
Abstract
Background/purpose:
Recently, there is more emphasis on the role of core muscles in pathogenesis and rehabilitation of patellofemoral pain (PFP). We aimed to investigate whether increased core muscle strength and endurance improve clinical outcomes.
Methods:
In a randomized controlled trial, 60 patients (M/F: 25/35, age = 32.28 (5.9) years) with PFP were randomly allocated into two groups of routine exercise (control) and combined core plus routine exercise (intervention). Home exercise was scheduled at least 5 times/week for 12 weeks. We assessed the outcomes of pain (Visual analogue scale) and function (Anterior knee pain score) before and immediately after interventions.
Results:
Significant improvements were reported in both groups (P < 0.001). There were significant between-group differences in both outcomes in favor of the intervention (Pain: 12.4, CI 95%: 7.1–17.8, P < 0.001; Function: 6.4, CI 95%: 2.2–10.5, P = 0.003).
Conclusion:
Outcome improvements were significantly greater in intervention group. Inclusion of core stability exercises may lead to additional benefits.
Introduction
Patellofemoral pain (PFP) is an overuse disorder, described as pain in the peripatellar/retropatellar region that aggravates with physical activities such as squatting, stair climbing, running and jumping or sitting for prolonged periods of time. 1 It is the most common source of anterior knee ailment in active adolescents and young adults 2 and is much more prevalent in women than men. 3
Due to multiple forces, influencing the patellofemoral joint, clinical evaluation and management of this ailment is particularly intricate. 4 There is obvious consensus that the etiology of PFP is multifactorial and various parameters may exist as potential risk factors. 5 –8
Generally, the usual approach of sports medicine experts to PFP is primarily on strengthening of quadriceps muscles, especially vastus medialis oblique, with open and closed-chain exercises. 9 However, previous study by authors has shown that incorporating assessment and modification of other risk factors into clinical practice may have additional treatment effects. 10 In recent years, PFP was suggested to be related to low core and hip muscle activity. 11 –14 At present, some studies have been done to conclude whether increases in hip muscle strength improve rehabilitation outcomes in PFP patients and majority of them have shown some degree of significant improvements in main outcomes of pain and function. 12,13,15 –17 However, there is few high quality studies addressing other important core muscles including abdominal, pelvic and paravertebral muscles. Therefore, a well-designed controlled trial to directly compare knee targeted versus knee and core targeted rehabilitation program may be helpful to clarify the additional benefits.
The main goal of this RCT was to compare pain, function and core endurance in patients with PFP assigned to either 12 weeks knee-targeted rehabilitation program (control) or combined knee and core stability rehabilitation program (intervention).
Our hypothesis was that improvements in pain and function of PFP patients involved in intervention group would be greater than control group. We further hypothesized that improvements in core endurance measures would be greater for PFP patients involved in combined knee and core stability rehabilitation program (intervention).
Methods
Design
A parallel randomized controlled trial was designed with allocation ratio of 1:1. Research protocol was registered in the Iranian Trial Registry (http://www.irct.ir) with trial number of IRCT201111168117N1. An ethical clearance was obtained from the Medical Ethics Committee of the Tehran University of Medical Sciences, Tehran, Iran. Patients were randomized after providing informed consent.
Participants
Persons with the following eligibility criteria were enrolled. Inclusion criteria were (1) Age between 18 and 40 years; (2) Presence of at least three of the following signs and symptoms: peri-/retropatellar pain with walking down or upstairs, running, squatting, sitting with knees flexed for an extended period of time, grinding of the patella, and a positive provocative test (such as Clarke’s test); (3) Pain duration of more than 4 weeks; (4) Absence of severe knee osteoarthritis (clinical judgment using American College of Rheumatology criteria and radiography in suspicious cases); (5) BMI < 30 kg/m2; (6) No history of other knee, hip or spine disorders including Osgood-Schlatter disease, patellar tendinopathy, knee ligamentous injury/instability; (7) No history of rheumatologic disease; (8) No previous history of knee-related injuries or surgery; (9) No prior treatment with taping, orthosis and exercise therapy in the past 6 months.
