
Abstract
Introduction:
Geriatric patients with a fragility fracture of the hip (FFH) are especially prone to sarcopenia with poor functional outcomes and quality of life. We assessed the prevalence of sarcopenia in older South African patients with FFH. Risk factors for sarcopenia were also investigated.
Materials and Methods:
From August 1 to November 30, 2018, all older patients with FFH were invited to participate. Sarcopenia was diagnosed based on the revised criteria of the European Working Group on Sarcopenia in Older People (EWGSOP2). Handgrip strength (HGS) and muscle strength were assessed. Muscle quantity was determined by dual-energy X-ray absorptiometry. Demographic information was collected, and 25-hydroxyvitamin D (25[OH]D) status was determined.
Results:
Of the 100 hip fracture cases, 65 were enrolled, and 52% (34/65) were sarcopenic (women: 62%; men: 38%). HGS accurately identified sarcopenia (sensitivity and specificity: 100%). Patients >80 years of age had a prevalence of sarcopenia twice (18/21 [83%]) that of younger patients (18/44 [36%]). Women with sarcopenia were smaller than those without (weight: p < 0.001; height: p < 0.001; body mass index: p = 0.018). Low 25(OH)D was almost universally present, with median 25(OH)D levels significantly lower in the patients with sarcopenia (27 nmol/L [interquartile range {IQR}: 20–39] vs. 40 nmol/L [IQR: 29–53]). Several risk factors, including advanced age; female sex; a smaller body size, especially among women; limited physical activity; and low 25(OH)D levels, were identified.
Discussion:
The accuracy of HGS testing in this cohort underscores EWGSOP2’s recommendation that muscle strength is key to sarcopenia. Further study and follow-up are required to determine the clinical relevance of sarcopenia among FFH patients.
Conclusion:
The prevalence of sarcopenia in our FFH population is high. Sarcopenia is associated with poor patient outcomes following surgical intervention. Orthopaedic surgeons should therefore be cognizant of the presentation and associated risk of sarcopenia as our patient populations age.
Introduction
Sarcopenia is a progressive and generalized skeletal muscle disorder that is associated with an increased likelihood of adverse outcomes including falls, fractures, physical disability, and mortality. 1
The European Working Group on Sarcopenia in Older People published a revised operational definition for sarcopenia as well as changed cutoff points for diagnostic purposes in 2019 (EWGSOP2). 1 Low muscle strength is regarded as the primary parameter of sarcopenia and is deemed the most reliable measure of muscle function. The diagnosis of sarcopenia is confirmed by the presence of low muscle quantity or quality. To diagnose sarcopenia, the presence of both reduced muscle strength and reduced muscle quantity or quality are required.
Limited attention has been paid to sarcopenia in the orthopaedic literature in the context of hip surgery for fragility fractures of the hip (FFH). This may be due to the absence of a clearly defined clinical consequence of sarcopenia. Fragility fractures result from low-velocity trauma caused by mechanical forces that would not ordinarily result in fracture. The World Health Organization has quantified this as forces equivalent to a fall from a standing height or less. 2,3
Sarcopenia is especially common in older people, with reported prevalence rates ranging between 5% and 13%, 4 and present in up to 44% of patients undergoing orthopaedic surgery. 5 A 3-fold increase in the risk of falls, a 4-fold increase in the risk of disability, and a significant increase in the risk of postoperative morbidity and mortality 6 -10 have been ascribed to sarcopenia. Patients with sarcopenia are particularly vulnerable in the setting of major physiologic stressors such as trauma, surgery, or surgical complications. 11
Sarcopenia has also been identified as an independent predictor of both patient expense and hospital costs, especially in a post-operative setting. 12 Evidence indicates that sarcopenia prolongs in-hospital stay with a mean additional duration of 3 days, with hospitals operating on a negative margin when patients with sarcopenia are admitted for surgical procedures. 12 In addition, older trauma patients with sarcopenia are more likely to require frail care facilities after discharge from hospital, which further adds to the total healthcare costs. 13
The incidence rate of FFH appears to be stabilizing in more developed countries 14 ; however, it is projected that the burden of FFH will shift to developing countries such as Latin America, Asia, and Africa. A recent multicenter, multi-ethnic study conducted in South Africa confirmed a significant increase in the incidence rate of hip fractures, with a current incidence rate of 68.6 per 100 000. 15 It is predicted that in 2050, 70% of over 6-million predicted fractures worldwide will occur in developing countries such as South Africa. 14
Therefore, the primary objective of this single-center study was to determine the prevalence of sarcopenia following hip surgery for FFH in older patients at a tertiary hospital in South Africa. Potential risk factors for sarcopenia were sought as a secondary objective.
