
Abstract
Introduction
Bone grafting is an important method of treatment in modern day's orthopedics. 1 Autologous bone grafting for the treatment of bone defects due to tumours, trauma or chronic infection is now a standard procedure. 2 Bone-healing properties of autologous bone grafts are very well established. The donor site should provide bone that is similar in histology to the recipient site and that can be readily shaped to fit. The donor site should also allow for simple and fast graft harvesting with a low risk of morbidity. 3 The anterior iliac crest is a good source of both cortical and cancellous bone. The medial or internal table of the ilium is a preferable site, owing to its easy accessibility and its low morbidity, especially when only cancellous bone is harvested. 4 The medial table has a thin cortical plate compared with the superior or lateral border of the iliac crest. The area of the lateral iliac crest where the medial gluteus muscle inserts is called the tubercle and here the cortical bone has a high density and thickness. This area is used when large amounts of cortical bone are needed. The disadvantage of harvesting bone from the superior or lateral border of the iliac crest is the interference with the insertion of the gluteus muscles and the inherent risk of gait disturbance. 5 Excessive amounts of bone harvested from the superior or lateral part of the iliac crest can also result in a change in appearance of the hip contour.
The purpose of this study was to evaluate the donor site morbidity and complications when harvesting bone from the outer cortex in the anterior iliac crest compared with those when harvesting bone from the inner cortex and by Wolfe Kawamoto method (table splitting technique) of the anterior iliac crest.
Method
The randomized, prospective and comparative study was conducted in LLRM Medical College, Meerut (Uttar Pradesh) from 2017 to 2018 on patients requiring bone grafting as a part of their treatment plan were included (delayed union and non-union of bone, patient requiring bone grafting as a primary method in treatment of their fractures and bone defect due to tumour, infection and patients aged between 18 and 70 years). Cases with the following findings were excluded: patient having previous iliac crest bone harvesting and patient having infection at the graft site. A total of 74 patients were treated out of which 14 patients were lost to follow up. So the sample size of 60 patients remained with us, which were analysed for final results. Informed written consent was taken from every patient. Patient biography, detailed history and clinical evaluation were done along with plain radiograph of the site that required graft. The subjects were divided into three study groups, each consisting of 20 patients. Telection of patients for each group was done randomly based on inpatient number. Group A consists of patients with bone graft from the outer cortex, group B consists of patients with bone graft taken from the inner cortex and group C consists of patients with bone graft taken by the table splitting technique.
