
Abstract
In the following report, we present the case of a patient who presented with a proximal humerus fracture dislocation and an associated brachial plexopathy. After undergoing a reverse total shoulder arthroplasty, the brachial plexopathy showed signs of improvement plateaued until the patient started having increased pain in the involved extremity and the brachial plexopathy began to worsen. At that time, it was discovered that the patient had heterotopic ossification (HO) encasing the brachial plexus and axillary artery. To our knowledge, this is the first reported case of HO involving the brachial plexus and axillary artery.
Keywords
Introduction
Although heterotopic ossification (HO) of the shoulder has recently been discovered to be more common than originally thought, 1 to our knowledge, there have been no reported cases of HO involving the brachial plexus leading to impingement on the plexus and vasculature. The following case report discusses a patient who suffered a 3-part proximal humerus fracture dislocation with associated brachial plexopathy which was treated with a reverse total shoulder arthroplasty. The patient subsequently developed extensive HO that encased the axillary neurovasculature including the brachial plexus.
Case History
The authors of the following case report have had the patient consent to having her data being submitted for publication. A 67-year-old female presented to the emergency department after a fall from standing height onto her left shoulder causing a 3-part proximal humerus fracture dislocation (Figure 1(a) and (b)). During this consultation, the patient had decreased motor function in the ulnar, radial, and median nerve distributions and decreased sensation in the axillary nerve distribution. The patient was admitted to the hospital for pain control and on day 4 of admission, the patient agreed that a reverse total shoulder arthroplasty would be the best treatment for her condition, and she was scheduled for surgery the following day.
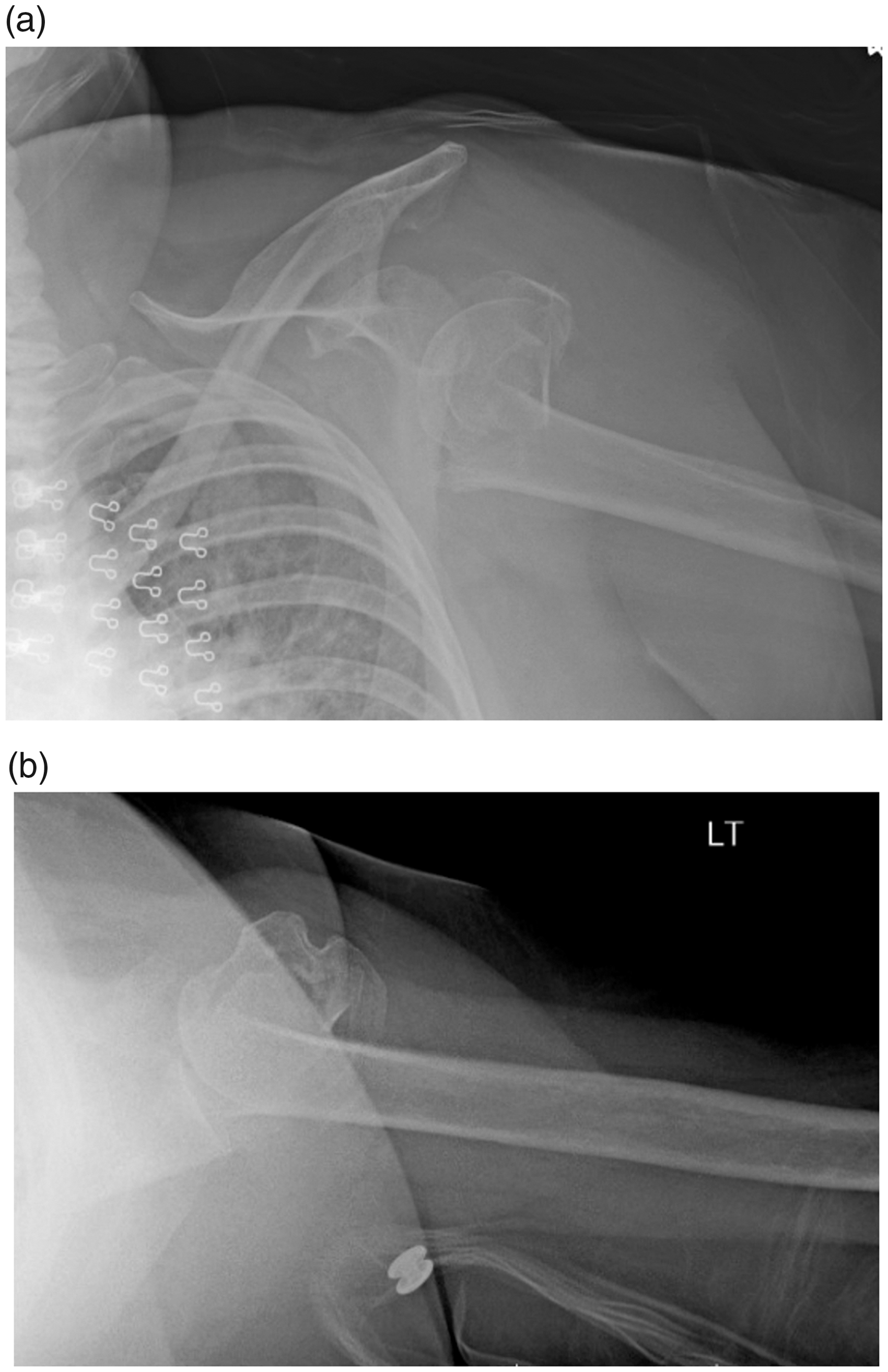
a–b, AP and axillary radiographs of a left shoulder demonstrating a 3-part proximal humerus fracture dislocation.