Materials and Methods
Study Design and Setting
The study followed a descriptive, cross-sectional design. The study population included patients admitted to the Division of Orthopaedic Surgery at Tygerberg Hospital with FFH from August 1, 2018, to November 30, 2018, who underwent hip surgery. Tygerberg Hospital is a tertiary level hospital that serves as a referral center for more than 3.4 million people residing in the Cape Town Metropole. All patients admitted with FFH were eligible for inclusion in the study provided that written informed consent could be obtained. Patients were excluded if the hip fracture was deemed to be traumatic or pathological, in the case of acute concomitant illness, and if they refused a dual-energy X-ray absorptiometry (DXA) study. The research complied with the World Medical Association Declaration of Helsinki ethical principles for medical research involving human subjects and was approved by the Stellenbosch University Health Research and Ethics Committee (HREC ref S18/03/065).
Sarcopenia Assessment
The EWGSOP2 proposes a Find-Assess-Confirm-Severity (FACS) approach across clinical practices and research studies. 1 As sarcopenia was assessed in our total cohort, the case finding part of the proposed strategy was not required (Figure 1). A physical performance test (e.g., gait speed) was not practically possible because the recent FFH and the severity of sarcopenia were not evaluated in the present study.
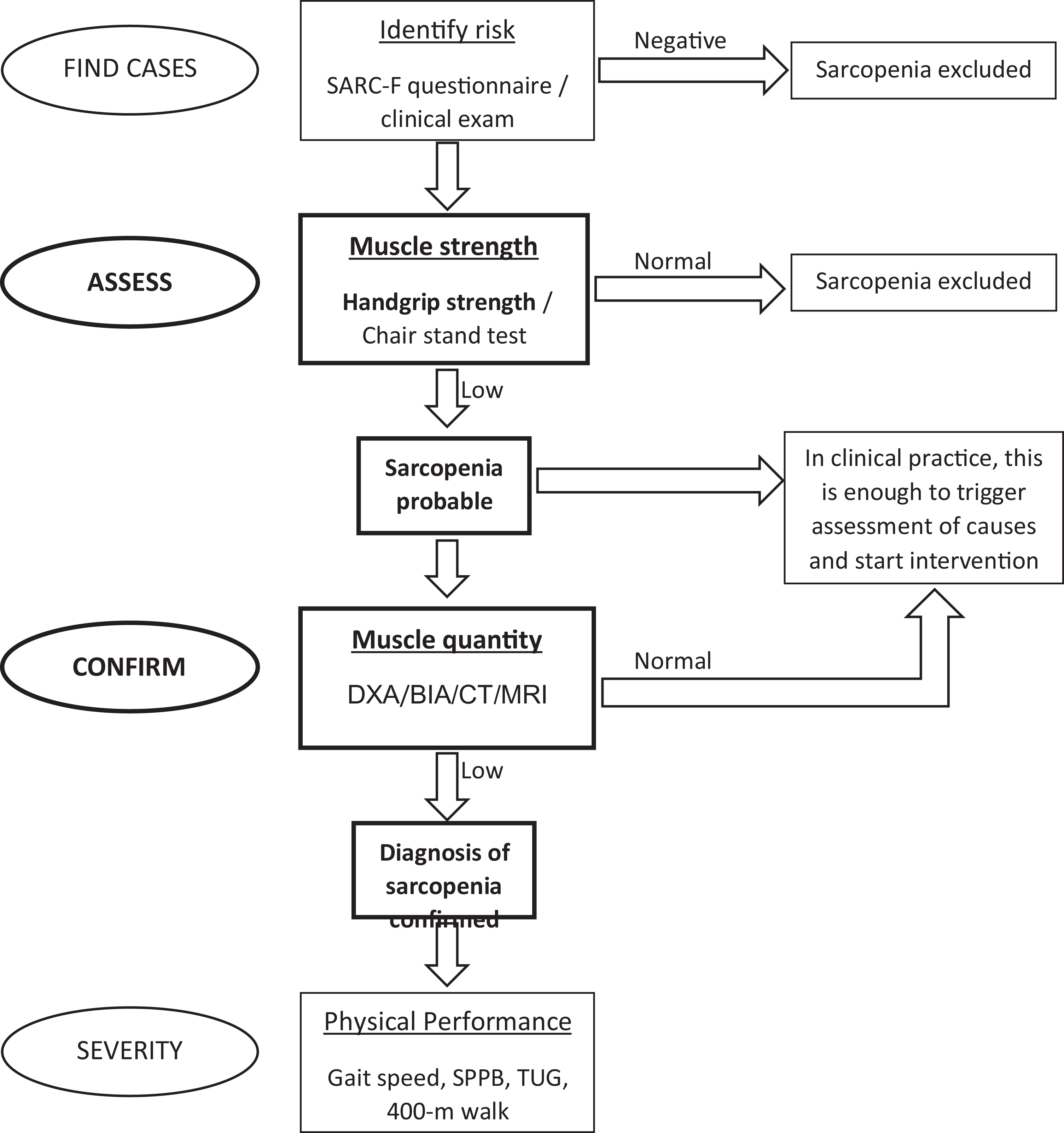
Find-Assess-Confirm-Severity approach proposed by the EWGSOP2. Figure adapted from Cruz-Jentoft AJ et al. Sarcopenia: Revised European consensus on definition and diagnosis.1 Steps taken and tests performed in this study highlighted and indicated in bold text. DXA: dual-energy X-ray absorptiometry; BIA: bio-impedance analysis; CT: computed tomography; MRI: magnetic resonance imaging; SPPB: short physical performance battery; TUG: timed-up-and-go test.
Sarcopenia was regarded as probable in the presence of low muscle strength and confirmed in the presence of both low muscle strength and low muscle quantity.
