
Abstract
Introduction
Maltracking of the patella is a key contributor to early failure of patellofemoral arthroplasty (PFA). Native femoral trochlear morphology dictates implant rotation and patella tracking of in-lay PFA implants. This is the first study amongst Asians designed to assess the normal rotational alignment of the trochlear groove and evaluate its implication on PFA implant choice and position.
Methods
Trochlear inclination angle (TIA) was measured from 211 magnetic resonance images of Asian knees retrieved from a single centre in Hong Kong. TIA assesses rotation of the femoral trochlear groove relative to the axis perpendicular to Whiteside’s line (anteroposterior axis of the femur).
Results
The mean trochlear inclination in normal Asian knees was 11.5° ± 2.5° (mean ± standard deviation) internal rotation. High-grade dysplastic knees, according to Dejour classification, were significantly more internally rotated with a mean of 12.8° ± 3.6° (p = 0.025).
Conclusion
Trochlear inclination in Asians is comparable to Caucasians. In-lay PFA implants do not alter native pathological bony trochlear anatomy, and may result in patella maltracking in patients with high grade trochlear dysplasia or excessive trochlear inclination. These patients may benefit from on-lay implants, which allows restoration of normal trochlear inclination, as well as lateralisation and deepening of the trochlear groove. Patella tracking is however, dynamic and multi-factorial. Further clinical studies are therefore warranted to reconcile our anatomical findings with clinical outcomes.
Keywords
Introduction
Isolated patellofemoral joint osteoarthritis (PFJOA) is an unique entity accounting for 15% patients suffering from knee osteoarthritis. 1 It has been shown to be a different disease process than tibio-femoral osteoarthritis, and is associated with trochlear dysplasia in up to 75% patients, as well as patella instability and maltracking. 2 Despite purported advantages of unicompartmental patellofemoral arthroplasty (PFA) for treatment of isolated end-stage PFJOA, such as lower blood loss, earlier recovery as well as bone and cruciate ligament preservation, 3 total knee arthroplasty (TKA) is often favoured over PFA due to inconsistent results and historically high failure rates of PFA.4–7 According to registry data, revision rate for PFA has been reported to be up to 27–45% at 15 years post-operation.4,5 Increasing evidence suggests, however, that failures are often accounted for by poor patient selection, as well as shortcomings of first-generation “in-lay” implants. 8
First-generation in-lay resurfacing PFA implants replace worn cartilage without altering underlying subchondral bone. Rotational alignment of the implant is thus dependent on the native anatomy of the femoral trochlea. Second-generation on-lay anterior-cut PFA implants replace the anterior compartment of the knee entirely. Rotational alignment of the implant is typically, similar to anterior femoral cuts demanded of TKR, determined by the surgeon according to the femoral condylar reference plane of choice, the transepicondylar, Whiteside's or posterior condylar line 9 (Figure 1). Contrary to on-lay implants, in-lay implants are rendered unable to correct the underlying, often dysplastic, trochlear anatomy, resulting in malrotation 10 (Figure 2). Similar to a malrotated TKR femoral component, an excessively internally rotated PFA trochlear component predisposes to patella maltracking by medialising the trochlear groove, increasing Q angle as well as increasing tension over the lateral retinaculum. 11 Recent studies reporting mid-term outcomes have found that PFA revision rates are comparable to TKR when on-lay implants alone are used, with some authors reporting 95–100% survival at 5 years post-operation.12–17 Better outcomes have been observed in patients with underlying trochlear dysplasia, patella instability and meticulous exclusion of tibiofemoral osteoarthritis.18–22
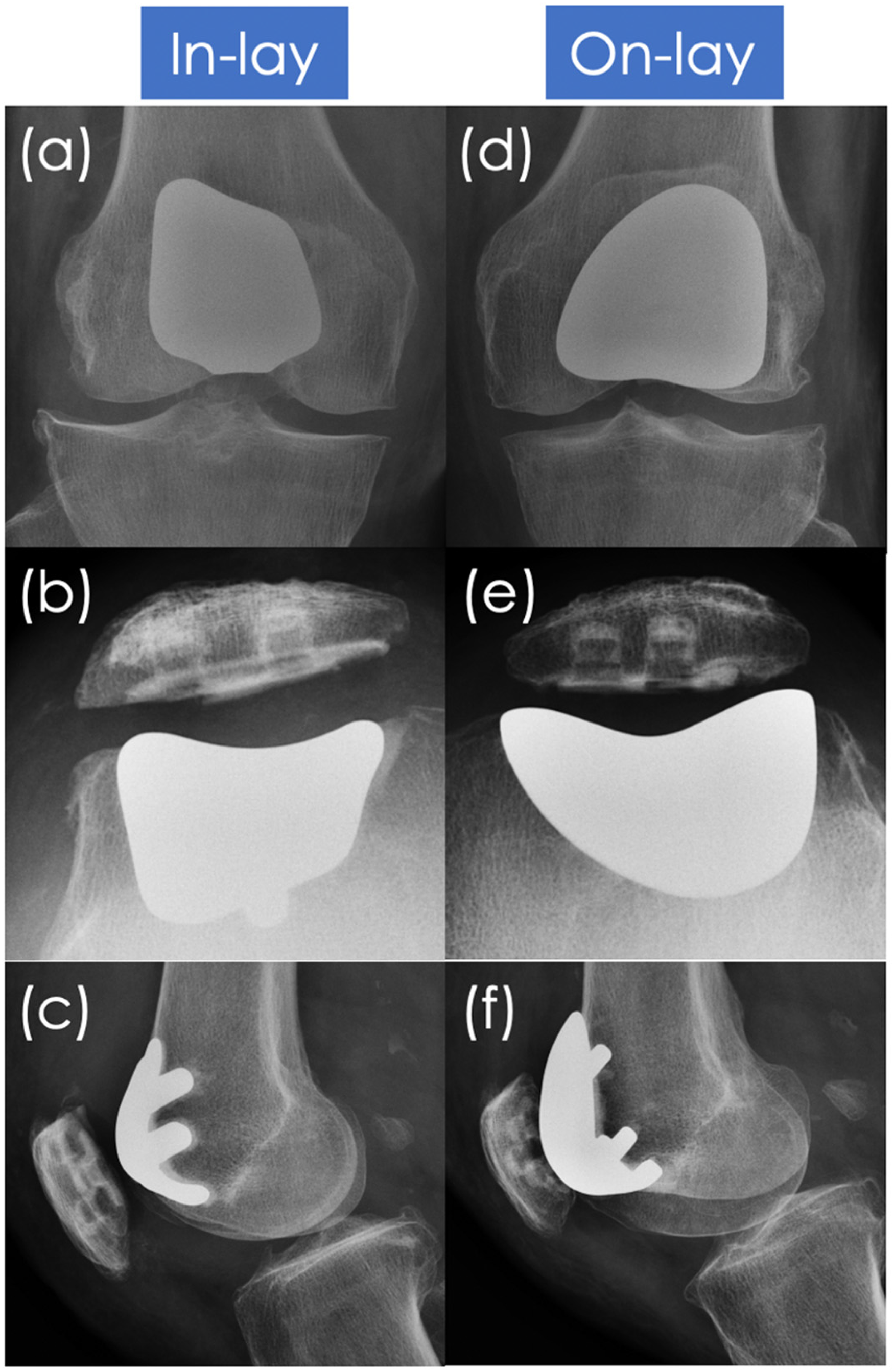
Post-operative bilateral knee radiographs of a patient with right sided in-lay PFA performed (a–c), and left sided on-lay PFA performed (d–f).
