
Abstract
Background
Patellofemoral pain syndrome is the most common knee condition and is associated with patellar maltracking. Ultrasound is used in studying patellar maltracking. The objective is to determine if the technique which analyzes the displacement of the patellar tendon in the trochlear sulcus is associated with patellofemoral pain syndrome.
Methods
In total, 68 knees of 34 football players (males = 20, females = 14) were included. Patellar tendon displacement was assessed in supine and standing positions. Patellar tendon displacement difference in the two positions was determined.
Results
There was a significant difference in the lateral patellar tendon displacement during standing which was larger in patellofemoral pain syndrome than without patellofemoral pain syndrome (Mean Rank = 39.20 vs. 30.32, p = 0.02). There was no significant difference between the two groups for lateral patellar tendon displacement in supine and the difference in patellar tendon displacement from supine to standing.
Conclusion
The technique could be a potential method in assessing patellar maltracking. It could be used to have a comprehensive understanding of the pathomechanics and treatment of patellofemoral pain syndrome.
Keywords
Introduction
Patellofemoral pain syndrome (PFPS) is the most common form of knee pain characterized by the presence of retropatellar and peripatellar pain during activities that involve loading of the lower extremity such as ascending/descending stairs, hopping/jogging, prolonged sitting, kneeling and squatting. 1 Males and females adolescents have a prevalence rate of 7.2%. For female adolescent athletes, the prevalence was as high as 22.7%. 2
It may be due to trauma or an overuse injury caused by patellar maltracking on the femoral trochlea during movement. Maltracking is usually characterized by lateral translation of patella during full extension. 3 There is an increase in contact pressure between the lateral patellar facet and trochlear groove. This results in stimulation of nerve endings of the subchondral bone, synovium, or lateral retinacular ligaments leading to pain perception. 1 There are many potential inter-related factors causing lateral maltracking of patella. These are vastus medialis obliquus deficiency, medial patellofemoral ligament laxity, lateral retinaculum tightness, increased quadriceps angle (Q), hip abductor weakness, patella alta, and trochlear dysplasia. 4
About 50% of those diagnosed with PFPS have patellar maltracking which could be the precursor of this condition. 5 With this, studies have focused on assessing patellar maltracking to explain its pathomechanics and the effects of different strategies in its prevention and management.6,7
One of the frequently used parameter in analyzing patellar maltracking is the bisect offset index measured through magnetic resonance imaging (MRI). Bisect offset index is defined as the percentage of the patella which is lateral to the midline of the femur and measures the medial and lateral translations of the patella. 8 A meta-analysis showed that of all imaging modalities used in the study of PFPS, the bisect offset index has a large standardized mean difference of 0.99 (95% CI: 0.49, 1.49). 9
Recently, the tibial tuberosity–trochlear groove(TT–TG) distance which is a gold standard used to assess patellar instability has been used in patients with patellofemoral syndrome.10,11 It quantifies the lateralization of the tibial tubercle by measuring the distance between the most anterior portion of the tibial tuberosity and the deepest point of the trochlear groove in the coronal plane using either computed tomographic (CT) scan or MRI.12,13 Because of the variability of the cut-off point for patellar instability using CT and MRI and different positions of the knee with TT–TG distance, it was suggested that the midpoint of the patellar tendon instead of the tibial tuberosity known as the patellar tendon–trochlear groove (PT–TG) distance be utilized. It showed better intra-rater and inter-rater reliabilities as compared to TT–TG distance.14–16 PT–TG distance is the distance between the midsection of the patellar tendon and the deepest point of the trochlear groove in the coronal plane using MRI. However, the disadvantages of using MRI are its cost, unavailability in different localities, and not being suitable for clinical assessment.
