 (p-value = 0.0393) and L5-S1(p-value = 0.0022) only; and cross-sectional area of disc and DSA at L5-S1(p-value = 0.049) in LBP patients (group A). No such association was observed in the healthy volunteers (group B). Kajer et al. 32 reported a statistically significant cross-sectional association between disc height and dral sac area. Many studies in the past had reported associations between LDH or disc degeneration with spinal canal area or dural sac area in the lower lumbar levels. Similar to the findings of the current study, these studies reported smaller dural sac area and/or spinal canal area in symptomatic patients treated either conservatively or undergoing discectomy.7,32,34
Back pain is a complex and multifactorial condition that likely develops as a result of the interaction between several risk factors. 35 Systematic reviews have suggested that physical risk factors, an unhealthy lifestyle, and psychological factors increase the risk of a back pain episode.36,37 As there is a poor correlation between LBP severity and its radiological findings; clinicians should incorporate comprehensive subjective, observational, and physical examinations, as well as proxy reports to make accurate diagnosis. 38 A multidisciplinary approach to the management of LBP that integrates biological, psychological, and social aspects is required. 39
The study has several strengths. The cohort included two groups (study and controls) that were comparable in all the demographic variables. We used a validated quantitative measuring method for calculating the parameters of disc and dural sac and which had shown good intra- and inter-rater agreement as well as reliability. 13 The present study has few limitations. It is a cross-sectional study and the sample size is small. We have not evaluated the overall lumbar lordosis and the global sagittal balance. And also did not evaluate the parameters in the uploaded spine position to see postural changes. Longer follow-up and measurements of the disc at different points of time would have helped us to understand how these parameters change with time.
The findings of the present study have clinical implications that even if an MRI appears normal in a patient with LBP, the underlying etiopathogenesis of LBP may be the altered morphology of the discs (orientation, height, volume, CSA, and length). Shape and volume of the IVDs influence the load-carrying capacity of the spinal column. 40 Future research is required to further elaborate on this “cause and effect relationship” and what specific therapeutic measures can be used to alleviate the associated back pain.
The present study has limitation of small sample size. Statistically proven results and unique nature of the study are the strength of our study.
Conclusions
There was a significant difference in the lumbar disc orientation and dimensions between LBP patients and healthy individuals. Larger disc parameters (height, volume, CSA, and length) and altered orientation may affect the biomechanics of the spine, thus predisposing to LBP. Further studies in the future are required to substantiate this and observe how these quantitative parameters change in long-term follow-up periods for a better understanding of the pathophysiology of LBP.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical standard statement
The study was approved by the Institutional Review Board. IRB approval No. Endst.No. Surg/Dean/17.2369-77 Dated 16/8/2017.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was obtained from all participants in this study.