
Abstract
Background
Distal radius fractures have been reported as a predictor of subsequent osteoporotic fragility fractures. This retrospective study evaluated the proportion of patients with distal radius fractures at a government hospital in Hong Kong who received diagnostic evaluation or treatment for osteoporosis within 1 year.
Methods
Five hundred sixty-one postmenopausal women aged >50 years admitted to a public hospital between 2013 and 2017 for a low-energy distal radius fracture were analysed for initiation of osteoporosis medications and/or arrangement of dual-energy X-ray absorptiometry screening within 1 year of injury.
Results
Within 1 year, 8.4% of patients were prescribed osteoporosis medication and 6.1% of patients had dual-energy X-ray absorptiometry arranged. Patients with a previous fracture were more likely to receive osteoporosis medication (18.6% vs 7.5%, P = 0.012) and either intervention (screening or medication) overall (23.3% vs 10.4%, P = 0.011).
Conclusions
Few postmenopausal women who suffered a distal radius fracture received osteoporosis intervention within 1 year. Orthopaedic surgeons should be aware of the possibility of underlying osteoporosis and opportunity for intervention when managing fragility distal radius fractures.
Keywords
Introduction
In Hong Kong, the prevalence of osteoporosis is steadily growing alongside its aging population, with life expectancy having reached 82.3 and 88.1 years, respectively for males and females in 2019. 1 Postmenopausal Hong Kong women are at particularly high risk, with up to 35.8% of Hong Kong women reported as being osteoporotic, compared to 20% of Caucasian women. 2 Osteoporosis is characterised by decreased bone strength predisposing a person to an increased risk of fracture. 3 Osteoporotic fragility fractures, among which hip fractures are a major cause of morbidity and mortality, pose a major burden to the public healthcare system. Diagnosis of osteoporosis is commonly performed through dual-energy X-ray absorptiometry (DXA) scan, where the T-score of the test denotes the number of standard deviations below the healthy young adult mean for an individual's bone mineral density (BMD). 4 A T-score of 2.5 or lower is indicative of osteoporosis. 5 Treatment of osteoporosis by bisphosphonates has been shown to increase BMD and decrease future fracture risk. 6 Early recognition of risk factors, timely diagnosis and initiation of treatment are therefore of paramount importance, particularly postmenopausal women.
Distal radius fractures (DRFs) have been reported as a predictor of subsequent fragility fractures. 7 While DRFs often limit functions and affect activities of daily living, other fragility fractures such as hip fracture or vertebral collapse are arguably more debilitating and associated with premature mortality. 8 Patients with DRFs have been shown to have almost twice the relative risk of future hip fracture. 7 As such, timely intervention for underlying osteoporosis could potentially lower the incidence of future fragility fractures in high-risk patient groups. 9 Despite this, studies suggest only a small proportion of patients are offered screening and treatment for osteoporosis following a DRF.10,11 In fact, few postmenopausal women are reported to have been offered osteoporosis treatment following fragility fractures in general. 12 Until now, little local data has been published in this regard. The objective of this study was to evaluate the proportion of patients admitted to a major Hong Kong government hospital for an acute DRF who subsequently underwent diagnostic evaluation or treatment for osteoporosis for the first time.
Methods
Ethical approval for this study was waived by our centre’s institutional review board. Informed consent was not required due to the retrospective nature of the study. All data were extracted from Clinical Data Analysis Reporting System (CDARS), the central patient database of the Hong Kong Hospital Authority. The Hong Kong Hospital Authority is a public healthcare institution that provides medical services to the majority of patient loads in Hong Kong. Since 1999, data on hospitalisation, demographics, diagnosis, surgical procedures, and outcomes have been computerised using CDARS, which has demonstrated high positive predictive value in the identification of major fractures with the use of the International Classification of Diseases-9 code algorithm. 13 Inpatient and outpatient medical charts review were performed for all included patients.
