
Abstract
The use of fluoroscopy is widespread within different medical specialties. Improper protection may cause significant radiation hazard to medical personnel. To evaluate the concepts on radiation safety and fluoroscopy use among orthopaedic surgeons and to reflect our current training on this issue, a survey was distributed to perform an audit in our department, an academic unit. Twenty-eight orthopaedic surgeons replied. Amongst our participants, 96.4% used a lead apron at all times. Only 33% used a thyroid shield, 67% never used radiation goggles and 96% never used radiation protection gloves. 53.6% and 46.4% of participants position the fluoroscopy incorrectly in the anteroposterior and lateral positions, respectively, during use. There is clearly a need for improved safety amongst orthopaedic surgeons. A literature review was further performed, showing the hazards of fluoroscopy for doctors, including the risk of cataracts, radiation dermatitis, skin cancer and thyroid cancer. Hazards specific to females, including breast cancer risk, and in-utero irradiation of foetus were also thoroughly discussed. Recommendations towards radiation safety and practical measures to reduce fluoroscopy radiation hazard during procedure were made. Education and training to doctors on this invisible hazard is strongly advised.
Introduction
In 1895, Professor Wilhelm Roentgen, a German physicist, discovered the X-ray radiograph. For his significant contribution, Roentgen was awarded the first Nobel Prize of Physics. Since then, X-ray application has become widespread and liberal 1 for medical purposes. However, this widespread use also caused hazards to emerge. In fact, in 1896, Thomas Edison invented the ‘Edison Vitascope’ as a home fluoroscopy, and his assistant Clarence Dally, had his hands frequently radiographed. Dally gradually developed pain, ulcers and squamous cell carcinoma on his hands which finally required bilateral arm amputation. 1 However, the first formal regulation for X-ray safety did not occur until 1934. 1
The International System of Units (SI) for radiation is in gray (Gy), which is defined as 1 joule (J) of energy absorbed by 1 kilogram (kg) of matter. When applying to the harmful effects of radiation, the dose is measured in Sievert (Sv), named after the Swedish physicist Rolf Maximillian Sievert. 2 One Sievert is equal to 1 Gray multiplied by a quality factor, and the higher the value, the more harmful the radiation. For example, the quality factor for gamma ray and X-ray is 1, whilst for alpha radiation is 20. 1 Sv of radiation is equivalent to 1 Gy of X-ray or 0.05 Gy of alpha radiation. 2 Besides medical use, radiation also arises from various sources, including rocks, earth and cosmic radiation. Most of the world's population is exposed to <1 to 10 mSv background radiation per year. 2 Cosmic radiation doubles for every 1500 m increase in altitude.2,3 For example, an airflight from Paris, France to Tokyo, Japan would bring 76 microSv (mSV) of radiation to the passenger. 4 The International Commission on Radiation Protection (ICRP) recommends the radiation dose limit for the general population to be 1 mSv above background radiation. For medical professions, including orthopaedic surgeons, radiologists, cardiologists, urologists and so on, the limit is 20 mSv per year (averaged over 5 years), with a single year not exceeding 50 mSv. 2
Importance of radiation safety among physician cannot be overstated. Mastrangelo et al. studied at an Italian hospital where radiation protection was poor. During the period of 1976−2000, the cancer incidence in orthopaedic surgeons were exceptionally high, reaching up to 29%. In fact, the incidence was also 6% in other exposed medical personnel. Cumulative radiation dose from the dosimeter was 35.2 and 7.5 mSv for the orthopaedic surgeons and exposed medical personnel, respectively, although the use of dosimeters was irregular and inconsistent. Further analysis also showed that orthopaedic surgeons were a significant risk factor, with odds ratio at 5.37. 5
More importantly, fluoroscopy is widely used in many medical specialties for various procedures. It allows physicians to make dynamic assessment and receive real-time feedback for intervention procedures. It reduces the need of open surgery and enables minimal-invasive procedures. 6 − 8 However, this also creates an important occupational hazard to medical personnel due to the ionizing radiation. Therefore, education on radiation safety is of paramount importance, to have proper protection and minimizing its hazards. In the professional training curriculum for specialist doctors in Hong Kong, dedicated radiation hazard education is not widespread. We performed a survey to review the awareness and medical practice related to radiation safety for orthopaedic surgeons in our department. We also performed an updated literature review on the occupational hazard of X-ray ionizing radiation to medical personnel to suggest strategies to reduce the risk.
Radiation safety audit among orthopaedic surgeons
We evaluate the concepts on radiation safety and fluoroscopy use among orthopaedic surgeons. We adopted the survey by Fidan et al., 9 where the authors had performed an online survey on Turkish orthopaedic surgeons regarding training, radiation and fluoroscopy usage behaviours, and the use of protective equipment. About 277 replies were received in their study, and it reflected inadequate training for fluoroscopy, low use of radioprotective goggles and dosimeters. The result had no difference among junior, senior and professors, 9 suggesting a continuous training deficit in radiation safety field. By conducting this audit we also aimed to assess the awareness of radiation safety, current training/knowledge and practice at our unit.
Forty-two electronic survey forms were distributed online to orthopaedic surgeons in our centre, which is a regional tertiary referral centre. The audit included the experience (trainees, specialists, associate consultant or consultant), gender, protective equipment use (lead apron, thyroid shield, radio-protective goggles, radio-protective gloves), dosimeter use, whether the surgeon knew the dosimeter results, knowledge of C-arm fluoroscopy positioning, and whether they were worried about radiation hazard based on their current knowledge/practice. The correlation between level of experience and use of protective equipment, and fluoroscopy tube position in anteroposterior (AP) and lateral position, is compared with Chi-square test. A p < 0.05 was considered as statistically significant. Please refer to Table 1.
The audit survey distributed to orthopaedic surgeons.