A more cost-effective modality is musculoskeletal ultrasound. However, the patella is visualized by ultrasound in longitudinal scan and there are technical difficulties in seeing it within the trochlear sulcus of the femur which is being performed in MRI. 17 Studies using sonography have focused on the morphologic changes of the vastus medialis and the lateral retinacular ligaments.18,19
The patellar tendon which is composed of deep and superficial layers originates from the inferior pole of the patella. It lies partially at the most inferior portion of the trochlear sulcus and the central third of the proximal tibia (Figure 1). It then inserts at the tibial tuberosity. Because of its origin, the direction of the movement of the patella will also be the direction of the movement of the patellar tendon. 20 The patellar tendon may be visualized in transverse scan in the most inferior area of the trochlear sulcus provided that the ultrasound head is placed immediately inferior to patella (Figure 1). The authors hypothesized that the patellar tendon could be used the alternate structure of the patella during sonography to determine maltracking using the same principles of the bisect offset index, TT–TG and PT–TG distances.8,12–16
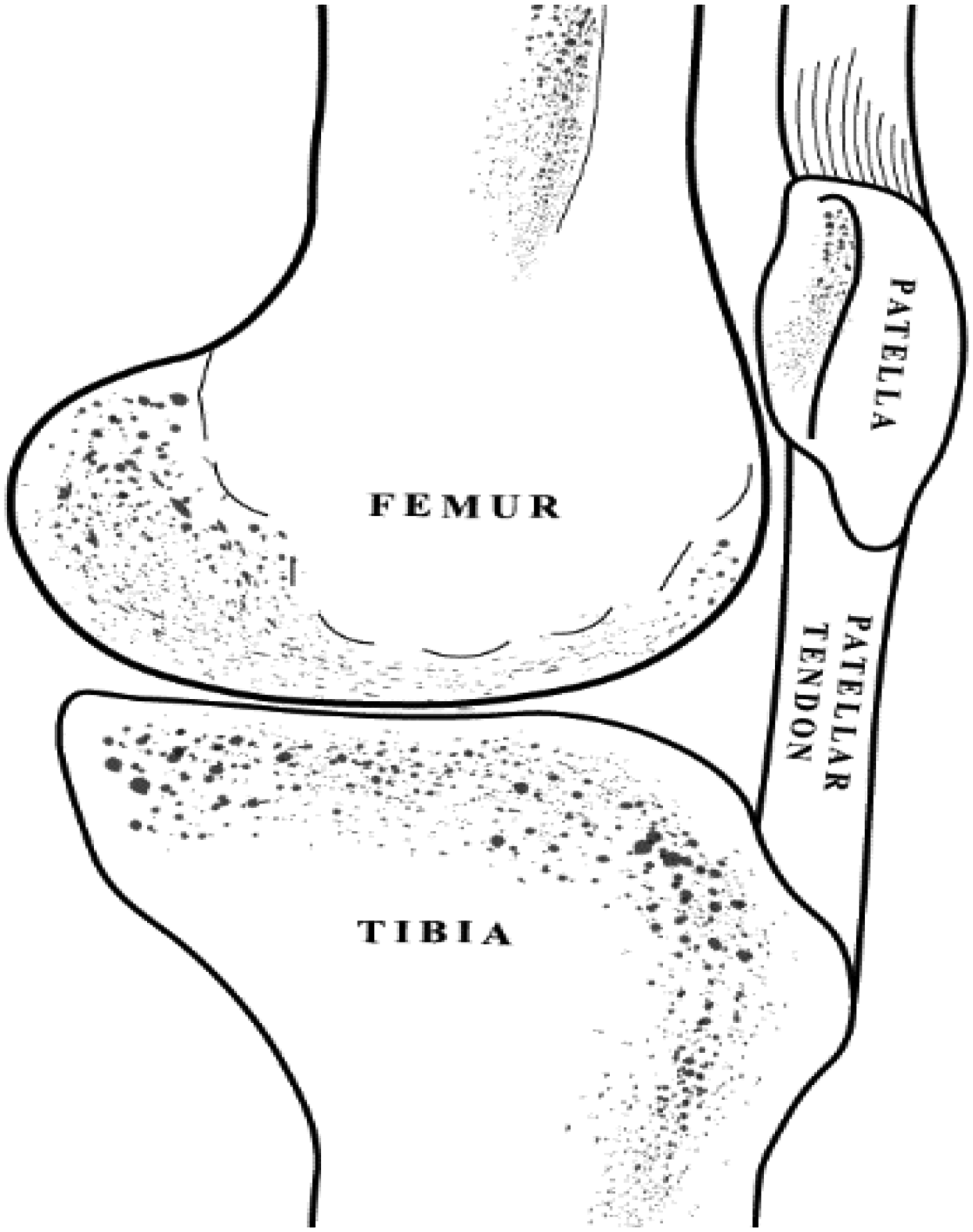
Schematic drawing of the patellar tendon.