All patients admitted to a publicly funded hospital, with the principal diagnosis of DRF during the 5-year period from 1 January 2013 to 31 December 2017 were identified in the CDARS database. Inclusion criteria were women aged 50 years or older with a DRF. Women in this age group were selected based on previous evidence for osteoporosis treatment coming mostly from studies of postmenopausal women.14,15 Exclusion criteria were death within 6 months of fracture, pathological fracture and high-energy trauma (energy greater than fall from standing height) as the cause of DRF. Patients who previously had a DXA scan performed or were previously prescribed osteoporosis medications were also excluded, as our aim was to identify the proportion of patients who were offered osteoporosis screening or treatment for the first time following a DRF. Osteoporosis medication included calcium and vitamin D, all anti-resorptive agents and anabolic agents for osteoporosis.
Baseline parameters including age, sex, history of previous fracture and method of treatment of the index fracture (plaster of Paris or surgical fixation) were abstracted from medical charts by a structured medical record review. Both primary and secondary osteoporosis were considered as a whole in the analysis. The primary outcome was an initiation of pharmacological treatment and/or arranging of diagnostic evaluation via DXA for underlying osteoporosis within 1 year of index fracture, by any doctor across all medical specialties. Most DXA reports at our centre use the femoral neck and lumbar spine for BMD measurement. Osteoporosis medications included calcium, vitamin D and all anti-resorptive agents or anabolic agents for osteoporosis. Time to either intervention from index fracture was also recorded.
All data were anonymised to ensure personal data privacy and entered into an encrypted file. Data analysis was performed using IBM SPSS Statistics version 26 (IBM, Armonk, NY, USA). Categorical data were presented as frequencies and percentages and compared using Pearson Chi-squared (χ2) tests. Continuous data were presented as means ± standard deviations and compared using independent sample t-tests and one-way analysis of variance tests. The comparison of baseline parameters by univariate analysis was performed between patients who received osteoporosis intervention and those who did not. A P-value of less than 0.05 was considered statistically significant. Multivariate analysis by means of binary logistic regression was also performed to estimate the strength of association between the independent variables and intervention outcomes.
Results
Baseline statistics
A total of 1263 patients were identified in the CDARS database from 1 January 2013 to 31 December 2017 with DRF coded as the primary diagnosis. Further evaluation excluded the following: 433 male patients, 89 patients under 50 years of age, six patients with high-energy trauma as a cause of DRF, six patients who died within 6 months of follow-up, and 134 patients with previous DXA or osteoporosis medications. A further 34 patients were excluded for miscellaneous reasons such as loss to follow-up, non-acute fractures or old injuries, and non-DRF status (such as wrongly coded scaphoid or distal ulna fractures). None of the patients suffered from a pathological fracture. The final pool for analysis consisted of 561 patients who met the inclusion criteria.
Baseline patient characteristics are presented in Table 1. Two-thirds of patients were between 50 and 69 years old. A total of 7.7% had a history of the previous fracture in the wrist or any other parts of the body, of which 79% of patients suffered from common fragility fractures including hip, pubic rami, proximal humerus, contralateral distal radius and vertebral collapse. The other 21% were miscellaneous fractures, such as patella and ankle fractures. Further fracture subclassification was not performed in the analysis since the authors believed most clinicians would be more inclined to start osteoporosis interventions when the DRF was already the patient's second fracture, regardless of whether the first was a fragility fracture. A total of 53.5% of patients had surgical fixation of the index fracture. The reason for surgical fixation was not included in the analysis.
Baseline patient characteristics.