Muscle strength was assessed by measuring handgrip strength (HGS) with a Jamar Hydraulic Hand Dynamometer (JLW Instruments, Chicago, IL). A validated protocol of the American Society of Hand Therapists was followed. 16 HGS was measured in the sitting position with the elbow flexed at 90° and the wrist in the neutral position. Patients were asked to apply the maximum HGS with the left and right hands, respectively. The measurements were repeated 3 times for both hands. A resting interval of 30 s between each measurement was allowed. The maximum measured HGS of either hand was used to indicate the patient’s HGS. An HGS of <27 kg in men and <16 kg in women denotes low muscle strength in keeping with a diagnosis of sarcopenia. 1
The Hologic Discovery QDR system (S/N 87664; software version 13.4.2:7; Hologic, Marlborough, MA) was employed to assess muscle quantity. DXA-derived appendicular skeletal muscle mass (ASM) was used as a surrogate measure of muscle mass and as a diagnostic criterion. ASM was determined as the sum of the lean mass (LM) in both the upper and lower limbs. As little as 50 g of metal may spuriously elevate soft tissue mass measured by DXA. 17 To avoid overestimating LM in the fractured hip due to the metal implants, a published protocol by Di Monaco et al. was employed. 18 The doubled LM of the non-fractured lower limb was substituted for the fractured side (ASM = 2 × [LM in non-fractured lower limb] + LM in both upper limbs). Reduced muscle quantity was confirmed in the presence of an ASM of <20 kg in men and <15 kg in women. To account for differences in body size, the skeletal muscle mass index (SMI), expressed as ASM/height, 2 was calculated and reported. An SMI of <5.5 kg/m2 for women and <7 kg/m2 for men was regarded as indicative of low muscle quantity corrected for body size. 1
Patient Data
A standardized interviewer questionnaire and in-patient hospital records were used to obtain patient information on age, sex, self-reported ethnicity, the total length of in-hospital stay, and fracture type. Lifestyle questions addressed current cigarette smoking, total pack years in smokers, daily alcohol intake (< or ≥3 units per day), and degree of mobility (inactive being ambulant indoors only and active being ambulant outdoors) prior to hospitalization. Anthropometry included measurement of mass and height with a calculated body mass index (BMI). All subjects were weighed on the same balanced beam scale. Height was measured with a Harpenden stadiometer (Holtain, Crosswell, UK) with a sliding headpiece to increase the accuracy of the reading. BMI was calculated as mass divided by height squared in kg/m2.
