
Abstract
Background/Purpose
Fragility hip fracture (FHF) is the most prevalent fragility fracture, causing deterioration in ambulatory ability and disability. Early detection of patients who are at risk of prolonged hospitalization and functional decline after FHF is crucial as this facilitates post-operative management and healthcare resources allocation. Handgrip strength (HGS) is an easily-administered and cost-effective tool to assess whole body strength. The objectives of this study were to examine the relationship between pre-operative HGS, length of stay (LOS) and functional outcomes at 1-year follow up in patients with FHF in Hong Kong.
Methods
Patients aged 65 years old or above who were admitted to a local acute hospital from April 2017 to March 2020 due to FHF that were treated operatively, and subsequently attended the multidisciplinary fragility fracture clinic at 1-year follow up were evaluated. HGS measured at pre-operative physiotherapy initial assessment, post-fracture total LOS, Modified Functional Ambulation Classification (MFAC) and Elderly Mobility Scale (EMS) at 1-year follow up were retrieved for analysis. Correlation between HGS and LOS was analyzed using Pearson's correlation coefficient. Correlations between HGS and MFAC, and HGS and EMS were analyzed using Spearman's rank correlation coefficient.
Results
One hundred and nineteen patients (mean age = 80.8 ± 7.3 years) (33 males, 86 females) were evaluated. Statistical significant negative correlation between HGS and LOS was found (r = -0.245, p = 0.007), implying that the lower the HGS, the longer the period of hospitalization. HGS also showed statistical significant positive correlation with MFAC (r = 0.358, p < 0.001) and EMS (r = 0.507, p < 0.001), suggesting that the greater the HGS, the better the functional outcomes after 1 year. In short, pre-operative HGS measured by physiotherapists was shown to be associated with LOS and functional outcomes at 1-year follow up.
Conclusion
HGS is significantly associated with patient's LOS, MFAC and EMS after FHF. HGS is an easily-administered and cost-effective tool to facilitate frontline practitioners to determine and stratify patients’ rehabilitation potential and subsequently establish customized rehabilitation and discharge plan, such as intensive training, caregiver education and potential prediction of discharge destination.
Key Messages
HGS is significantly associated with patient's LOS, MFAC and EMS after FHF. HGS is an easily-administered and cost-effective tool to facilitate frontline practitioners to determine and stratify patients’ rehabilitation potential and subsequently establish customized rehabilitation and discharge plan.
Introduction
Fragility hip fracture (FHF) is one of the most prevalent and devastating kind of fragility fractures which associates with impaired functions and loss of long-term independence, causing economic burden.1,2 Approximately 30% of FHF patients suffered from significant deterioration in ambulatory ability while 20% to 40% were sent to old-aged home in view of persistent disability.1,3
Length of stay (LOS) is a healthcare resource utilization indicator. Long LOS implies intensive use of hospital beds and manpower, causing an increase in costs. Besides, LOS may pose negative impacts to both patient and staff experience. 4 Barriers of hospital discharge can be related to communication among members of the medical team and delays in decision-making or delays in discharge planning. 5 FHF accounted for more than 10% of hospital admission under the Department of Orthopaedics and Traumatology (O&T) in a local acute hospital in Hong Kong, Queen Elizabeth Hospital, over the past 5 years which caused a significant impact.
FHF is usually managed by surgical intervention. Post-operative rehabilitation is emphasized to optimize patient's functional performance. In spite of the implementation of early mobilization, multidisciplinary management and recent advancement of fracture liaison service, post-operative functional decline, complications and subsequent disabilities are still common in FHF patients. 6
Early detection of patients who are at risk of prolonged hospitalization and functional decline after FHF is crucial as this facilitates post-operative management and healthcare resources allocation. By predicting the rehabilitation potential in pre-operative phase, it enables practitioners to stratify the patients into different groups, set realistic rehabilitation goals, offer effective interventions, implement appropriate discharge plans and manage healthcare resources accordingly. 2
Handgrip strength (HGS) is an easily-administered, reliable and cost-effective tool to assess whole body muscle strength and function. 7 It is also used to measure frailty in elderly. According to the Asian Working Group for Sarcopenia (AWGS) consensus update in 2019 8 and the European Working Group for Sarcopenia in Older People (EWGSOP) revised consensus in 2019, 9 HGS remained an indispensable measurement for sarcopenia. However, few studies have shown that pre-operative HGS was associated with patients’ LOS.10,11 In the meantime, limited studies have investigated the relationship between HGS and long-term validated functional outcomes.12–14
The objectives of this study are to examine the relationship between pre-operative HGS, LOS and functional outcomes at 1-year follow up in patients with FHF in Hong Kong.
