
Abstract
Introduction
The rotator cuff plays a significant role in the static and dynamic stability of the shoulder.1,2 The shoulder can become unstable after losing the active and passive restraints of the rotator cuff. 3 A rotator cuff tear is among the most common shoulder disorders. While there is an age-related increase in the prevalence of rotator cuff tears, they can occur in patients of all ages, as a result of differing pathophysiology. 4 Age-related degeneration and trauma have been implicated in the pathogenesis of rotator cuff tears.5,6 While asymptomatic tears are rare in those under 40 years of age, estimates of a full-thickness tear range from 6% to more than 50% in those over 60 years of age.5–10 This can have an impact on quality of life that is comparable to that of diabetes, myocardial infarction, congestive heart failure, or depression.11–14
A distinct age-related prevalence also exists with proximal humerus fractures. A sharp increase in numbers occurs during the sixth and seventh decades of life, as a result of the development of osteopenia and osteoporosis.15–17 Substantial overlap should therefore be expected between the two patient populations of proximal humerus fractures and rotator cuff pathology. Indeed, up to 40% of individuals sustaining a proximal humerus fracture will have a full-thickness rotator cuff tear. 18 The degenerative state of the rotator cuff in the elderly makes it more vulnerable to injury in proximal humerus fractures. 3 It is therefore appropriate to consider a tear as an endpoint of degenerative tendinopathy in the elderly. 19
There are similar rates of shoulder dislocation in patients younger and older than 45 years of age. 20 However, many studies have demonstrated differences in clinical manifestations and prognosis in elderly patients. The pathophysiology of anterior shoulder dislocation differs between young and elderly patients as a result of changes in tissue elasticity. 21 Failure of anterior capsulolabral structures are most commonly implicated within young patients, whereas posterior structures are more likely to fail secondary to pre-existing rotator cuff pathology within the elderly population. 22 Some studies however have reported that anterior structures may have a contributory role in elderly patients sustaining recurrent dislocation. 23 Recent biomechanical studies have demonstrated that it is unclear whether shoulder dislocation induces rotator cuff injury or whether pre-existing and asymptomatic rotator cuff pathology results in abnormal shoulder movement resulting in shoulder dislocation with trivial trauma.23,24 The overall frequency of a rotator cuff tear following an anterior shoulder dislocation ranges between 7% and 32% and increases with advancing age.25,26
Although this study does not specifically consider treatment modalities and the subsequent outcomes it is worth noting that management of rotator cuff tears continues to be a source of debate, with a role for both non-operative and operative interventions. 27 Many studies focus on elderly patients or fail to delineate between older and younger populations. 4 Numerous differences exist between young and old patients with regards to healing potential, tear etiology, and functional demand in addition to long-term expectations.28–30 In contrast, much of the literature regarding clinical outcomes of shoulder dislocation in the elderly included patients older than 40 years of age.31,32 Conclusions made in an elderly population are not necessarily applicable to younger patients and vice-versa, and as such both need to be approached differently. There are further implications for management within an elderly population in light of the use of the reverse total shoulder prosthesis in the management of proximal humerus fractures for patients who are likely to be cuff-deficient. 33
The aim of this study was to determine the prevalence of a concomitant rotator cuff tear, without age-based exclusion and including multiple treatment modalities, in the following patient populations:
Group 1. Proximal Humerus Fractures Group 2. Shoulder Dislocations Group 3. Proximal Humerus Fracture-Dislocations
Materials and methods
This is a cross-sectional epidemiological study which did not require IRB/ethics committee approval. A retrospective review between the period of August 2012 and August 2014 was performed on all patients who sustained one of the following injuries: Proximal Humerus Fracture (Group 1), Shoulder Dislocation (Group 2) or Proximal Humerus Fracture Dislocation (Group 3) at the authors' institution. Management of the shoulder injuries included both operative and non-operative intervention. Operative intervention encompassed intramedullary nail, plate fixation, or hemiarthroplasty. No exclusion criteria were applied. All patients within the study underwent x-ray imaging at the time of diagnosis. Information obtained by the authors from the radiological imaging at the time of injury included Neer classification 34 and AO classification 35 when considering Proximal Humerus Fractures with or without an associated dislocation. The decision for further imaging of ultrasound or magnetic resonance imaging (MRI) to assess for rotator cuff tears was made at widely variable time periods after initial injury where clinically indicated by the overseeing clinician. This was based on clinical evaluation of history and examination including provocative tests of the rotator cuff. The choice of scan was at the clinician's discretion and these were performed by either the consultant radiologists or diagnostic radiographers under the supervision of the radiologists.