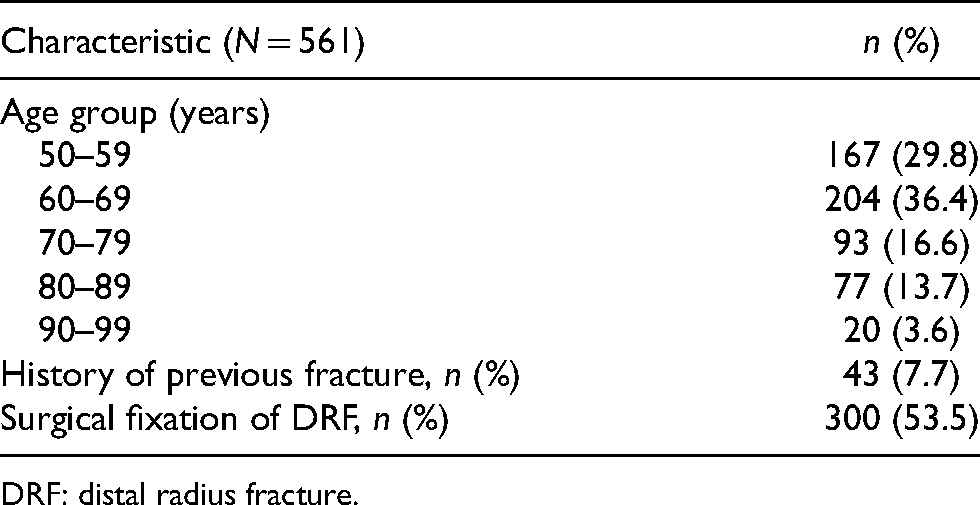
DRF: distal radius fracture.
Outcomes
Forty-seven patients (8.4%) were started on osteoporosis medication within 1 year (Table 2). Of these patients, only three were started on bisphosphonates or denosumab; the remainder were started on calcium and/or vitamin D only. Average time to initiation of osteoporosis medication from injury date was 113.0 ± 111.6 days (range 2–365 days). Thirty-four patients (6.1%) had DXA scans arranged within 1 year. Among those who received DXA, 20.7% had normal bone mass (T-score greater than or equal to −1.0), 48.3% were osteopenic (T-score between −1.0 and −2.5) and 31.0% were osteoporotic (T-score less than or equal to −2.5). Five patients defaulted their DXA scan appointment. Average time from index fracture to DXA scan arrangement was 78.5 ± 84.8 days (range 2–313 days). Sixty-four patients (11.4%) received either osteoporosis intervention (medication initiation and/or DXA arrangement) within 1 year. The annual proportion of patients receiving osteoporosis intervention increased across the study period from 2.2% in 2013 to 16.4% in 2017 (Figure 1). Average time from index fracture to either osteoporosis intervention was 108.3 ± 107.9 days (range 2–365 days).
Percentage of patients receiving any osteoporosis intervention within one year of distal radius fracture.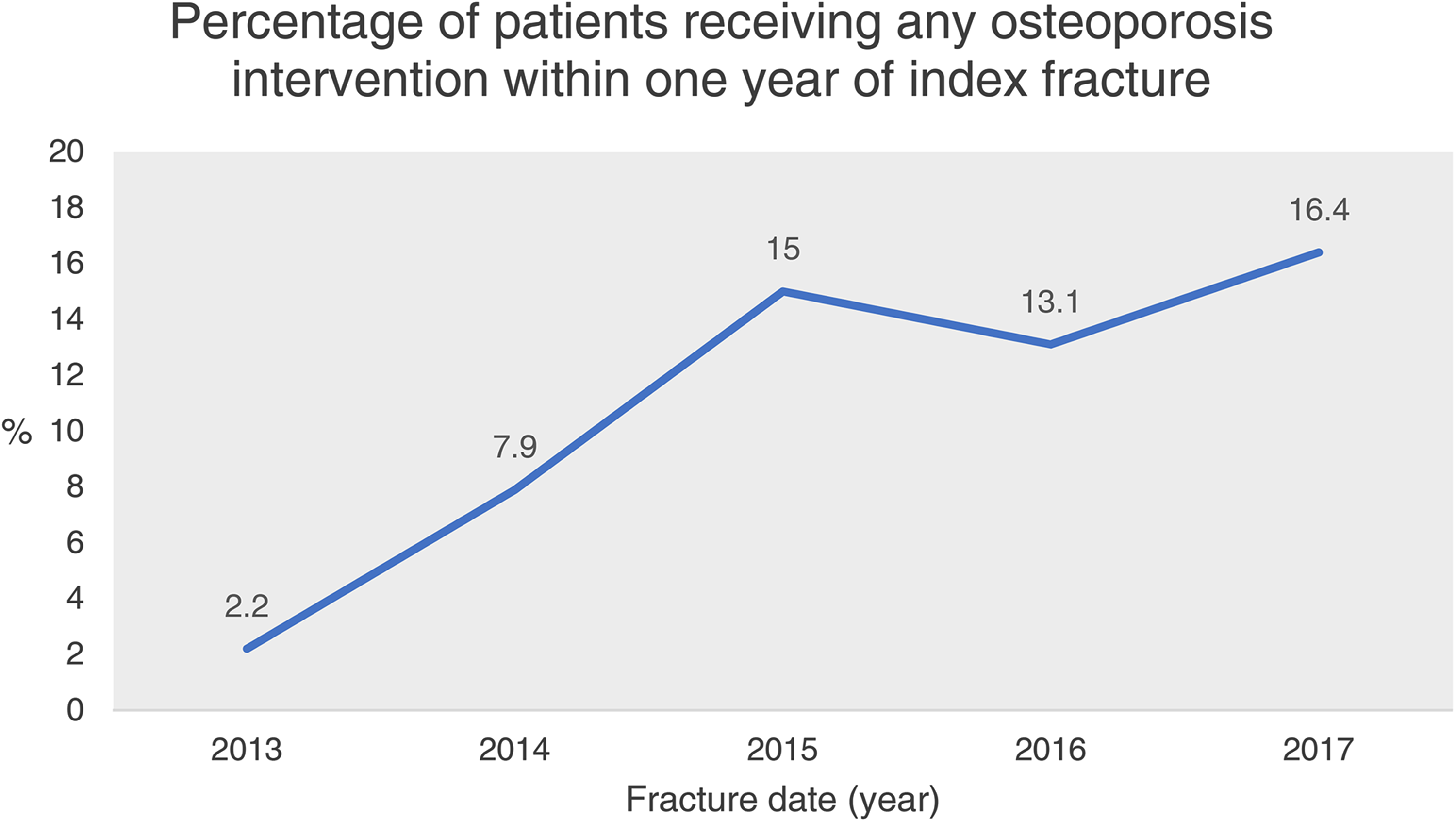