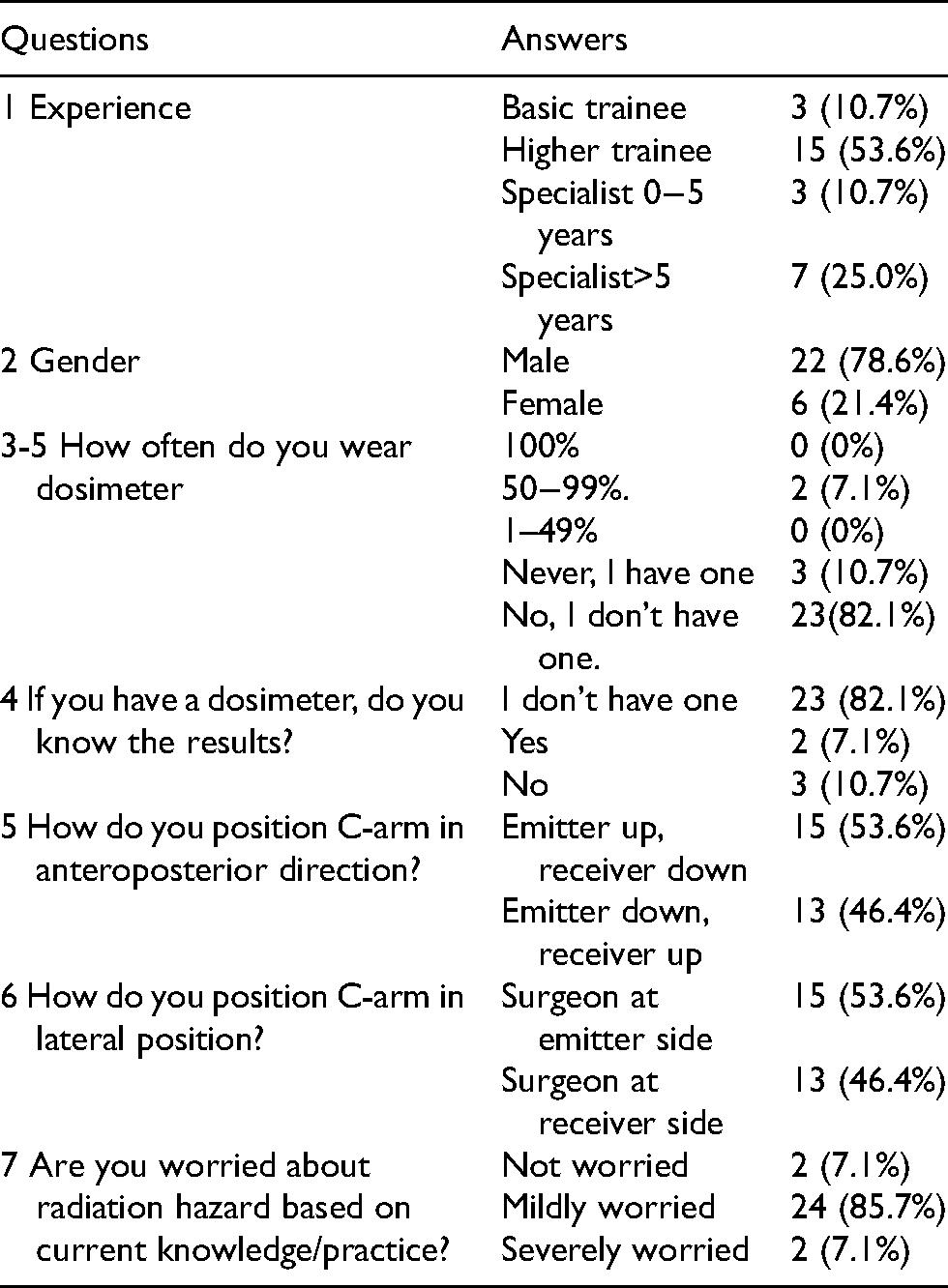
Twenty-eight replies (28 out of 42, 66.7%) were received. The results are listed in Table 2 and Figure 1(A) to (D). Among the results, 100% participants replied they always used a trunk lead apron. For thyroid shield, 33% (n = 9) used it all the time, 48% (n = 13) used it 50–99% of time, 11% (n = 3) used it 1−49% of time, and 8% (n = 2) never used one. For radiation protection goggles, no Surgeon used it all the time, 7% (n = 2) used it 50−99% of time, 26% (n = 7) used 1–49% of time and 67% (n = 18) never used one. For radiation protection gloves, only 4% (n = 1) used it 1−49% of time, while all other surgeons never used one. There was no statistically significant correlation between experience and use of protective equipment (Table 3), except for 1 specialist with 0−5 years of experience that did not 100% of the time use a trunk lead apron and this difference led to statistical significance in Question 3 (p = 0.03). Among five participants who had dosimeters, four were senior specialists for more than 5 years, and 1 was a higher orthopaedic trainee. The remaining surgeons did not have a dosimeter. There is correlation between experience (higher orthopaedic trainee vs. senior specialist) and possession of dosimeter (p = 0.008).
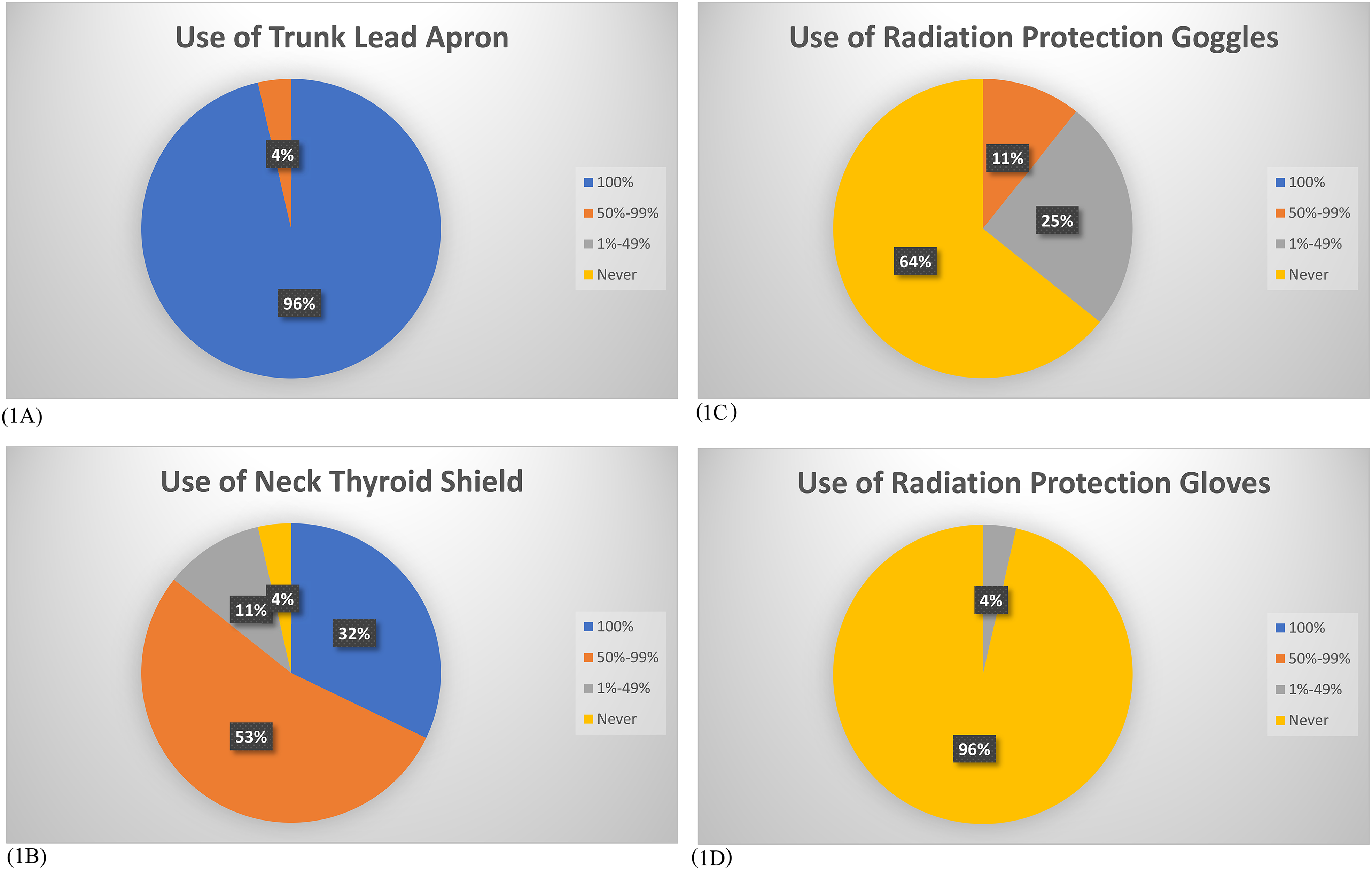
(A) to (D) showed reply on use of (A) trunk lead apron, (B) neck thyroid shield, (C) radiation protection goggles and (D) radiation protection gloves.
