
Abstract
Elective Total Hip Replacement (THR) surgery is one of the most common elective surgeries in the UK, costing the National Health Service (NHS) over £300,000,000 annually. A review of the literature identified preoperative rehabilitation, known as ‘prehabilitation’, improves patient outcomes and decreases Length Of hospital Stay (LOS). This approach follows NICE guidelines which recommend prehabilitation for all patients undergoing joint replacement surgery.
Challenges accessing prehabilitation classes at UK hospitals due to inadequate transport and COVID-19 restrictions present an opportunity to provide prehabilitation virtually. Physiotherapy services are increasingly utilising technology, in line with The NHS Long Term Plan to increase service accessibility.
A review of the literature has established virtual prehabilitation is effective, feasible, and preferable for patients. Quality Improvement methodology has been used to propose an implementation plan for a virtual prehabilitation service. Further research is required to create a standardised prehabilitation protocol, and to assess the long-term effects and sustainability of virtual prehabilitation.
Keywords
Introduction
Total Hip Replacements (THR) are one of the most common elective surgeries in the UK, with 52,816 performed in 2019–20. 1 Costs for the average elective THR surgery are £6,571, with an average hospital length of stay (LOS) of 3–5 days and a cost of £406.63 for each excess bed day.2,3 These costs are higher than the average elective surgery, which costs £3894 and £346 per excess bed day.3,4 Excess bed days for elective surgery cost the NHS £5.4bn per year. 4
Traditionally Physiotherapy for elective THR patients is only provided post-operatively, however evidence suggests this alone does not result in functional improvements or shorter LOS. 5 It has been established that pre-operative rehabilitation, known as ‘prehabilitation’, is necessary to improve patient outcomes. 5 Patients who undertake prehabilitation have better functional outcomes and shorter LOS.6,7
Patients awaiting elective THR surgery are at risk of deconditioning (loss of skeletal muscle due to inactivity) which results in poorer physical function and extended LOS.8,9 COVID-19 restrictions, plus suspension of elective surgeries to focus NHS resources on the pandemic, have further increased this risk. 9 Prior to the pandemic prehabilitation compliance for orthopaedic patients was low (47%), often due to difficulties accessing hospitals. 10 Good patient outcomes but poor compliance suggest it is essential a suitable method of prehabilitation delivery is established.
Virtual Physiotherapy provision is a developing area which has become prominent in recent years. 11 In the UK the shift to virtual service provision following the COVID-19 pandemic aligns with the NHS Long Term Plan, and it is likely virtual services will remain after social distancing restrictions have been lifted.12,13 The introduction of virtual prehabilitation is proposed to transform UK elective THR services. This paper provides an overview of the literature and proposes an implementation plan, using quality improvement methodology to ensure a structured approach.
Literature review
To establish an evidence base for the introduction of virtual prehabilitation a combined population, intervention, comparison, outcome (PICO) search was completed (Table 1).
PICO combined search.
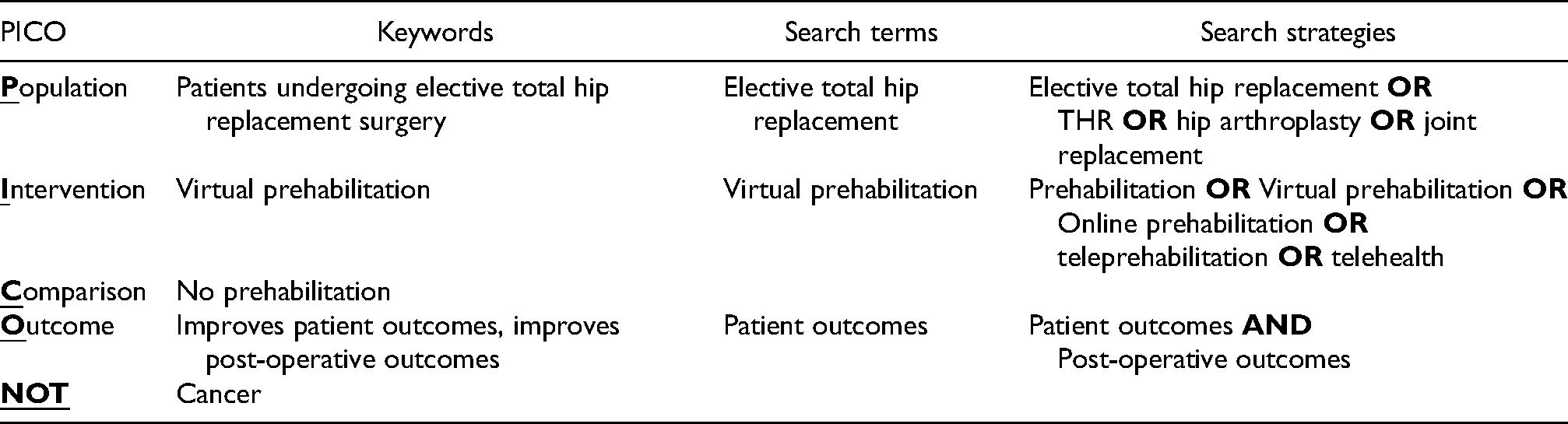
LOS was hypothesised to be an important outcome; however, this did not yield adequate results. Subsequently the outcome element of the PICO search was amended to focus on patient outcomes. LOS was often included as a secondary outcome measure in the literature, so this data is included, although to a lesser extent than anticipated.
The literature search was undertaken on 28th July 2021 on the University of Lincoln databases which comprise 238 databases including PubMed, CINAHL, and PEDro. 14 The following search strings were used:
(“Elective total hip replacement” OR [MeSH Terms] “THR” OR “hip arthroplasty” OR “joint replacement”) AND (“prehabilitation” OR [MeSH Terms] “virtual prehabilitation” OR “online prehabilitation” OR “tele-prehabilitation” OR “telehealth” [All Fields]) AND “patient outcomes” [MeSH Terms] OR “post-operative outcomes” [All Fields]); NOT (“Cancer”) [All Fields].
515 studies were retrieved, and limiters applied to narrow results. The publication date was limited from 2016 onwards. Although this may bias results towards recent publications rather than papers with long-term impact, this is appropriate given the rapid changes in service provision following the COVID-19 pandemic. 13 Only papers published in English were selected due to the language capabilities of the reviewer. Once duplicates were removed articles were then screened based on title and abstract, with 9 suitable for inclusion.
Whilst searching the literature it became apparent few papers addressed both prehabilitation and virtual service provision. In order to gain a thorough understanding of the evidence base it was decided to relax the inclusion criteria to incorporate papers that addressed either prehabilitation or virtual service provision. It is anticipated this deficit in the literature will be addressed imminently due to the impact of COVID-19. 13 This review considered secondary sources, as well as primary sources, to ensure a comprehensive appraisal of the literature.