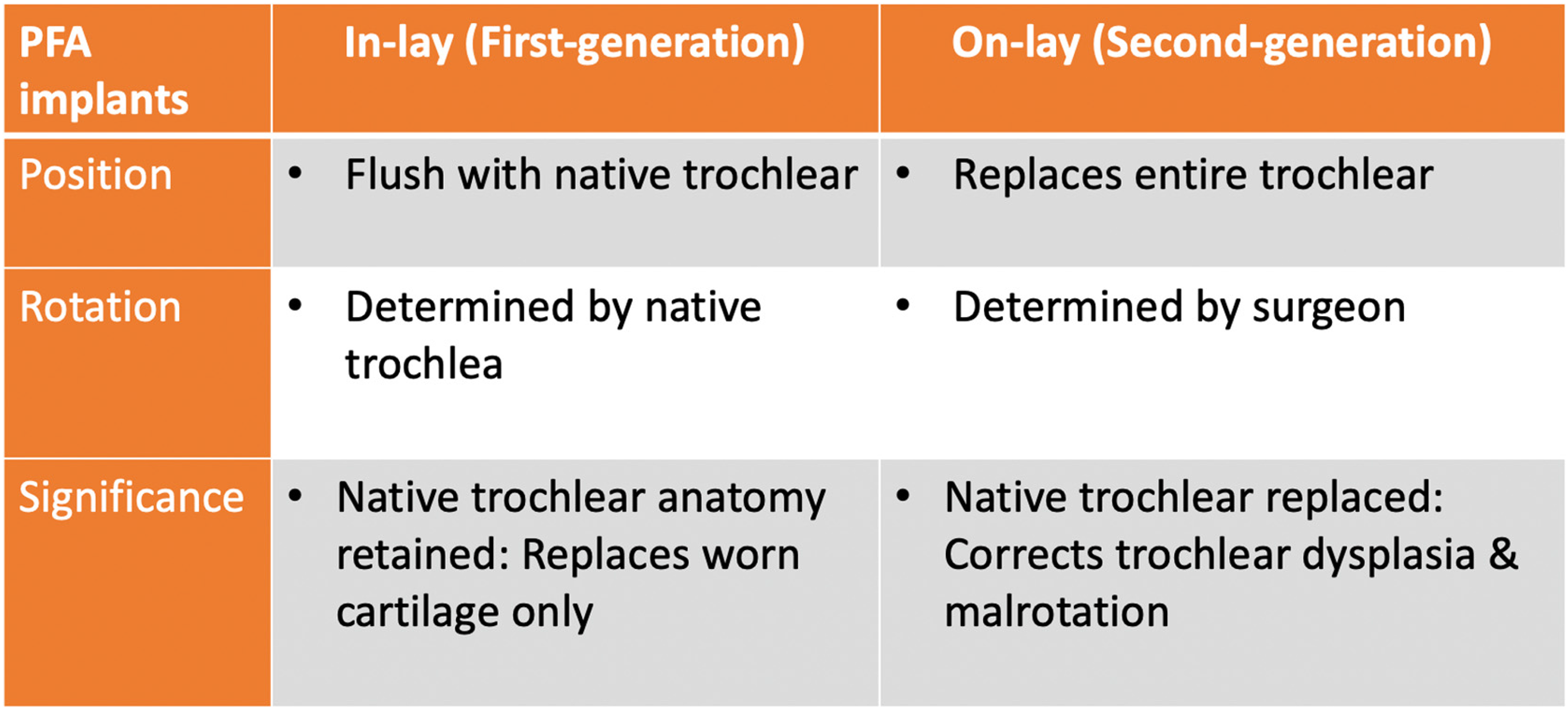
Table illustrating differences between in-lay and on-lay PFA implants.
It has been established in literature that the native femoral trochlear carries an inclination of 11.4° internal rotation relative to the axis as perpendicular to Whiteside's line in Caucasians, 23 and that there are anatomical differences in lower limb axial alignment between Caucasians and Asians that can influence the rotation of arthroplasty components. 24
We therefore attempted to assess the average rotation of the femoral trochlea in normal Asian knees via the trochlear inclination angle (TIA), evaluate for variation among normal and dysplastic knees, gender and age, as well as gauge whether our findings inform us of the decision between using in-lay or on-lay PFA implants. To our knowledge, this is the first attempt in literature to establish normal values for trochlea rotation in Asians. We hypothesize that variation in TIA exists, which is of concern as excessive internal rotation may result in patella maltracking among in-lay implants.
Methods
We conducted a single centre retrospective review of knee magnetic resonance imaging (MRI) for all patients referred to a joint replacement centre in Hong Kong for acute traumatic knee injury requiring subsequent arthroscopic intervention, from January 2013 – December 2019. 242 consecutive patients with available MRI were identified. 24 were excluded due to age < 18, 7 were excluded due to Caucasian descent. Paediatric patients were excluded from the study, as trochlear dysplasia typically presents during adolescence. 25 Of the 211 subjects remaining (age range 18–51 years, mean 28.6 years), all suffered from cruciate ligament injury, either anterior or posterior, with or without associated meniscal or collateral ligament injury, and were asymptomatic prior to injury. None suffered from fractures. 173 patients were male (82%, age range 18–51, mean 28.6 years) and 38 were female (18%, age range 18–57, mean 28.3 years). 19 patients were aged 40 or above (9%), 192 were aged younger than 40 (91%) (Figure 3).