Method of iliac crest bone graft harvesting technique
Skin incisions are the same for all approaches. Make an incision along the subcutaneous border of the iliac crest at the point of contact of the periosteum with the origins of the gluteal and trunk muscles, carry the incision down to the bone.
Table splitting techniques
The table splitting technique utilizes harvesting a full thickness graft by splitting the iliac crest obliquely both medially and laterally so that the edges of the crest may be re-approximated after the bone has been excised (Figures 1 and 2).
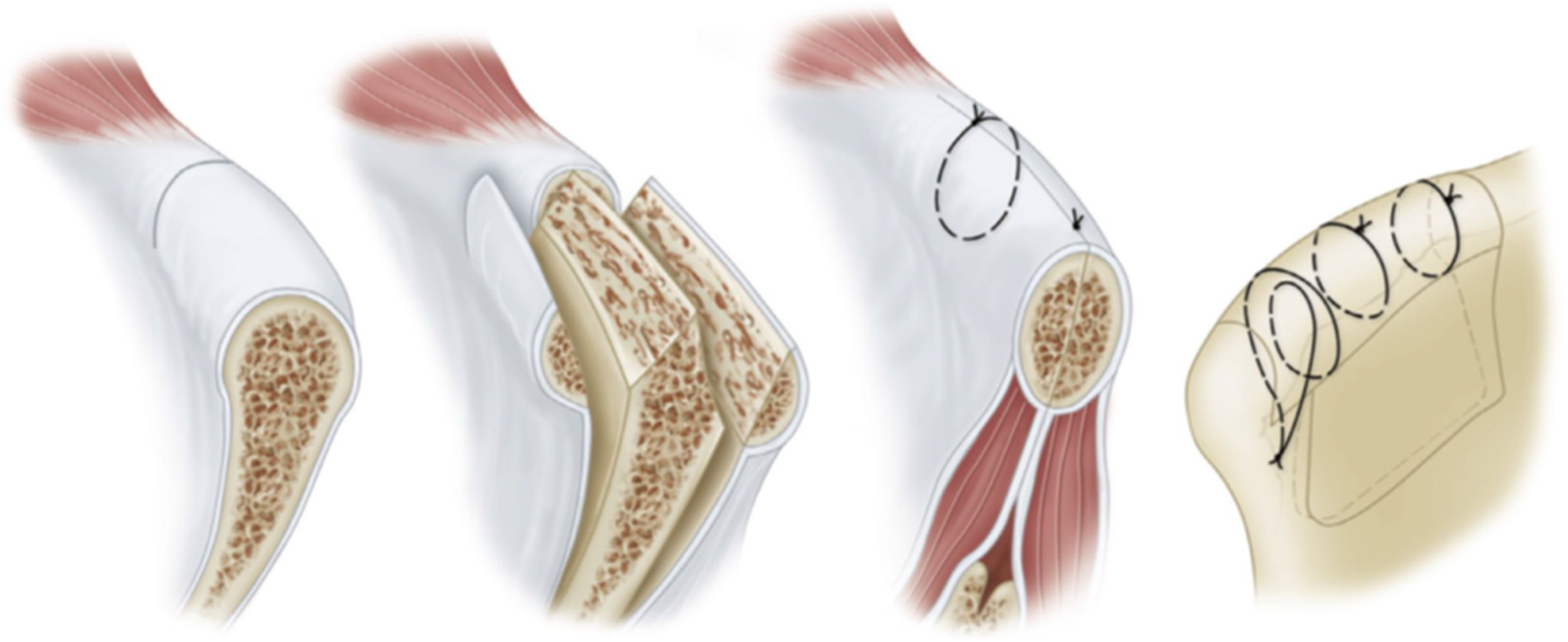
Table splitting technique.

Table splitting technique.
Graft from the outer cortex
It is harvested by exposing the outer table by sub-periosteal dissection of the gluteal muscle after outlining the area with an osteotome or power saw and the graft is peeled off by slight praying motion with a broad osteotome (Figure 3).

Outer cortex technique.
Graft from the inner cortex
Sub-periosteal dissection is done to expose the inner table and graft harvested in the same manner as of the outer cortex (Figure 4).

Inner cortex technique.
Post op follow up
The patients were followed up immediately on the next day after surgery, followed by scheduled appointments at post-op 2 weeks, at 6 weeks, at 3 months, at 6 months and at 1 year. The visual analogue scale (VAS) was used for pain assessment and an additional pre-tested pre-validated questionnaire was administered for assessment of other co-morbidities.
Results
The age wise distribution of study participants showed that majority of them were in the age group of 31 to 50 years. The mean age of the study group was 42.9 ± 11.7 years (mean ± s.d.) and range = 20 to 70 years.
Table 1 presents the morbidity patterns observed in study subjects in all comparison groups. Overall, the most common morbidity observed was pain (measured by VAS) and almost 100% subjects experienced some kind of pain at various follow-ups. After pain, numbness was the other most common morbidity. Among numbness, the majority was temporary numbness and only 2 patients experienced chronic long-term (possibly permanent) numbness at the end of 1 year follow-up. The incidence of numbness was least in the table splitting group, followed by the inner cortex group and then the outer cortex group (p < 0.05). The next common morbidity observed was abnormal gait (p < 0.05) and most patients got corrected by the end of 6 months.
Morbidity.
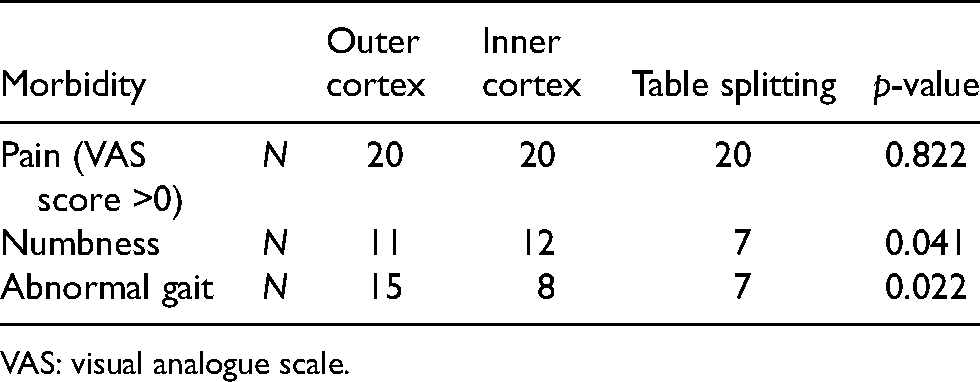
VAS: visual analogue scale.