Methods
A retrospective study was conducted. All patients aged 65 years old or above who were admitted to a local acute hospital, Queen Elizabeth Hospital (QEH), in Hong Kong from April 2017 to March 2020 due to FHF that were treated operatively and subsequently attended the multidisciplinary fragility fracture clinic at 1-year follow up were evaluated. Subjects with repeated transferring history between acute and rehabilitation or convalescence hospitals were excluded.
All patients admitted due to FHF were enrolled into a fragility hip fracture clinical pathway, in which physiotherapy was included in the clinical management. Pre-operative physiotherapy assessment was performed within 24 h of admission, except those patients who were admitted in weekend or in holidays.
HGS was measured at pre-operative physiotherapy initial assessment and based on the protocol recommended by the American Society of Hand Therapists (ASHT), using the second handgrip position of the Jamar dynamometer. 7 The subject was instructed to squeeze the handle maximally and sustain for 3–5 s with shoulder adducted and neutrally rotated, elbow flexed at 90°, forearm in mid-prone and wrist in neutral to 30° extension, with neutral radioulnar deviation. Three successive measurements were taken for both dominant and non-dominant hands with a rest of 15–20 s between measurements. The maximum readings for both hands were recorded. 7 The maximum reading was selected to minimize the confounding factors from hand dominance, hemiplegia and physical constraints such as hand drip sites.
Total LOS which summated the acute and rehabilitation or convalescence LOS was captured from the Clinical Data Analysis and Reporting System (CDARS) of the Hospital Authority. Data with repeated transferal between acute and rehabilitation or convalescence hospitals was excluded to avoid outliners or prolonged LOS due to unstable medical conditions or lack of social support. 5
Upon discharge or early out-patient follow up, patients who opted for osteoporosis medication administration were referred to multidisciplinary fragility fracture (FF) clinic at 1-year follow up. Comprehensive physiotherapy assessment was conducted at the FF clinic, including Modified Functional Ambulation Classification (MFAC) 15 and Elderly Mobility Scale (EMS). 16 MFAC was used to categorize functional ambulation status, 15 while EMS was used to measure functional and physical performance of patients and reflect the level of independence. 16
Correlation between HGS and LOS was analyzed using Pearson's correlation coefficient. Correlations between HGS and MFAC, and HGS and EMS were analyzed using Spearman's rank correlation coefficient. All analysis was two-tailed and the level of significance alpha-value was set at 0.05 for statistical analysis.
Results
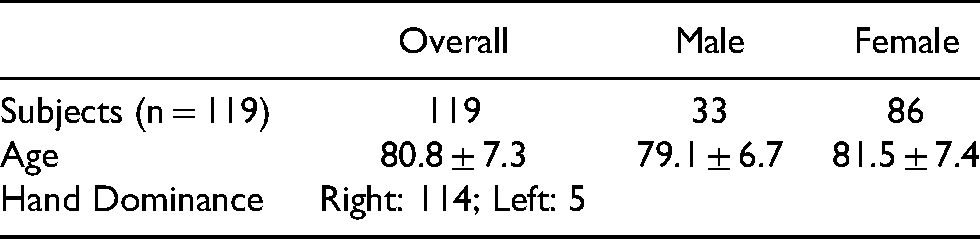
One hundred and nineteen patients (33 males, 86 females) were evaluated for data analysis (Figure 1). Their mean age was 80.8 ± 7.3 years old. Subjects' demographic and different outcome measures are shown in Table 1 and Table 2.