Results
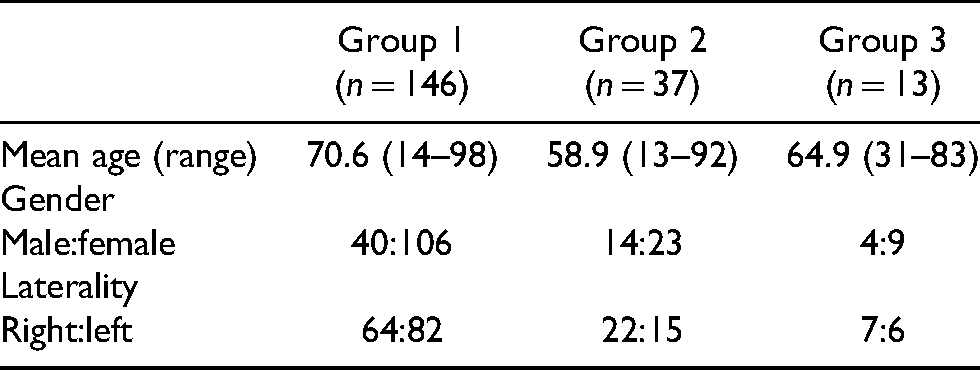
Table 1 shows the patient demographics and Table 2 shows the results of the prevalence analysis. A total of 23 rotator cuff tears were found within the study population of 196 patients, equating to an overall prevalence of 11.7%. The highest number of tears was found in Group 1 (n = 14). However, the highest percentage of rotator cuff tears was seen in Group 2 (18.9%). The mean age of patients sustaining a dislocation was lower than that of the other two groups. Within all three study groups, there was an increased number of females sustaining injuries compared to males.
Patient demographics.
Prevalence of rotator cuff tear in each group.
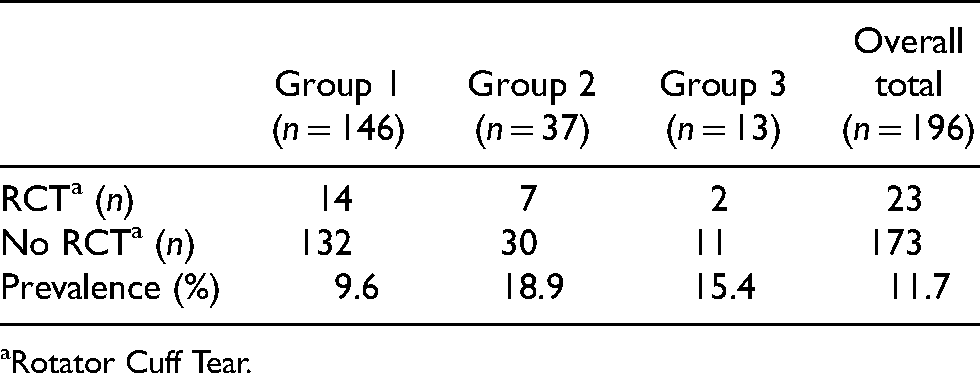
Rotator Cuff Tear.
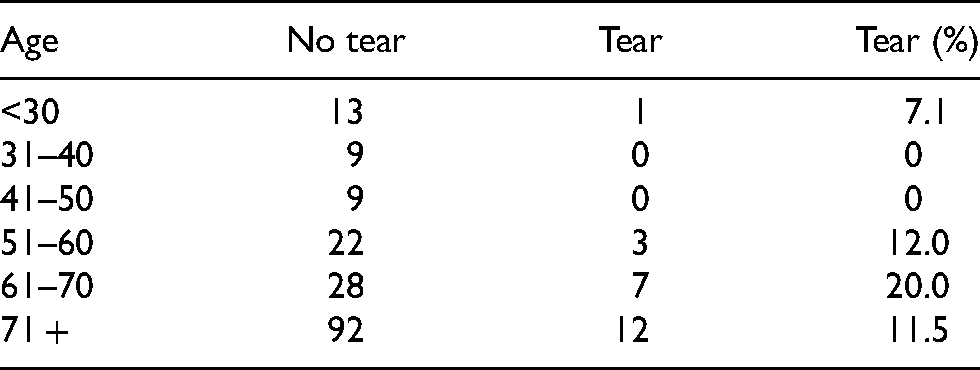
On average, patients sustaining a rotator cuff tear were 4.2 years older than those without a tear. Moreover, there was a trend towards an increasing prevalence of rotator cuff tears with age. There was an age-related increase in rotator cuff tears, peaking at a prevalence of 20% in the 61–70 age group (Table 3).