Biochemistry
Laboratory analyses were performed on-site by the Tygerberg Hospital National Health Laboratory Service, a South African National Accreditation System-accredited medical laboratory service. Biochemistry performed included serum creatinine, total calcium, albumin, phosphate, magnesium, hemoglobin, and 25-hydroxyvitamin D (25[OH]D) levels. A Cobas® analyzer (Roche, Basel, Switzerland) was used for the measurement of both serum total calcium (spectrophotometric detection) and 25(OH)D (electrochemiluminescence binding assay). Laboratory reference ranges were as follows: normal total calcium 2.15–2.50 mmol/L, and 25(OH)D levels, expressed in nmol/L, were defined as deficient (<50 nmol/L), insufficient (52.5–72.5 nmol/L), or normal (>75 nmol/L). 19
Statistical Analyses
Data were analyzed using Statistica version 13 (TIBCO Software Inc, Palo Alto, CA), and continuous data were expressed as means ± standard deviation or median (interquartile range, IQR), depending on the distribution. Categorical data were expressed as counts and frequencies. Differences between groups were detected by means of independent t-tests or Mann-Whitney U tests for continuous data, whilst a Chi-square test or Fisher’s exact two-tailed test was used to detect differences between groups for categorical data. An analysis of variance (ANOVA) was performed to detect differences between age groups for sarcopenia-specific criteria, with a Tukey’s post-hoc test to determine the location of differences, when present. p-values <0.05 were considered significant. The prevalence of sarcopenia was calculated by determining the number of patients with sarcopenia in the entire cohort that presented over the study period.
Results
Of the 100 patients who underwent hip surgery for FFH at Tygerberg Hospital during the 4-month study period, 65 patients were included in the study (Figure 2).

Flow chart of the study FFH: fragility fracture of the hip; DXA: dual-energy X-ray absorptiometry; 25(OH)D: 25-hydroxyvitamin D.
Sarcopenia Assessment in the Total Cohort
Thirty-four patients in our study cohort (52%) had sarcopenia. Sarcopenia criteria in the total cohort and in the cohort with and without sarcopenia are depicted in Table 1. A low HGS was present in 34/65 (52%) patients. Reduced muscle quantity, as evidenced by low ASM, was present in 55/65 (85%) of the study cohort. A diagnosis of sarcopenia was confirmed in 34/65 (52%) patients with low HGS and low muscle quantity. All 34 patients with low HGS had low muscle quantity, and low HGS thus identified patients with sarcopenia with 100% sensitivity and 100% specificity. Low muscle quantity was documented in an additional 21 patients with normal HGS, representing 68% of the cohort without sarcopenia. In the total cohort, only 10 patients had both normal HGS and muscle quantity (15%).
Sarcopenia Criteria in the Total Cohort and in the Cohorts With and Without Sarcopenia.

HGS: handgrip strength; CI: confidence interval; DXA: dual-energy X-ray absorptiometry; ASM, appendicular skeletal muscle mass; SMI, skeletal muscle mass index.
* Low handgrip strength refers to a handgrip strength <16 kg in women <27 kg in men.