Table 2 shows post-operative complications in the graft site. Overall, the post-operative complications seemed to be very infrequent and only 4 patients encountered post-operative infection, 1 patient had hematoma and 3 patients had itching at the surgical site. This shows that the post-operative level of care was excellent in all the three groups. None of the complications were statistically significant in the comparison groups (p > 0.05).
Post-operative complications.

Table 3 shows a post-hoc comparison revealed that the significant difference was observed between the outer cortex and the inner cortex at 2-week follow up, between outer and inner cortex and between outer cortex and table splitting at 6 week follow up and between outer cortex and inner cortex at 3 month follow up (p < 0.05).
Post hoc comparison.
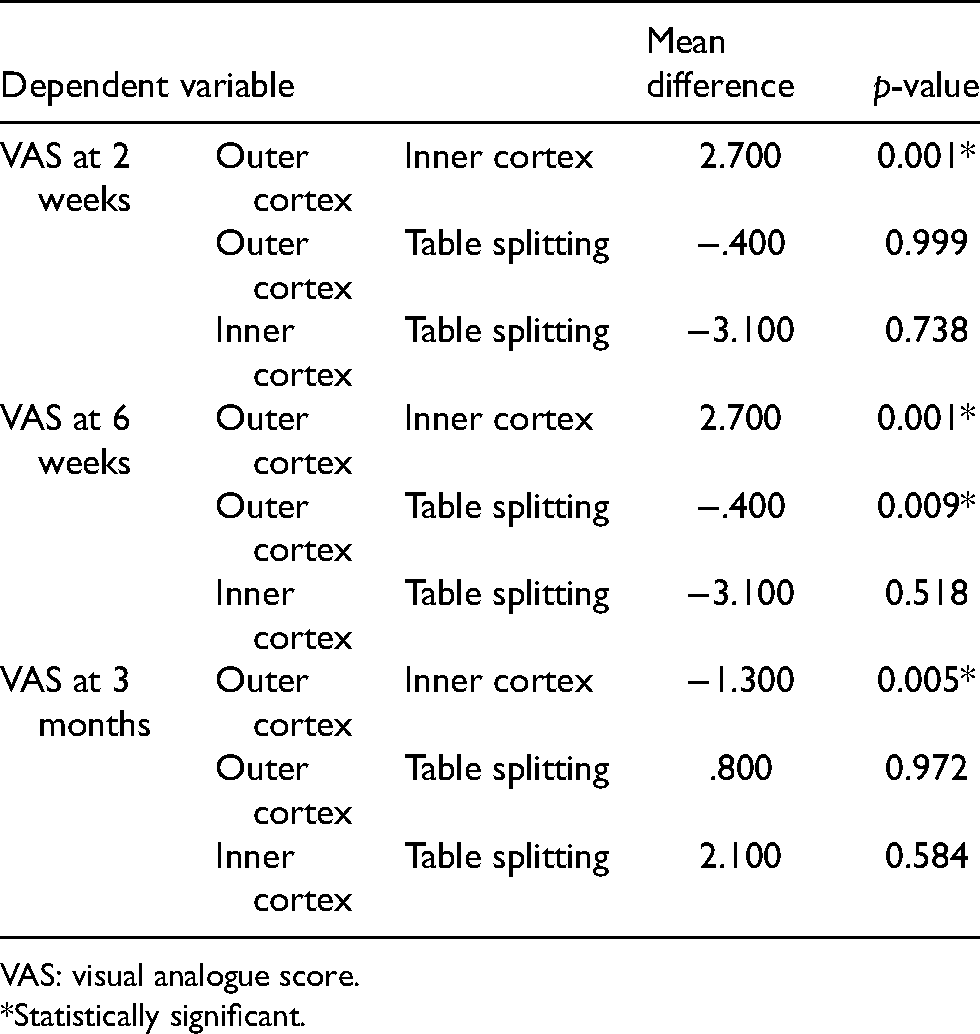
VAS: visual analogue score.
*Statistically significant.
Table 4 shows the abnormal gait pattern among study population and its comparison among study groups. Out of a total of 20 subjects in each group, the highest percentage of abnormal gait individuals was seen in the outer cortex group, followed by the inner cortex group and then the table splitting group in most of the follow-ups. A statistically significant difference was seen at baseline, 2 weeks, 3 months and at 6 months of follow up, where the table splitting group had a significantly lower number of abnormal gait individuals as compared to other groups (p < 0.05).