Osteoporosis interventions within 1 year of DRF.
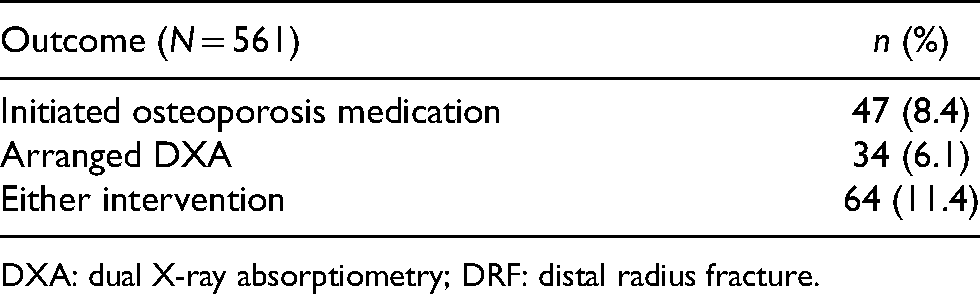
DXA: dual X-ray absorptiometry; DRF: distal radius fracture.
Factors predicting rate of osteoporosis intervention
Patients with a previous fracture history were significantly more likely to be started on osteoporosis medication (18.6% vs 7.5%) (P = 0.012, χ2) (Table 3) and either osteoporosis intervention as a whole (23.3% vs 10.4%) (P = 0.011, χ2). Older age was also associated with a higher rate of initiation of osteoporosis medication (P = 0.007, χ2), with the exception of the 90–99-year-old age group. Treatment method for the index fracture was not associated with a rate of osteoporosis intervention considered either separately or as a whole. No baseline parameters were associated with a rate of DXA arrangement within 1 year. In the multivariate analysis, history of the previous fracture was associated with receiving either intervention (OR 2.51, P = 0.020), with the association between history of previous fracture and initiation of osteoporosis medication being marginally below statistical significance (OR 2.35, P = 0.051) (Table 4). No significant associations were found between any baseline parameter and time to initiation of osteoporosis medication, time to DXA arrangement or time to either intervention (Table 5).