** Low ASM refers to an ASM of <15 kg in women and <20 kg in men.
*** Low SMI refers to <5.5 kg/m2 for women and <7 kg/m2 for men.
Sarcopenia diagnosis required both low handgrip strength and low ASM.
Clinical Characteristics and Biochemistry of the Total Cohort
The clinical characteristics, hospital stay, fracture type, and 25(OH)D status of the total study cohort and the cohorts with and without sarcopenia are shown in Table 2. The study population was predominantly female (39/65 [60%]) and had a mean age of 74 ± 10 years (95% confidence interval: 72.1-76.9). Patients in the sarcopenic group (78 ± 10 years) were significantly older (p = 0.002) than those in the non-sarcopenic group (71 ± 8 years); 32% of the cohort was ≥80 years of age. The prevalence of sarcopenia in this age category was more than twice (18/21 [83%]) that in the younger age groups (16/44 [36%]). Table 2 shows that of the 34 patients with sarcopenia, 24 (71%) were women, and 10 (29%) were men; sarcopenia was documented in 24/39 (62%) women and 10/26 (38%) men. Thirty-one patients in the total study cohort (48%) did not fulfill the sex-specific criteria for the diagnosis of sarcopenia, of which 15 were women, and 16 were men. Figure 3 shows the age- and sex-specific HGS, ASM, and SMI. HGS declined significantly with age in women, with the most pronounced decline noted earlier in women (<70 compared to >80 years, post hoc p = 0.015) (Figure 3A). In both sexes, the mean ASM was low in all age categories (Figure 3B), while in SMI, a significant reduction was observed in females in the 70–79-year and >80-year categories (post-hoc p = 0.045) (Figure 3C).
Characteristics in the Total Cohort and in the Cohorts With and Without Sarcopenia.

Data are expressed as n (%), mean* ± SD, or median** (interquartile range).
BMI: body mass index; NOF: neck of femur fracture; IT: intertrochanteric fracture; 25(OH)D: 25-hydroxy-vitamin D.
Length of hospital stay refers to the number of days spent in hospital following surgery.
Activity and smoking were evaluated in 59 patients, 31 with sarcopenia and 28 without sarcopenia; 25(OH)D levels were tested in 61 patients, 31 with sarcopenia, and 30 without sarcopenia.
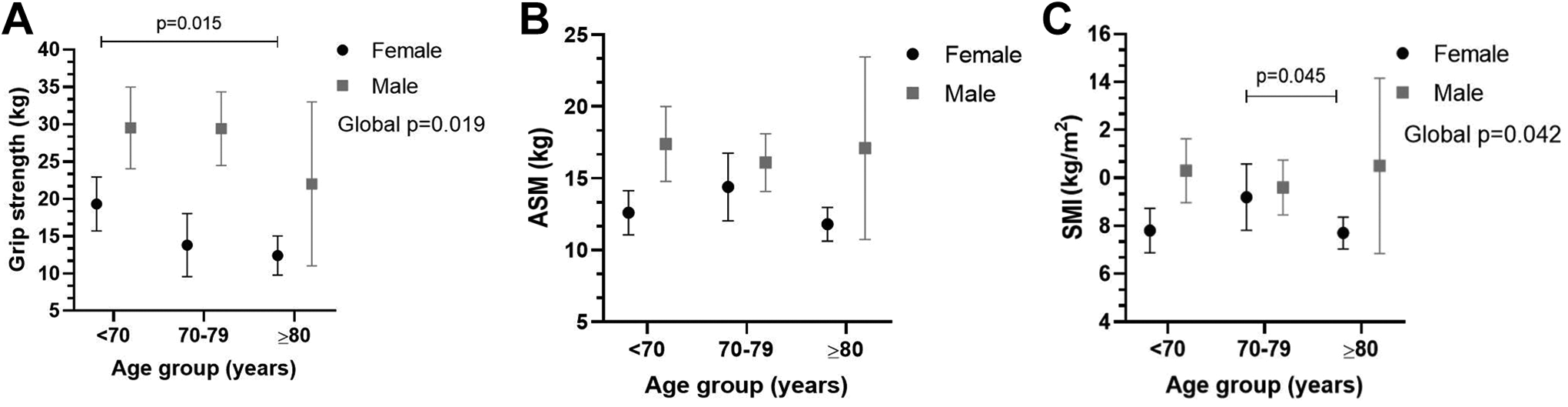
(A) Handgrip strength, HGS (kg), (B) appendicular skeletal muscle mass, ASM (kg), and (C) skeletal muscle mass index, SMI (kg/m2) between female (black circle) and male (gray square) patients for <70, 70–79, and >80 year age categories.