The patient was taken to the operating room and placed in the beach chair position. A standard deltopectoral approach was utilized. Dissection was taken down until fracture hematoma was encountered and evacuated, the conjoint tendon was then freed and the humeral head was noted to be dislocated anteriorly and inferiorly. The shaft was noted to be displaced with the tip extending into the subcoracoid space. The humeral head was then removed using the pectoralis major tendon as the uppermost marker of the humeral shaft, and the humeral shaft was prepped in the standard fashion. At this time, the axillary nerve was identified and a tug test was performed which showed it to be intact and running into the deltoid. With the axillary nerve protected, the remainder of the surgery went as planned. Prior to closure, the shoulder was taken through full range of motion and found to be well reduced with appropriate tension. Postoperative x-rays were taken following the conclusion of surgery and with the patient safely in the postanesthesia care unit (Figure 2).
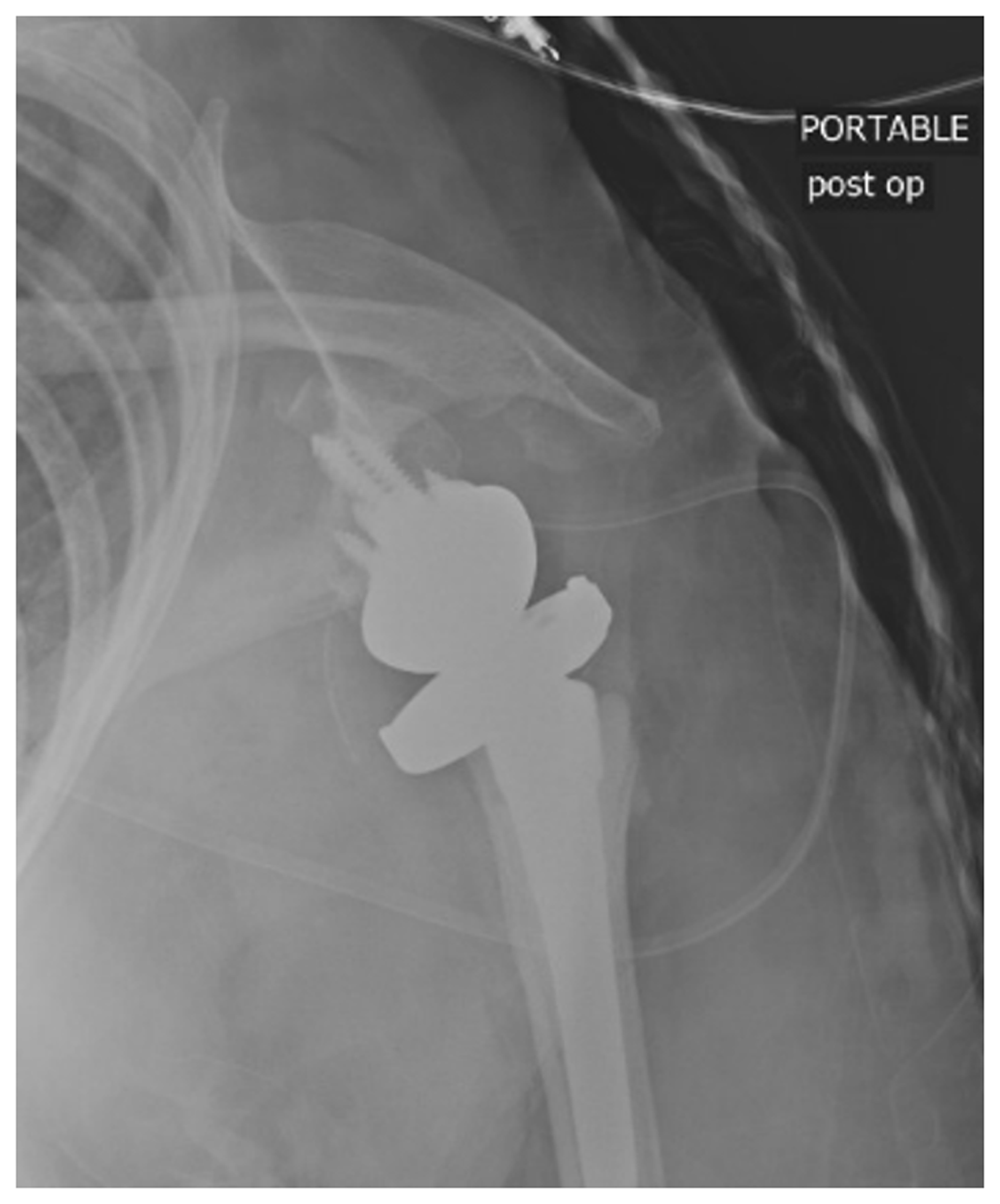
AP radiograph status postreverse total shoulder arthroplasty demonstrating appropriate alignment of components.