Exclusion Criteria were (1) Pain exacerbation necessitating additional treatments and (2) Acute trauma or surgery of lower extremity and trunk.
The planned trial was set in the daily routine of sports medicine clinic in Imam Khomeini Hospital of Tehran University of Medical Sciences (TUMS). Patients are often referred to clinic by general physicians, rheumatologists or orthopedic surgeons without doing any intervention. After patient’s oral consent, eligibility criteria were checked by the research physician. When eligibility was confirmed, participants signed a written consent. Patients then underwent baseline assessment including a standardized clinical examination protocol for patellofemoral pain 18 and three questionnaires (demographic characteristics of participants, Kujala patellofemoral scale (anterior knee pain score) and 0–100 Visual analogue scale for pain) 19,20 as well as assessment of core stability endurance using three clinical tests. 3,12
To assess core endurance, we applied simple clinical tests (Front plank, modified Bering-Sorensen and side bridge for anterior, posterior and lateral core muscle endurance, respectively) which their proper reliability has been shown in literature. 3,12,21,22
Procedures (independent variables)
After baseline assessment, we randomly assigned the patients to one of the intervention or control groups with balanced block randomization method using block sizes of 4, 6 and 8. The sports medicine practitioners that collected outcome measures remained blind to treatment allocation.
We advise a 12-week exercise program consistent with the patients’ allocation.
Based on systematic review on exercise interventions in the management of patellofemoral pain, routine exercise program focusing on quadriceps strengthening using selected closed and open chain exercises (CKC and OKC) plus hamstring, quadriceps and iliotibial band stretch was prescribed for control group. 23,24
Intervention group performed half volume of above-mentioned routine exercise plus exercises concentrating on core stability and hip muscles. This makes the volume of both exercise protocols relatively similar. Patients did all exercises bilaterally (Table 1).
Overview of interventions for the study groups.
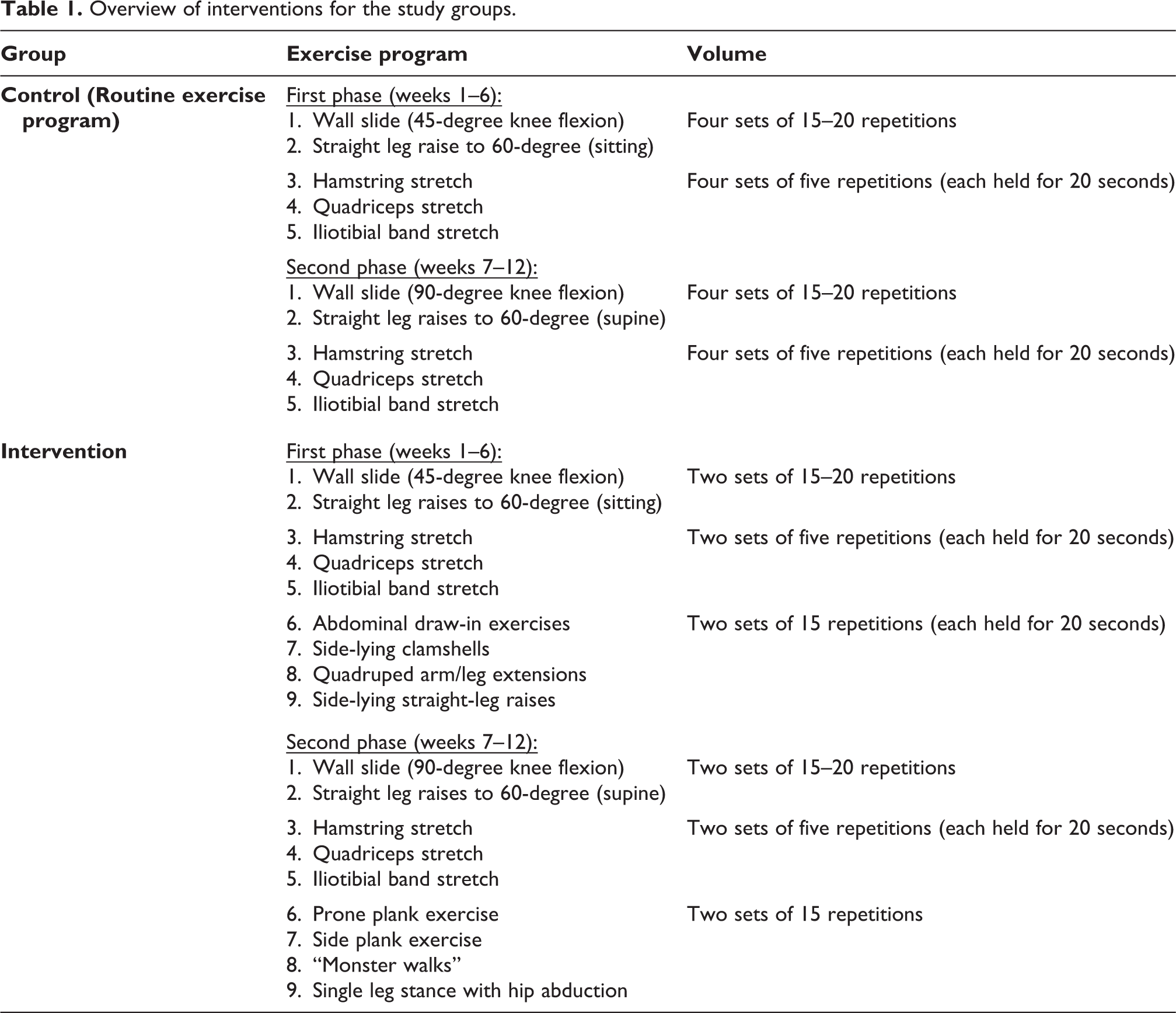
All participants had at least four supervised rehabilitation session in the clinic during 12 weeks period (1, 3, 7 and 9th week) and each lasting 45 to 60 minutes to ensure familiarity with exercise program and their approved execution. Sports medicine practitioners supervised these rehabilitation sessions. All participants asked to do their designed exercises a minimum of 5 days per week (including the supervised rehabilitation in clinic) for 12 weeks.