Results of the audit survey are summarized. Answers from 3-1, 3-2, 3-3, 3-4 are presented in Figure 1(A) to (D).
Comparison of surgeons’ experience with audit response.
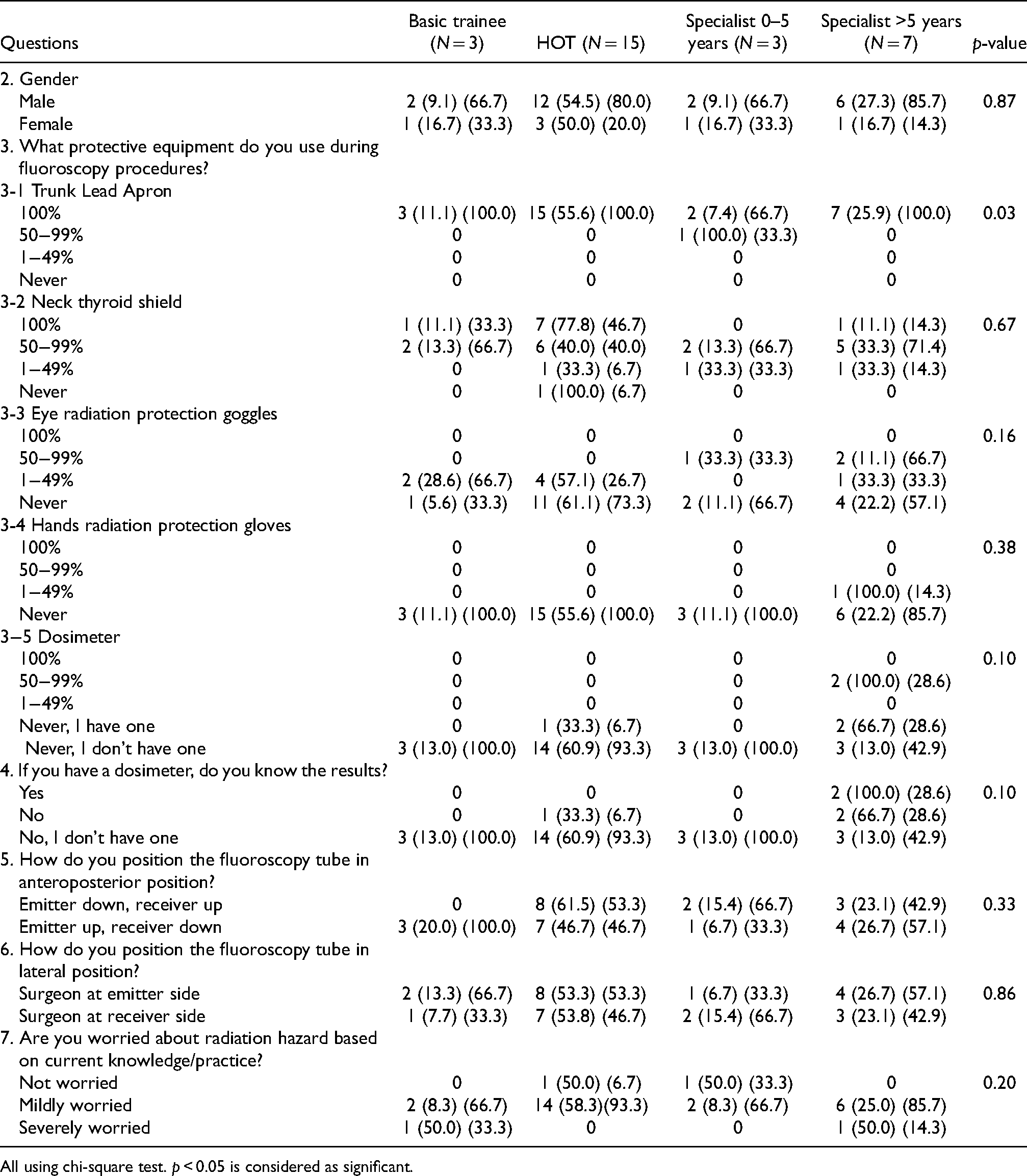
All using chi-square test. p < 0.05 is considered as significant.
Our results demonstrated a pattern similar to other articles,9,10 with a high usage rate of trunk lead aprons, high to moderate use of thyroid shield, but low use of radiation goggles, and minimal use of radiation protection gloves. Hafez et al. reported possible causes for not using protective equipment were due to heavy lead aprons, tight neck thyroid shield, and rigid lead gloves that hinder operative procedures. 11 The medical community should promote more complete and frequent the use of protective equipment, and manufacturers could consider producing lighter and more comfortable lead aprons and thyroid shield that still ensure protection. Radiation protective gloves should also be more agile.
Similar to our results, other have shown that dosimeter possession and use were limited, 9 and some participants do not know the results.9,10 Amongst our participants, few had possession of dosimeters, especially among junior staff. In Hong Kong, the Department of Health is responsible for monitoring radiation dose and managing dosimeters. Enhancing feedback to orthopaedic surgeons about radiation dose is recommended.
53.6% and 46.4% of participants do not position fluoroscopy tube correctly for radiation exposure minimization in AP and lateral position, respectively. This high rate of inaccurate positioning is a worrying result. The correct position, which minimize the surgeons’ radiation exposure, is emitter down, receiver up 1 (Figure 2(A)); and the doctor standing at the receiver side 1 (Figure 3(A)). No correlation between level of experience and correct positioning of the fluoroscopy is demonstrated. This may reflect inadequate training regarding fluoroscopy tube positioning, or a false sense of security about radiation exposure under the lead apron and thyroid shield, with inadequate knowledge of radiation risk on eyes and skin.
