
Abstract
Background/purpose:
To determine whether sedentary behaviour and physical activity differ according to initial weight-bearing status 2 weeks and 6 months after lower limb (LL) fracture.
Methods:
Two weeks and 6 months following LL fracture, 47 adults aged 18–69 wore ActiGraph and activPAL accelerometers for 10 days. Sitting time, steps, and moderate-intensity physical activity (MPA) were compared between weight-bearing (WB) and non-weight-bearing (NWB) groups.
Results:
Two weeks post-discharge, the NWB group sat significantly more than the WB group (median: 14.1 h/day vs. 13.3 h/day; p = 0.04). These differences were apparent for female and middle-aged participants. At 6 months, there were no significant differences between weight-bearing groups for sitting time, steps or MPA.
Conclusion:
Weight-bearing restriction had an early impact on sitting time, but this impact lessened over time. While considering the need for rest, advice about reducing sitting time may be particularly important for people who are NWB post-fracture.
Introduction
Fractures are common amongst working age adults, with approximately one half of men and one-third of women sustaining a fracture before the age of 65. 1 Recovery from even minor fractures can be slow. Lower limb (LL) fractures, in particular, can lead to deficits in range of motion, reduced muscle strength and pain up to 6 months post-injury. 2 The resulting healthcare and productivity costs range from $9800 to $23,100 USD within the first 6 months of recovery for working age adults. 3
Recent research has demonstrated that, for certain lower limb fractures, including fractures of the ankle and tibial plateau, early weight-bearing, and even immediate weight-bearing on the injured limb can improve outcomes. 4,5 Early weight-bearing is not possible for every fracture, particularly those that are unstable. However, for some fractures, less conservative weight-bearing protocols may hasten recovery, without any adverse effects. 6
The benefits of early weight-bearing are likely to relate to patients having a greater capacity for activity, leading to reduced joint stiffness and muscle atrophy. 7 There may also be important psychological and health benefits from being more active. While it is intuitive that patients permitted to weight bear would be more active and less sedentary following fracture, there has been no research to date investigating whether device-measured activity levels differ according to weight-bearing status following LL fracture, nor the magnitude of the difference in activity levels between weight-bearing groups. These data are vital for understanding potential mechanistic pathways to recovery following lower limb fracture.
A previous study investigated return to sport following ankle fracture and found an earlier return to sport with unprotected weight-bearing, compared to non-weight-bearing and protected weight-bearing. 4 While return to sport is an important marker of fracture recovery, the capacity to perform certain activities is not necessarily indicative of a patient’s level of activity. As such, sedentary behaviour and physical activity are important outcomes to measure following fracture.
The aim of this study was to determine whether sitting time, steps and levels of moderate-intensity physical activity differed according to initial weight-bearing status 2 weeks and 6 months after LL fracture in working age adults. A secondary aim was to determine whether differences varied by age and sex.
Methods
Participants
Participants were consecutively recruited for this prospective cohort study from a single major trauma centre in Victoria, Australia over a 6-month period. We included participants aged 18–69 years who were admitted >24 h for an isolated, non-pathological LL fracture (confirmed by X-Ray) and discharged home. Participants were excluded if they had sustained additional severe head or spinal injuries or upper limb/thoracic fractures, or had cognitive or English language deficits. Participants were recruited by a research assistant during their hospital stay and all provided written, informed consent. The study received ethics approval from the Monash University and Alfred Hospital Human Research Ethics Committees.
Procedures
To reduce participant burden during hospitalisation, baseline data collection took place 2 weeks post-discharge on a scheduled outpatient visit to the trauma centre. At this visit, participants were provided with two activity tracking devices. The ActiGraph GTX3+ (ActiGraph LLC, Pensacola, FL, USA) is a tri-axial accelerometer which was used in this study to measure moderate-intensity physical activity (MPA) (equivalent to brisk walking). 8 Participants were instructed to wear the device at the right hip during waking hours for the next 10 days. Waking hours were defined as the time between waking up in the morning and going to bed at night. The activPAL3™ (PAL Technologies Limited, Glasgow, UK) is a tri-axial accelerometer and inclinometer, and the gold standard device for the measurement of sedentary behaviour. 9 This device was used to measure participants’ sitting time and steps. The activPAL has proved more accurate for measuring steps than the ActiGraph at slow walking speeds and when using gait aids. 10 Participants were instructed to wear the device under a waterproof adhesive on the anterior thigh of the unaffected limb 24 h per day for the same 10-day period. During this time participants were also asked to complete a daily log book recording sleep-wake times and any non-wear periods >15 min. Participants returned both devices and the log book via mail. At 6 months post-discharge, the same activity data collection procedures were repeated. Participants received the devices via mail, wore them for 10 days and then returned them to investigators via mail.