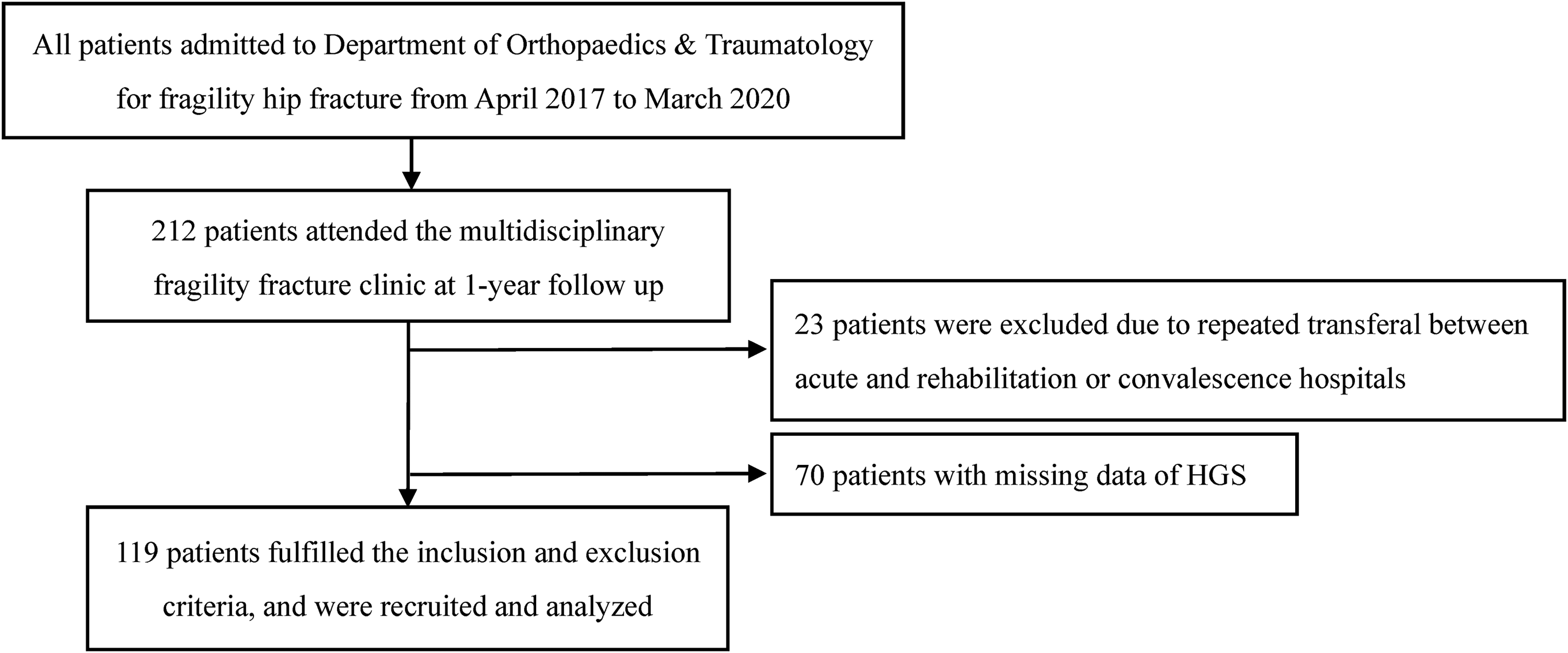
Flowchart of subject recruitment.
Subjects' demographic.
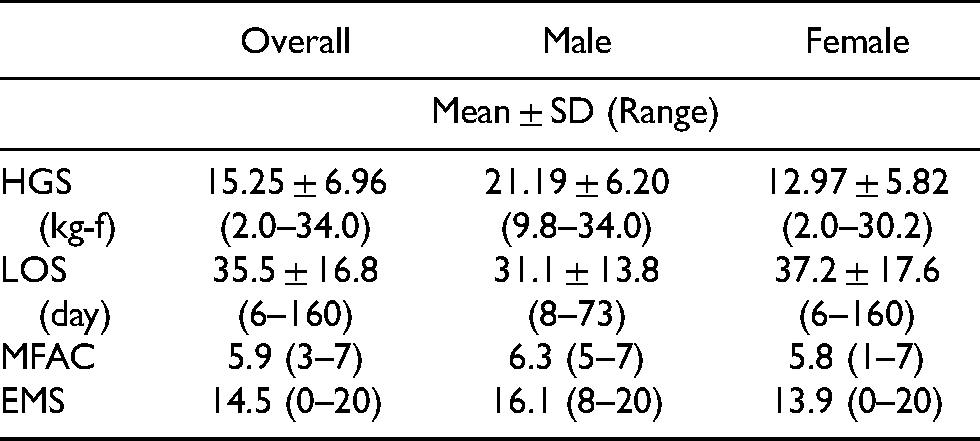
Different outcome measures in all subjects, male subjects and female subjects.