At the first week and beginning of seventh week treatment, all participants received an educational booklet with a detailed description and illustration of each exercise, as well as a logbook for documentation of the weekly home exercise schedule during the first and second phases of intervention. Logbook was applied to identify the persons who did not achieve the minimal adherence criteria (at least 2 weekly sessions of home exercise and no interruption more than a week between sessions). In these conditions, non-adherence to the intervention considered as a type of protocol deviation.
Adherence of patients to exercise program was followed up by telephone calls each week after the first session. No other therapeutic interventions were used (i.e., medication, modalities, orthosis, taping and bracing). Ice was used as needed during severe pain. Ice pack was applied for 15–20 minutes, once an hour, at least three times a day with a cloth between skin and the ice pack.
The outcome measures were re-assessed in a single session after completion of 12-week exercise period.
Outcome measures (dependent variables)
Patients were evaluated at baseline and 12 weeks afterward. Outcome measures of this study were selected according to their validity and reliability in relation to the study population, as well as the sensitivity to distinguish changes statistically. Other significant consideration was their convenient application in clinical setting. Pain and function were the main focus of study. So, primary outcome measures include pain severity (visual analog scale) and functional disability (anterior knee pain scale).
Both baseline and post-exercise questionnaires were completed by the patients themselves.
Pain and discomfort in previous week were documented on 100-mm VAS. 25 Patients marked their worst pain in the prior week. Crossley et al suggested that it is more reliable than recording “usual” pain. 26
The combined subjective and functional assessment of the knee was performed with the anterior knee pain scale (AKPS) questionnaire. 27
It is a self-reporting tool used for patients with PFP 27 and is a 0- to 100-point scale (100 = best score evaluating pain during stair walking, jumping, squatting, running, and prolonged sitting with the flexed knees; swelling; the presence of a limp; subluxation; the amount of quadriceps atrophy; flexion deficiency; and the need for walking aid). 28
The VAS and the AKPS have been considered as valid, reliable, and responsive tools for outcome measurement in PFP 12 and were selected as the primary outcome measures of our study.