A range of additional self-reported data were collected by a research assistant at the 2-week visit, including age, sex, height (m) and weight (kg) (for the calculation of body mass index (BMI) 11 ), pre-injury physical activity levels (via the International Physical Activity Questionnaire-Short Form (IPAQ-SF) 12 ), and current weight-bearing status. Weight-bearing status was categorised as either non-weight-bearing (NWB) where participants were not permitted to bear any weight on the affected limb (e.g. used crutches to hop on the unaffected limb), or weight-bearing (WB) where participants were either partial weight-bearing or weight-bearing as tolerated.
A medical record review was conducted to collect fracture type and management, presence of other injuries and comorbidities, and to verify participants’ weight-bearing instructions at discharge. All participants were automatically registered by the Victorian Orthopaedic Trauma Outcomes Registry (VOTOR), which collects data on all orthopaedic admissions to four trauma centres in Victoria, including the recruiting site. 13 Participants are given the opportunity to opt-off the registry and the current opt-off rate is <2%. 14 Participants in this study also gave written informed consent allowing the investigators to access their VOTOR record. The registry has ethics approval from the ethics committees of all participating hospitals and Monash University. From the registry we extracted participants’ pre-injury work status and their self-reported pre-injury disability status. 15
Data processing
Age followed a bimodal distribution and was subsequently categorised. Pre-injury physical activity levels were categorised as low, moderate and high according to IPAQ protocols. 12 Fracture severity was coded using the predicted Functional Capacity Index based on the Abbreviated Injury Scale (pFCI-AIS). This scale provides a score, ranging from one (worst possible state) to five (perfect state), for the likely functional state 1 year after a specific injury. 16
Activity data were downloaded using ActiLife (Version 6.13.3) and activPAL3™ software. All data were transferred to SAS™ 9.3 (SAS Institute Inc., Cary, NC, USA) for processing. ActiGraph data were sampled at 30 Hz and valid days determined using the Choi algorithm. 17 Additionally, for each day of data collection, heat maps of data were visually inspected for any potential classification errors (e.g. sleep time as waking time). Finally, any potential errors were checked against the patient diaries and the most plausible classification chosen and applied. 9 For activPAL data, the algorithm outlined by Winkler et al. 18 was used to determine sleep/non-wear intervals. To allow for potentially very low activity levels in this population, the ‘any one activity that accounts for >95% of waking wear time’ condition described by Winkler et al. 18 was removed from consideration and the threshold for invalid days was lowered from 500 to 100 steps/day. Where participants had at least four valid days (with ≥600 min of waking wear time/day), 19 total daily sitting time (h/day), steps (n/day), and MPA (1952 cpm–5724 cpm) were standardised to a 16-h day, and then averaged across all valid days. 20 Accelerometry cut points were appropriate for the pre-injury health status and age range of our participants.
Statistical analysis
We conducted a sample size calculation based on previously published data quantifying sitting time in people following limb fracture and a minimal clinically important difference in sitting time of 1 h per day. 21,22 A sample size of 32 was needed to detect a 1 h difference in sitting time between weight-bearing groups (power = 80%, p = 0.05).
Summary statistics were reported as frequencies and percentages for categorical data and the median (interquartile range (IQR)) for skewed continuous data. Participants’ characteristics were compared between weight-bearing groups using chi-square statistics for categorical variables and the Mann Whitney U test for skewed continuous variables. Owing to activity data being highly skewed, even after log transformation, parametric tests were not possible. As such, sitting time (h/day), steps (n/day) and MPA (min/day) at both 2 weeks and 6 months were compared between weight-bearing groups using the Mann Whitney U test and presented graphically using box plots. Additional subgroup analyses compared activity data between age groups and genders using Mann Whitney U tests. All analyses were performed using Stata v.15 (StataCorp LLC, College Station, TX, USA) and a p-value < 0.05 was considered statistically significant.