As a preliminary study, this research aims to develop a novel technique using the displacement of the patellar tendon as an indirect sign of patellar maltracking and determine if the patellar tendon is displaced in supine and standing positions in persons with PFPS. It also correlates the patellar tendon maltracking with Q angle which assesses the lateral line of pull of the quadriceps relative to the patella.
Methodology
Study design
This is a cross-sectional study. The study was conducted from May to November 2018.
The study protocol was approved by the University of Santo Tomas Hospital-Institutional Review Board.
Participants
Male and females university football athletes aged 18–25 years old were included in the study. Participants with asymptomatic knees and those with PFPS were included. The presence of PFPS was determined using the required core criterion by Crossley et al. 21 which was pain around or behind the patella aggravated by more than one activity that loads patellofemoral joint during weight bearing on a flexed knee such as squatting, stair ambulation, jogging/running, hopping/jumping. Exclusion criteria were the following: lower extremity fractures and patellar dislocations, surgical procedures on the lower extremity, history of recent knee trauma and physical examination consistent with patellar tendinosis, patellar instability (presence of J sign), meniscal, and ligamental lesions.
All subjects underwent a physical examination to rule out the presence of any other lower extremity conditions by a physiatrist and physical therapists of the research team. Q angle was also measured.
Ultrasonographic imaging of the patellar tendon
To prevent the potential decrease in reliability, only one sonologist performed the ultrasound study. CBGS was a registered musculoskeletal sonologist, with at least 10 years of experience in performing musculoskeletal ultrasound. Prior to the study, an intra-rater reliability study was performed. She was blinded to the physical examination of the participants. GE Logiq E-pro ultrasound machine with a frequency of 5–13 MHz and 12L-RS linear array head was used (Milwaukee, USA).
Patellar tendon placement
The participant was placed in supine with the knee flexed at 30° and the ankle joint in a neutral position. To ensure that the trochlea is being measured on the same location, the inferior pole of the patella was used as an external landmark for transducer head placement in both supine and standing positions. The transducer was placed immediately below the inferior pole of the patella where the patellar tendon within the trochlear surface of the femur was visualized in the transverse plane. The midpoint of the patellar tendon and the femoral sulcus were identified and both served as a marker for placement. The femoral sulcus was measured from midpoint to the most medial and lateral edges. It was then divided into three equal parts from midpoint to lateral and medial areas with one assigned to the part nearest to the midpoint and three as the part farthest from the midpoint. A negative or positive sign was assigned if the part was lateral or medial to the midpoint, respectively. A score of 0 was given if the midpoint of the patellar tendon is lying directly at the midpoint of the femoral sulcus. A score of 1 or −1 was assigned if the midpoint of patella was between 0 and 1 or −1; 2 or −2 if the midpoint of the patella was between 1/−1 and 2/−2 respectively and 3 or −3 if the midpoint of patella was between 2/−2 and 3/−3 (Figure 2(a)–(d)). This assessment was also performed in standing position. The location of patella in supine was subtracted with its position in standing to determine if there was a change in the location of the patella with a change in position from supine to standing (Figure 2).