The median duration of hospital stay was similar in the groups with and without sarcopenia (6 vs. 5 days, respectively; p = 0.168). Most patients in this cohort presented with an intracapsular fracture (65%). Patients with extracapsular hip fractures appeared more likely to be sarcopenic; however, the likelihood did not reach statistical significance (p = 0.068; extracapsular: 16/23 [70%] intracapsular: 18/42 [43%]).
Patients with sarcopenia were less active than those without sarcopenia (p = 0.046). Only a minority of the total cohort admitted to excessive alcohol intake (≥3 units daily), and only 30/65 (46%) ever smoked. While excessive alcohol intake was not more prevalent in the sarcopenic group, the non-sarcopenic group included more active smokers (p = 0.009).
Significantly smaller body size, represented by lower body mass (p < 0.001), shorter height (p < 0.001), and a lower BMI (p = 0.018), was present in women with sarcopenia compared to those without sarcopenia. A similar trend was also observed in men; however, the differences in body size parameters between men with and without sarcopenia did not reach statistical significance.
The median 25(OH)D levels were significantly lower in the patients with sarcopenia (27 nmol/L [IQR: 20–39]) than those without sarcopenia (40 nmol/L [IQR: 29–53]). Deficient 25(OH)D status was documented in 28 of the 31 patients (90%) with sarcopenia in whom a result was available and in 21/30 (70%) patients without sarcopenia. Normal 25(OH)D levels were recorded in only 4 patients (7%), all without sarcopenia.
Serum calcium (p = 0.04), serum phosphate (p < 0.001), and albumin levels (p = 0.05) as well as the hemoglobin value (<0.001) were significantly lower in the cohort with sarcopenia. These results are not tabulated.
Discussion
Sarcopenia is common in older people. Geriatric patients with FFH are especially prone to sarcopenia, with potential adversity in terms of functional outcome and quality of life following hip surgery. 20 This study showed that sarcopenia following surgery in older South Africans with FFH is common, with a prevalence of 52% based on EWGSOP2 criteria, while different prevalence figures for women and men were documented (62% and 38%, respectively). A low HGS identified all cases with sarcopenia obviating the need for more expensive modalities such as DXA to confirm the diagnosis in our cohort. Several risk factors, including advanced age (≥80 years); female sex; a smaller body size, especially in women; limited physical activity; and low median 25(OH)D levels, were identified as significant predictors of the risk for sarcopenia.
Previously published study data on the prevalence of sarcopenia in FFH patients are summarized in Table 3. The prevalence of sarcopenia obtained in European and Asian population groups following FFH 18,20 -29 varies considerably, with prevalence rates ranging between 14.6% and 67.7% in women and between 12.4% and 95% in men. This variation may be explained in part by inherent differences in muscle strength and muscle quantity among people of different ethnicities. Different methodologies and diagnostic cutoffs (normative data) employed by both European and Asian researchers also contribute to this finding. Most of the observed variation is noted among European studies per se, with a more consistent prevalence reported for both sexes in Asian studies. The Asian Working Group on Sarcopenia’s (AWGS) diagnostic cutoff points for sarcopenia have been consistently used in Asian studies since 2014. The AWGS requires both a low HGS and a low muscle quantity based on DXA-measured ASM corrected to size (SMI) to diagnose sarcopenia. The revised EWGSOP2 introduced in 2019 provides a simple set of diagnostic criteria and specific diagnostic cutoff points for HGS, muscle quantity, and physical performance. Similar to the AWGS, this revised diagnostic set also requires both HGS and muscle quantity to be low in order to diagnose sarcopenia. Specific cutoff values for HGS, however, differ between the AWGS and the revised EWGSOP2 criteria. Furthermore, EWGSOP2 allows for either ASM or SMI to be utilized as a diagnostic index and does not specifically prescribe correction for body size as does the AWGS. This makes the comparison between work performed in Asian populations and populations elsewhere in the world difficult. A universal set of diagnostic criteria is vital to ensure uniformity in research outputs and will allow comparison of findings among studies and different population groups.