On postoperative day 1, the patient was seen and noted to have 1/5 radial and ulnar nerve motor strength as well as diminished sensation in the axillary nerve distribution. By postoperative day 4, the patient was noted to have continued improvement in her neuropraxia with 3/5 muscle strength in the radial nerve and 5/5 strength in both median and ulnar nerves. Sensation was also noted to be improved in the axillary nerve distribution. The patient was then discharged from the hospital to a subacute rehabilitation facility for further strengthening before returning home.
One week after surgery, the patient was seen in the office and was noted to have absent motor function in the axillary nerve but intact function of the musculocutaneous nerve. She had 4/5 motor strength in the median and ulnar nerves but had weakened thumb extension and absent extension of the fingers. Sensation was diminished in the ulnar, median, radial, axillary, and musculocutaneous nerve distributions. The patient was again seen at both 3 and 6 weeks postoperative and found to have minimal change with sensation dulled in the axillary, musculocutaneous, radial, ulnar, and median nerve distributions. At both examinations, there was no motor function of the axillary or radial nerves with intact musculocutaneous, median, and ulnar nerves. Her range of motion was 90° of passive forward flexion, 90° of passive abduction, and 30° of passive adduction and external rotation. The patient had x-rays taken at 6 weeks postoperative which were unremarkable aside from normal postoperative changes. The patient was referred for electromyography (EMG) at the 3-month postoperative time interval since the brachial plexus injury symptoms had not improved; however, the study was not completed at this time.
Over the course of the next 12 months, the patient was randomly assessed in the emergency department for complaints including forearm cellulitis, secondary to a burn she suffered from her decreased sensation, and left upper extremity deep vein thrombosis (DVT). The DVT was treated with xarelto and came to a complete resolution; however, there was still minimal improvement in neurologic exam during these visits.
At approximately 17 months status postleft reverse total shoulder arthroplasty, the patient presented to the emergency department with complaints of dramatic increase in left shoulder pain and decline in function. She denied any history of trauma or falls. The patient at this time had regained full sensation in the radial, ulnar, median, and musculocutaneous nerve distributions and also admitted to an increase in sensation in the previously absent axillary nerve distribution. Her motor function was still absent in the axillary nerve and radial nerve function below the elbow; however, the ulnar, median, and musculocutaneous motor function was intact. The patient had a significantly decreased shoulder range of motion with a 30° flexion contracture of her left elbow and was only able to flex the elbow to 110°. X-rays were performed which showed a reverse total shoulder arthroplasty with intact components and showed no evidence of loosening or abnormal wear. However, at closer examination, the x-rays did demonstrate abnormal bone formation extending from the lateral margin of the scapula to the medial aspect of the proximal humeral shaft (Figure 3). A computerized tomography (CT) scan (Figure 4(a) to (c)) was then ordered to evaluate the extent of HO and to determine if any occult fracture or component loosening was present. The CT results demonstrated HO extending from the anteromedial aspect of the proximal humeral shaft to 5.1 cm distal to the humeral base plate. It also extended superiorly and medially along the neurovascular bundle, partially encasing the axillary artery and likely components of the brachial plexus.

AP radiograph 1.5 years status postsurgery demonstrating appropriate alignment of reverse total shoulder components with significant heterotopic ossification extending from the inferior glenoid to the proximal humeral shaft.

(a) Axial CT image demonstrating heterotopic ossification encasing the axillary vasculature (b) and (c). Coronal CT images of left shoulder demonstrating heterotopic ossification surrounding the axillary neurovascular bundles.