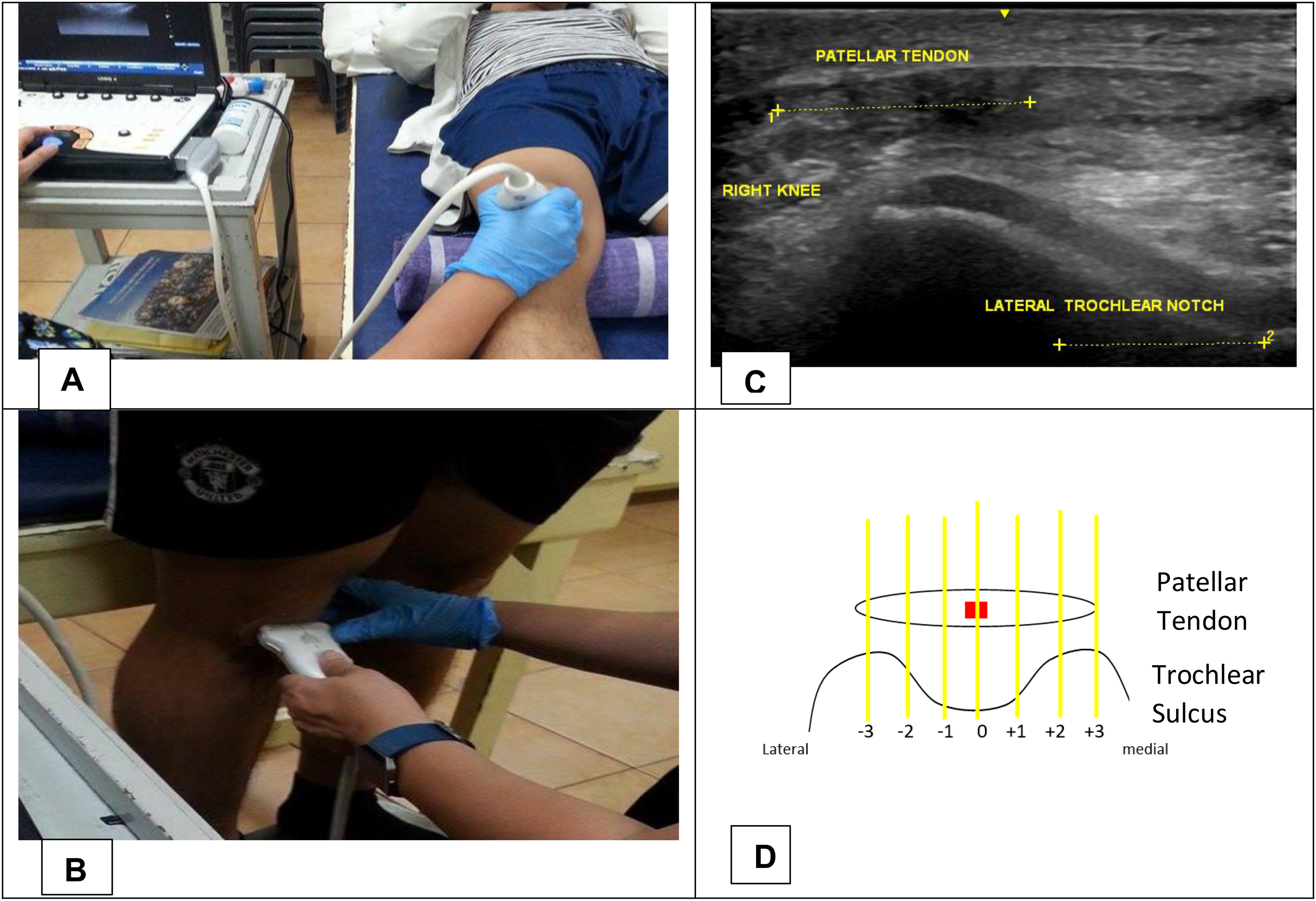
(a, b) Position of the transducer head in supine and standing position; (c) sonographic image of the patellar tendon and trochlear sulcus; (d) schematic drawing of the regions of the trochlear sulcus.
Data analysis
All the data was entered in a purpose-built Excel file. SpSS software was used for the analysis of data. For intra-rater reliability, Cronbach’s α was used. Means, median, and standard deviation were employed for descriptive data, Independent t-test and Mann–Whitney U-test were performed to analyse group differences of those with PFPS and those without PFPS. Pearson’s correlation was used to determine the relationship between Q angle and patellar lateral displacement. Post hoc analysis was done to determine if the number of participants was adequate for an effective size. p value of <0.05 was considered significant.
Results
Intra-rater reliability
An intra-rater reliability testing, which showed high intra-rater reliability (Cronbach’s α = 0.78, intra-class correlation = −0.22–0.977, p value <0.05) was performed prior to the testing.
Participants
There were 20 males and 14 females who were included in the study with both knees of the participants examined. A total of 68 knees were evaluated. There was no statistical difference with age of both sexes. However, the playing years of the male players were significant longer as compared to the females. There was equal number of knees, which were asymptomatic and with PFPs with 34 per group. Q angle of knees with PFPS and without PFPS was 10.97 ± 3.64 and 12.31 ± 3.67, respectively with a p value of 0.91 (Table 1).
Participants' profile.