Chi-square associations between baseline parameters and intervention outcomes.
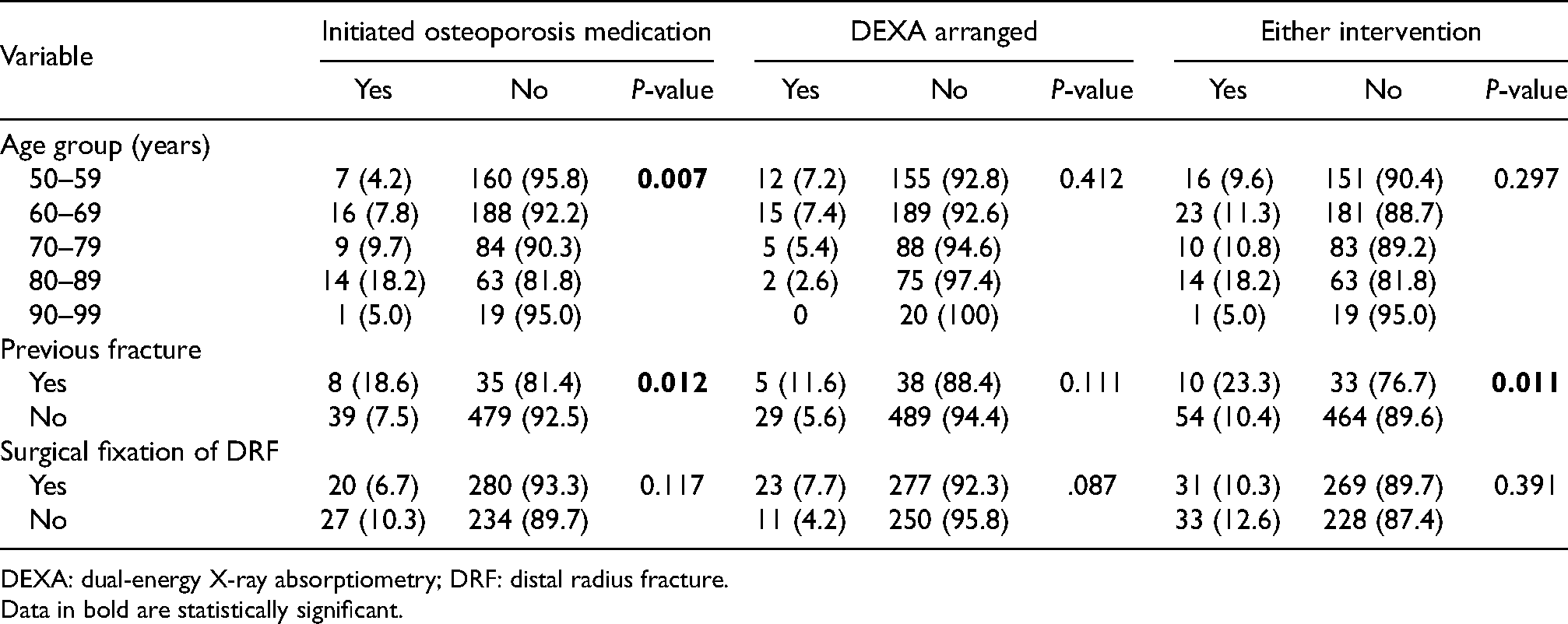
DEXA: dual-energy X-ray absorptiometry; DRF: distal radius fracture.
Data in bold are statistically significant.
Multivariate logistic regression results.