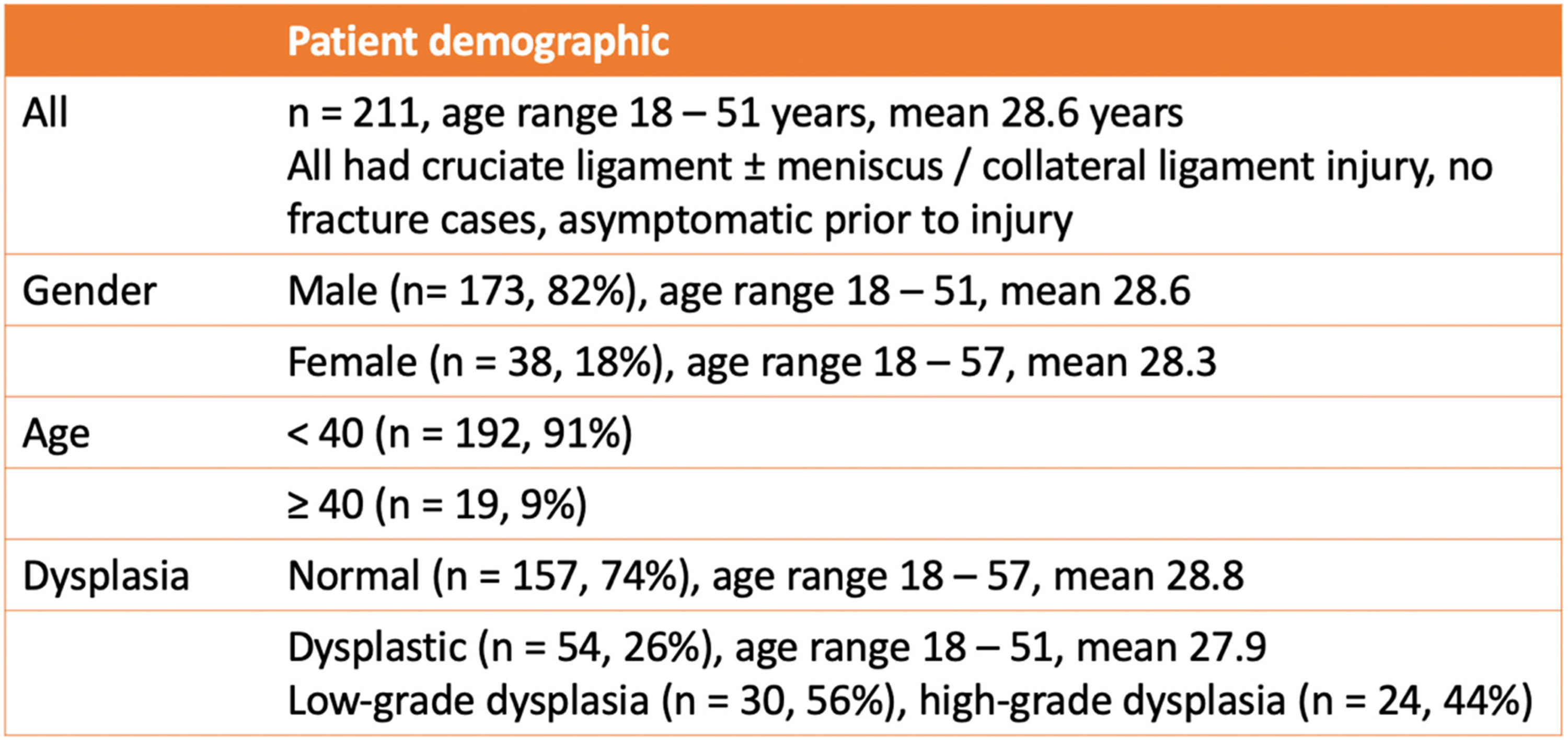
Table illustrating demographic of 211 study subjects.
Plain MRI was obtained in a non-weight bearing knee in full extension with 3 mm cuts. Fat saturated proton density-weighted sequence was selected for interpretation.
Knees with trochlear dysplasia were classified according to Dejour's two-grade classification validated for axial MRI,26–28 which defines Dejour Type A knees as those with “low-grade” dysplasia, and Dejour Type B, C and D knees as those with “high-grade” dysplasia, on the first craniocaudal axial MRI cut demonstrating the complete cartilaginous trochlea (Figure 4). 54 knees with trochlear dysplasia were identified (26%, age range 18–51, mean 27.9), with the remaining 157 being “normal” knees without trochlear dysplasia (74%, age range 18–57, mean 28.8). 24 knees were found to have high-grade dysplasia (44%), and 30 knees were found to have low-grade dysplasia (56%).
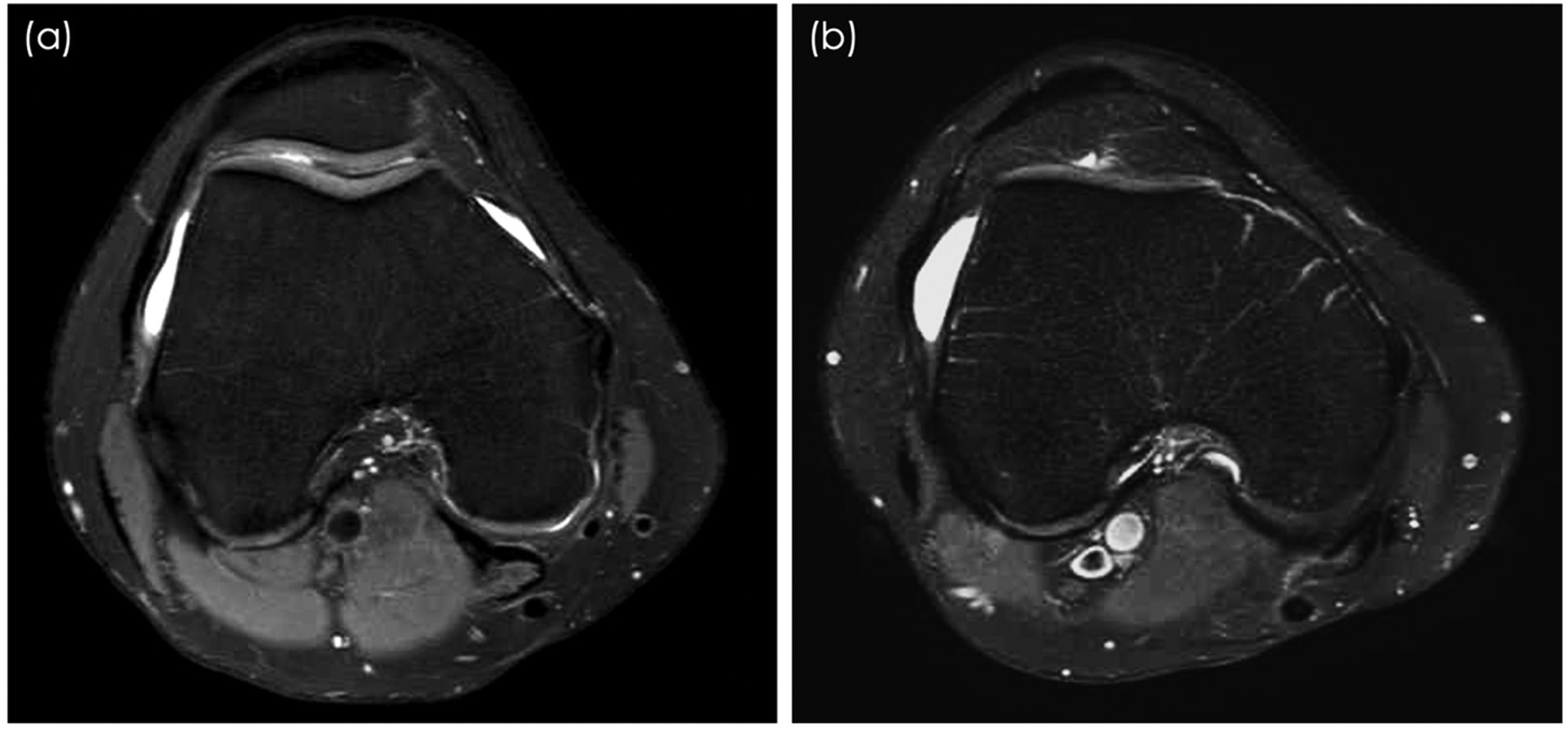
Magnetic resonance images (MRI) of a patient's right knee with low-grade trochlear dysplasia as evidenced by a shallow trochlea with sulcus angle > 145° (ie Dejour type A) (a). Another MRI of a second patient's right knee with high-grade trochlear dysplasia, as evidenced by a flat trochlea (ie Dejour Type B) (b). Other features suggestive of high-grade trochlear dysplaisa as defined by Dejour include medial femoral hypoplasia (ie Dejour Type C) and cliff pattern (ie Dejour Type D).