The flow diagram in Figure 1 provides full details of the literature search and is based on the updated PRISMA 2020 statement. 15
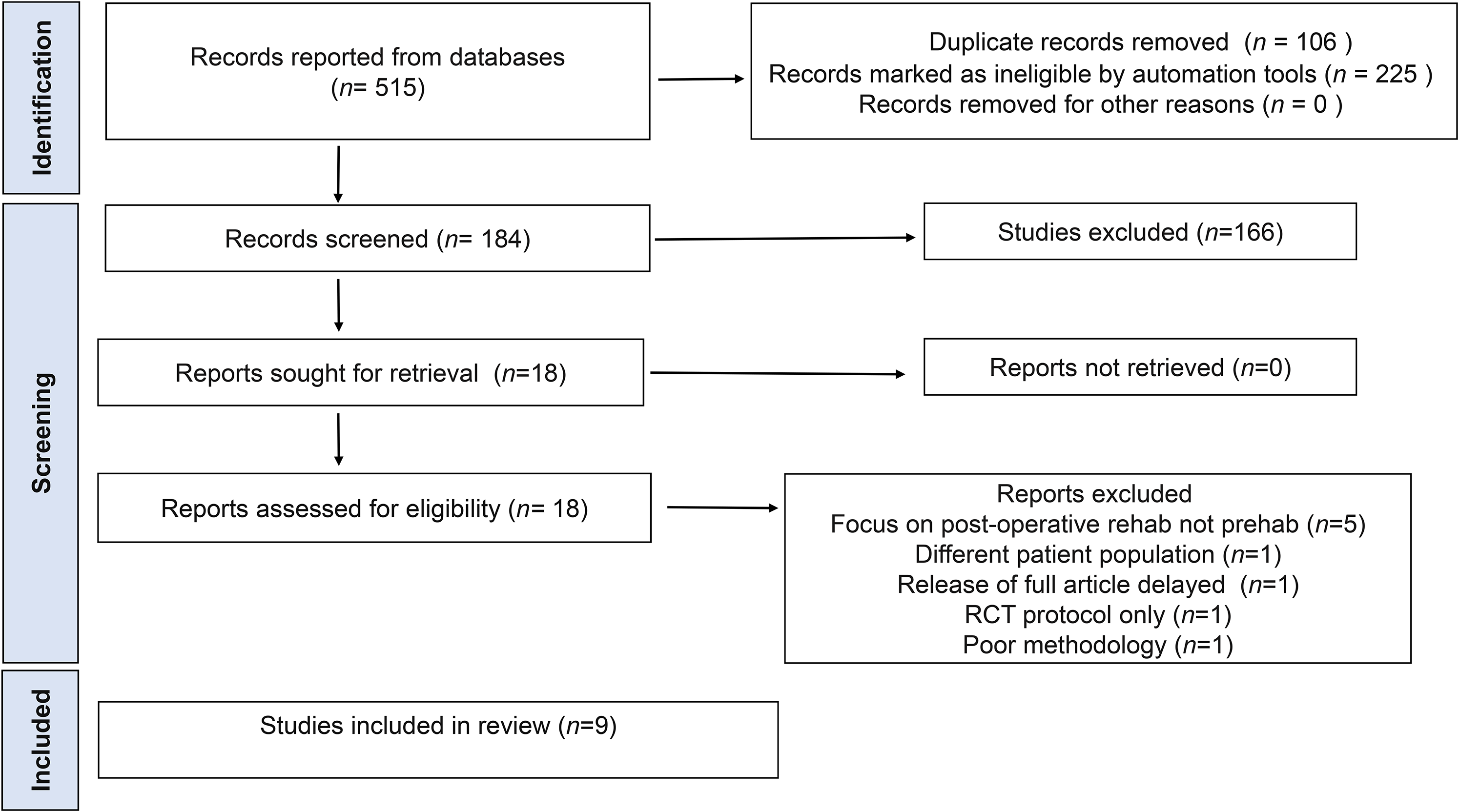
PRISMA flow diagram of study selection.
Quality of studies
Evidence quality was assessed by determining the level of evidence (LOE) and assigning a grading of recommendations, assessment, development, and evaluations (GRADE quality rating.16,17 (Table 2)
Quality of evidence.
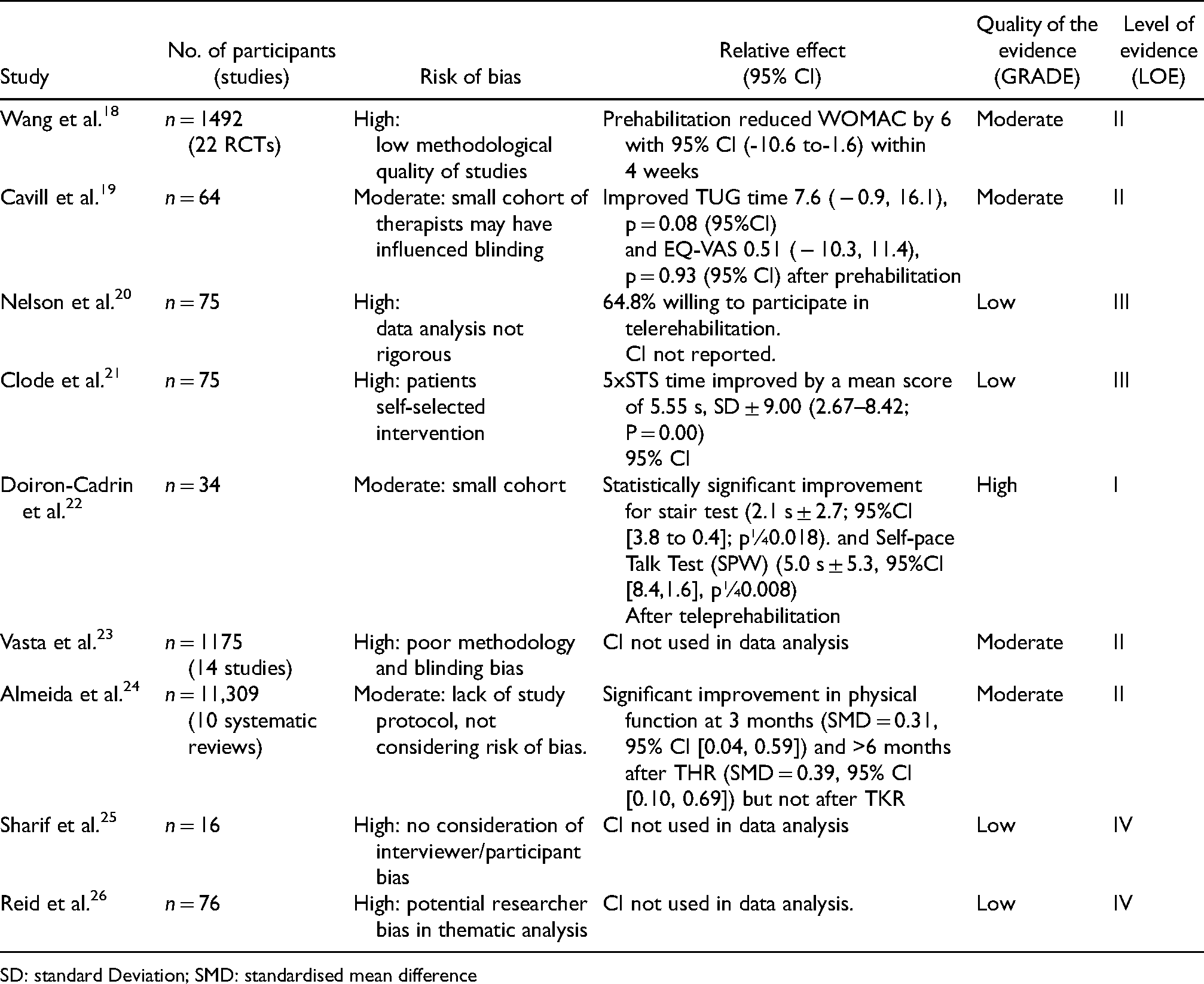
SD: standard Deviation; SMD: standardised mean difference
Demographic data
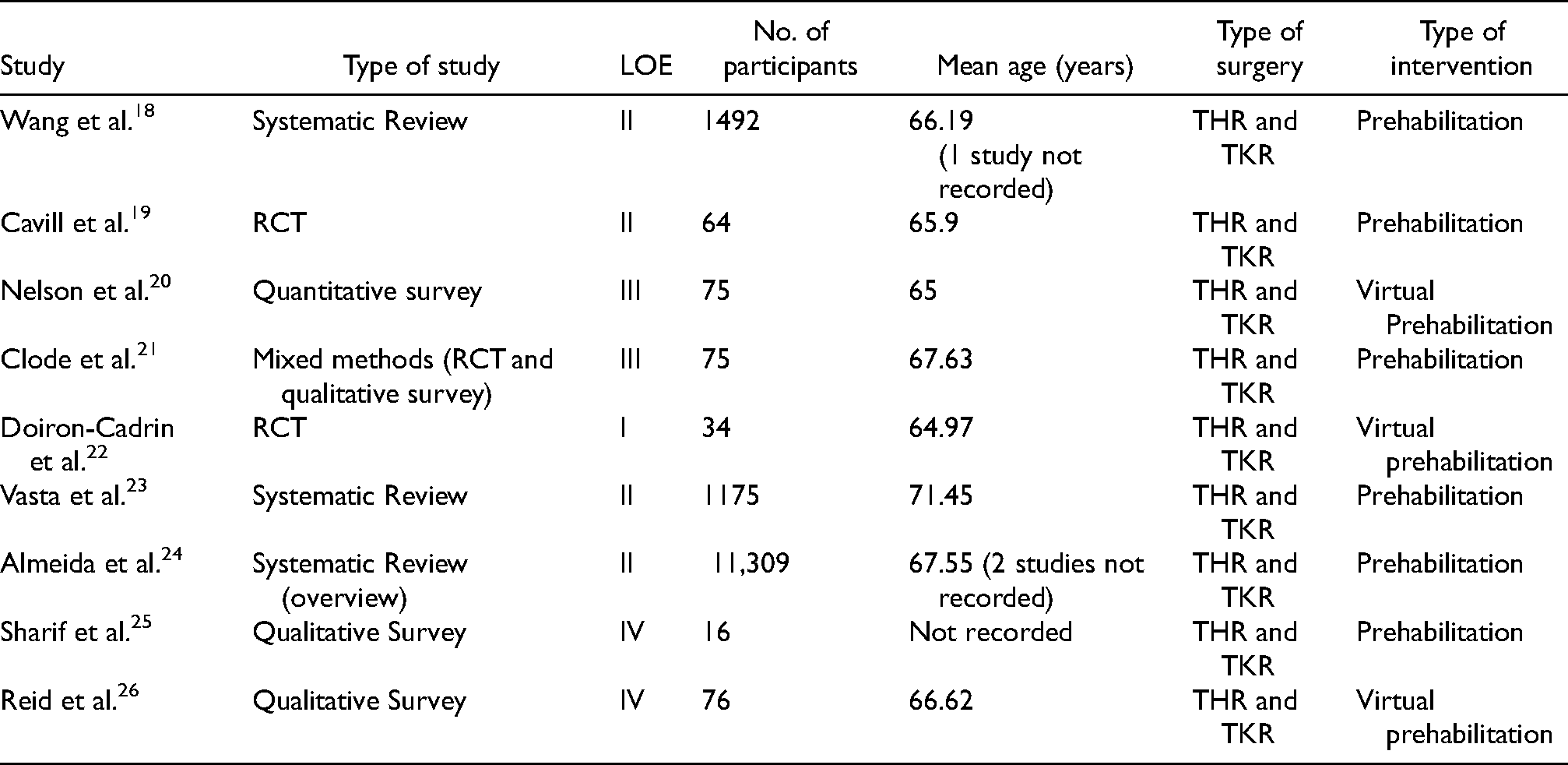
The included studies reported data on 14,316 participants. However, 2667 of these are duplicated due to the Almeida et al. 24 systematic review reviewing 2 papers18,23 included in this review. Without duplications, the total number of participants is 11,649.
11,617 participants were patients undergoing total joint replacements (TJR), 16 were caregivers for TJR patients and 16 were healthcare professionals (HCPs). (Table 3)
Demographic data.
Completion of the literature review revealed four main themes: the effect of prehabilitation on patient functional outcomes, the effect of prehabilitation on LOS, patient satisfaction with teleprehabilitation, and the feasibility of implementing teleprehabilitation. The terms ‘teleprehabilitation’ and ‘virtual prehabilitation’ are synonymous and are used interchangeably throughout this paper.
Effect of prehabilitation on patient functional outcomes
The most common theme was the effect of prehabilitation on patients’ functional outcomes, which was found in 6 papers. 24
The earliest study, Wang et al., 18 was a systematic review and meta-analysis of 22 RCTs (n = 1492) analysing the effect of prehabilitation compared to no prehabilitation for patients undergoing TJR surgery. Primary outcome measures assessed were patient function and post-operative pain, with 2 studies showing prehabilitation reduced Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) pain score by 6 with 95% CI (−10.6 to −1.6) within 4 weeks, but no difference >4 weeks. Prehabilitation allowed patients to resume ADLs 0.9–1.4 days earlier than no prehabilitation, however the difference is trivial. Of the 22 studies, 18 had a high risk of bias and poor methodological quality. Whilst Wang et al. 18 established prehabilitation improved pain and function, effect sizes were small, and results were not statistically significant.