Available and Published Study Data on the Prevalence of Sarcopenia in Patients With FFH.

FFH: fragility fracture of the hip; DXA: dual-energy X-ray absorptiometry; AWGS, Asian Working Group for Sarcopenia; EWGSOP, European Working Group on Sarcopenia in Older People; FNIH, Foundation for National Institutes of Health. Prevalence figures for European studies indicated in normal text, Asian studies noted in italic font.
We defined sarcopenia in the presence of both low HGS and low muscle mass based on the EWGSOP2 diagnostic cutoff criteria. DXA-derived ASM was used to categorize patients as having either normal or low muscle quantity and was also expressed as SMI; however, the latter was not used to diagnose sarcopenia. In comparison, HGS measurements are easy and inexpensive. In our study, all patients diagnosed with sarcopenia were accurately and correctly identified with HGS per se (100% sensitivity and 100% specificity). Considering ASM only, 20/31 (65%) of the patients without sarcopenia had low muscle quantity but did not have impaired HGS (specificity 32%). Patients with sarcopenia in our cohort, similar to findings by others, 20 had a smaller body size based on mass, height, and BMI, with significance reached only in women. Correction of ASM for body size by expressing muscle quantity as SMI in our study cohort resulted in a decrease in the prevalence of sarcopenia in the total cohort to 43%. The specificity to correctly identify sarcopenia when using SMI was 35%, which was only slightly better than for ASM. Of the 6 patients defined as not having sarcopenia using SMI, not surprisingly, 5 were female, and 1 was male, thus, reducing the prevalence of sarcopenia in women to 49% and in men to 35%. Not correcting for body size in our patient population may thus result in the overestimation of the true prevalence of sarcopenia, especially among our female patients. Utilizing SMI as the only muscle quantity index should be considered in the future.
In most published work, a higher prevalence of sarcopenia was noted among men. The higher prevalence of sarcopenia in men is attributed to older age at presentation with FFH and poorer general health with more associated comorbidities at the time of presentation. 22 In the most recent study of sarcopenia and FFH from Taiwan, sarcopenia was again more prevalent among men. 20 This contrasts with our findings, where women were noted to be at increased risk of sarcopenia (62% vs. 38%). In addition, age was identified as a significant predictor of sarcopenia in our cohort (p = 0.002), and our female FFH patients were significantly older than the men (77 ± 10 vs. 70 ± 9 years; p < 0.003), a finding that may have contributed to the higher prevalence of sarcopenia among women. Furthermore, intrinsic factors such as a lower LM and strength ad initium, which worsens after menopause 30 in women compared to men, would also argue for a higher prevalence among women, as seen by us in this study. However, the association between sex and sarcopenia has not been fully elucidated.