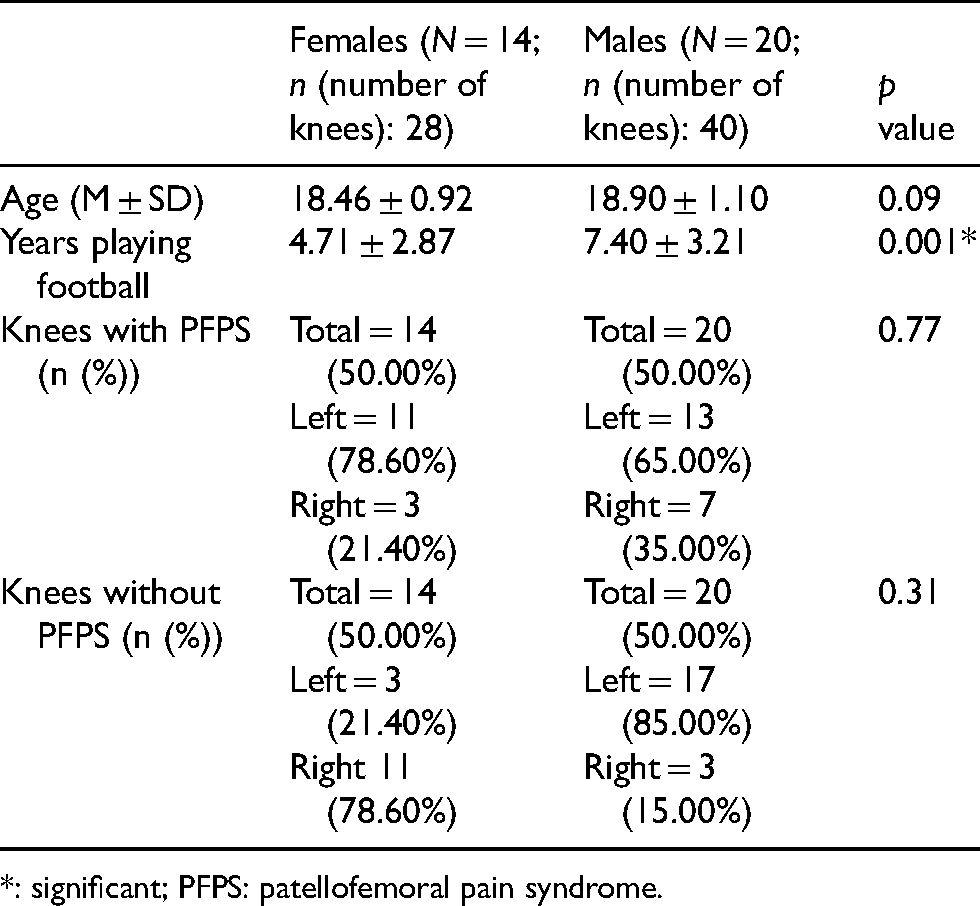
*: significant; PFPS: patellofemoral pain syndrome.
Patellar tendon displacement
A series of Mann–Whitney t-test between knees with and without PFPS on their patellar lateral displacement in supine and standing, and its difference was performed (Table 2). It showed a significant difference in the patellar lateral displacement during standing which was larger for subjects with PFPS (Mean Rank = 39.20, Median = −2) than for those without PFPS(Mean rank = 30.32, Median = −2), U = 425.50, p = 0.02. There was no significant difference between the two groups for patellar lateral displacement in supine and the patellar lateral displacement difference from supine to standing. Patellar displacement in supine is not larger for the PFPS group (Mean Rank = 35.02, Median = −1) than for those without PFPS (Mean Rank = 34.04, Median = −1), U = 559.50, p = 0.82. The difference in the patellar lateral displacement from supine to standing positions was not larger in the PFPS group (Mean rank = 32.88, Median = 1) when compared to the non-PFPS group (Mean Rank = 35.94, Median = 1), U = 524.00, p = 0.44.
Displacement of the patellar tendon.