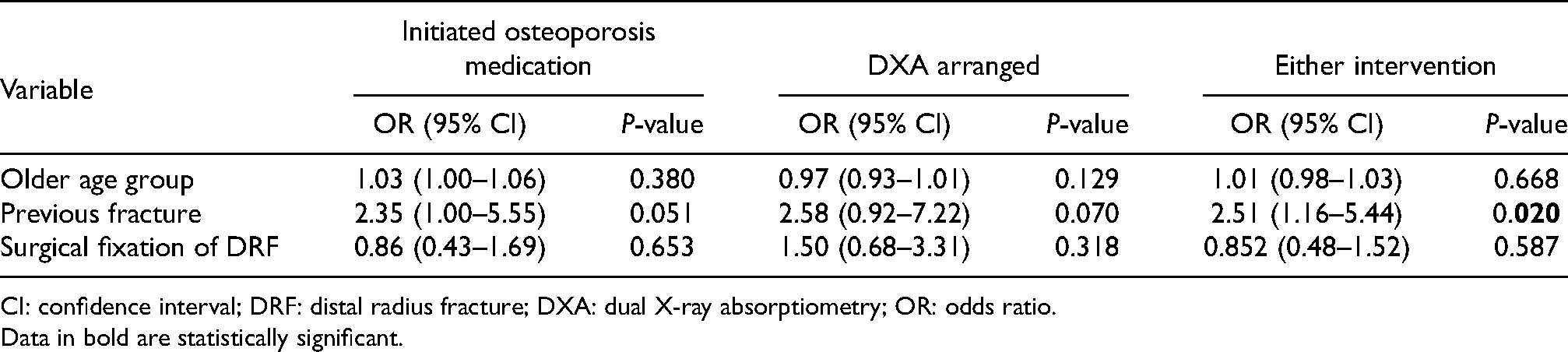
CI: confidence interval; DRF: distal radius fracture; DXA: dual X-ray absorptiometry; OR: odds ratio.
Data in bold are statistically significant.
Relationships between baseline parameters and mean duration to osteoporosis intervention.
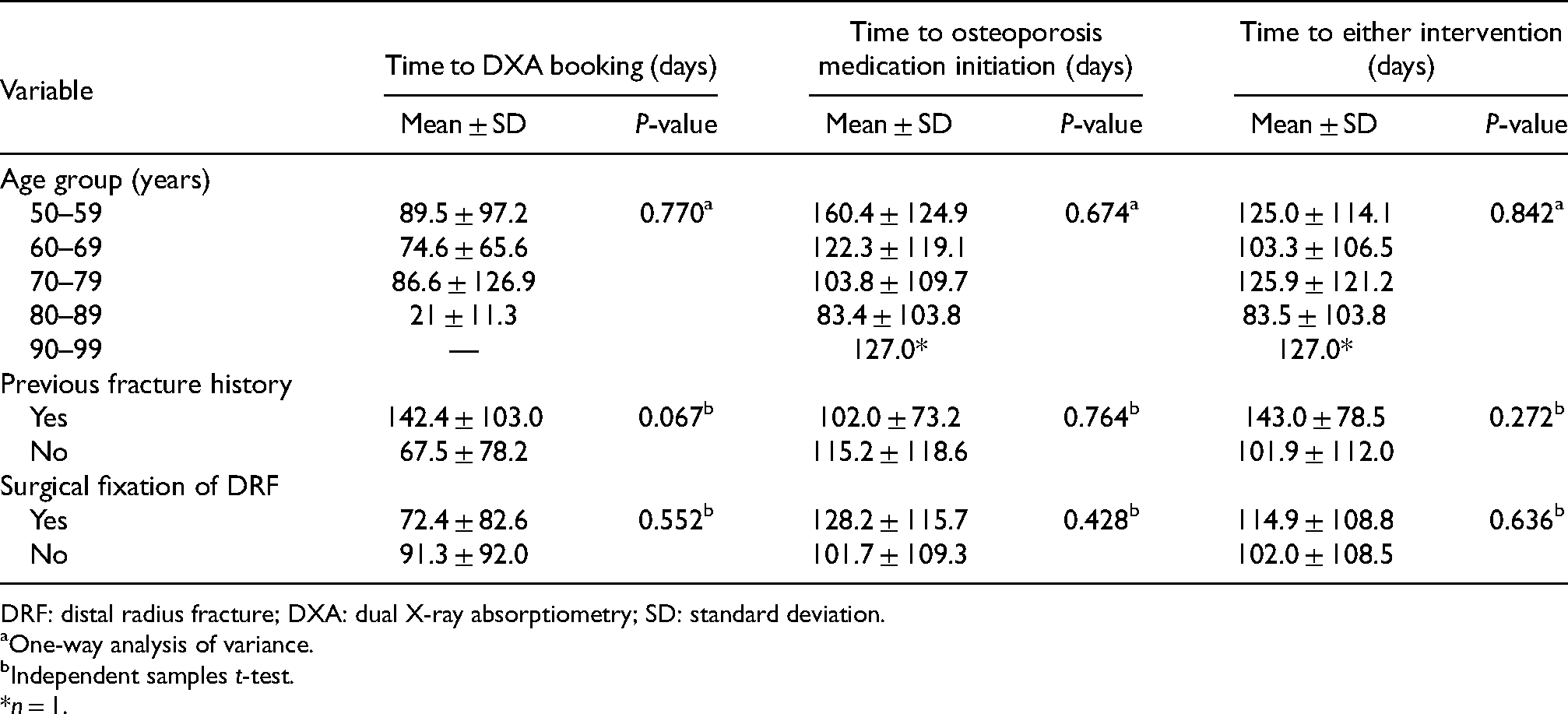
DRF: distal radius fracture; DXA: dual X-ray absorptiometry; SD: standard deviation.
One-way analysis of variance.
Independent samples t-test.
*n = 1.
Discussion
This retrospective study revealed a concerningly low proportion of postmenopausal females who received diagnostic evaluation or initiated medication for osteoporosis within 1 year of a DRF. Only 8.4% of patients were started on an osteoporosis medication, and the majority of these were supplemental calcium or vitamin D. Taking into account only anti-resorptive or anabolic agents, the rate of medication initiation within 1 year was as low as 0.5%. Average time to either intervention was over 3 months from the date of the index fracture, representing a considerable delay from the time that a significant predictor of osteoporosis risk was present. Older age was associated with a higher rate of intervention, with the exception of the 90–99-year-old age group. This was likely due to members of this age group having poorer premorbid health statuses, increased risk of cardiovascular events, and the desire to avoid polypharmacy. History of a previous fracture was also associated with a greater likelihood of intervention.
With increasing awareness of the public health burden posed by undetected osteoporosis, more studies worldwide are finding similarly low rates of preventative measures offered by clinicians in response to fragility fractures.10,16,17 This is seen not only in low-trauma fractures such as DRFs, but hip fractures as well. 18 A 2013 publication by the International Osteoporosis Foundation, which summarised the national audits of secondary fracture prevention in 10 countries, paints a clear picture that even in developed regions with generally adequate healthcare resources, secondary fracture prevention following osteoporotic fragility fractures is lacking. 17