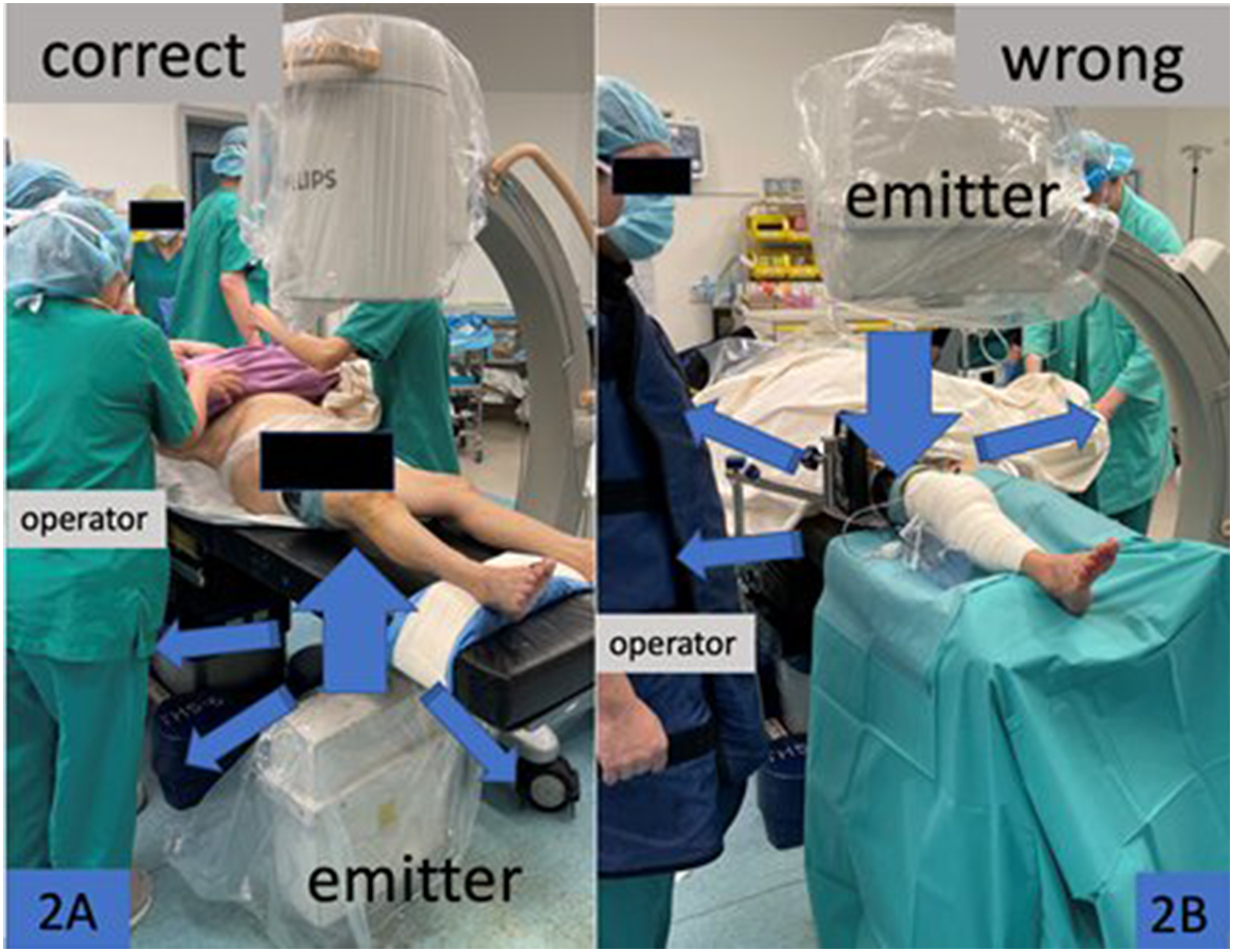
(A) and (B) The main radiation beam (large arrow) and direction of scattered radiation (small arrows). In (A) (emitter down, receiver up), the scattered radiation is mainly distributed to the floor and the lower trunk of operator, which is protected by lead apron. In (B) (emitter up, receiver down), the scattered radiation will affect the hands, eyes, thyroid and other staffs in the theatre.
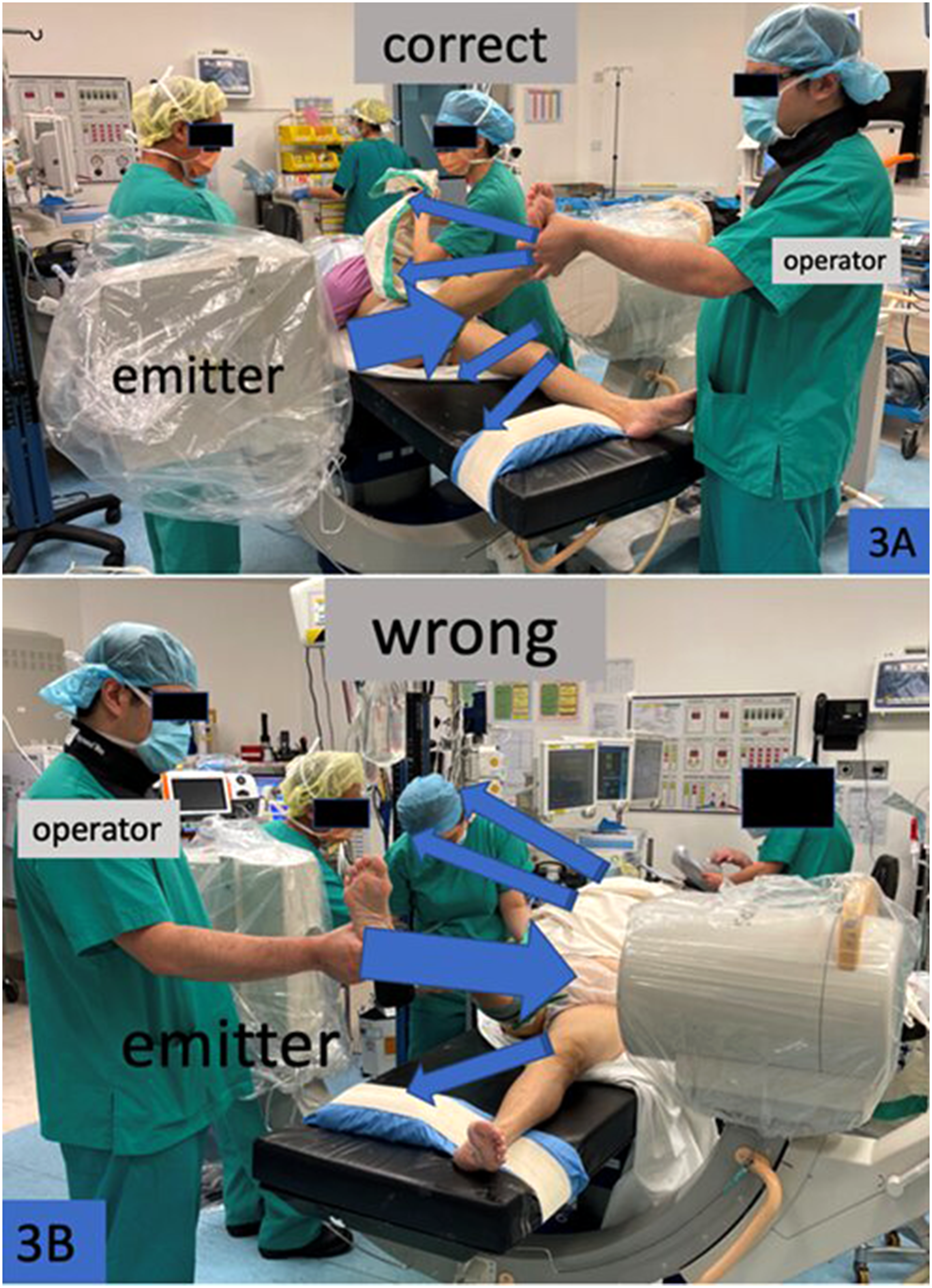
(A) and (B) The main radiation beam (large arrow) and direction of scattered radiation (small arrows). In (A) (surgeon at receiver side), the scattered radiation is directed away from the operator. In (B) (surgeon at emitter side), the scattered radiation is directed towards the operator.