Cavill et al. 19 also analysed prehabilitation compared to no prehabilitation prior to TJR in their pilot RCT. 64 participants were randomly allocated to prehabilitation or usual care. Preliminary evidence demonstrated THR patients in the prehabilitation group improved EuroQol (EQ)-visual analogue scale (VAS) (P = 0.93 with 95% CI) and timed up and go (TUG) times (p = 0.72 with 95% CI). The same results were not found in the TKR patients, which suggests prehabilitation effects TKR and THR patients differently, however authors were unable to suggest a rationale for this difference. Cavill et al. 19 provide no long-term data, with follow-up at 8 weeks only.
Another study analysing the effectiveness of prehabilitation by comparing it to usual care was Clode et al. 21 Their mixed methods observational cohort study assessed pre-surgical patient outcomes and patient expectations. Prehabilitation produced statistically significant improvements in all outcome measures and positively influenced patient expectations and satisfaction. Primary outcomes analysed were pain (NPRS), function (WOMAC, TUG, 5xSTS) and QOL (EQ-5D) with LOS analysed as a secondary outcome. Five times sit to stand time (5xSTS) improved by a mean score of 5.55, TUG improved by 3.75, WOMAC improved by 4.56%, and numeric pain rating scale (NPRS) improved by 0.68 all with 95% CI and above the agreed statistical significance threshold of P = ≥0.05. Clode et al. 21 report results consistent with Wang et al.’s 18 findings which indicate prehabilitation induces small increases in function.
The mixed methods approach used by Clode et al. 21 provided a holistic view of the topic, however, methodological flaws reduced validity of results. The study was not randomised, with patients self-selecting into either group (out of 75 patients 52 chose prehabilitation and 23 usual care). Patient self-selection introduced an element of systematic bias; however, it can be argued greater numbers choosing prehabilitation suggest this is a preferable intervention. Patients who opted for prehabilitation had greater baseline levels of pain and physical impairment, therefore may have experienced greater improvements than patients whose baseline was better. Follow-up adherence for the qualitative survey was low, with only 22 patients out of 75 participating, limiting validity of the results.
Two of the papers returned by the literature search were large systematic reviews analysing the effect of prehabilitation on patient outcomes.23,24 Vasta et al. 23 analysed 14 studies assessing the effect of prehabilitation on post-operative outcomes following TKR and THR. Vasta et al. 23 included a large cohort (n = 1175), however 10 of the 14 studies analyse TKR not THR, limiting application to this paper. This is pertinent given the evidence from Cavill et al. 19 suggesting TKR and THR patients experience different results after prehabilitation.
Vasta et al. 23 included objective and subjective clinical outcome measures providing a holistic approach. Authors established prehabilitation improves functional and QOL outcomes, with most studies demonstrating post-operative improvement of VAS, range of movement (ROM), WOMAC and Knee injury and Osteoarthritis Outcome Score (KOOS), and improved QOL. However, power analysis and confidence intervals were not reported, potentially leading to overestimation or underestimation of results.
Vasta et al. 23 found no difference between progressive strength training and standard strength training in prehabilitation, however, heterogeneity of prehabilitation interventions makes it difficult to draw accurate conclusions. 23 This proved an issue for most papers, with only Cavill et al. 19 providing explicit details of their prehabilitation program.
Almeida et al. 24 provided an overview of 10 systematic reviews analysing the effects of prehabilitation on post-operative function for TJR's. Only systematic reviews were included, which ensured a large amount of data was captured (n = 11,309), although this included 2 studies analysed in this literature review.18,23 Caution is advised as no studies after mid-2020 were included. Consequently, Almeida et al. 24 does not incorporate any interventions implemented due to COVID-19, which may limit transferability of results to current practice.
Almeida et al. 24 conclude there is no clear effect of prehabilitation on clinical outcomes for the following reasons: the effectiveness of prehabilitation programs is not assessed pre-operatively, the influence of individual patient characteristics is not assessed, prehabilitation programs are too heterogeneous (mode, intensity, frequency, duration) to be combined, most programs did not use recommended exercise dose/intensity from American College of Sports Medicine (ACSM), and none assessed compliance. The authors reach a similar conclusion as Vasta et al. 23 that there is a need to develop standardised prehabilitation protocols based on exercise guidelines.
A pilot RCT by Doiron-Cadrin et al. 22 was one of 2 papers that analysed both prehabilitation and virtual service provision. Authors investigated the feasibility of teleprehabilitation compared to in-person prehabilitation and usual care. A small sample size (n = 34) was assigned to teleprehabilitation, 12 in-person prehabilitation, 11 and usual care. 11 Teleprehabilitation made a statistically significant improvement in the stair test (mean difference −2.0 with 95% CI) and the Self-pace Talk Test (mean difference −4.2 with 95% CI). The in-person prehabilitation group also improved (mean difference −4.2 with 95% CI), supporting data from other studies21-23 which report prehabilitation is effective.
Doiron-Cadrin et al. 22 acknowledges several limitations in their study. Potential performance bias in the experimental groups, or negative compensatory bias in the control group could have influenced results and the inclusion criteria of access to high-speed internet may have excluded patients from low socioeconomic backgrounds. This study was underpowered due to small sample size (n = 34) and long-term data is not available, with follow-up only undertaken at 12 weeks.
Effect of prehabilitation on LOS
The literature search found few articles assessed LOS, however, five studies did include LOS data as a secondary outcome.24-21
Wang et al. 18 found 1 out of 10 studies demonstrated prehabilitation significantly reduced LOS (mean difference = -0.8 days). In contrast, Cavill et al. 19 reported prehabilitation made no difference to LOS, however a healthier cohort was recruited, with reviewers selecting patients more likely to be discharged. Consequently, prehabilitation results may be underestimated due to a healthier baseline of participants and it can be hypothesised prehabilitation has a greater effect on patients with worse physical function.
Clode et al. 21 established the time and location (outpatient setting, daytime) was a potential barrier to attendance. Barriers to attending prehabilitation reduced the reliability of this data due to a smaller cohort participating, which may not reflect the overall elective THR population. 21
A recurring topic in LOS data is the low methodological quality. Vasta et al. 23 found all studies showed reduced LOS after prehabilitation, however all had a high risk of bias. Almeida et al. 24 reported improvement in LOS following prehabilitation, however methodology is poor, reducing the validity of the data. Clode et al. 21 identify the effect of prehabilitation on LOS as a valuable area of future research. LOS correlates with improved patient outcomes and could therefore be an important indicator of the efficacy of prehabilitation. 27
Patient satisfaction with teleprehabilitation
The third theme in this literature review is ‘patient satisfaction with teleprehabilitation’ with three studies including this.21,22,26 All studies reported high levels of patient satisfaction with teleprehabilitation, suggesting this would be a well-received intervention.