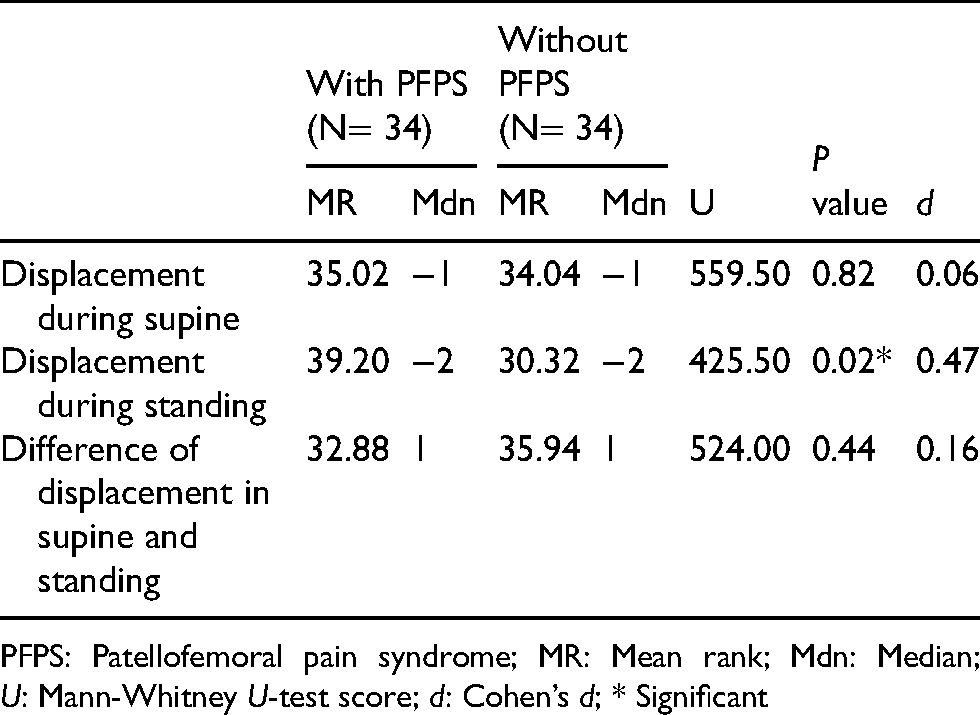
PFPS: Patellofemoral pain syndrome; MR: Mean rank; Mdn: Median; U: Mann-Whitney U-test score; d: Cohen’s d; * Significant
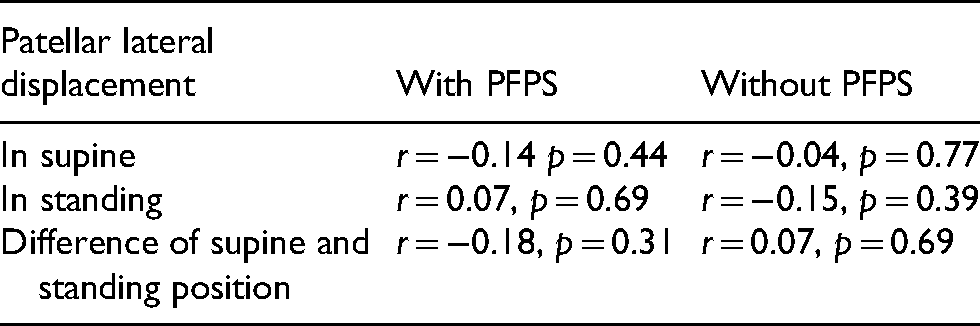
There was no correlation between Q angle and lateral displacement of patellar tendon in all the positions (Table 3).
Pearson correlation of Q angle and lateral displacement of patellar tendon in supine, standing, and the difference of supine and standing position.
Post hoc sample size analysis
The results of the Mann–Whitney U test were subjected to a post hoc analysis of sample size adequacy. Using Cohen’s d (G*Power ver 3.1.9.7), there was moderate effect size (d = 0.47) for patellar lateral displacement in standing.22,23
Discussion
The aim of the study was to develop a novel technique to assess patellar maltracking using ultrasound that could be easily performed by clinicians managing PFPS using the same principles of the bisect offset index, TT–TG and PT–TG distances and to determine if there is a difference in between participants with PFPS and those are asymptomatic using this technique.
Realizing that the limitation of sonography in its inability to visualize the patella in the transverse view as it rests in the trochlear sulcus has led the authors to use the patellar tendon as proxy structure of the patella. This is based on the hypothesis that the direction of the patellar will also be the direction of patellar tendon because of its origin from the inferior pole of the patella and that the proximal part of the patellar tendon is still within the femoral trochlear sulcus.