Rotator cuff tears with age.
Proximal humerus fractures
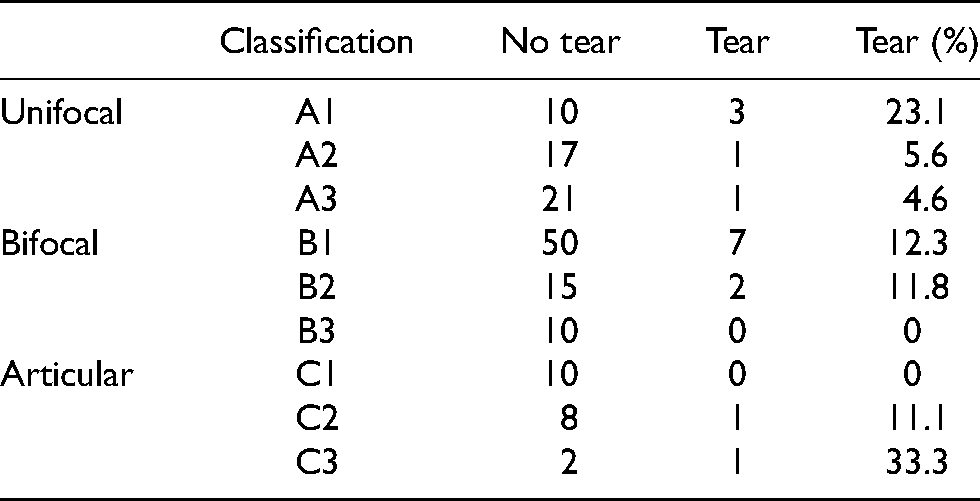
There was a trend toward a higher rate of rotator cuff tears in Neer 1-part fractures and in the 3-part surgical neck and greater tuberosity fractures (Table 4). When applying AO classification to the fracture types, there was a higher prevalence of rotator cuff tear in the A1 and C3 groups (Table 5).
Rotator cuff tears by Neer classification.
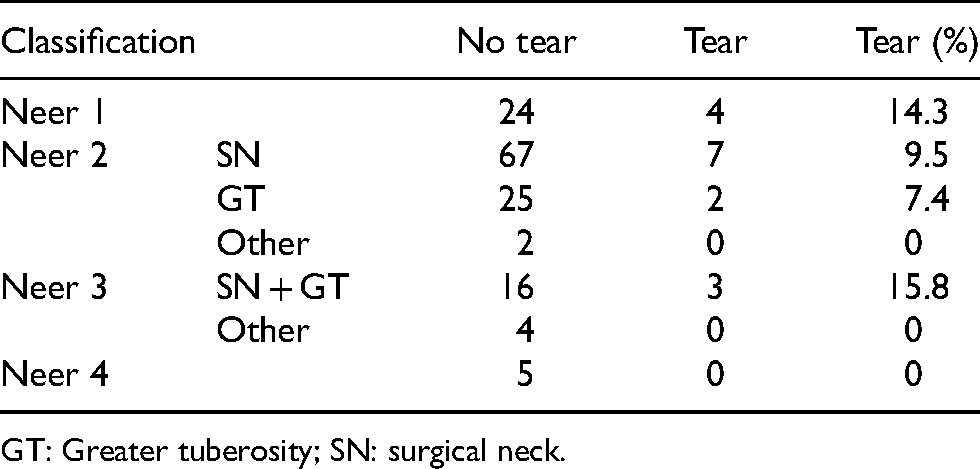
GT: Greater tuberosity; SN: surgical neck.
Rotator cuff tears by AO classification.