Abnormal gait among study groups.

Table 5 shows the numbness at thigh and over scar among the study groups. A significant difference was observed only at 6 months and 1 year follow up. At 6 months follow up, maximum numbness was seen in the outer cortex group and at 1 year, maximum numbness was seen in the inner cortex group (p < 0.05).
Numbness at thigh.
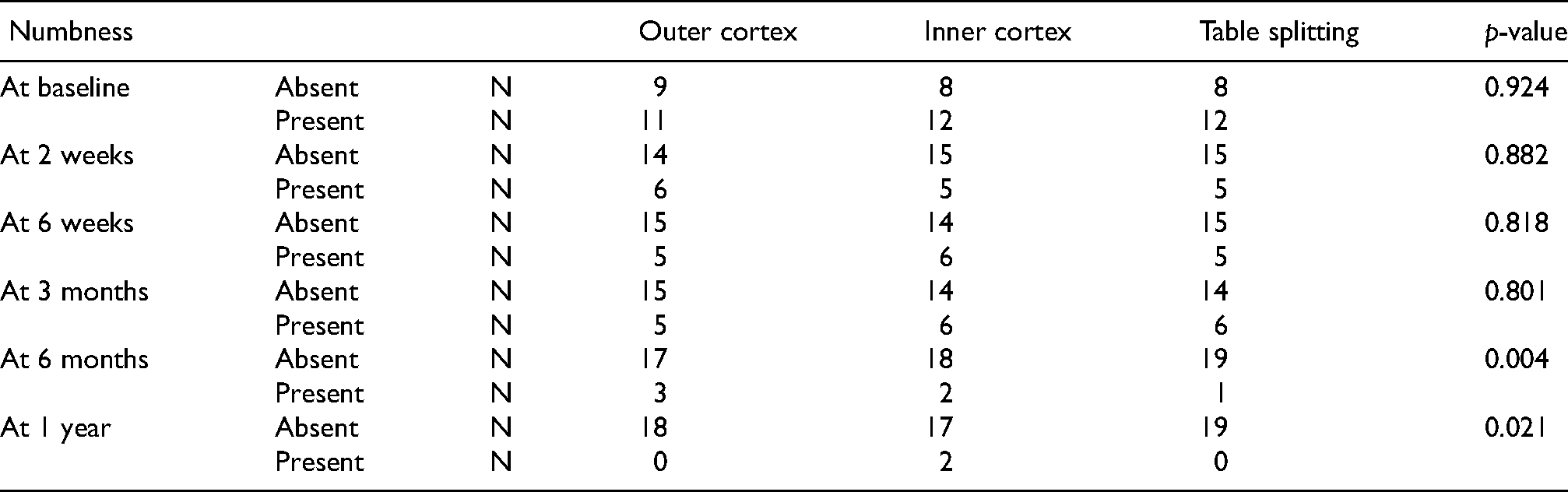
Table 6 shows the comparison of other parameters among study groups. There were no significant difference in scar satisfaction among comparison groups, although the outer cortex group had the highest score (p > 0.05). Also, the table splitting group had the maximum surgery time as compared to other groups. The post-hoc comparison revealed significant difference in all groups (p < 0.05).
Other parameters.

Discussion
Autologous bone grafts harvested from the iliac crest are commonly used in reconstructive orthopedic surgery. Autologous bone is used to help promote bone healing and to provide structural support for reconstructive surgery. 6
However, there are potential complications in obtaining graft from iliac crest, including chronic pain, infection, hematoma, incisional hernia, fracture and disturbed sensation. Due to the associated morbidity, the optimal donor technique for harvesting autogenous bone graft remains open to debate.7,8 Therefore, the present study was undertaken. The iliac crest is the most common donor site because of its easy access, low morbidity and availability of large quantities of both cortical and cancellous bone. Cortical bone is used mostly for fixation, while cancellous bone is needed for osteogenesis.