Rotation of the femoral trochlea was determined by measurement of the trochlear inclination angle, according to protocol established by Kamath. 23 TIA was defined as the angle between the line perpendicular to Whiteside's line (anteroposterior axis of the femur), 29 and the line joining the most anterior points of the medial and lateral femoral condyles. The axial MRI cut demonstrating the maximum height of the lateral femoral condyle was selected for interpretation (Figure 5). Such points were chosen as they are expected to reflect the most anterior position of the trochlear prosthesis when using an in-lay implant. Measurements were obtained first with cartilage landmarks (intermediate signal intensity on MRI) and repeated with underlying subchondral bone landmarks (high signal intensity on MRI).
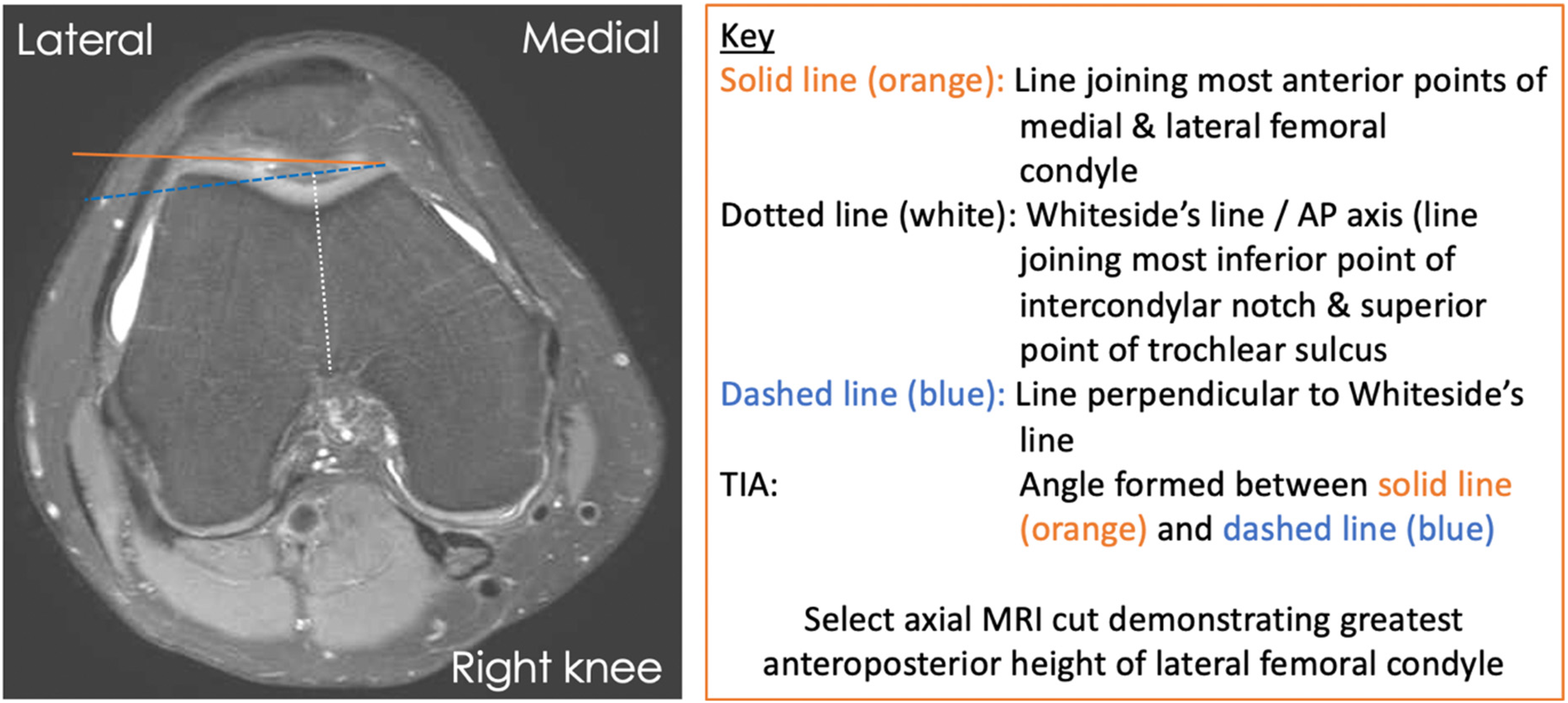
Schematic representation of trochlear inclination angle measurement on axial MRI using cartilage landmarks according to protocol established by Kamath.