Clode et al. 21 found patients who underwent teleprehabilitation felt more prepared for surgery, with patients >85 years old benefiting most. 21 Subsequently, it is suggested elderly patients have more to gain from prehabilitation. Future studies into the effect of prehabilitation on different ages would advance the evidence base, which is currently limited by under-powered studies with homogenous patient populations
Doiron-Cadrin et al. 22 reported high patient satisfaction with teleprehabilitation (91% satisfied with technology, 100% satisfied they met their prehabilitation goals, 91% felt teleprehabilitation as good as in-person therapy). However, patients would still like to see a Physiotherapist in-person.
Reid et al., 26 provides qualitative data on patients and caregivers’ views of teleprehabilitation prior to elective THR or TKR surgery. 76 participants were recruited (46 with Hip OA, 14 with knee OA, and 16 caregivers) and data gathered via semi-structured interviews (SSIs) and focus groups. Overall patients and caregivers were positive about virtual services. Patients preferred interaction with HCPs, consistent with findings from Doiron-Cadrin et al. 22 Most participants in the study were able to use technology, but Reid et al. 26 cautioned digital literacy is still a potential barrier.
The benefits of including qualitative studies are the rich data they provide about patients’ lived experience. Reid et al. 26 also includes caregivers’ feedback, supplying well-rounded data. As with all qualitative studies, there is a risk of researcher bias and the small cohort limits transferability of results.
Feasibility of implementing teleprehabilitation
Four studies analysed the feasibility of implementing teleprehabilitation.20,22,25,26 Nelson et al. 20 assessed the feasibility of introducing telerehabilitation for TJR patients. Overall, 64.8% were willing to participate in telerehabilitation (72.2% <65 years old, 55.3% >65 years old). Nelson et al. 20 found high levels of technology access (70% overall, rising to 85% <65 years old), suggesting telerehabilitation is achievable. However, technology access dropped from 90% for <65 years old to 40% for >66 years old (p < 0.05). This is important in light of findings from Clode et al. 21 who identified patients >85 years old as most likely to benefit from prehabilitation. Subsequently, this suggests patients most likely to benefit from teleprehabilitation may have more challenges accessing these services.
Nelson et al. 20 established online classes were the preferred method of telerehabilitation, suggesting patient-clinician interaction is important, in concurrence with Reid et al. 26 Doiron-Cadrin et al. 22 propose patient-clinician interaction affects compliance with prehabilitation, which subsequently influences the feasibility of virtual services. Doiron-Cadrin et al. 22 found although compliance with teleprehabilitation was high (77% ± 13), it was slightly less than in-person prehabilitation (80% ± 12). It can be argued this supports the hypothesis that patient-clinician interaction is important in compliance.20,26
Equipment provision and digital literacy were identified as barriers to teleprehabilitation, in agreement with Reid et al. 26 Patients also cited travel issues attending outpatients’ appointments as a reason for preferring telerehabilitation, in concurrence with Clode et al. 21 Nelson et al. 20 had a small cohort and only 59 (79%) completed all questions, thus reducing reliability of results. The study was of low methodological quality but provides a useful understanding of patient preferences.
Sharif et al. 25 explored attitudes of HCPs in using technology pre-operatively via SSIs, with virtual services considered beneficial overall. Digital literacy was suggested as a potential barrier, in agreement with Reid et al. 26 and Nelson et al. 20 Sharif et al. 25 hypothesises the resistance to change mentality in the NHS may have influenced participants and this should be considered when applying results. Sharif et al. 25 is a recent study in an NHS hospital, making it relevant to this paper. However, participant numbers are small, and staff are from one NHS Trust, reducing the generalisability of results. The information provided is a useful insight into implementation of virtual prehabilitation, but the limitations of the study suggest they should not be given too much credence.
To summarise, there is moderate evidence prehabilitation improves patient outcomes and strong evidence virtual service provision is feasible and acceptable to patients. The literature review provides sufficient evidence to implement virtual prehabilitation into practice.
Proposed implementation plan
This paper intends to provide a basic template for services wishing to implement virtual prehabilitation. NHS policy on service transformation and change management have been used to provide an implementation plan aligned with the NHS Long Term Plan and UK national policy.2,11,12 Logistical details are only outlined briefly, therefore it is suggested clinicians wishing to implement virtual prehabilitation can use the UK policies referenced for further support.
Quality improvement (QI) is ‘the use of methods and tools to continuously improve quality of care and outcomes for patients’. 28 The ‘Plan, Do, Study, Act’ (PDSA) QI model can be used to structure service transformation. PDSA implements changes on a small scale, to limited stakeholders initially, ensuring minimal service disruption. 29 (Figure 2)
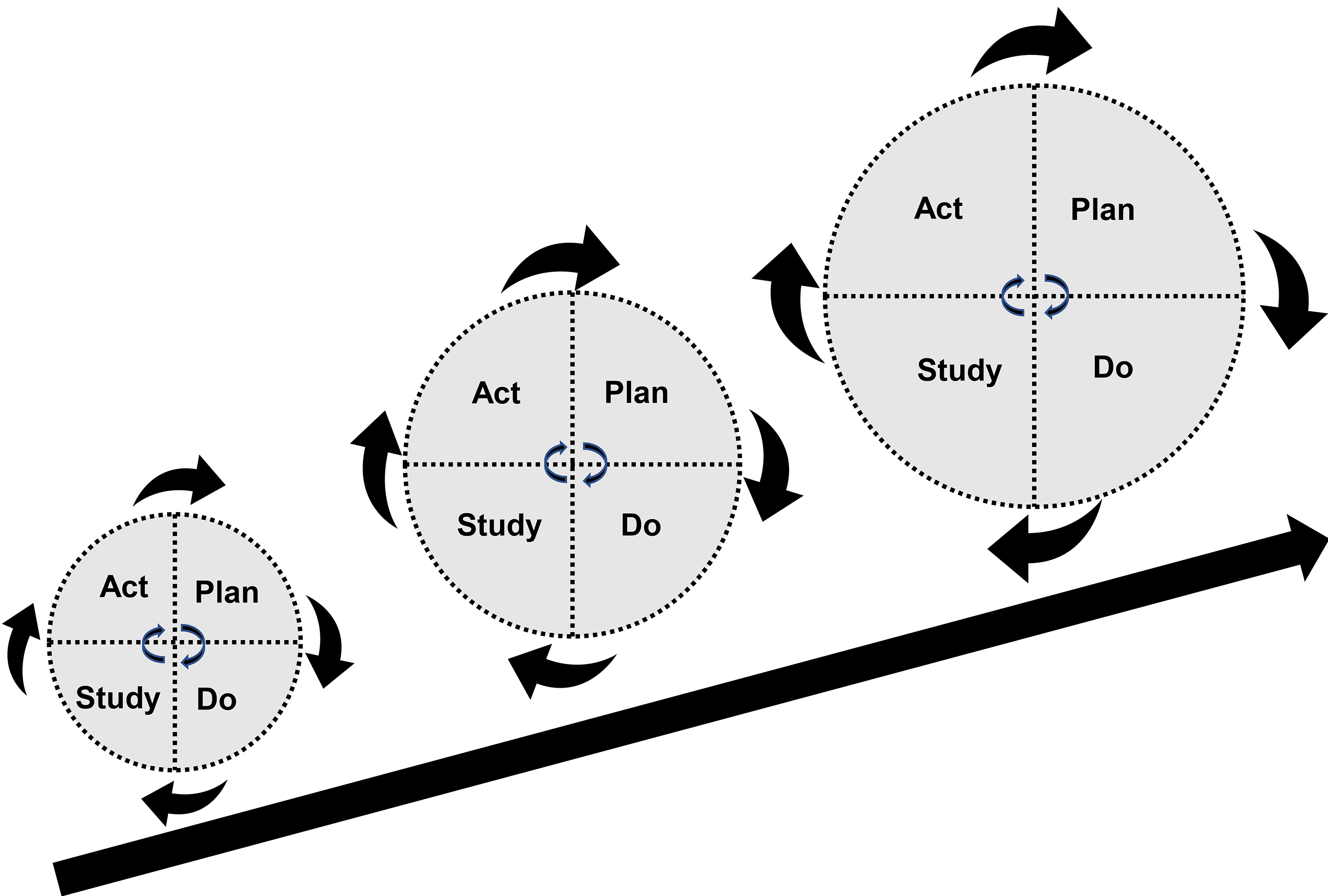
PDSA cycle.