Improvements of >20 millimeters on the VAS or >8 points on the AKPS were regarded as successful outcomes. 12,26
As secondary outcomes, core endurance was assessed using three tests of front plank (for anterior core), modified Bering-Sorensen (for posterior core) and side bridge (for lateral core). A study implies that no difference exists between right and left side bridge endurance times. 23 As a result, the injured leg was positioned superior in the side-lying position to avoid additional stress on the knee.
After patients’ familiarization with the tests, a single trial of each test was performed with 1 to 2 minutes of rest between tests. The length of time (in seconds) that the patient could hold the position was documented. 29
Statistical analysis
Quantitative and categorical variables were presented as mean (standard deviation) and frequency (percentage), respectively. To estimate between-group mean differences in primary outcomes after 12-week period, a multiple linear regression model was used (with 95% confidence intervals) with adjustment for probable confounders including sex (male or female), age (years), BMI (kg/m2) and baseline outcome measures (VAS and AKPS). We define the statistical significance as P < 0.05. All analyses were performed using SPSS version 17.
For sample size calculation, the treatment success was defined as a decrease in VAS by a minimum of 20 mm and an increase in AKPS by a minimum of eight points. 26
The sample size of 70 patients (35 in each group) was calculated to reveal the clinically important differences with a power of 80% at the significance level of 0.05. It permits for a 30% drop-out rate.
Results
After enrolling eligible patients, participants were invited for clinic visits at baseline (the time of randomization) and after 3, 7, 9 and 12 weeks of intervention period. A flow chart of the trial is shown (Figure 1).
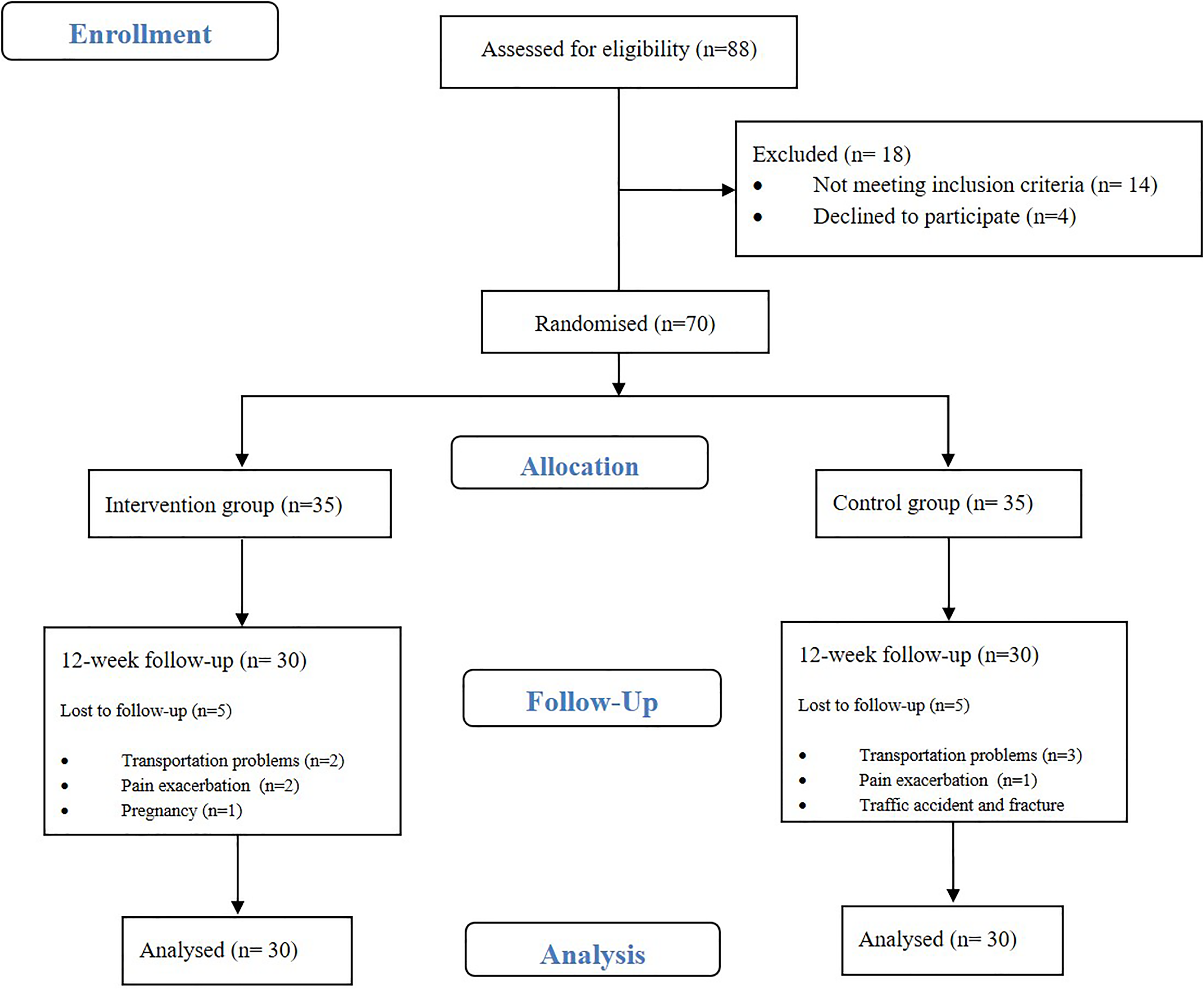
Flow of participants throughout the intervention.
After patients’ recruitment, 88 patients with diagnosed PFP were screened and after checking for eligibility criteria, 70 patients entered the study [40 female, 30 male, Age: 32. 28 (5.91)] and randomly allocated in two groups [intervention (n = 35): 21 female, 14 male, age: 32.10 (5.98); and control (n = 35): 19 female, 16 male, age: 32.47 (5.92)]. During 12-week period, 10 participants lost to follow up (5 in each group) and 60 patients completed the trial. According to the physical activity recommendations by American College of Sports Medicine (ACSM) and American Heart Association (AHA), 18 and 23 patients were physically active in intervention and control groups, respectively. No case of non-adherence was reported after assessment of the participants’ logbooks.
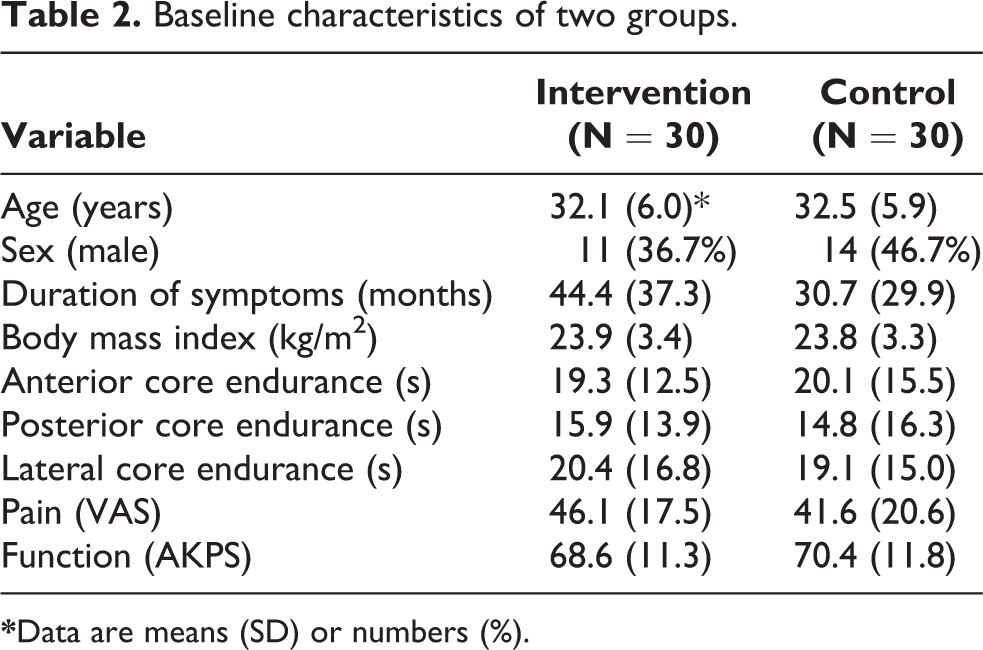
Table 2 shows the baseline characteristics of two groups.