The 25(OH)D level was low in most of our cohort with FFH, irrespective of the presence of sarcopenia. However, median 25(OH)D levels were significantly lower in the sarcopenia cohort (p = 0.006), with deficient 25(OH)D levels documented in 28/31 (90%) patients with sarcopenia in whom the test was available. Hypovitaminosis D is common in older people and is even more common in those with skeletal fragility. Low 25(OH)D levels were documented, except for 4 patients in the non-sarcopenic cohort, in all of our study patients and deficiency noted in 90% of the patients with sarcopenia. 25(OH)D is the main hormone of bone metabolism with a deficiency associated with decreased bone mass, impaired mineralization, and increased risk for skeletal fragility and fractures. Vitamin D receptors are expressed in many other tissues and are implicated in a variety of biological effects and molecular pathways, including skeletal muscle function and performance. The association between sarcopenia and hypovitaminosis D has been noted in a previously published study 31 and confirmed in our cohort. The potential physiological mechanisms for this association have not been fully elucidated; however, the loss of the positive impact of adequate 25(OH)D on myocyte proliferation and function 32,33 and chronic inflammation due to loss of its anti-inflammatory effect 34 have been implicated in the reduction of muscle strength and function. Hypovitaminosis D and the associated increased risk of falls were previously thought to be only due to skeletal fragility. 35 However, current understanding has highlighted the direct effect of 25(OH)D on muscle function and mass to explain this association. 36,37
Sarcopenia is a predictor of poor outcomes, for example, higher in-hospital mortality rates, increased postoperative complications, decreased survival, and although not consistently shown, also an increase in the length of hospital stay. 38 -41 A recent study by a Boston group noted that length of stay was independently correlated with sarcopenia in a group of 91 patients hospitalized following FFH specifically. 39 However, we were unable to confirm this finding in our sarcopenic cohort (p = 0.168).
In our study, patients with extracapsular hip fractures were more likely to be sarcopenic (16/23; 70%) than those with intracapsular fractures (18/42; 43%). Conversely, Di Monaco et al. reported a lower prevalence of sarcopenia in patients with extracapsular versus intracapsular hip fractures (50% vs. 64%). 25 Patients who sustain intracapsular hip fractures tend to be more mobile than those sustaining extracapsular fractures, 42 which alludes to better physical performance. Further studies are needed to better define the impact of fracture type on the risk of sarcopenia in older people.
This study has some limitations. Only 65 patients were enrolled in this study, and they may not be representative of the overall geriatric FFH population in South Africa. Moreover, this was a cross-sectional, descriptive study of the prevalence and did not include assessment of longer-term outcomes in those with and without sarcopenia.
The strengths of the study include the fact that a repeatable definition of sarcopenia was used with a limited chance of observer bias. Furthermore, an experienced DXA technician evaluated all the study subjects, thereby ensuring excellent performance and low intra-operator variability (coefficient of variation <1%) of the reported DXA measurements. The fact that 100 patients presented to our facility in a limited time of 4 months bears testimony to the high prevalence and importance of FFH and associated sarcopenia in older people. We obtained a 65% response rate in this study. The 35 patients who did not participate most likely represented a group of patients at increased risk of associated sarcopenia, and if included, may have resulted in an even higher prevalence of sarcopenia in our cohort.
Conclusions
This study is the first to report on the prevalence of sarcopenia and associated risk factors in older South Africans after hip surgery for FFH. We demonstrated that sarcopenia in geriatric patients with FFH after hip surgery is common, with a prevalence of 52%. HGS, an easy and inexpensive measurement, was identified as a highly sensitive and specific tool to confirm the diagnosis in our cohort. Advanced age (≥80 years); female sex; a smaller body size, especially in women; limited physical activity; and low 25(OH)D levels were identified as significant predictors of the risk for sarcopenia.
The loss of lean muscle is associated with impaired perioperative outcomes. In a trauma population, sarcopenia is an insidious disease that needs to be actively excluded. Further research is needed to determine the medium- to long-term outcomes of orthopaedic trauma patients with sarcopenia. Moreover, as our patient population ages, at risk patients should be identified within all other orthopaedic subspecialties.
Footnotes
Author Contributions
CLV Laubscher: protocol writing, data collection and analysis, and writing the dissertation. MC Burger: research supervision, editing protocol, data analysis, and manuscript editing. MM Conradie: data collection and analysis and manuscript editing. M Conradie: clinical supervision, editing protocol, writing dissertation, and manuscript editing. JD Jordaan: clinical supervision, study/concept development, editing protocol, and manuscript editing. M Conradie, MB, ChB, PhD and JD Jordaan, MB, ChB, H Dip Orth (SA), FC Orth (SA), These authors contributed equally to the manuscript
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.