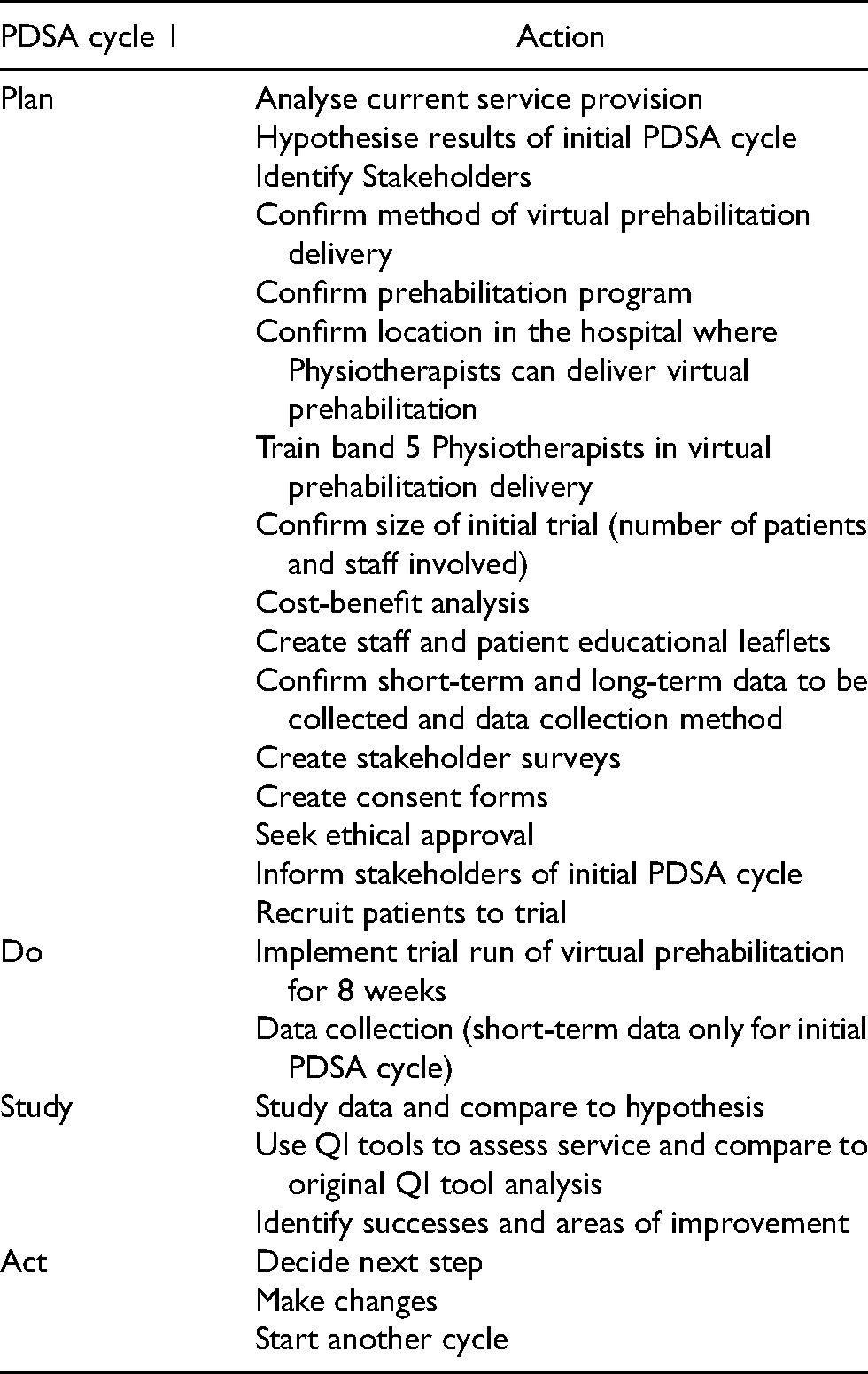
‘Plan’ phase
Table 4 outlines the plan for the initial PDSA cycle.
Initial PDSA cycle action plan.