Tear pattern
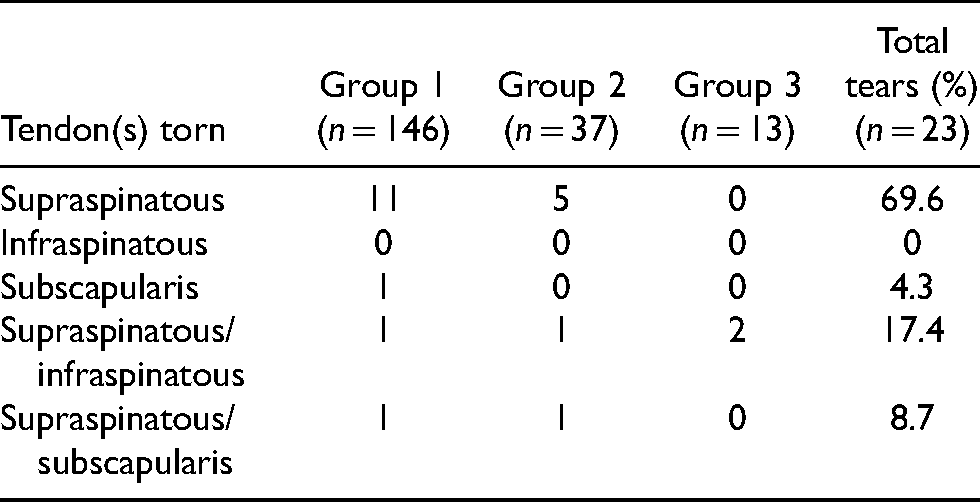
Twenty-three people sustained a concomitant rotator cuff tear in total, with 18 being detected by ultrasound scan with the other 5 detected by MRI scan. Tables 6 and 7 demonstrate the breakdown of these tears by the group as well as the pattern of the tear. Of the 23 tears, 14 (60.9%) were full-thickness tears while the other 9 (39.1%) were partial-thickness tears. Full-thickness rotator cuff tears had an overall prevalence of 7.1% in the study. Single tendon rotator cuff tears involved 17/23 (73.9%) cases, with supraspinatus being the most commonly injured tendon (69.6%). Twenty-one of those sustaining concomitant rotator cuff tears were treated non-operatively.
Tear pattern by shoulder injury.

Rotator cuff tendon torn by shoulder injury.
Discussion
The main finding in this study was that a higher prevalence of rotator cuff tear is found in patients over the age of 50 years and in association with shoulder dislocation.
The rotator cuff contributes significantly to the active and passive stability of the glenohumeral joint.1,2 While multiple studies have demonstrated an age-related increase in the prevalence of rotator cuff tears, the rotator cuff may also become susceptible to injury in younger athletes who endure repetitive microtrauma during contact sports or during overhead throwing motions.36,37 While the underlying pathophysiology and mechanisms of rotator cuff tear differ between the young and elderly, injury to the shoulder in either population may damage the already weakened rotator cuff, causing ongoing dysfunction or instability thereafter. Prompt evaluation and appropriate treatment are necessary to avoid this.
A number of studies have established a strong age-related increase in the incidence of proximal humerus fractures, showing a growth pattern for women from 40 to 84 years old, that places it among other osteoporotic fractures. 16 With this in mind, it should not be uncommon to find a concomitant rotator cuff tear among those sustaining a proximal humerus fracture. In contrast, there is a well-established relationship between rotator cuff tear and shoulder dislocation in those older than 40 years of age. 38 However, no other study has exclusively considered shoulder dislocation as a factor when considering rotator cuff tear prevalence. Although diagnostic modalities differed and reported prevalence to vary significantly, all studies demonstrate increasing rates of rotator cuff tear with age.5–10,39
The aim of the study was to determine the prevalence of a concomitant rotator cuff tear among three patient populations; proximal humerus fractures, shoulder dislocations, and proximal humerus fracture-dislocations. Other studies have tended to focus on an individual injury modality in order to better define the relationship with an associated rotator cuff tear, with the majority concentrating on proximal humerus fractures. Differences among methodology are evident between studies, with Fjalestad et al. 40 and Nanda et al. 41 examining the rotator cuff by MRI and ultrasound, respectively, and only including patients who were treated non-operatively. In contrast, Choo et al. 42 excluded patients managed via non-operative means, concentrating on those treated surgically. Moreover, the majority of studies focus on the elderly population. With regards to the current study, there were no exclusion criteria applied to age while both non-operative and operative treatment modalities were included.