Baseline characteristics of two groups.
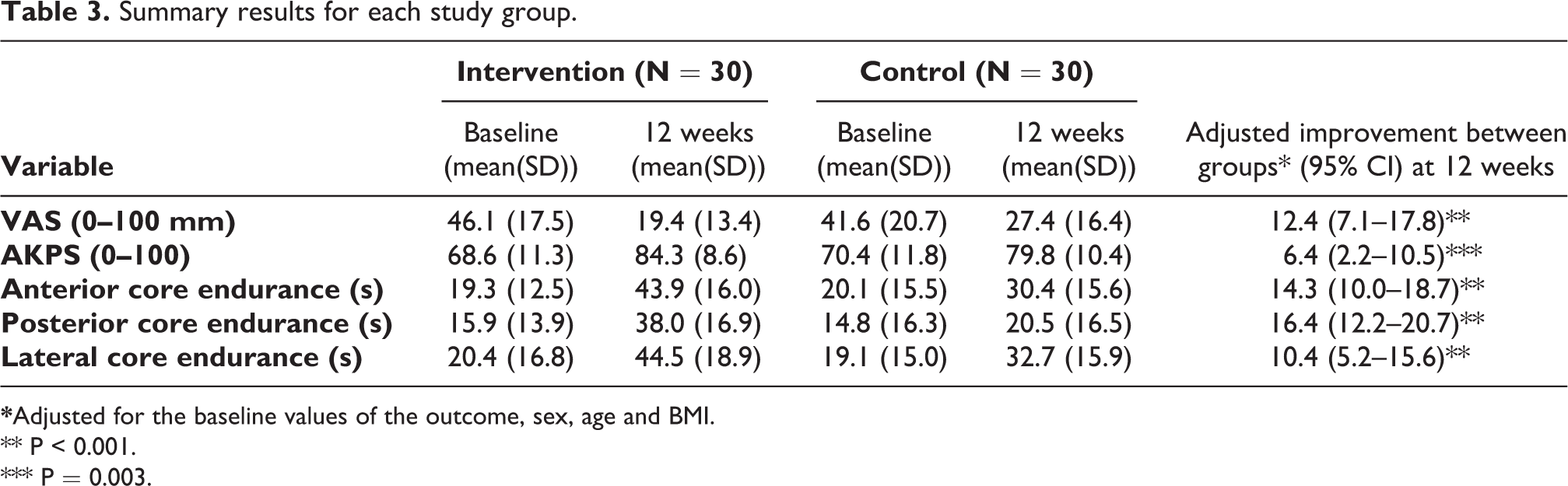
As demonstrated in Table 3, both VAS and Anterior knee pain scores (AKPS) were significantly improved within both groups after the intervention period (Pain: 26.7 V.S. 14.2 and Function: 15.7 V.S. 9.4 in intervention and control groups, respectively). These changes were more significant in intervention group, following adjustment for the baseline values of the outcome, sex, age and BMI (P < 0.001, P = 0.003).
Summary results for each study group.
** P < 0.001.
*** P = 0.003.
Patients involved in intervention group had a significant improvement in self-reported pain (VAS) and function (AKPS) based on our prior definition of success. 21,26 In control group had a significant reduction only for function (AKPS).
After 12 weeks, anterior, lateral and posterior core endurance significantly improved in both groups (P < 0.001), but this improvement was significantly greater in intervention group (P < 0.001).
Discussion
Development of practical and effective clinical protocols for PFP is a central part of clinical research in sports medicine due to high prevalence and chronic nature. Our study revealed that the implementation of core exercises to the routine exercise program might have additional effects on pain and function.
Although the role of isolated hip and core exercises in rehabilitation of PFP patients has been shown in a few studies, 12,13,15,16,30 our trial is perhaps the first RCT to study the additional effects of core exercises to improve pain and function of PFP patients while measuring core endurance changes in 12 weeks rehabilitation program.