Hypothesis
The literature suggests virtual prehabilitation will have high attendance and low attrition rates, however patients may need support using technology.20,26
Delivery
Clinician-patient interaction significantly increases adherence, therefore virtual prehabilitation should be delivered via live online classes run by a Physiotherapist.22,26 Classes should be provided via Skype, based on NHS recommendations. 30 ACSM guidelines on strength training should be used to provide evidence-based prehabilitation. 31
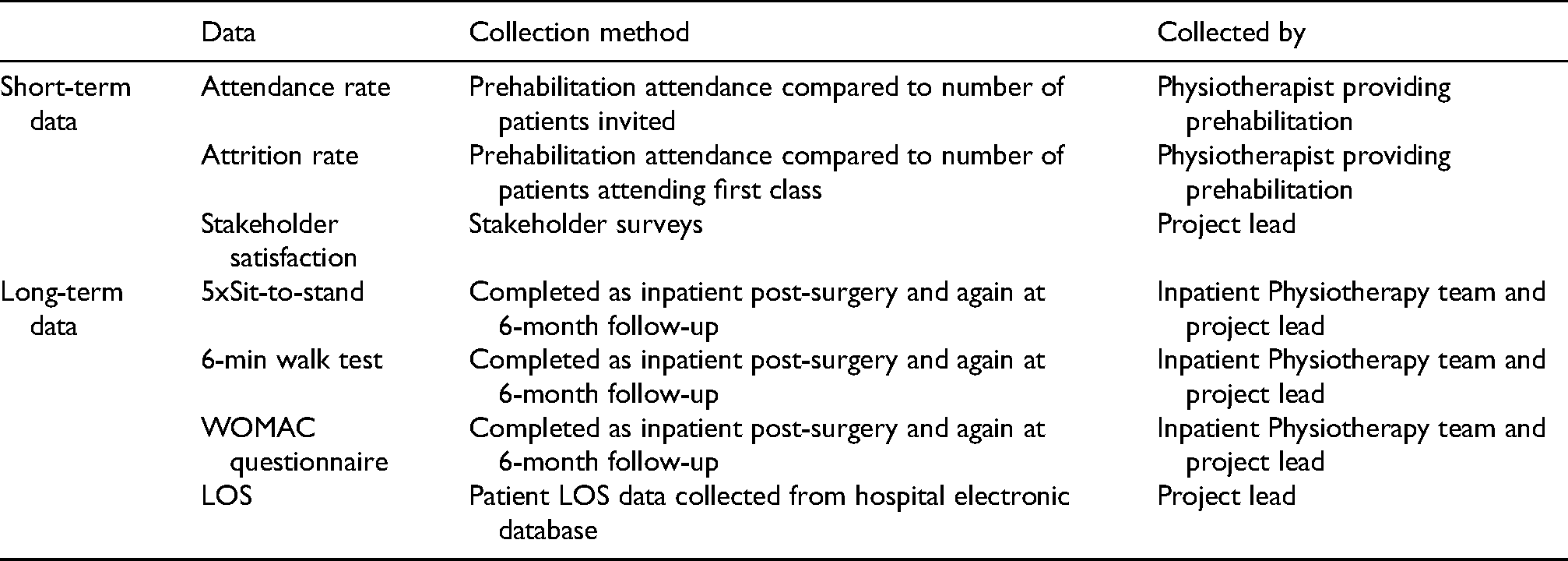
Data collection
Short and long-term data will be collected for analysis (Table 5.) The outcome measures were selected as they were commonly reported in the literature, with LOS data collected to rectify deficits.
Data collection.
Recruitment
The initial inclusion criteria should be: <65 years old, technology access, digitally literate.20,26 40 participants should be recruited initially, based on evidence 40 data points reliably predict overall population behaviour. 32
Ethics
Ethical approval should be sought from the Health Research Authority (HRA) prior to implementation of the initial PDSA cycle. 33 Patients must provide explicit consent to participate. 34
Patients undergoing THR are older (mean age 66.82 years old) and subsequently more likely to experience cognitive difficulties.35,36 Physiotherapists must be certain patients have mental capacity before recruiting. 37
Stakeholder analysis
Stakeholders should be identified, prioritised using a power/interest grid, and a readiness to change matrix applied to identify those for and against change. 38
Behaviour change theory
It is suggested that the Capability opportunity motivation (COM)-B model of behaviour change is used to support effective change, as this is the theoretical framework which underpins NICE behaviour change guidelines.39,40 (Figure 3)
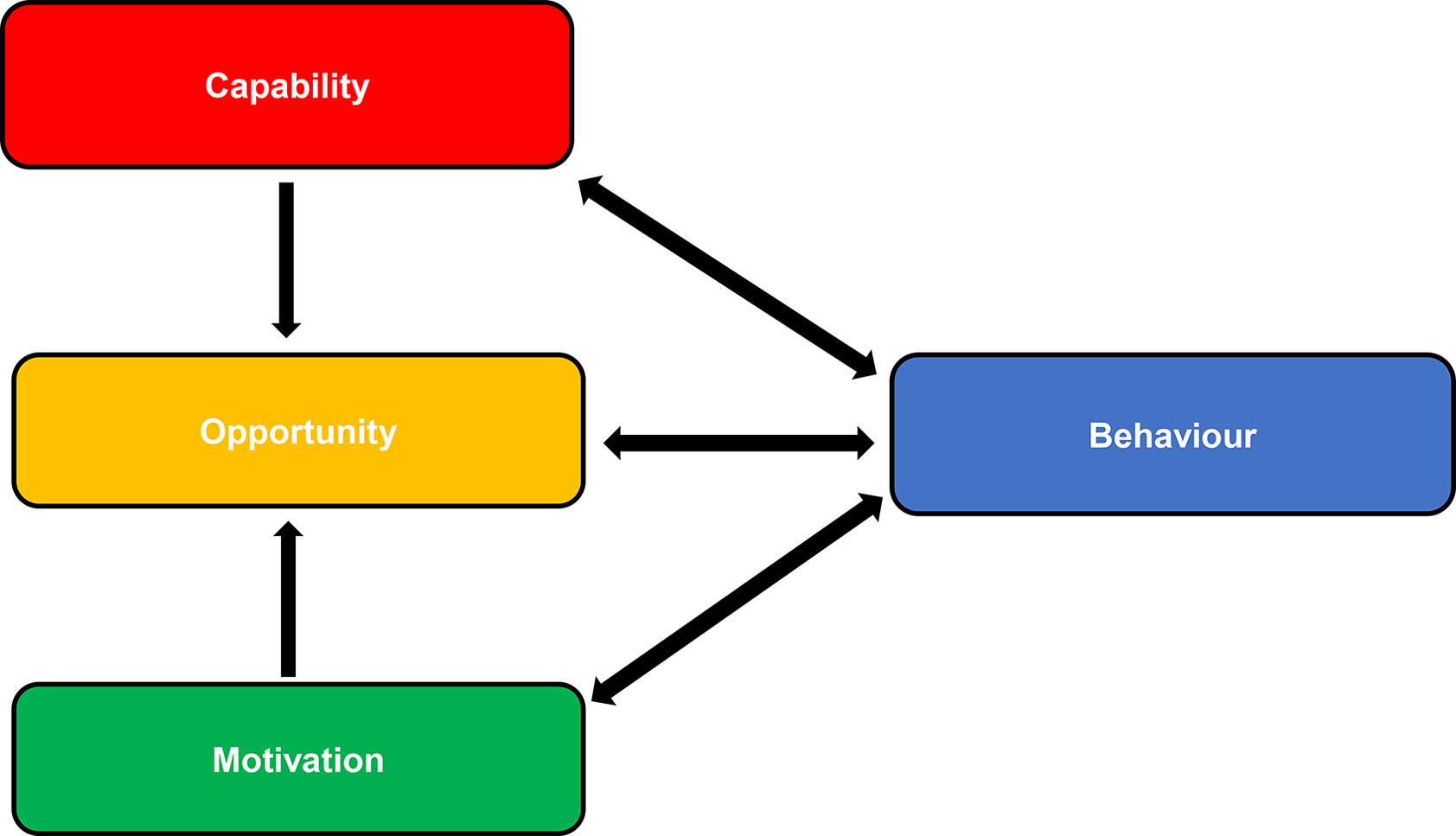
COM-B model of behaviour change.