Treatment offered by orthopaedic surgeons during acute hospital admission typically focuses on assessing the injury and selecting the optimal treatment to achieve good bony union. Subsequent outpatient assessment usually consists of reassessing functional and radiological status, and rehabilitation planning. When patients regain satisfactory upper limb function and bony union, they are often discharged without further follow-up. Only when patients later suffer a subsequent and often more debilitating fracture are surgeons likely to acknowledge the severity of disease progression and intervene. This scenario holds especially true in Hong Kong's public hospitals, with the ever-increasing volume of fragility fractures and degenerative orthopaedic conditions in outpatient clinics. In a 2013 study of postmenopausal women who were hospitalised for low-trauma fractures across eight Asian regions, Hong Kong was found to have the lowest rate of body mass index testing and the second-lowest rate of osteoporosis medication prescription in the 6 months following hospital discharge. 18
Because care pathways following acute fractures often lead to consultation with an orthopaedic surgeon, these clinicians are in a unique position to funnel patients into an appropriate osteoporosis care system. Unfortunately, data from around the world shows that this system often does not exist in practice. Several reasons have been cited for this, including orthopaedic surgeons’ lack of comfort in providing ongoing management for patients who have suffered an acute fracture and a preference for primary care providers and endocrine specialists to do so. 19 Clinicians frequently lack formal guidelines and referral linkages necessary to provide comprehensive ongoing care, 20 contributing to a lack of clarity about clinician roles. The result is a fragmented system of care in which patients who ought to receive ongoing reassessment fall through the cracks and go on to develop additional, more serious fractures. In our study, mean duration to osteoporosis intervention was not associated with any baseline parameters, including age group or history of previous fracture. We included this in our analysis to evaluate whether there were any baseline factors that would trigger clinicians to start intervention earlier. However, the result is unsurprising as there were no formal guidelines or protocols for osteoporosis management following acute DRFs in our hospital. Intervention often, therefore, relied on the surgeon noticing the unmanaged osteoporosis during follow-up. At the clinician level, it is important that surgeons be aware of the risk of unmanaged osteoporosis and the options for treatment, however, it would further benefit patients if standardised protocols for osteoporosis management were applied for all DRFs and designated staff were responsible for arranging osteoporosis assessment.