We used the principle of the bisect offset, TT–TG and PT–TG distances. The bisect offset measures the medial/lateral displacement of the patella in weight-bearing and non-weight-bearing positions using MRI. 24 The similarity with the technique the authors developed was that the midpoint of the femoral sulcus was used as the reference point. Whereas in the bisect offset index, the line from the trochlear sulcus was extended up to the patella and the patella width that is lateral to this line is divided by the total patellar width. Larger bisect offset value means that the patellar is more displaced laterally and 65% has been set as its cut-off. 24 Our method used the midpoint of the trochlear sulcus and divided the sulcus into three equal regions, medial and lateral to the midpoint. It then located the midpoint of the patellar tendon and determined which region of the trochlear sulcus it is situated.
The TT–TG distance which is being used to assess patellar instability is recently being studied with its correlation to PFPS. The distance corresponds to the distance between the line which passes through the deepest part of the trochlear groove which is at the right angle to the tangent along the posterior femoral condyles and the line passing through the most anterior portion of the tibial tuberosity. The first line is transferred to the most superior axial slice where the second line is drawn. 10 Our technique and the TT–TG used the trochlear sulcus as a reference point but our technique used the midpoint of the trochlear sulcus while TT–TG distance used the deepest part of the trochlear groove. The study of Carlson showed that TT–TG distance was greater in those with PFP as compared with health control (13.0 ± 3/6 mm vs. 10.8 ± 3.0 mm, p = 0.001).10 While the study of Tahmasebi et al. (2019) showed that TT–TGD was 12.3 ± 3.3 mm in patients with PFP and 9.3 ± 2.4 mm in controls (p value <0.001). 11 The studies concluded that the TT–TG distance could be used to assess patients with intractable anterior knee pain.
A newer technique which is the PT–TG distance is being compared to the TT–TG distance for reliability. This is due to the fact that the patellar tendon has well-defined borders and is inserted lateral to the most anterior aspect of the tibial tubercle. Furthermore, the midsection of the patellar tendon is more reliable during measurement.15,16 This is similar to the TT–TG distance where a first line is drawn from the lowest point of the femoral trochlea which was perpendicular to the tangent of the posterior femoral condyles. This line was maintained up to the most superior axial cut where the patellar tendon attaches to the tibial tuberosity. A second line was drawn at the midsection of the patellar tendon. The distance between the two lines is the PT–TG distance. This technique is most similar to our technique because it uses both the patellar tendon and the trochlear groove. However, researches have only focused on the reliability of this technique as compared to the TT–TG distance which showed better inter-rater and intra-rater reliability.15,16 Future studies are needed to verify its correlation with PFPS.
Clinical examination and special tests have been used in assessing patellar maltracking in patients with PFPS. However, they may not be valid objective measures. A systematic review by Smith et al. (2008) was able to identify 18 diagnostic tests for patellar instability and only five of these were assessed for validity. The authors were not able to conclude which of the tests is most valid and recommended that more studies are needed in order to determine the most appropriate test for patellar instability. 25 A study by Draper et al. 26 showed that which clinically classified patients as having patella maltracking using patellofemoral arthrometer had inconsistent results when compared with the bisect offset index results. Three participants clinically diagnosed to have maltracking had to bisect offset index that was not statistically different from the control while five participants who were diagnosed as maltrackers using arthrometer had an increased bisect offset index as compared to the controls. This affirms the need of a more precise method of assessing patellar motion.
Imaging techniques such as x-ray, ultrasound, CT scan and MRI have been used in assessing patellar maltracking. As previously stated, bisect offset index is the most valid parameter in its assessment. However, an open configuration upright MRI scanner with real-time imaging or cine phase-contrast MRI is being utilized and aside from the cost, it is not readily available in most settings. This has been one of the major limitations of researches in PFPS.
Sonography has been used in studies about PFPS which focused on quadriceps muscle and the lateral retinacular ligament with conflicting results. Jan et al. 18 studied the characteristics of vastus medialis obliquus, namely, insertional level, fiber angle, and volume of patients with PFPS as compared to normal individuals and revealed that all these parameters were significantly smaller in the PFPS group (p value <0.05). The thickness of the lateral retinacular ligament and its association with PFPS showed that there is an increase in thickness of the lateral retinacular ligament with patients with PFPS although it was non-significant. 19 No study, to our knowledge, has assessed patellar maltracking in PFPS. Our technique assessed the lateral/medial translation of patellar tendon as an indirect sign of patellar maltracking.