Results of this study are consistent with studies reporting the effectiveness of hip and core exercises on primary outcomes of pain and function. 12,13,15 For example, a study investigated the influence of strengthening the hip abductor, external rotator and quadriceps musculature compared to quadriceps strengthening alone in 70 females with patellofemoral pain syndrome after 4 week program and demonstrated that the improvements of pain and function were greater for the hip and quadriceps strengthening group. 15
In another study, 12 researchers conducted a case series, 19 women with PFP participated in an 8 week program to strengthen the hip and core muscles and improve dynamic malalignment. They reported significant improvements in pain, functional ability; lateral core endurance, hip abduction, and hip external rotation strength. However, the lack of control group and random assignment may be considered as the limitations of this study.
Another study 30 investigated 14 patients with PFP who were randomly assigned to the intervention group (strengthening of quadriceps plus strengthening of hip abductor and lateral rotator muscles) or to the control group (strengthening of quadriceps). After a 6-week home exercise program, only the intervention group improved perceived pain symptoms during functional activities. Authors concluded that supplementation of strengthening of hip abductor and lateral rotator muscles provided additional benefits with respect to the perceived pain. Pure core muscle exercises were not included in this study and function of the patients was not addressed as an important outcome.
A study compared pain, function, knee and hip muscle strength, and core endurance between knee and hip protocols after 6 weeks of rehabilitation in PFP patients. 16 Although outcomes were similar after 6 weeks, the hip protocol showed that earlier resolution of pain and more gains in strength compared with the knee protocol. In contrast to our study, authors in this study have used hip exercises in place of, not in addition to, the knee exercises. Otherwise, 6-week program may not be able to increase the anterior and lateral core endurance, significantly.
The findings of this study support the growing evidence, which suggests that addressing the proximal risk factors of PFP, especially core endurance is probably an efficient intervention for PFP management. However, although significant improvements in pain and function were measured in participants allocated to the intervention group, the possible mechanisms for these changes cannot be extracted from the current trial.
There are some limitations for this trial: First, the participants of current study consisted of a rather small homogenous group (patients with 18–40 years old and chronic pain). Whether the findings of this trial could be generalized to all PFP patients (such as adolescents, elderly, professional athletes, patients with acute presentation, or associated knee ailments) is still unknown.
Second, the 12-week follow-up period may not be sufficient to conclude whether the interventions remain effective, and studies with sound follow-up beyond the end of the exercise period should be designed to ascertain the durability and continuous efficacy of the interventions. However previous RCTs duration, most of the time were 4 to 6 weeks and we evaluated the participant longer. Another limitation was related to the difference in symptom duration between two groups despite our completely randomized allocation which, at the first glance, may affect the results. However, as the mean duration was higher in the intervention group, the reported effect size cannot be undervalued. It also applies to the mean VAS baseline score which was higher in the intervention group. Also, physically inactive patients were more in the intervention group that may influence the results.
Conclusion
This study provides evidence that addition of core exercises may lead to lesser pain and better function after 12-week program compared with routine exercise therapy in persons with patellofemoral pain. It appears that inclusion of core stability exercises to rehabilitation of PFP patients may be reasonable.
Supplemental material
Supplemental Material, sj-pdf-1-otr-10.1177_2210491721989075 - Additional effects of core stability exercises on pain and function of patients with patellofemoral pain: A randomized controlled trial
Supplemental Material, sj-pdf-1-otr-10.1177_2210491721989075 for Additional effects of core stability exercises on pain and function of patients with patellofemoral pain: A randomized controlled trial by Behnaz Tazesh, Mohammad Ali Mansournia and Farzin Halabchi in Journal of Orthopaedics, Trauma and Rehabilitation
Footnotes
Acknowledgement
The authors highly appreciate the cooperation of all patients and clinical staffs of department of Sports and Exercise Medicine – Imam Khomeini Hospital who aided us for this project.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This trial has been funded by the grant No. 9011225002 from Vice-Chancellor for Research of Tehran University of Medical Sciences (TUMS) and also was part of an MD thesis.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.