Results
A total of 47 patients agreed to participate in the study. Forty-six out of 47 participants with LL fractures (98%) returned valid activity data 2 weeks post-discharge and 37 (79%) returned valid activity data at 6 months (Table 1). Approximately two-thirds of participants were non-weight-bearing at the 2-week visit, using crutches or a knee scooter to ambulate (n = 32). All but three of these participants were required to be non-weight-bearing for 6 weeks post-operatively (n = 29). The remaining three were required to be non-weight-bearing for 8 weeks (n = 2) and 12 weeks (n = 1). At the 6-month time point, all participants were fully weight-bearing. All participants but one had their LL fracture treated surgically (n = 45). The mean (SD) age of participants was 38 (13) years. There was a higher proportion of middle-aged adults (35–49 years) in the WB group and a higher proportion of younger adults (18–34 years) in the NWB group, although these differences were not significant. Ankle fractures were the most common fracture type. As expected, there was a significant association between fracture location and weight-bearing status, with the majority of ankle and foot fractures non-weight-bearing, and all hip and patella fractures allowed some degree of weight-bearing. Fracture severity, according to the pFCI-AIS, did not differ significantly between WB and NWB groups. There were no differences in waking hours between the two groups at either time point.
Demographics and injury characteristics for participants with valid data at 2 weeks and 6 months post-lower limb fracture, divided by weight-bearing status.†
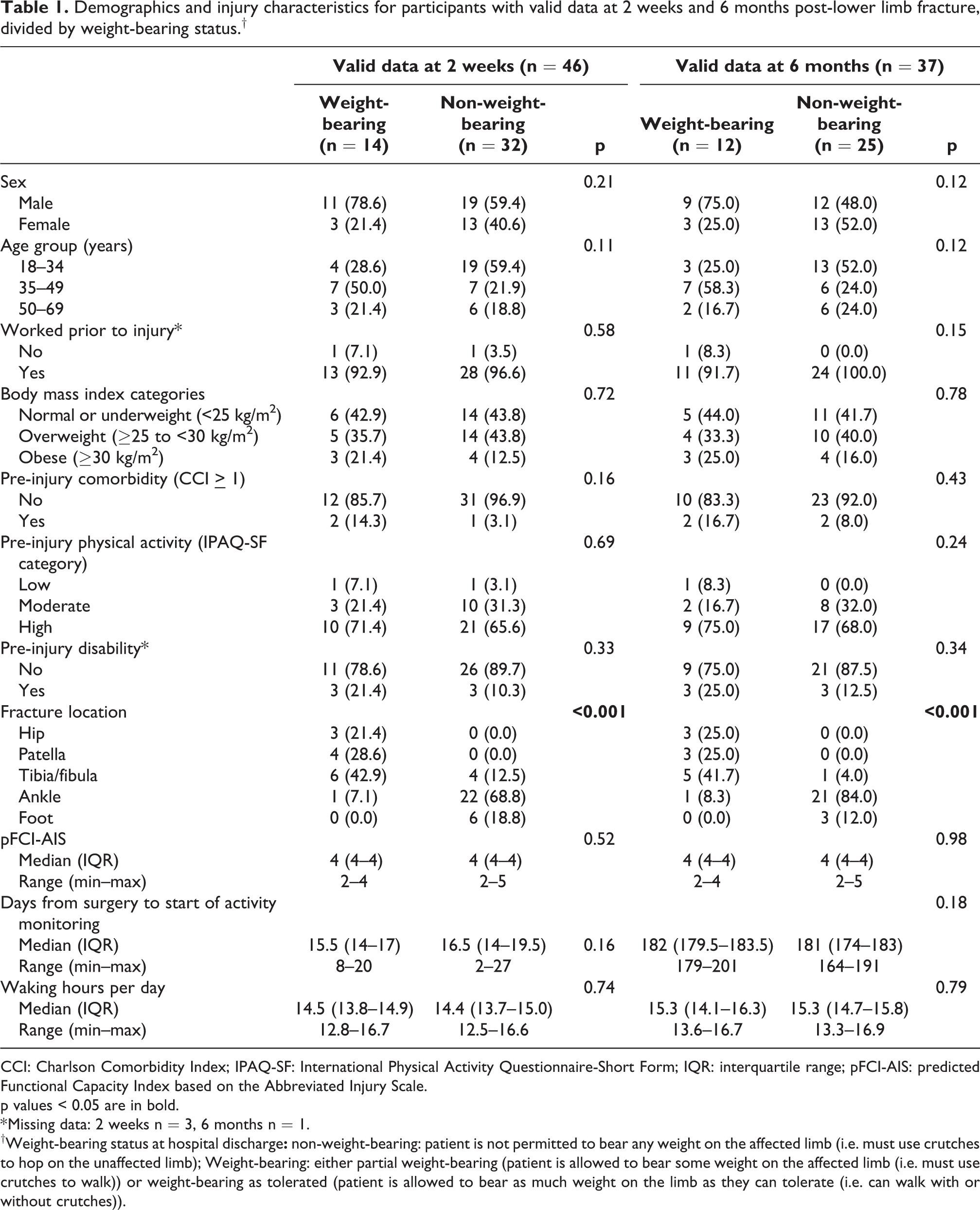
CCI: Charlson Comorbidity Index; IPAQ-SF: International Physical Activity Questionnaire-Short Form; IQR: interquartile range; pFCI-AIS: predicted Functional Capacity Index based on the Abbreviated Injury Scale.