In our study, significant lateral displacement of the patella tendon was seen with the knee in full extension weight-bearing position. This is similar to the studies of Becher et al. 27 and Draper et al. 5 using open configuration upright MRI. Becher et al. 27 showed that there was a significant effect of weight bearing of the bisect offset index. There was an increase of 13.8% ± 10.3% in those with patella instability and 11.7% ± 5.3% in the control group (p value ≤0.001). 27 Draper et al. 5 showed that those who are maltrackers (bisect offset index of more 65%) had 5% greater lateral displacement in standing and weightbearing activity as compared when measured in supine position in flexion angle between 25° and 30° with p value of <0.001). However, with those with normal bisect offset index classified as non-maltrackers had 7% greater bisect offset index in supine position as compared to upright position.
Changes in patellar maltracking in standing has been associated with vastus medialis activation and decrease in hip abductor strength. The studies analyzing muscle activity have used weight-bearing activities.6,28 Pal et al. 6 showed that there was a significant relationship between patellar maltracking and vastus medialis activation delay during walking (R2 = 0.89 and p value <0.001) in participants with PFPS where both patellar tilt and bisect offset index were abnormal. The study of Nakagawa et al 28 demonstrated that there was a 5.7% diminished activation of the gluteus medius (p value <0.05) in females with PFPS as compared to controls during single-leg squat. However, no difference was seen in the male groups.
This could be also explained by the screw home mechanism which causes either external rotation of the tibia or internal rotation of the femur in full extension of the knee. More lateralization of the patellar tendon and tibial tubercle is produced. 12 Furthermore, a study by Camathias et al. 13 in 20 human cadavers showed that full extension with external rotation (10.9 ± 4.8 mm) gave the highest value of the TT–TG distance as compared with full extension with neutral or internal rotation (7.8 mm ± 3.4 mm vs. 5.4 ± 2.3 mm) and 30° flexion with internal or external rotation.
The limitations of our study are the following: (1) The authors were not able to determine the effects of trochlear dysplasia as a factor associated with PFPS. The study of Harbaugh et al. 29 showed that measures of trochlear dysplasia had a higher prevalence in patellofemoral pain. But there was no statistical difference between asymptomatic and the maltracking cohorts which may due to the fact that the participants in this study who were maltrackers did not have gross patellar instability. This is also the case for our participants since those with excessive lateral tracking were excluded in the study. (2) The authors evaluated the patellar tendon in the supine position with knee in 30° flexion. This is the recommended position in assessing the knee. However, the study of Becher et al. 27 showed that results of the bisect offset index is significantly reduced if the knee is flexed at 45° regardless of weight-bearing status. Likewise, the patellar tendon was only assessed in full extension during standing. It is, therefore, recommended that future studies assess the effect of knee joint angle and weight-bearing status on patellar tendon displacement.
Future directions for this research include the following: First, the validity of this technique should be assessed by comparing it with the bisect offset index, TT–TG and PT–TG distances using MRI. Second, to establish which technique of computation in assessing lateral/medial displacement of the patellar tendon is the most valid. There are three possible ways which it could be measured which are (a) the technique which was presented in this study; (b) using the technique which is similar to the bisect offset index which is the percentage of the patellar width lateral to the midpoint of the trochlear sulcus; and (c) using true value of the difference of the midpoint of the trochlear sulcus and the midpoint of the patellar tendon like the TT–TG and PT–TG distances.
This technique developed by the authors is easily performed. If proven valid, it could be used to determine the effectiveness of the management of PFPS and in research to further progress the understanding of the pathomechanics and treatment of PFPS.
Footnotes
Acknowledgement
The authors would like to thank Jose Ma. D. Ramos, OTRP, MBAH for the illustration he has drawn for the paper. We would also want to thank GE Healthcare Philippines for providing the ultrasound machine used in this research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Commission on Higher Education
Ethical approval
The study protocol was approved by the University of Santo Tomas Hospital-Institutional Review Board.