There were little differences in harvest-site pain between different techniques used in our study, though it averaged around 0.67 (iliac crest). The post-operative pain was minimized to a great extent by the end of 1 year, which is consistent with the study done by Kukreja et al. 8 reported pain in the donor site in the early post-operative period (up to 3 months, included in the temporary group) in 5 patients (8.9%). Only one patient (1.8%) had residual donor site pain at 6 months. 9
Donor site pain is one of the most frequent complications associated with iliac crest bone grafting (ICBG) and almost 100% subjects experienced some kind of pain at various follow-ups. Donor site pain was evaluated using VAS, a common measure to assess the pain. Donor site pain is caused due to nerve injury or destabilization of the muscular origin at the time of harvest. 10 Chronic pain at the donor site is probably unavoidable in a small number of patients. Chronic pain often has a psychosomatic component and therefore may not be entirely under control of the surgeon.
Gait disturbance is one of the most common complications observed next to pain and numbness. 11 Gluteal gait is a persistent type of dragging of the lower limb caused by extensive stripping of the lateral surface of the ilium with weakening of the attachment of the gluteal musculature and fascia lata. 12
In addition, clicking produced by the fascia lata slipping suddenly over the greater trochanter in walking has also been reported. 13 The gait disturbances in each group were comparable at baseline, 2 weeks 6 weeks and 3 months (nearly one-third) in the present study. This could be attributed to pain at the donor site post-operatively in all the three groups. In a study conducted by Rawashdeh, 14 no patient showed gait disturbance 1 month postoperatively. However, in a study conducted by Baqain et al., 15 50% of the patients had gait disturbances even after 14th postoperative day.
Nerve injury is a common complication associated with iliac bone grafting. Damage to the nerves adjacent to the ilium most likely results due to direct transaction or excessive traction. As these nerves are sensory in nature, the characteristic symptoms include pain, paresthesia, numbness and dysesthesias in the distribution of the affected nerve. In our study, 6 patients continued to have numbness at 6 months and 1 year follow up. A study of 205 cadaveric specimens found that 9.9% of nerves had an aberrant course and were vulnerable to injury following anterior iliac crest graft harvesting. 16 Palmer et al. 16 and Schaaf et al. 17 also reported 3% and 22.7% sensory disturbances, respectively. It is reported that the risk of nerve injury is significantly higher in cases, in graft where deeper than 30 mm is harvested. As for the length of the graft, the incidence was 20% when the graft was 45 mm long or more 16% when it was 30 mm or more and 8% when it was <30 mm long. We should therefore carefully consider the size of the graft, which is required, before harvesting.
Scar satisfaction in the present study had an overall good score, ranging mostly above 85 in all patients. The difference between comparison groups regarding scar satisfaction was statistically non-significant (p > 0.05). Scar satisfaction is a subjective feeling and it depends on various factors such as socio-economic status, gender and other local factors at the site of operation. Further exploration is suggested in this regard.
Also, the inner cortex group had the least surgery time while the table splitting group had the longest. No particular studies could be found in this regard, however, a similar study conducted by Mirovsky and Neuwirth 18 showed that in an intra-osseous method, less bone is harvested and longer duration of surgery is required compared with that of the outer table method.
In our study a very low rate of post-operative infection and hematoma formation were observed. This rate of minimal post-operative complications may be due to the use of a proper technique, haemostasis, and antibiotic coverage. Overall, the post-operative complications seemed to be very infrequent, and only 4 patients encountered post-operative infection, 1 patient had hematoma and 3 patients had itching att surgical site. This shows that the post-operative level of care was excellent in all the three groups. None of the complications were statistically significant in the comparison groups.
Infection is a complication that is seen in all surgeries at one time or another. Infections can be superficial and require only antibiotics or be more extensive and require surgery. Schulhofer and Oloff 19 presented a series of 40 patients who underwent ICBG and described a hematoma and infection as their only complication.
Complications that are related to blood loss have also been reported. Hematomas are seen with any type of iliac crest bone harvests there are no different in that regard. 20
Conclusion
From the current findings, we conclude that few differences do exist in harvest-site morbidities between different techniques used in our study. Overall, the most common morbidity observed was pain and almost 100% subjects experienced some kind of pain at various follow-ups. After pain, numbness was the other most common morbidity. Among numbness, the majority was temporary numbness. The incidence of numbness was least in the table splitting group, followed by the inner cortex group and then the outer cortex group. There was no significant difference regarding scar satisfaction among comparison groups. However, the table splitting group had the maximum surgery time while the inner cortex group had the minimum. Given its low morbidity, bone harvesting by table splitting appears to be a very good option when reconstructing bone defects. Overall, the post-operative complications seemed to be very infrequent, showing that the post-operative level of care was excellent in all the three groups.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.