Values were obtained independently by two observers, both orthopaedic residents. Studies were interpreted twice by the first observer within a 4-week time span after random re-arrangement. The independent sample Student t tests was used to compare the trochlear inclination angles among normal and dysplastic knees, knees of different gender, as well as knees of different age groups, with significance set at p < 0.05. Subgroup analysis comparing high and low grade dysplastic knees with normal knees was performed using ANOVA with LSD correction, with significance set as p < 0.05. Statistical analysis was performed using SPSS version 26.0 (SPSS, Inc, Chicago, Ill). Inter-class and intra-class correlation coefficients were determined for reliability of measurements made between the two observers, and within the first observer respectively.
Results
The average femoral trochlear rotation as determined by the TIA in normal knees (n = 157) was 11.5° ± 2.5° (mean ± standard deviation) internal rotation when cartilage landmarks were used, and 10.3° ± 2.4° internal rotation when bony landmarks were used, relative to the axis perpendicular to Whiteside's line (anteroposterior axis of the femur). None of the trochlea were neutral or in external rotation.
Dysplastic knees (n = 54) were found to be more internally rotated when compared to normal knees when cartilage landmarks were used (12.3° ± 2.9° vs. 11.5° ± 2.5°, p = 0.048), and also when bony landmarks were used (11.2° ± 2.7° vs. 10.3° ± 2.4°, p = 0.018) (Figure 6). Subgroup analysis showed no significant difference in rotation between knees with low grade dysplasia (n = 30) and normal knees with cartilage (11.9° ± 2.2° vs. 11.5° ± 2.5°, p = 0.395), and without cartilage (11.1° ± 2.3° vs. 10.3° ± 2.4°, p = 0.125) (Figure 7). However, knees with high-grade dysplasia (n = 24) demonstrated significant higher degree of internal rotation with cartilage (12.8° ± 3.6° vs. 11.5° ± 2.5°, p = 0.025), and without cartilage (11.5° ± 3.2° vs. 10.3° ± 2.4°, p = 0.036) (Figure 8).
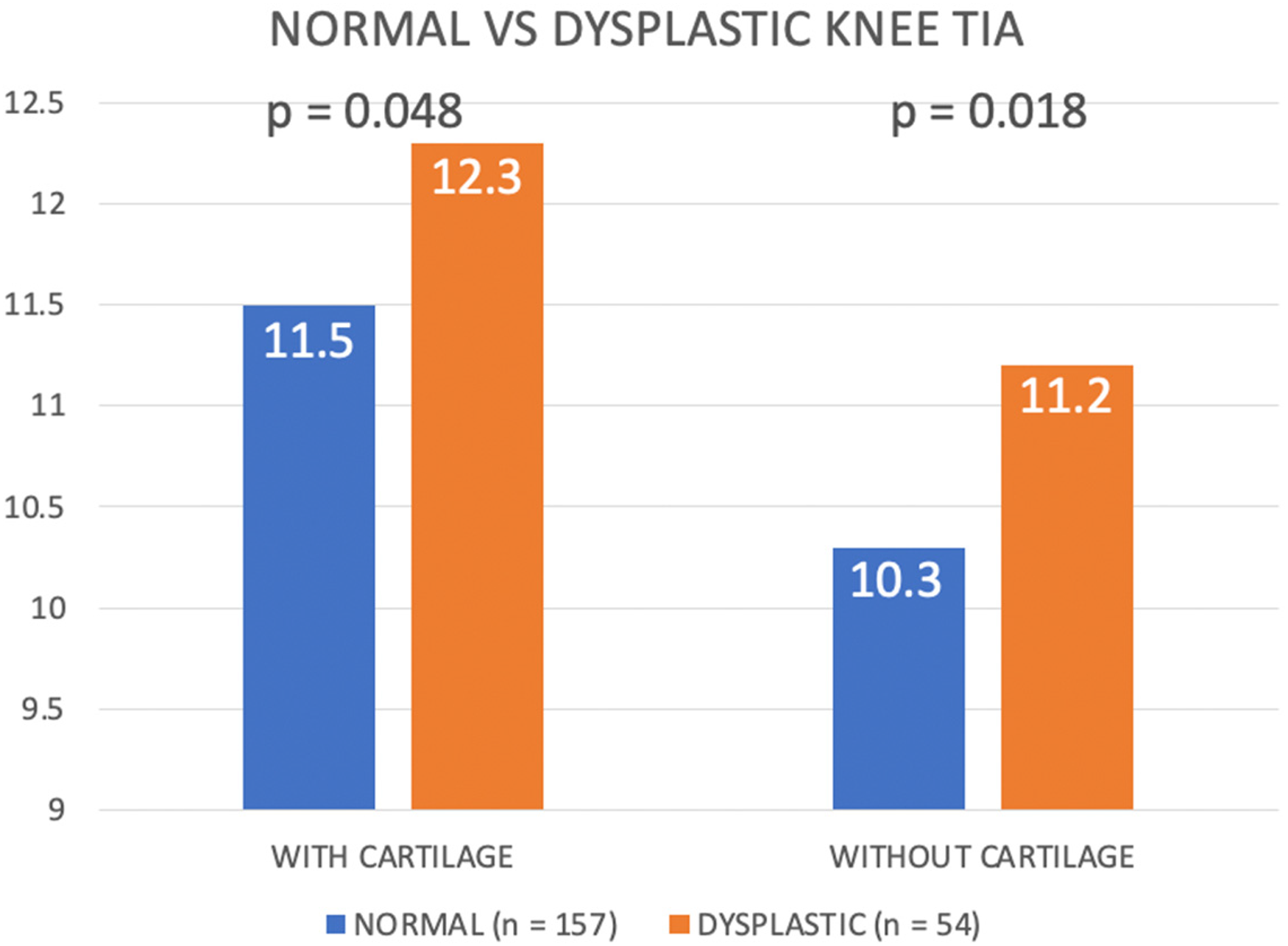
Comparing trochlear inclination angle among normal and dysplastic knees.