This world-wide occupational hazard regarding ionizing radiation is well-documented and training on fluoroscopy and radiation hazard should be enhanced. Knowledge on radiation hazard to different body parts should be disseminated. Use of protection equipment, including thyroid shield, radiation protection goggles and gloves should be promoted. Correct fluoroscopy positioning should be also taught. Dosimeter use should be wide-spread with feedback to surgeons. We review the literature to update the knowledge on radiation safety and its risks.
Literature review on X-ray radiation and its risks
Radiation dosage and procedures in different medical specialties
Fluoroscopy is widely used in many specialties. Cardiologists use fluoroscopy for percutaneous coronary procedures as a minimally invasive approach to diagnose and intervene cardiac pathologies. 12 Procedures include diagnostic catheterization of coronary systems, percutaneous coronary intervention (PCI) and cardiac resynchronization therapy pacemaker. 12 Amongst which PCI causes one of the highest radiation exposures, with double the radiation dose of a diagnostic catheterization. 12 For PCI, the median fluoroscopy time for PCI procedures is 12.7 min, and air-kerma radiation dose (mean ± 1 SD) is 927.6 ± 548.1 mSv. 12 Complex PCI, including multiple catheters, balloons, rotational atherectomy, bypass stents, needs longer time and higher radiation dose, 12 mean ± SD 1292.7 ± 515.8 mSv. 12
Multiple medical specialties also use fluoroscopy for a variety of procedures. Urologists use fluoroscopy for percutaneous nephrolithonomy (PCNL) or urteroscopy. Orthopaedic surgeons use fluoroscopy for multiple procedures including fracture fixation, vertebral stabilization procedures and vertebroplasty. Vascular surgeons use fluoroscopy for abdominal aorta aneurysm stenting, peripherally inserted central catheter. Neurosurgeons use fluoroscopy for head and neck endovascular procedures (HN), or ventriculo-peritoneal shunt use. 13 Fluoroscopy can also be used by hepatologists for Transjugular Intrahepatic Portosystemic Shunt (TIPS). 14 Hepatobiliary surgeons also use fluoroscopy for endoscopic retrograde cholangiopancreatography (ERCP). In fact, with the advance in medical technology, the usage of fluoroscopy is now more widespread with minimally invasive procedures.
Kim et al. 15 performed a review regarding radiation dose of different fluoroscopy use, including PCNL, vertebroplasty, extremity nailing, biliary procedures, TIPS, HN and ERCP. It was found that TIPS and HN had the longest fluoroscopy time, with median time of 60 min (35−100 min) and 59 min (32−78 min), respectively. TIPS harbour the highest effective dose of radiation, median 17 mSv (2.5−74). The radiation to the hand had a median of 935 microSV (447−1350), and at the trunk it had a median of 205 mSv (35−589). This is related to the prolonged fluoroscopy time. 15 The effective dosage of radiation in descending order was vertebroplasty (median 14.3 mSv, 0.1−101), extremity nailing (median 9.8 mSv, 2.5−88), PCNL (median 6.2 mSv, 1.7−56), HN (median 5.2 mSv, 1.8−53), biliary procedures (median 5 mSv, 2−46) and ERCP (median 1.1 mSv, 0.2−49). Effective dosage were calculated according to the widely used, standardized algorithm, Niklason 16 (two dosimeters) and Padovani 17 (one dosimeter) algorithm.
Vertebroplasty had the lowest fluoroscopic time (median 8 min, 2−35 min), however its effective dose was the second highest amongst all compared procedures. Vertebroplasty is a common procedure performed by orthopaedic surgeons, which involves the injection of bone cement, under X-ray guidance, into vertebral compression fractures due to osteoporosis, or tumour. 18 This is due to the frequency of the operator’s hand placed near the X-ray field. The operator is typically 40 cm from the field, and the operator's hand is 25−30 cm from the surgical site, or even within the X-ray field.
Risks to the medical personnel
Ophthalmological risk – cataracts
Cataract is the clouding of lens, which causes visual blurring symptoms and is classified according to location including nuclear, cortical, posterior or mixed. Specific to radiation exposure is the posterior lens cataract. 1 A previous study by Chodick et al. 19 found that there was no threshold to dosage and cataracts were associated with chronic low dose exposure. Another study involving 495 acute leukaemia patients receiving whole body irradiation showed that the rate of cataract had a dose-dependent relationship, but no threshold was identified. 20 Long-term, low-dose ionizing radiation can cause cataracts. A study involving 209 cardiological intervention personnel showed that there was a 3.2-fold increase in cataracts amongst interventional cardiologists. In fact, further studies showed a higher cataract incidence for interventional cardiologists and interventional cardiology nurses, with a risk ratio of 5.7 (95% CI 1.5−22) and 5.0 (95% CI 1.2−21), respectively. The mean ocular cumulative dose was 3.4 Gy and a strong dose-dependent effect was found. With increasing data showing risk of low dose, chronic radiation exposure, the ICRP has recommended eye exposure dosage from 150 mSv per year to 20 mSV per year, averaged over 5 years. 21 Therefore, the use of radiation-proof goggles is highly recommended. 22
Thyroid risk – cancer
Radiation is known to cause thyroid pathologies, including thyroid adenoma, radiation thyroiditis and thyroid cancer. 23 Thyroid cells have a fast metabolism and are susceptible to ionizing radiation effects. As of now, there is no known safe threshold. 1 Previous studies have shown that 65 mSv per procedure is associated with increased thyroid cancer risk. 24 This limit is frequently exceeded in multiple orthopaedic procedures. 24 Devalia et al. 24 reported the average thyroid exposure dose during femur intramedullary nail and dynamic hip screw procedure were 142 microSV and 55 microSV, respectively, when no thyroid shield is used. In fact, Muller reported a 70 times higher thyroid exposure if lead neck apron was not used. 25 However, if utilized, only 0.2% of annual dosage limit for the thyroid is reached. 25 The ICRP yearly upper limit of thyroid radiation remains at 500 mSV, 26 although some have suggested the permissible upper limit of thyroid radiation dosage should be as low as 150 11 or 300 mSV. 27
Elevated thyroid stimulating hormone were shown to be associated with cumulative radiation exposure. 28 Age is important in determining risk of thyroid radiation exposure. At a younger age, thyroid cancer risk is exponential in the relationship with radiation dose. 29 Therefore, thyroid shields should always be worn during fluoroscopy procedures. ICRP recommends neck collar use in orthopaedic surgeons younger than 30 and 40 years old in male and female, respectively. 30
Skin risk – dermatitis and cancer
For occupational exposure, ICRP recommends no more than 500 mSv per year of radiation dose to the skin or to the hand, and no more than 50 mSv per year for the public. 30 The risk to the skin for radiation dermatitis increases after a radiation dose threshold is passed. It presents with immediate erythema, acute inflammatory reaction with increased vascular permeability which last for hours to days. A second stage with more sustained erythema, likely mediated by cytokines, occurs after 10−14 days. 31 Below 2 Gy, no effect to the skin is expected. With a low dose of 2−5 Gy, transient epilation without permanent effect is expected. With a dose of 10 Gy, patient is expected to suffer from prolonged erythema, permanent epilation, dermal atrophy and induration. With a dose of 15 Gy and above, dermal atrophy, secondary skin ulceration, late skin breakdown and need of surgery is expected. 32
The risk of basal cell carcinoma and squamous cell carcinoma also increase with radiation. Radiation cause excess relative risk (ERR) of 0.52/Sv and absolute risk (AR) of 8·5 × 10 − 4 cases per person-year-Sv 33 for skin cancers. Therefore, proper protection of skin, especially the hands is recommended with radiation gloves.