p values < 0.05 are in bold.
* Missing data: 2 weeks n = 3, 6 months n = 1.
†Weight-bearing status at hospital discharge
At 2 weeks post-discharge, participants in the NWB group sat for significantly longer than those in the WB group (NWB: median = 14.1 h/day vs. WB: median = 13.3 h/day; p = 0.04) (Figure 1 and Table 2). At 2 weeks, participants who were non-weight-bearing also took fewer steps than those who were weight-bearing but this difference was not statistically significant. There were low levels of MPA at 2 weeks, regardless of weight-bearing status. However, there were also several outliers with high levels of MPA at 2 weeks (Figure 1). At 6 months post-discharge, there were no significant differences between weight-bearing groups for sitting time, steps or MPA (Figure 1 and Table 2). Values for steps and MPA were highly dispersed at 6 months, particularly in the WB group.
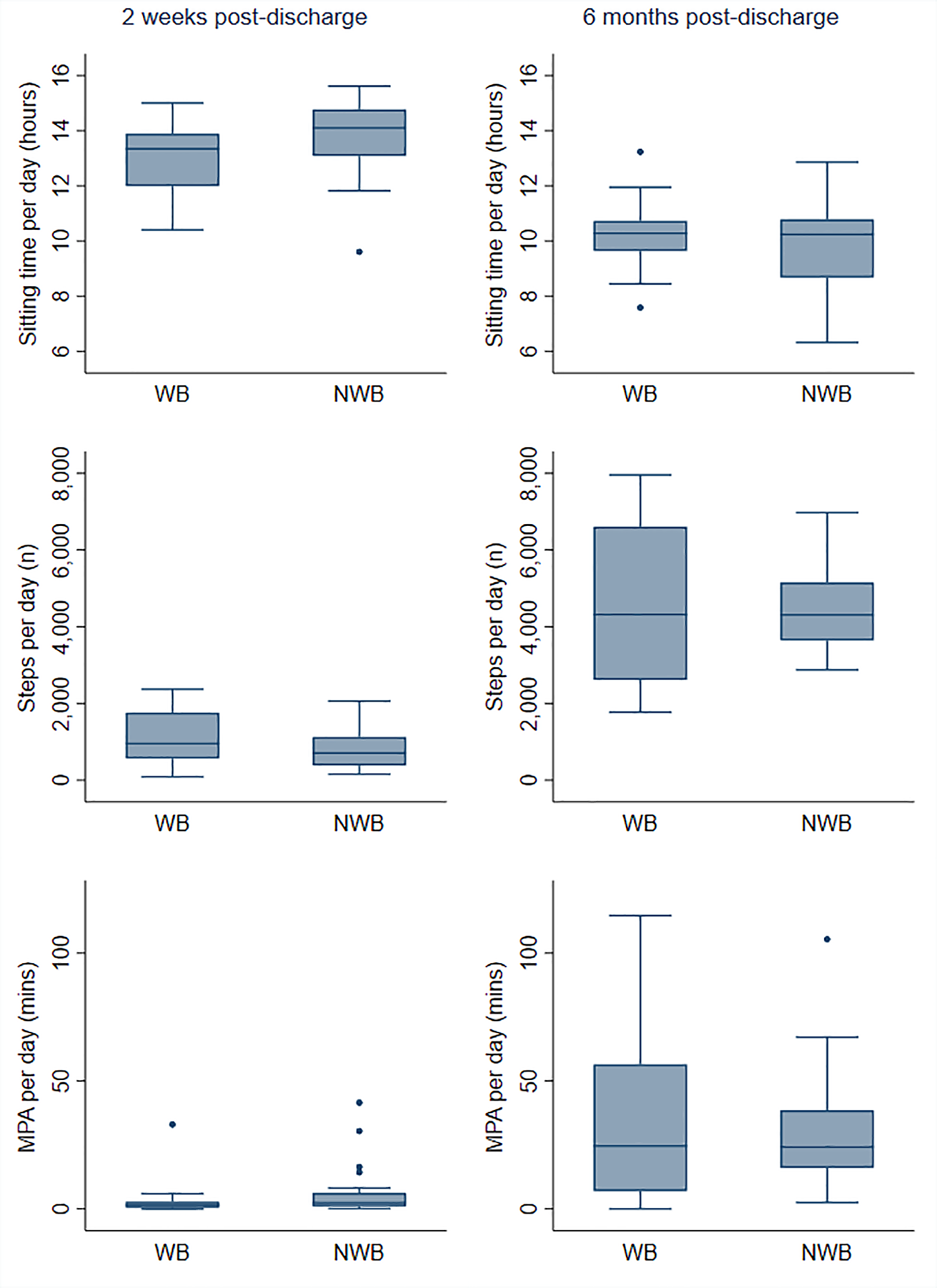
Sitting time, steps and moderate-intensity physical activity (MPA) (median, interquartile range, min–max values and outliers) at 2 weeks and 6 months post-lower limb fracture separated by weight-bearing status.
Median and interquartile range (IQR) for sitting time, steps and moderate-intensity physical activity (MPA) at 2 weeks and 6 months post-lower limb fracture, overall and separated by weight-bearing status.
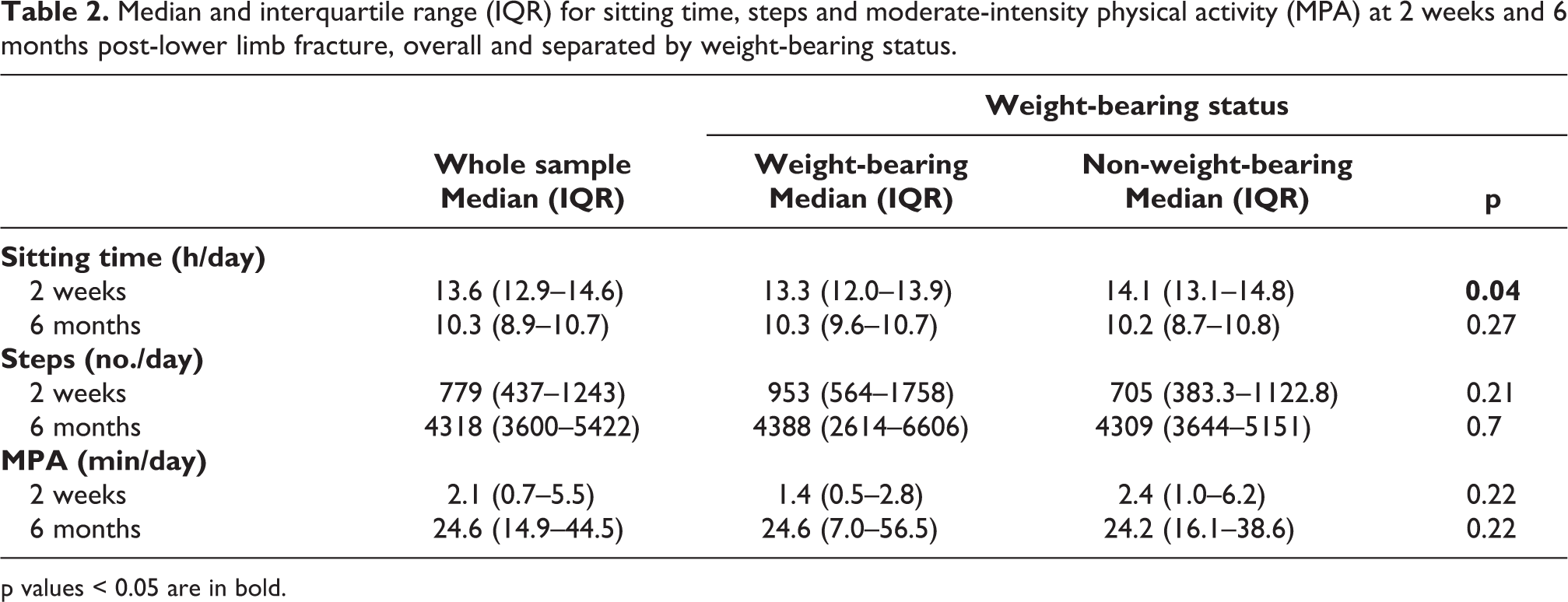
p values < 0.05 are in bold.