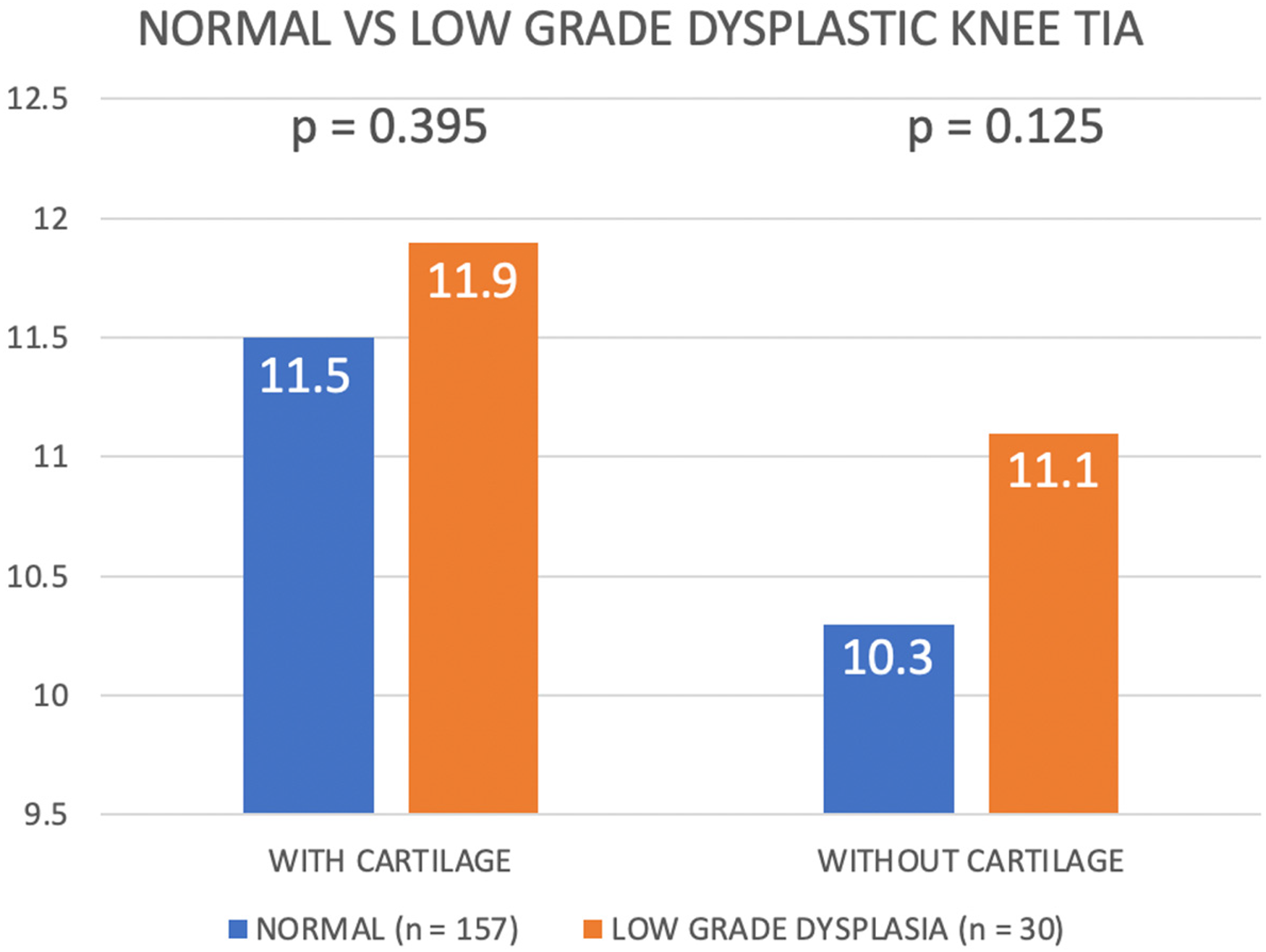
Comparing trochlear inclination angle among normal and low-grade dysplastic knees.
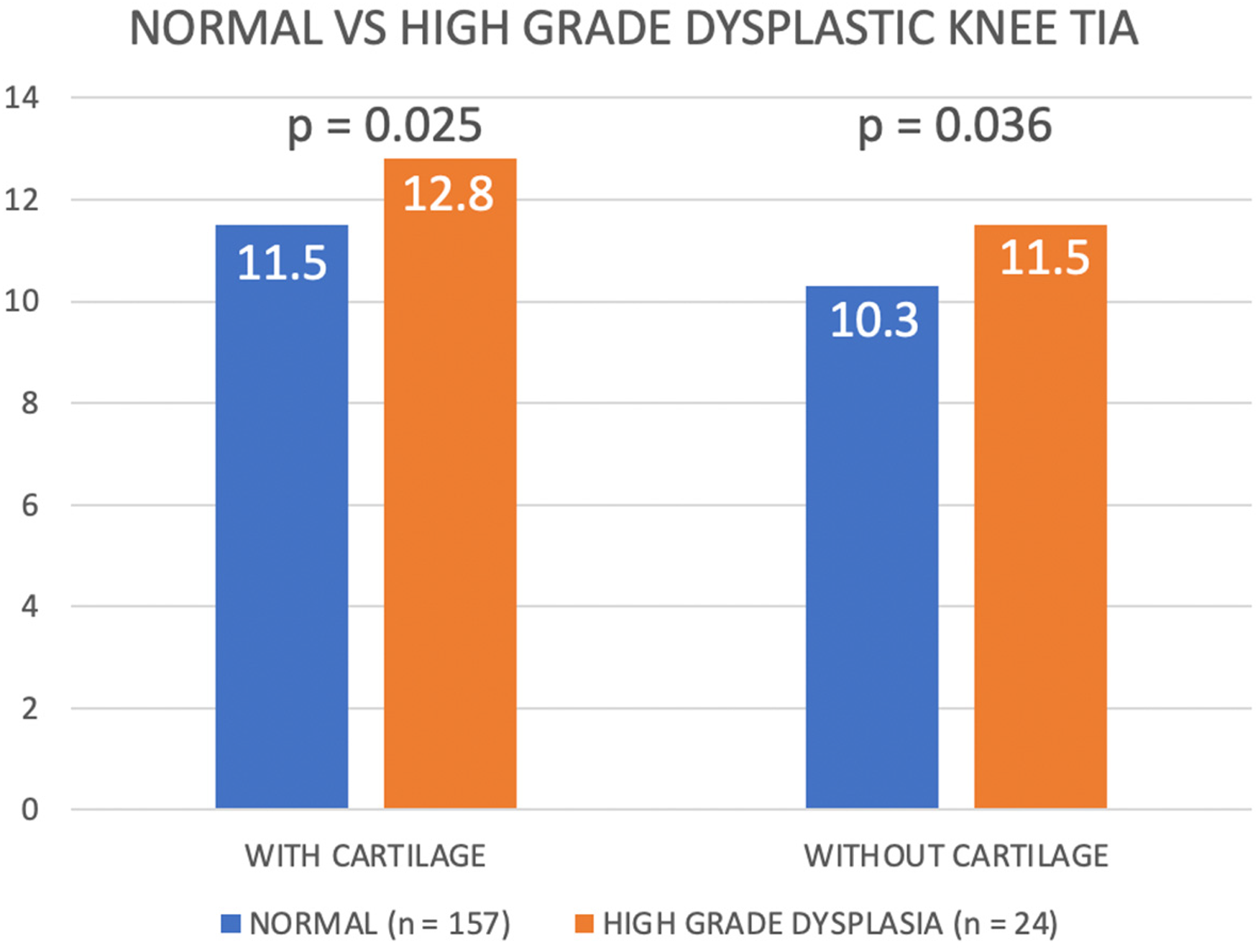
Comparing trochlear inclination angle among normal and high-grade dysplastic knees.