The overall prevalence of a concomitant rotator cuff tear in this study was 11.7%, within the large range of 5 to 50% reported in the literature.40,41 The figure could be broken down further into a full-thickness tear prevalence of 7.1% and a partial-thickness tear prevalence of 4.6%. The decision to include partial-thickness tears was made as these could cause dysfunction and progress to full-thickness tears although this study is limited without a further breakdown of partial-thickness tears. The study demonstrates that patients with a rotator cuff tear were more likely to be older and to have sustained a dislocation. Studies have shown that a rotator cuff tear was the most common associated injury following shoulder dislocation, with rates reported to range from 35% to 86% in patients older than 40 with increasing prevalence with age.32,43 Indeed, all patients over 70 years of age sustaining a shoulder dislocation, included in those studies, were found to have a concomitant rotator cuff tear.
Other studies, particularly those focusing on proximal humerus fractures, found an increased prevalence of rotator cuff tears with increasing age.5–10,41,44 In contrast Gallo et al. 18 findings contradict this. However, patients over the age of 65 years were excluded from the study, thereby removing the population where a rotator cuff tear would be expected.
Given that a rotator cuff tear can be viewed as the endpoint of degenerative tendinopathy in the elderly, 19 this raises the question of how many rotator cuff tears found were acute and traumatic. Sixty-six percent of rotator cuff tears in a study by Bahrs et al. 44 were traumatic, based on a comparison of the injured and uninjured shoulders.
When considering proximal humerus fractures individually, there was a trend towards a higher rate of rotator cuff tears in fractures involving 3-part fractures involving the greater tuberosity. Moreover, the majority of rotator cuff tears occurred in fractures involving the greater tuberosity, when considering the Neer classification. 34 Bahrs et al. 44 showed that 57% of patients with a fracture involving the greater tuberosity also sustained a dislocation, hypothesizing that the fracture was effectively a completed Hills-Sach lesion. With this and the current data in mind, this suggests that dislocation is a strong contributing factor with regard to a concomitant rotator cuff tear. Indeed, the prevalence of a concomitant rotator cuff tear within the dislocation and fracture-dislocation group were 18.9% and 15.4% respectively, compared with 9.6% within the proximal humerus fracture population. With regards to the AO classification, 35 there was a trend towards a higher rate of rotator cuff tears in fractures involving the articular surface.
The current study has a number of limitations. It is retrospective in design and is heavily reliant on correct clinical coding and appropriate interpretation of x-rays, particularly when applying Neer 34 and AO classifications 35 to the fracture population. The number of patients within each patient population varied significantly. It was difficult to determine the rate of acute versus chronic tears within the study. However, imaging modalities were only performed when a concomitant rotator cuff tear was clinically suspected following injury. This would therefore act to reduce the number of degenerative or asymptomatic tears detected, thereby providing an argument against imaging every person who sustains a shoulder injury. This could also explain the lower percentage of tears within the proximal humerus fracture population seen in this study compared to other studies. However, the inability to rule out incidental findings of previous rotator cuff tears limits the study, imaging of the shoulder prior to injury could rule out pre-injury rotator cuff tears but this is beyond the scope of the current study. Despite this, the results do show an increase in incidence compared to the background population incidence of 4.7% to 7.6%.8,45,46 There was a disproportionate number of patients in each of the 3 groups. This does not detract from the findings of the study as proximal humerus fractures are more prevalent conditions than shoulder dislocations and furthermore fracture-dislocations are severe but relatively uncommon injuries overall.
It is clear that certain recommendations could be made when considering a concomitant rotator cuff tear. In any patient sustaining a shoulder injury, where there is high clinical suspicion (i.e., risk factors) and subsequent management will be affected (i.e., surgery), imaging should be considered. In the event where there is ongoing dysfunction and symptoms following injury or recurrent dislocation, imaging should also be considered.
Conclusion
The current study demonstrated an overall prevalence of rotator cuff tear of 11.7% in a population of proximal shoulder injuries, encompassing fractures, dislocations, and fracture-dislocations. Those with a concomitant rotator cuff tear were more likely to be older and have sustained a dislocation.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This was a cross-sectional epidemiological study which did not require IRB/ethics committee approval.