Subgroup analyses by sex (Supplementary Material 1) showed that women who were non-weight-bearing sat more at 2 weeks than women who were weight-bearing (NWB: median = 14.3 h/day vs. WB: median = 11.5 h/day; p = 0.03). Also, middle-aged people who were non-weight-bearing sat more at 2 weeks than middle-aged people who were weight-bearing (NWB: median = 14.5 h/day vs. WB: median = 12.6 h/day; p = 0.02) (Supplementary Material 2). For steps and MPA, there were no differences between weight-bearing groups at 2 weeks or 6 months for any age group. However, there were very high levels of MPA at 6 months in younger adults who had been allowed to weight bear at discharge (median = 72.2 min/day).
Discussion
This study aimed to determine whether device-measured activity levels differed according to initial weight-bearing status following LL fracture, and whether differences varied by age and sex. People who were permitted to weight bear following fracture sat significantly less at 2 weeks post-discharge than people who were not permitted to weight bear. However, at 6 months there were no differences in sitting time or activity levels according to initial weight-bearing status.
There was a difference in sitting time between weight-bearing groups at 2 weeks post-discharge of approximately 1 h per day. This result was both statistically and clinically significant. Working-aged adults reporting mobility problems 6 months after fracture, have been shown to sit for almost an hour more per day in the early stage of recovery relative to people with no mobility problems. 21 Prolonged sitting is also detrimental to glucose control, fat metabolism and blood pressure in both healthy and clinical populations. 23 Furthermore, it is possible that an initial drop in activity levels following fracture could establish a pattern of persistent inactivity. Over extended periods, one extra hour of sedentary time is associated with a higher odds of developing type 2 diabetes and metabolic syndrome. 22
At 6 months post-fracture, we found no difference in sitting time or any other outcome between weight-bearing groups. These findings are similar to those of previous research showing that, while people permitted early weight-bearing recover more quickly, delayed weight-bearing groups eventually recover to a similar functional level. 4,5,24 For example, in a recent randomised controlled trial comparing weight-bearing and non-weight-bearing protocols after surgical treatment of ankle fractures, ankle function was higher in the unprotected weight-bearing group after 6 weeks compared to the protected weight-bearing and unprotected non-weight-bearing groups. However, there was no difference at 6 or 12 months. 4 In a retrospective cohort study comparing weight-bearing protocols following tibial plateau fracture, the time from surgery to achieving full weight-bearing was significantly shorter in the ‘permissive’ weight-bearing group compared to the ‘restricted’ weight-bearing group, but there were no significant between-group differences for either quality of life or pain after 1 year. 5 Nonetheless, there is good evidence that unrestricted post-operative weight-bearing reduces the risk of adverse events and complications, such as deep vein thrombosis. 24 Our results indicate that reduced sedentary behaviour may be an added advantage of unrestricted weight-bearing.
Subgroup analyses showed that for women, there was significantly more sitting time at 2 weeks in the NWB group compared to the WB group. This was not because of high amounts of sitting in women who were non-weight-bearing, but instead because of low amounts of sitting in women who were weight-bearing; whereas for men, there were high amounts of sitting in both groups. These findings are supported by research which has shown men to be more sedentary than women following hip fracture. 25 For steps and MPA, the association was reversed, with men tending to be more active than women at both time points. This is also supported by previous research. 25,26
We also showed a significant difference in sitting time at 2 weeks between weight-bearing groups for middle-aged people. Again, this was largely due to low amounts of sitting in the middle-aged WB group, rather than high amounts in the middle-aged NWB group. Contrary to expectations, the youngest age group had the highest amounts of sitting at 2 weeks amongst those permitted to weight bear. This is at odds with previous research, which has shown an increase in sitting time with age following fracture. 25 Similar to previous research however, for steps and MPA, the oldest age group were the least active. 26
Previous research has demonstrated that at 6 months post-injury, both adolescents and working age adults with LL fractures have higher amounts of sitting and lower levels of physical activity than those with UL fractures. 27,28 However, findings from the current study suggest that weight-bearing restrictions may not be the primary reason for this. Instead, it is possible that people with LL fractures experience more pain, more range of movement restrictions, a greater loss of strength, mobility and cardiovascular fitness, or more psychological impacts than people with UL fractures, and that these contribute to their lower activity levels at 6 months. Further research is required to understand the factors influencing activity following upper and LL fractures, and whether these can be altered with early intervention.