There was no significant difference in average TIA between male (n = 173, 82%) and female (n = 38, 18%) patients with cartilage (11.5° ± 2.4° vs. 12.5° ± 3.4°, p = 0.092), and without cartilage (10.4° ± 2.3° vs. 11.4° ± 3.3°, p = 0.064). The average TIA in patients younger than 40 (n = 192, 91%) and aged 40 or above (n = 19, 9%) did not differ significantly with cartilage (11.8° ± 2.7° vs. 10.8° ± 2.5°, p = 0.120), and without cartilage (10.7° ± 2.5° vs. 9.5 ± 2.8°, p = 0.053).
Overall, the average TIA was significantly greater when cartilage landmarks were used as compared to bony landmarks (11.7° ± 2.7° vs. 10.5° ± 2.5°, p < 0.001) (Figure 9).
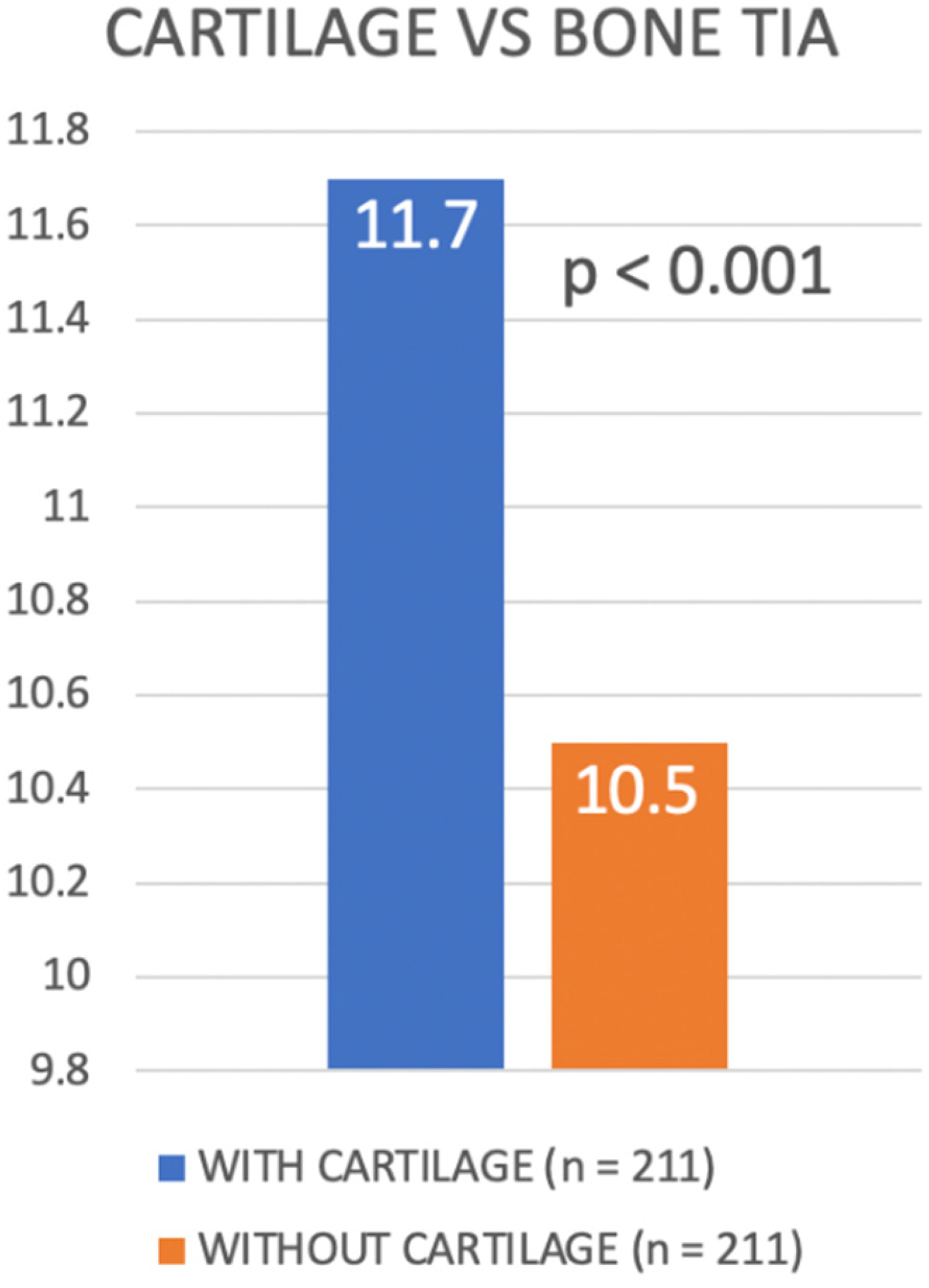
Comparing trochlear inclination angle using cartilage landmarks for assessment with subchondral bone landmarks.
The intraclass correlation for average measures was excellent at 0.933 when using cartilage landmarks (95% confidence interval 0.912–0.949), and 0.918 when using bony landmarks (95% confidence interval, 0.893–0.938). The interclass correlation for average measures was also excellent at 0.913 when using cartilage landmarks (95% confidence interval: 0.781–0.966), and 0.898 when using bony landmarks (95% confidence interval: 0.741–0.959).
Discussion
Patellofemoral arthroplasty was first conceptualised by McKeever in 1955 for treatment of isolated patellofemoral joint osteoarthritis, followed by the advent of first-generation in-lay implants in the 1970s and second-generation on-lay implants in the 1990s.3,30 Evolution of in-lay implants have also made robotic arm assisted PFA available in today's market. Observational data has shown that patients undergoing PFA have significant lower mean blood loss and hospital stay in comparison to TKR. 7 One randomized controlled trial also found better range of motion and patient reported quality of life in the PFA group at 2 years post-operation, while another found comparable outcomes and complication rates at 1 year post-operation.16,17 However, registry data from Australia and the United Kingdom have documented PFA failure rate to be up to 27–45% at 15 years post-operation.4,5 It is clear that while PFA demonstrates promise in the management of isolated PFJOA, the question remains; how do surgeons achieve more predictable and consistent outcomes?