Haematology risk – leukaemia
Radiation exposures harbour a risk for delayed presentation of haematological malignancy with a minimal latency of 2−5 years, and sometimes more than 20 years. 34 The risk of radiation induced solid organ tumour persists throughout the lifetime, 35 whilst haematological malignancy risk decreases with time. The rate of risk decrease occurs faster in children than in adults. 36 For example, if a patient was irradiated at 10 years old, it takes 5 years for leukaemia risk to decrease 5 cases per 10 4 Person-Year-Sv. For same extent of risk decrease, it takes 10 years for a patient irradiated at 25 years old. 36 Chronic myeloid leukaemia risk declines the fastest and approaches a very low level after 10 years. 36 Multiple studies also show the incidence of non-chronic lymphoid leukaemia risk among Japanese atomic bomb survivors and nuclear plants workers was excessive relative risk (ERR) 1.4−1.93 per Gy of exposure. 37 − 39 As leukaemia often originates from bone marrow 40 and red marrow mainly distributes in axial skeleton, this shows importance of using lead apron.
Breast risk – Cancer
Association between radiation and breast cancer is well established in literature. John et al. 41 studied 5685 patients and reported an association of breast cancer with previous radiotherapy (OR = 3.55, CI 1.47−8.54), diagnostic chest X-ray for tuberculosis (OR = 2.49, CI = 1.82−3.40) or pneumonia (OR = 2.19, CI 1.38−3.47). The maximum cumulative dose amongst these patients were 1 Gy. The risk is higher for women exposed at a younger age as well. 41 Preston et al. 42 reported radiation exposure in modern protection equipment to be associated with a marginal increased breast cancer risk, with ERR 0.07 at 100 mGy (95% CI −0.005–0.19). The risk was significantly higher for those born before 1930, with ERR at 100 mGy = 0.16, (95% CI 0.003−0.39), possibly related to radiation protection equipment and radiation safety.
A lead apron must be well fit to maximize its effect. Valone et al. studied the aetiologies of prevalent CA breast among female orthopaedic surgeon. An anthropomorphic torso phantom, simulating the female surgeon, was used. It was found that when the lead apron was too large or too loose, the upper outer quadrant of breasts will receive much higher radiation dosage compared to the lower outer quadrant (0.40 mrem/h vs. 0.06 mrem/h, p = 0.05). 43 C-arm cross-table lateral projections also cause higher breast radiation exposure than AP projection (0.98 mrem/h vs. 0.13 mrem/her, p < 0.001). Using cross-back aprons provide higher protection than vest shield configurations. 43
Pregnancy risk – harm to foetus
Ionizing radiation can cause harmful effects at cellular and molecular levels. Ionizing radiation also produces free radicals that disrupt important cellular functions. As a result, cellular enzymes disruption, DNA damage and cell death can occur. 44 Ionizing radiation can cause miscarriage, congenital malformation, growth retardation, stillbirth and cancer. Cancer risk is considered stochastic, that is, there is no threshold, and the risk increase proportionally with dose. In contrary, foetal malformation, growth retardation, mental retardation risk is considered deterministic, and risk increases after a radiation dose threshold is passed, in a linear manner. It is estimated that between 25 and 40% of radiation reaching the mother's abdomen and pelvis will penetrate the uterus and reach the foetus. 45
In the first 14 days post conception, the foetus is most sensitive to radiation, and it either withstands or succumb to the radiation, often termed an ‘all-or-none phenomenon’. 46 Early organogenesis is considered most critical for foetal malformation. Giles et al. 47 reported childhood cancer risk 2.5 times higher in the first trimester compared to the third trimester of gestation. The most critical period for mental retardation is 8th–15th week of gestation as the immature brain develops during this period. 48 The threshold for congenital malformation even at the most sensitive stage is reported at 0.1−0.2 Gy, and the threshold for growth retardation and miscarriage is higher, 48 suggested to be 0.5 Gy. 49 The known effective dose for CT abdomen/pelvis is typically 15 mSV, whilst CT of the thorax, brain, and extremities is even lower. Radiation effective dosage of CT lumbar and cervical spine is only 7 and 5 mSv, respectively. An AP pelvic X-ray only carries 0.48 mSv dosage. 34 These are all much lower than the threshold for malformation.