Statistically significant negative correlation between HGS and patient's LOS was found (r = -0.245, p = 0.007), implying that the lower the HGS, the longer the period of hospitalization. HGS also showed statistically significant positive correlation with MFAC (r = 0.358, p < 0.001) and EMS (r = 0.507, p < 0.001), suggesting that the greater the HGS, the better the functional outcomes after 1 year. In short, pre-operative HGS measured by physiotherapists was shown to be associated with LOS and functional outcomes at 1-year follow up (Figure 2).

Correlation of HGS and different outcomes. (a) Correlation between HGS and LOS. (b) Correlation between HGS and MFAC. (c) Correlation between HGS and EMS. *Correlation is significant at the 0.05 level; **Correlation is significant at the 0.01 level (2-tailed).
Discussion
HGS was known to correlate with different prognostic factors and to predict different aspects of outcome, in FHF patients in clinical practice, including age, gender, functional outcomes,12–14,17 nutritional status,10,18 pressure injuries 19 and mortality.13,20 This study also demonstrated that HGS was significantly correlated with total LOS and functional outcomes of FHF patients, implying that HGS assessment by physiotherapists in pre-operative period could provide important prognostic information to communicate with frontline physicians to determine and stratify patient's rehabilitation potential and subsequently establish customized rehabilitation and discharge plan, such as intensive training, caregiver education and potential prediction of discharge destination. 5
HGS was found to be negatively correlated with LOS. Our findings were similar to previous study that HGS could predict prolonged hospital stay in hospitalized patients. 10 Although reduced HGS did not provide satisfactory accuracy to identify malnutrition, HGS is a potential assessment to enhance nutrition assessment.10,18 However, clinicians or therapists should take note that malnutrition is associated with increased morbidity and clinical complications, higher risk of infections and mortality. 21 More importantly, enhancement in communication among members of the multi-disciplinary team could probably prevent delays in decision-making or discharge planning, which could further shorten the LOS of patients. 5
HGS was found to be positively correlated with MFAC and EMS. According to the published articles, it has been established that HGS is associated with long-term functional outcomes in FHF patients.13,14 HGS is one of the important indicators of sarcopenia and frailty. Sarcopenia or frailty in elderly would present with poorer functional outcomes in post-operative FHF patients.21–24 In addition, HGS shows strong correlation with post-operative early ambulation capacity with significantly fewer post-operative complications. 17 Early mobilization is essential to better long-term functional outcomes and recovery.
On the other hand, EMS was useful for classifying residential placements for elderly patients. 25 HGS was significantly correlated with EMS at 1-year follow up in our study. Therefore, early assessment on HGS could assist physicians to have earlier decision making and discharge planning even in the pre-operative period. 5
Limitation
Our study had some limitations. There were a proportion of patients excluded from our study due to both exclusion and attrition from the multidisciplinary fragility fracture clinic because of poor mobility (i.e. chair-bound or bed-bound cases), end-stage diseases such as organ failure or cancer, unwillingness to have follow up and etc. In addition, 23 patients were excluded due to repeated transferal between acute and rehabilitation or convalescence hospitals due to unstable medical conditions. Meanwhile, 70 patients with missing data of HGS were also excluded because of cognitive impairment or inability to follow commands for HGS assessment. All the forementioned factors probably contributed to potential selection bias. Therefore, the results of this study may be generalized to those relatively stable patients without cognitive impairment. Last but not least, clinicians or therapists should be reminded that HGS assessment should not be used solely to determine the patients’ rehabilitation pathway and discharge destination because functional outcomes of FHF patients are usually multifactorial in clinical practice.
Conclusion
HGS is significantly associated with patient's LOS, MFAC and EMS after FHF. HGS is an easily-administered and cost-effective tool to facilitate frontline practitioners to determine and stratify patients’ rehabilitation potential and subsequently establish customized rehabilitation and discharge plan, such as intensive training, caregiver education and potential prediction of discharge destination. Further studies are required to demonstrate the predictive effect of HGS on patients’ rehabilitation potential, long-term functional ability and discharge destination.
Footnotes
Acknowledgements
Physiotherapy Department, Queen Elizabeth Hospital and Department of Orthopaedics and Traumatology, Queen Elizabeth Hospital.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.