Normal patella tracking within the patella groove is primarily dependent on the medial patellofemoral ligament in early flexion, and on the bony lateral trochlear facet in later flexion. 31 Patients with PFJOA are often found to have unbalanced patella soft tissue stabilisers or trochlear dysplasia. An ideal PFA trochlear component should therefore provide adequate normal trochlear depth, as well as realign the extensor mechanism to normalize patella tracking.2,32
In her review of causes of failure in PFA, Strickland found that those failing early were attributed to pain (29%), mechanical reasons (6%) and infection (1%), while late failings were due to progression of tibiofemoral osteoarthritis (53%). 3 Another meta-analysis found higher odds of revision and re-operation for in-lay PFA implants when compared to on-lay implants, with on-lay implants demonstrating no significant difference in re-operation, revision, pain or mechanical complications when compared to TKR. 33 This implies that more stringent patient selection and use of on-lay implants for appropriate patients may address early PFA failures that are mostly technical in nature. This demands meticulous exclusion of tibiofemoral disease pre-operatively or intra-operatively, and selection of patients with trochlear dysplasia and history of patella instability, which have been shown by observational data to yield superior post-operative outcomes.18–22
Our study found an average trochlear inclination of 11.5° relative to the axis perpendicular to Whiteside's line in Asians, which is comparable to Kamath's finding of 11.4° among Caucasians. 23 We also found that knees with trochlear dysplasia, specifically high-grade dysplasia, were prone to a greater mean TIA of 12.8°. Rotational alignment of on-lay PFA implants is determined by the surgeon, while that of in-lay implants is dictated by the native anatomy of the femoral trochlear. As knees prone to PFJOA are often dysplastic, 2 we postulate that use of in-lay implants in patients with excessive trochlear inclination will result in trochlear component internal malrotation, medialising the trochlear groove and encouraging patella maltracking. An on-lay implant allows the surgeon to determine ideal implant rotation, and correct other dysplastic features such as a shallow trochlear groove, in order to mitigate complications arising from patella maltracking. We propose taking into account the trochlear inclination in PFA surgery, by positioning an on-lay implant such that a normal range of trochlear inclination can be restored after accommodating for variation in inclination among different implant designs. 34 We also propose routine pre-operative axial imaging, in the form of computed tomography (CT) or MRI, to facilitate surgeons in patient selection by identifying patients with trochlear dysplasia, and in surgical planning by allowing comparison of the existing TIA with normal values for intra-operative correction. Parameters such as tibial-tuberosity to trochlear groove distance (TTTG) may also be quantified, which informs the surgeon whether a concomitant osteotomy of the tibial tuberosity to realign the extensor mechanism is necessary. 35 One should however, be aware of the discrepancy in the anatomy of the cartilaginous femoral trochlear with underlying subchondral bone on CT and MRI, which has been well established in literature, and once again substantiated in our findings.25,36,37
Contrary to our study, Kamath was unable to find a difference in trochlear inclination angle between normal knees and dysplastic knees. 23 The discrepancy may be accounted for by the different means employed to identify patients with trochlear dysplasia. Kamath utilised lateral knee radiographs, while our study examined axial MRI. Although the four type Dejour classification was originally developed for lateral knee radiographs, Dejour subsequently updated his classification to accommodate axial CT as well as MRI, ultimately concluding that a 2-grade analysis (low-grade vs. high-grade) on axial MRI yielded best intra-observer and inter-observer correlation.26–28 True lateral knee radiographs are also difficult to obtain, and often underestimate the severity of trochlear dysplasia.
As a retrospective analysis, a shortcoming of our study stems from difficulty in sampling a normal population which would have had knee MRI performed. Though all subjects were asymptomatic prior to acute traumatic knee injury, they all suffered from cruciate ligament injury. While there is limited evidence in literature suggesting a direct causal relationship between cruciate ligament injury and PFJOA, anterior cruciate ligament (ACL) injury is associated with a higher incidence of trochlear dysplasia than the normal population, though the underlying pathology is still yet to be elucidated. 38 Risk factors for ACL injury such as global joint hypermobility and genu valgum are also shared in patients with trochlear dysplasia and patella maltracking.39–41
Furthermore, due to inter-operator differences, there was capacity for non-uniform leg position during MRI. Leg abduction or adduction during imaging is expected to alter the position of the most anterior points of the medial and lateral femoral condyles selected to measure TIA. 42 Consistent with Kamath's definition of TIA, Whiteside's line was also selected for measurement of TIA, although there has been criticism in literature that it may be more difficult to identify in dysplastic knees due to a poorly defined trochlear trough when compared to the transepicondylar axis. 43
Lastly, we recognise the limitations of this purely anatomical study. While we are able to postulate the implications of an excessively internally rotated femoral trochlea, we are unable to determine the clinically relevant upper limit for malrotation in trochlea inclination that precludes in-lay PFA implant use, nor whether restoring trochlear inclination to a normal range with on-lay implants in patients with trochlear dysplasia will correlate clinically with improved outcomes. Patella maltracking is also dynamic and multifactorial. While internal rotation and medialisation of the trochlea groove is expected to contribute to patella maltracking, other causes of increased Q angle (excessive femoral anteversion, excessive external tibial torsion, genu valgum), patella dysplasia, patella alta, as well as dynamic quadriceps activity are also relevant in the decision between in-lay and on-lay PFA implant choice, and have not been controlled in this study. 44
Conclusion
We conclude that the mean femoral trochlear inclination in normal Asian knees is 11.5° ± 2.5° of internal rotation, with high grade dysplastic knees being more internally rotated. This is the first attempt in literature to establish normal values in Asians, and our findings are comparable to established values for Caucasians. Pre-operative axial imaging, in the form of CT, and particularly MRI, allows accurate assessment of TIA and facilitates surgical planning. Patients found to have excessive trochlear inclination or high grade trochlear dysplasia may consider on-lay PFA implants to correct the TIA, lateralise, and deepen the trochlear groove. In-lay PFA implants do not alter native pathological bony trochlear anatomy, and may result in patella maltracking in these patients. While trochlear anatomy was explored in this study, patella tracking is multi-factorial and dynamic, with soft-tissue and bony contributors that have not been accounted for in this study. Further comparative clinical studies are warranted to reconcile our anatomical findings with clinical outcomes, in the pursuit for more consistent and reliable PFA outcomes.
Footnotes
Acknowledgements
The authors would like to acknowledge Mr Gene Chi Wai Man for his contribution to statistical analysis.
Authors’ contributions
All authors participated in the conception and execution of the study. JCHF, SYCW and YWH supervised the study. MKLL and KCHL measured radiological parameters and participated in data collection. MKLL participated in data analysis. MKKL prepared the manuscript. All authors read and approved the final manuscript.
Availability of data and materials
The datasets used or analysed during the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
This study was conducted with ethics committee approval (Clinical Research Ethics Committee CREC reference number 2021.295, submission reference number NTEC-2021-0242).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.