The main limitation of this study was the small sample size, which precluded adjustment for the potential confounding effects of sex, age, fracture location and severity, and other health markers, on the association between weight-bearing status and activity levels. We also did not collect data on other potentially relevant health markers such as such as polypharmacy and smoking status. Furthermore, the observational design of this study meant that there was an imbalance in participant numbers between weight-bearing groups which may have led to underpowered comparisons. Also, as is typical in studies of this kind, activity data were highly skewed, even after log transformation, which restricted analyses to non-parametric methods. The inclusion of a diverse range of LL fracture types was both a strength and limitation of this study. Focussing on one fracture type would have resulted in too little variability in weight-bearing advice. Thus, including different fracture types with diverse weight-bearing protocols enabled analysis of weight-bearing as an explanatory factor. However, results are not specific to fracture types or surgical techniques. An additional limitation was the collection of baseline activity levels at 2 weeks, rather than immediately following discharge. This was a pragmatic decision based on the desire to reduce participant burden at the time of hospital discharge, which for many patients is a stressful time. In addition, waiting 2 weeks allowed for acute pain to settle, thereby avoiding an undue influence of pain on activity. It is possible that had data been collected immediately, there might have been a larger difference between weight-bearing groups at baseline. However, weight-bearing status did not change between hospital discharge and the 2-week time point for any participants, and therefore activity levels were unlikely to differ greatly. Finally, while activPAL has been shown to have superior accuracy than ActiGraph for measuring steps in people using gait aids and at slow walking speeds, 10 it has not yet been validated for people hopping on crutches. This is an avenue for future research.
To our knowledge, this is the first study to investigate differences in device-measured sitting time and physical activity levels according to weight-bearing status following lower limb fracture. The results suggest that weight-bearing restriction has an early impact on sitting time, but that this impact lessens with time. While considering the need for rest, advice about breaking up prolonged bouts of sitting and reducing overall sitting time can have important implications for health, 29,30 and is recommended as part of routine post-fracture care, particularly for people who are not permitted to weight bear. Furthermore, our findings provide further encouragement for orthopaedic surgeons to consider early weight-bearing protocols for certain fracture types, where possible.
Supplemental material
Supplemental Material, sj-docx-1-otr-10.1177_22104917211020436 - Do levels of sedentary behaviour and physical activity differ according to weight-bearing status after lower limb fracture? A prospective cohort study
Supplemental Material, sj-docx-1-otr-10.1177_22104917211020436 for Do levels of sedentary behaviour and physical activity differ according to weight-bearing status after lower limb fracture? A prospective cohort study by Christina L Ekegren, Elton R Edwards, Lara Kimmel and Belinda J Gabbe in Journal of Orthopaedics, Trauma and Rehabilitation
Footnotes
Acknowledgements
William Veitch, Dr. Rachel Climie, Professor Neville Owen, Professor David Dunstan, Parneet Sethi, Jennifer Gong, Dr. Anthony Tsay, Praveen K and the Steering Committee of VOTOR are thanked for their assistance with this project. We gratefully acknowledge the participants of this research for contributing their time and effort.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by a Monash University Faculty of Medicine, Nursing and Health Sciences Strategic Grant. The funder was not involved in the study design, data collection, analysis and interpretation of data, the writing of the report or the decision to submit the article for publication. CE was supported by a National Health and Medical Research Council of Australia (NHMRC) Early Career Fellowship (1106633). BG was supported by an Australian Research Council Future Fellowship (FT170100048). The Victorian Orthopaedic Trauma Outcomes Registry (VOTOR) is funded by the Transport Accident Commission (TAC).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.