Miller et al. studied the effects of radiation on the survivors of Hiroshima and Nagasaki atomic bombs. He found that in the first trimester, a dose of 0.1−0.49 Gy led to 6% of mental retardation, and an average of 21−29 points intelligence quotient points. In the second trimester, a dose of 0.1−0.49 Gy causes a 2% incidence of mental retardation. The risk further decreases during the third trimester. Risk is negligible in radiation lower than 0.05 Gy. 48 Preston also studied the occurrence of solid organ tumour amongst Hiroshima and Nagasaki Atomic Bomb survivors at age of 12–55 years. A cohort of 2542 patients who were irradiated by the atomic bomb in utero were compared to a cohort of 15,388 patients who were irradiated by the atomic bomb at early childhood younger than 6 years of age. He found that the adult-onset of solid organ tumour risk was increased in both groups, but increased more in the early childhood group. At age 50, ERR was 1.7 per Sv, 95% CI 1.1 to 2.5SV for the early childhood group compared to the in-utero group at age 50 with ERR = 1.0 per Sv, 95% CI = 0.2 to 2.3 per SV. 35 This shows that the radiation effect is more prominent in the post-natal stage than in utero. To understand the scale of the above risk, one study showed ERR of small cell carcinoma of lung due to smoking was 20.7. 50
Animal experiments also show that a 0.01–0.02 Gy radiation in utero increases the risk of childhood cancer, particularly leukaemia, by a factor of 1.5 to 2. 51 A meta-analysis of 32 case-control studies in 2008 revealed paediatric leukaemia risk to increase by a RR of 1.32 (95% CI 1.19−1.46), related to diagnostic X-ray in utero. The ICRP recommends for a medical personnel with pregnancy, the radiation exposure limit should be the same as the general population (1 mSv per year), 2 and should minimise fluoroscopy exposure. Jones et al. 52 showed that for lumbar spine surgery, the placement of four vertebral pedicle screws on average results in 0.11 mGy per case to the Surgeon abdomen under lead apron. Assuming that a maximum of 40% radiation reaches the foetus, this represents a maximum dose of 0.044 mGy. 2 Therefore if there were 23 cases over a 9-month pregnancy period this would exceed the 1 mGy limit recommended by the ICRP, although this scale is far from teratogenicity or malignancy. 2
Female physicians should understand that radiation exposure dose is low if routine protection is performed, and that overall risk of teratogenicity or malignancy risk to the foetus may be low. Excessive worries may be unnecessary for most incidental fluoroscopy exposures under protection but caution is still strongly advised.
Genetics risk – instability
Although the general population appears to be safe from diagnostic fluoroscopy radiation, some populations are more susceptible. Patients with chromosome instability disorders, such as Nijmegen breakage syndrome (NBS, B-cell lymphoma) or ataxia-telangiectasia (AT, with leukaemia and lymphoma) were found to have an unusually increased leukaemia incidence after radiotherapy, with the lowest radiation dose found to be 3 Gy. 53 However, this susceptibility is unclear for fractional, chronic low dose radiation such as fluoroscopy procedures. 53 Other syndromes characterized with DNA repair disorder or instability including Fanconi anaemia, Gardner syndrome, hereditary malignant melanoma may also have increased susceptibility. 54
Strategies in reducing radiation risk for medical personnel
Ionizing radiation cannot be excluded from modern medical care. The ICRP proposed two key concepts: (1) Justification, which states that the use of radiation must be justified by its benefits to patient which will outweigh the radiation risk; and (2) Optimization, in which radiation should be minimized to as low as reasonably achievable (ALARA) while adequate to produce images suitable for medical use.
Protective wear
During fluoroscopy procedures, personal protective equipment (PPE) should be used. An appropriately sized neck collar can reduce radiation dose by a factor of at least 9. 55 Lead gloves can reduce radiation to the hand by 75%, 18 however concern about reducing surgeon's tactile sensation and ironically increasing operating time and radiation dose exists. Lead aprons can effectively block the radiation scattered below the patient in an AP beam, especially protecting the gonads. A 0.25 mm lead apron can reduce trunk radiation by 90%, whilst a 0.35 mm lead apron can reduce by 95%, and a 0.5 mm lead apron can reduce by 99%. 18 Ordinary eyeglass can reduce the radiation by 20%, whilst lead glass can reduce the radiation by 30−70%. 18
A thyroid shield can significantly reduce radiation exposures to the thyroid region 28 by a factor of9 55 to 70. 25 Furthermore, proper fitting is necessary. The superior 10 mm of neck that is frequently unprotected by loose neck collars receive higher proportion of radiation. 28 Fitting the thyroid shield tightly rather than loosely can reduce thyroid radiation by 23% further. 55 A bismuth thyroid masking reagent, a soft radiation-proof cover with customized shapes, can be added to a more loosely fit thyroid shield to provide similar protection as a tightly fitted thyroid shield 55 with better comfort. Example of use of radiation protective equipment in operation theatre is shown in Figure 4(A) and (B).
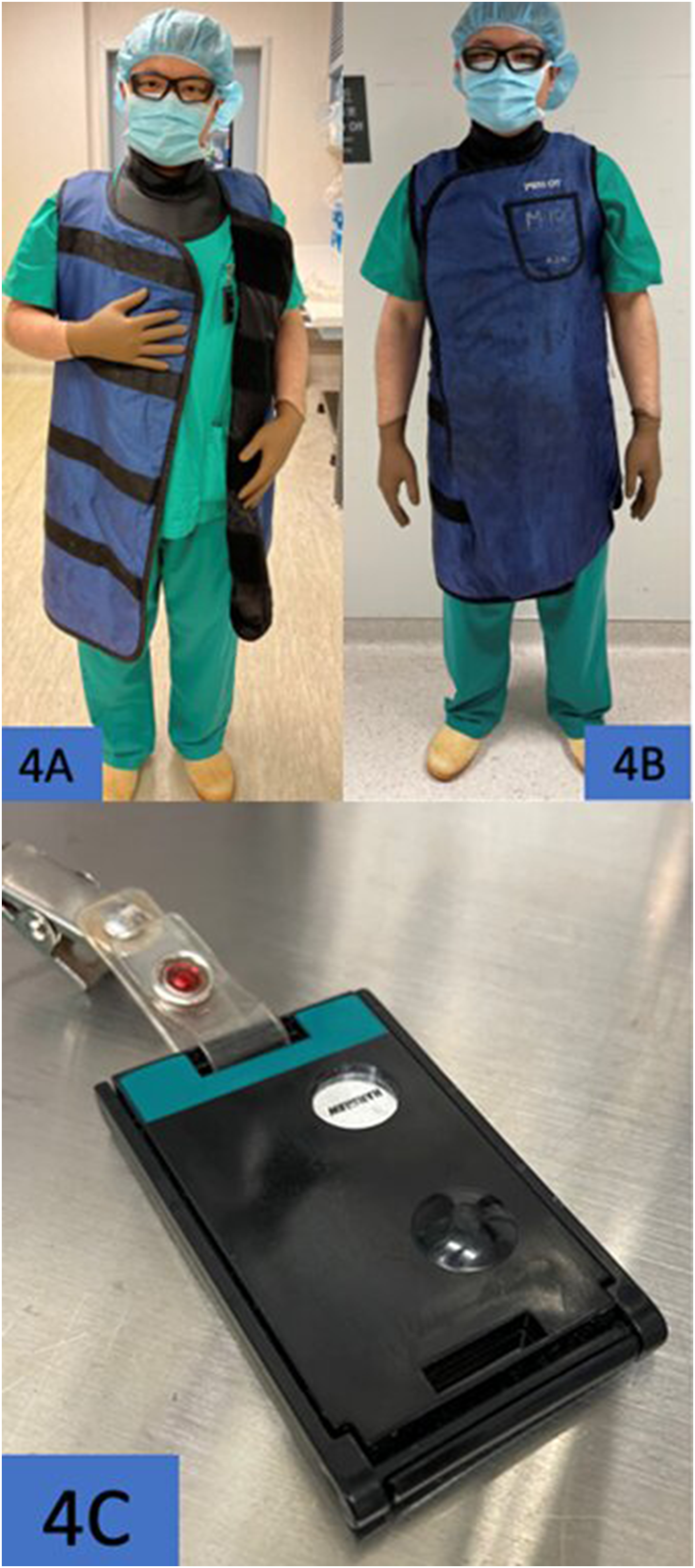
(A) The dosimeter is to be worn under the lead apron. (B) A full suit of protective equipment including a well fit neck collar, trunk apron, radiation protective glass and dosimeter (hidden under lead apron). (C) The side of dosimeter that should face outside.