Upon follow-up in the office, her neurologic impairment had essentially plateaued with gains in her Range of Motion (ROM) which the patient was comfortable with. The patient was referred again for an EMG at this time which was completed and confirmed that the patient had a left brachial plexopathy primarily involving the posterior cord. There was also evidence of active ongoing axon loss with findings consistent with ongoing reinnervation in the radial distribution.
Upon further evaluation, the patient had regressed to having pain with movement of her arm leading us to consider that the HO may have a tethering effect on her axillary nerve. Upon consultation and recommendation of a tertiary subspecialist, we speculated that this possible tethering effect on the posterior cord was causing irritation to the axillary nerve and that an axillary nerve block at the quadrangular space would be appropriate to assess for any relief. If relief was obtained, the tertiary subspecialist felt there would be an increased likelihood that surgical intervention for the removal of the HO would be an option for symptomatic management. Because of this, subsequent injections of carbocaine were given in the quadrangular space which provided pain relief. The results of the injections led to agree with our hypothesis that if there was an impingement, that it was only affecting the axillary nerve. At the time of these findings, the patient was referred to the subspecialists tertiary care center for evaluation of surgical options for resection of the HO. The patient, however, decided not to be evaluated at the tertiary care center even after an extensive discussion of the risks of what could occur without surgery.
Discussion
Displaced proximal humerus fractures historically are known to have many complications associated with them. One of these complications is nerve injuries due to components of the brachial plexus being affected by the fracture. The most common of the nerves to be affected is the axillary nerve due to its proximity being close to the humeral head; however, any brachial plexus component can be affected. 2 The incidence of nerve injuries following proximal humerus fractures has ranged in the literature with 1 study looking only at 4-part fractures reporting it as 6.1% 3 and another looking at complex fractures of the proximal humerus reporting a range of 5% to 30%. 4 Although this is a rarer complication, it is important to do a thorough neurological exam and not complete repeated attempts at closed reduction as this is something that can be easily missed and caused iatrogenically. 5
Although there are complications that can occur with any fracture, there are also many complications that can occur from surgical intervention. One of these surgical complications is HO or bone formation in the soft tissue. Although HO is more commonly known for its formation following hip surgery than it is following shoulder surgery, 6 the development of shoulder HO is being shown in the literature to be more common than originally thought. Because of this, Kjaersgaard-Anderson et al. developed a grading system focused on the amount of HO in the glenohumeral space. Their classification, however, does not take into account HO that develops outside of this area. Their primary focus was this area due to the fact that they discovered that HO occurred in 45% of their patients following total shoulder arthroplasty. 7 Since then, there have been reports of HO occurring in other areas of the shoulder. One of these areas is the long head of the triceps tendon where Ko et al. discovered that 61.6% of their patients who underwent a reverse shoulder arthroplasty developed HO and 23.2% had osteophytes that were considered impinging. 1
Even though this is a unique case, it adds to the evidence provided by others that HO development after total and reverse total shoulder arthroplasty is more common than was originally thought. It also represents the morbidity that a patient can experience secondary to a complex proximal humerus fracture dislocation and the subsequent problems that can come from a brachial plexopathy. While the patient in this case had an initial improvement in her brachial plexopathy, the development of HO of the axillary neurovasculature complicated her overall recovery and she had a regression in her neurologic symptoms at the same time as an increase in pain. While the authors of this paper realize that serial neurological exams are not the most reliable evaluation, we feel that they were valuable for demonstrating improvement in the patient’s brachial plexopathy examination which demonstrated improvement and then a plateau followed by a sharp decline in the setting of no acute trauma.
Due to the subspecialists recommendations, we hypothesized that the development of the HO subsequently led to an impingement of the axillary nerve causing the patients sudden increase in pain and decrease in function without any traumatic event. For this reason, we elected to use the recommendations of a subspecialist and attempt an axillary nerve block at the quadrangular space which led to a moderate relief of symptoms. Due to the positive response to the injection, the patient will be referred to a specialist for possible excision of the HO to relieve the impingement of the axillary neurovasculature. While this is our hypothesis of what led to her decline after initial improvement and plateau of symptoms, we are unable to definitively state that the HO was the cause of her neurological change in symptoms. Because of this, we must also consider other possibilities such as the time to surgery, initial fracture, and brachial plexopathy that all could have contributed.
To our knowledge, this is the first reported case of HO of the axillary neurovasculature in the literature. As orthopedic surgeons, it is important for us to learn from this case in the sense that it provides additional evidence that HO is more common in the shoulder than was originally thought. Using this knowledge, it is important to evaluate x-rays not just for osseous abnormalities but also for changes in the soft tissue. In this particular case, a closer evaluation of the soft tissue may have led to an earlier recognition of the heterotopic bone formation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.