These deficiencies at the system level highlight the need for better coordination of fracture care between institutions and clinicians that allows for thorough and continuous assessment and reassessment following an initial fracture. Fracture liaison services (FLSs) have recently been implemented successfully in many countries and are reported to be cost-effective or cost-saving. The aim of an FLS is to identify patients with initial fragility fractures and provide long-term education, monitoring and treatment via a multidisciplinary care pathway. 21 Unfortunately, this system has not been widely implemented in Hong Kong. As of 2013, only 10–25% of hospitals in Hong Kong were estimated to have an FLS. 22 Established FLS models have been described by the International Osteoporosis Foundation Capture the Fracture campaign, where the Best Practice Framework sets the benchmark and outlines the recommendations for effective FLS implementation. 17 As of 2005, the American Orthopaedic Association has operated a nationwide ‘Own the Bone’ registry since 2005 which identifies patients with fragility fractures and coordinates FLS for osteoporosis treatment. 23 The registry has proven successful in raising awareness of healthcare professionals regarding osteoporosis and has led to increased diagnosis and treatment initiation. 24 Fortunately, in our study we observed the proportion of patients receiving osteoporosis intervention has gradually increased over the years. This may reflect increased awareness of osteoporosis in both doctors and the general public. While FLSs alone cannot solve Hong Kong's issues of underdeveloped primary care and overwhelmed specialist outpatient clinics, they are a good starting point for identifying at-risk patients and preventing them from slipping through the cracks after their first fracture heals.
Our study was limited by the fact that only recruited patients who were admitted to either Accident and Emergency Department or Department of Orthopaedics and Traumatology were recruited. Patients who were referred directly from community clinics to our trauma outpatient specialist clinic were not recruited. Both groups of patients, however, were cared for by the same team of surgeons in the same clinical setting. Hence, there should be no significant difference in the treatment of both groups of patients. In addition, treatment information from private medical centres was not included in the analysis unless documented in the admission notes or outpatient consultation records. This includes fractures treated in the private sector, DXA scans performed in private centres, and patients seeking further treatment in the private sector without follow-up in a public hospital. The proportion of these patients remains unknown.
In conclusion, a low percentage of postmenopausal females suffering from acute DRFs were offered diagnostic evaluation (6.1%) or initiation of treatment (8.4%) for underlying osteoporosis within 1 year. Older patients and patients with previous fractures were found to have higher rates of osteoporosis medication initiation, while patients with a previous fracture were found to be more likely to receive osteoporosis intervention overall. Surgeons should be made aware of the possibility of underlying osteoporosis and opportunity for intervention when managing DRFs. Clinical guidelines should be put in place to facilitate recognition and intervention.
Footnotes
Acknowledgements
The authors thank Dr Fred Lui, Dr Jun Lau and Dr Lei Ma for their assistance with data collection.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval
This study was given ethical approval by the Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster (IRB Reference no.: UW 20-429).
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Availability of data and material
The data supporting the findings of this study are available from the Hong Kong Hospital Authority, but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are available from authors upon reasonable request and with permission of Dr Christian Fang.