Communicating change
A systematic plan for communicating change to stakeholders should be created based on NHS England's stakeholder communication plan. 38
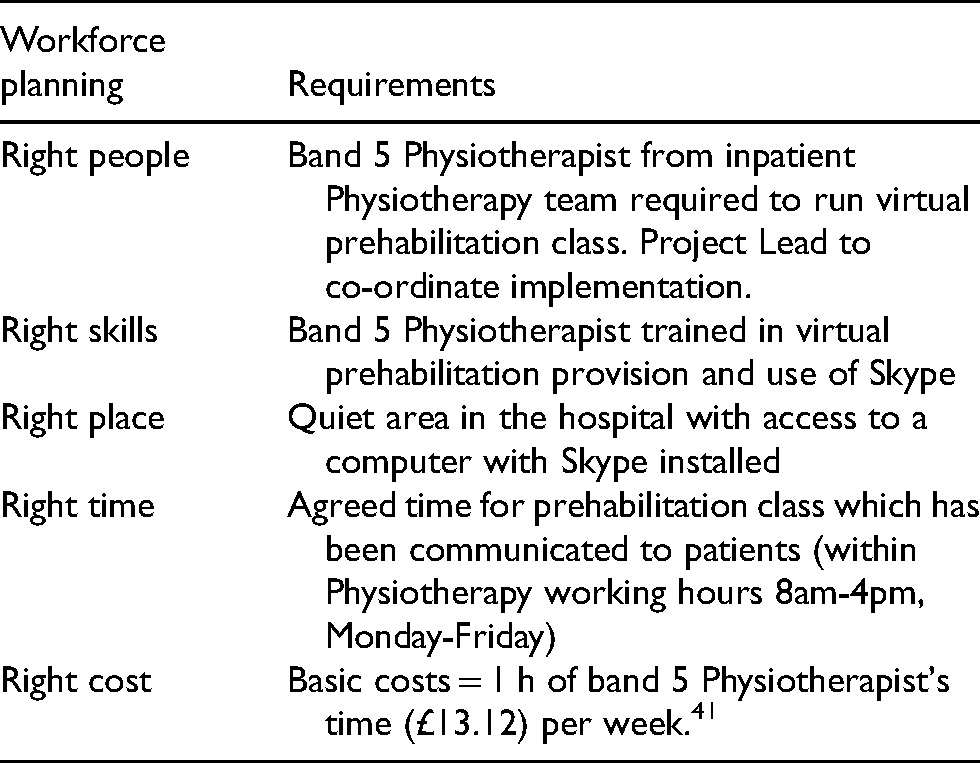
Workforce planning
The NHS Five Year Forward View proposes efficient workforce planning is the most effective way to deliver care. 11 (Table 6)
Workforce planning requirements.
‘Do’ phase
The initial trial duration should be 8 weeks, as this was the median prehabilitation duration in the literature.19,21-23 Implementation can be monitored using a Gantt chart, to track project progress against goals. 42
‘Study’ phase
Data collected will be analysed by comparing results to the hypothesis and summarising successes and areas of improvement.
‘Act’ phase
Insight gained from data analysis highlights necessary changes and another cycle commences. 43 The end point will be when virtual prehabilitation is offered to all elective THR patients. The literature suggests this should be when patient satisfaction is 90% and compliance is 80%. 22
Discussion
The literature review provides moderate evidence prehabilitation improves patient outcomes when undergoing elective THR surgery 21-23 and strong evidence virtual services are effective, feasible, and acceptable to patients.20-22,25,26
These results build on existing evidence that prehabilitation improves patient outcomes and virtual services are effective. 24 Whilst findings correlate with previous studies, close examination challenges the validity of previous research due to the significant methodological flaws identified (47). It can be argued the evidence reviewed is sufficient to support the implementation of virtual prehabilitation, however, it highlights the necessity of further research.
Data regarding virtual services contributes a clearer understanding of patient and clinician preferences. The literature review established virtual services are most effective when they provide patient–clinician interaction. 26 Earlier studies have not scrutinised this aspect of virtual service provision, however lack of interaction with clinicians was previously considered a disadvantage. 26 These results had practical implications as they influenced the proposed method of virtual prehabilitation delivery.
Limitations
One significant limitation in the literature is the heterogeneity of prehabilitation interventions. There is no standard prehabilitation protocol and most studies do not include explicit details of exercises, sets, etc., making it difficult to draw reliable comparisons. 24 This limitation makes using the evidence base to implement prehabilitation challenging, and highlight flaws with UK policy. NICE 2 recommends prehabilitation prior to THR surgery but does not specify a program, therefore implementation is likely to vary. To overcome this, it is proposed prehabilitation programs follow the ACSM 31 strength training recommendations to provide an evidence-based protocol.
Another limitation identified was the literature quality. Many studies were underpowered, with small cohorts and high-risk of bias, therefore results were not statistically significant. The primary studies reviewed had difficulty blinding researchers due to their required involvement, thus increasing the risk of bias. 44
Hospital LOS was underreported in the literature, with included studies only reporting LOS as a secondary outcome. 21-24 The literature provided some evidence prehabilitation decreases LOS, however scant details were supplied, making it difficult to draw strong conclusions. 18 There is a known correlation between shorter LOS and improved patient outcomes, subsequently this is an important area of research. 27 The proposed QI strategy addresses this deficit by collecting LOS data.
Lack of follow-up data makes it difficult to draw conclusions on the long-term effects of prehabilitation, and subsequently the sustainability of virtual prehabilitation. 22 It is proposed follow-up data continues to be collected after virtual prehabilitation is fully implemented to supply long-term data and allow assessment of sustainability.
The literature review recognised the resistance to change mentality in the NHS as a potential barrier to implementation of virtual services. 25 HCPs are prone to change fatigue due to constantly evolving practice recommendations, which have increased with the rapid changes made due to COVID-19. 13 Digital literacy and technology access were also identified as potential barriers to virtual prehabilitation. 26 Gradual implementation using the PDSA cycle will allow technology issues and resistance to change to be identified and dealt with as they arise.
One limitation of note is that this literature review and project proposal were completed as part of an MSc dissertation. Subsequently the theoretical nature of the work and the authors’ lack of experience of implementing service transformation in clinical practice limit the impact of this paper.
Conclusion
This proposed service transformation is based on reliable evidence that virtual prehabilitation will be effective, feasible, and acceptable to patients. Whilst the evidence for virtual prehabilitation has flaws, it can be argued there is a clear requirement for transformation in UK elective THR services following the COVID-19 pandemic.
This literature review also revealed aspects of UK elective THR services which can be improved. It is proposed prehabilitation programs are implemented virtually to meet patient needs, and a standardised prehabilitation program is established. It is also recommended that future research analyses the effect of prehabilitation on LOS, with more high-powered primary studies required to examine the long-term impact of prehabilitation.
Footnotes
Acknowledgements
I would like to thank my dissertation tutor Alex Carlin for all her help and support with writing my dissertation and her encouragement to publish my work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.