X-ray positioning and modes
Design of fluoroscopy significantly affects the scattered radiation. With the use of a collimator, radiation is concentrated in a narrow and parallel beam towards the receiver, therefore minimizing reflection or scattering to the environment. However, scattering still unavoidably occurs when the X-ray beam passes through human tissue or when reflecting from the detector. If the C-arm is placed in the AP direction, the emitter should be placed inferiorly under the bed such that scattered radiation is limited to below the bed (Figure 2(A) and (B)). 1 Jones et al. found in a source-inferior position, at 25 cm from the patient the scattered radiation is reduced by a factor of 4.64. 52 When the C-arm is placed in a horizontal position (Figure 3(A) and (B)), the surgeon should stand opposite of the emitter (i.e. same side as the receiver) to minimize effects of scattering.1,56,57 Physicians should wear an apron as scattered radiation concentrates at the operator's lower trunk and gonadal region.56,57 Modern fluoroscopy systems help to reduce radiation dose by automatic adjustment of dosage (automatic brightness control; ABC) and there are functions to save the last image. 58 When ABC is being used, one should avoid putting radio-opaque objects inside the beam as this will cause an automatic increase in radiation dose. One study demonstrated that when radio-opaque objects including lateral operating table support, endoscopy cameras, light cords and flexible ureteroscopy is placed inside the field, the C-arm radiation dose increases by 35%. 58 The physicians and assistants should pay attention to clear clutters of instruments and objects on the operating table. Fluoroscopy settings also help reduce the radiation hazard. Reduction of pulse rate (i.e. frame rate) has a significant effect. A study on cardiac catheterization showed reducing fluoroscopy pulse rate from 10 frame/second (f/s) to 7.5 f/s can reduce radiation dose by 21%. 59 A study on carotid artery stenting showed that a reduction of pulse rate from 7.5 to 4 f/s reduced radiation dose by about 51%, with no increase in procedure complication. 60 Operators should find out the minimal pulse rate appropriate for the specific procedure and provide training to staff. Moreover, multiple static images should be used in place of continuous imaging (cine) whenever possible. Olcay et al. 61 showed by using the last fluoro hold mode instead of cine mode during cardiac coronary angiography, the radiation exposure, fluoroscopy time and contrast use is reduced by 79%, 57% and 21%, respectively. Zweers et al. 62 demonstrated that high tube potential and low tube current resulted in a significant dose reduction for the patient and staff.
Medical personnel position from patient
Physician can reduce radiation exposure by various efforts during the procedure. Radiation dose decreases with distance according to the inverse square law. Studies showed that a physician standing 1 m away from the patient and if the fluoroscopy X-ray beam is perpendicular to the physician, the physician receives only 0.1% of the patient’s radiation dose. 56 When the physician distance increase to 2 m, the radiation dose received by physician is only 0.025% that of the patient. 56 Physicians should minimize the use of fluoroscopy and should be used as short as possible. Unnecessary repeated exposure should be avoided. Furthermore, stationary rather than continuous image is encouraged. Physicians should not place any body parts including their hands inside the radiation beam directly, and should use long instruments to maximize the distance of their hand from the radiation field.
Dosimeters for monitoring
Personal dosimeters can be used to record the dosage received by medical personnel. It allows objective recording of the actual dose and allows adaptive action accordingly should the received dose approaches or even exceed the dose limit. To monitor doses to the skin, hands, feet, and the lenses of eyes, special dosimeters (e.g., a ring dosimeter for wrist) can be used on different procedures. 63 It should be worn inside the lead apron, rather than outside, to correctly record radiation dose received by the physician body (Figure 4(A)). The correct side facing outwards (Figure 4(C)) should be noted.
Medical education
Improvement of physician knowledge towards fluoroscopy and radiation is of utmost importance. In a survey of 323 orthopaedic surgeon, only 12% were formally trained on fluoroscopy use, and up to 33.3% replied they wear no protective equipment during fluoroscopic procedures, and only 10.6% used a dosimeter. 9 Furthermore, a systemic review in 2010 reviewed 14 studies on physician knowledge from Europe, North America, Turkey and Israel. It was found that there was only low to moderate knowledge among physicians on radiation hazard and health risks. 64 This shows that education is relatively low and proper education on radiation safety should be made to doctors in different specialties.
Radiation safety and regulations in Hong Kong
In Hong Kong, the Radiation Health Division, Department of Health enforces the Radiation Ordinance (Cap. 303). The Department of Health has also made useful radiation safety recommendations. For example, based on the Radiation Health Series,
65
the annual occupational dose limits is stipulated as:
Whole body: 20 mSv in any calendar year Abdomen of women with reproductive capacity: 5 mSv in any consecutive 3 months interval Abdomen of a pregnant woman: 1 mSv from declaration to delivery and intake radionuclides is limited to 1/20 ALI Lens of eye: 150 mSv Skin, average over 1 cm2: 500 mSv Other individual organs: 500 mSv
The employer should provide to their employees a suitable personnel radiation monitoring device approved by Radiation Board to monitor their radiation doses. Each dosimeter is normally worn for 1 month and should be returned for assessment and monitoring for radiation exposure and then replaced. Regular medical examinations on radiation workers should be performed. The recording of irradiation time in fluoroscopy is also useful in reminding the operators that the time should be kept to a minimum.
The Department of Health also recommends a radiation safety officer or supervisor to be appointed in each facility where work with radiation is undertaken. This person would be responsible to prepare written safety instructions, assist in management and safety, ensure compliance and appropriate actions. PPE use is also recommended. 65
Conclusion
Fluoroscopy has undeniable contribution to modern medicine but also brings radiation hazard to the physicians and other staffs in operating theatre. Risk of leukaemia, risk to eyes, thyroid, skin, breast and fetes cannot be underestimated. Physician should properly use protective equipment including lead aprons, thyroid shields, radiation protection goggles and gloves, and dosimeter, to protect one-self from the invisible radiation hazard. Improved techniques in using fluoroscopy can also help reducing radiation hazard. The medical field should observe principles of justification and optimization, to reduce the radiation hazard to ALARA.
The current conducted survey also shows the awareness of radiation safety can be improved. Proper understanding of radiation risk will encourage doctors to use proper protection gear, and to clear unnecessary worries. Formal training on radiation safety and safe fluoroscopy use should also be encouraged and adopted.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.