
Abstract
A number of options are currently available to treat symptomatic knee and hip pain. Among them, there is the use of thermal radiofrequency ablation. It is a more recent technique and we still have a lack regarding safety and effectiveness. In this report, we briefly present a case series of patients with refractory knee and hip pain, treated with thermal radiofrequency ablation, where we discuss the results in safety and effectiveness, concerning not only the pain control, but also the return to participation in activities.
Introduction
Musculoskeletal conditions are the most frequent cause of chronic pain. 1 Knee and hip pain are part of this burden, 1 particularly due to osteoarthritis, since it is the most frequent join diagnosis, and a leading cause of disability with a massive health, social and economic burden. 2 For example, it is expected that nearly half of the population will have symptomatic knee osteoarthritis before the age of 85. 3 Despite readily associated with older age, osteoarthritis can also affect younger people, particularly in certain circumstances, as joint trauma, occupational exposure, obesity or even to genetic predisposition. 4,5 For instance, half of the individuals diagnosed with ligament injuries and meniscal tears will have pain and functional impairment 10–20 years later. 5 Younger people with osteoarthritis are four times more likely to have distress and report a less quality of life than the general population. 4
Currently, some options are available to treat symptomatic knee and hip pain. Among the available options are physical therapy, oral medications (paracetamol, opioids, non-steroidal anti-inflammatory drugs) and supplements, intra-articular injections of corticosteroids, platelet-rich plasma (PRP) solutions or viscosupplements and surgery. 2,6 The use of thermal radiofrequency ablation (TRA) is a more recent intervention to treat knee and hip pain. This technique uses thermal energy produced by an alternating current and delivers this energy to destroy nerve tissue, blocking pain conduction. 7 Many studies have demonstrated the analgesic benefits. 8 –14 However, due to the heterogeneity of the techniques and the lack of long-term safety and effectiveness data, this recommendation is still consider conditional. 6
In this report, we briefly present a first case series of patients with refractory knee and hip pain, treated with thermal radiofrequency ablation. We discuss the main outcomes of effectiveness and safety, comparing these data with the current literature.
Case series
We describe a case series of different patients, all of them with refractory knee or hip pain. We consider eligible patients that failed the pain control, after a combination of a conservative rehabilitation program (directed to the treatment of the knee or hip condition) and oral analgesics and intra-articular procedures (if patients were consider eligible). All patients were treated with TRA and all of them were free of any other treatment for at least 4 weeks (including oral analgesics). The procedure was performed with ultrasound guidance, with visualization of the nerves and tube trajectory. After needle placement, it was used sensitive electrical stimulation to be aware of the nerve proximity and then performed under peripheral nerve block/anesthesia. It was performed by physicians with excellent ultrasound skills and experience in the technique and took place in the office setting of a Musculoskeletal Rehabilitation and Intervention Unit. Visual Numeric Scale—VNS—(0-10) was used to characterize pain intensity. The patients were evaluated 6 weeks after the procedure and a long-term follow-up was scheduled (at 3, 6 and 12 months). Immediate and late adverse effects were screened. The return to the usual/previous interrupted activities because of the pain were asked. For all patients, the procedure was explained, considering risks and benefits. All patients gave their informed consent to perform the intervention. All patients gave their consent to be included in this report. We treated the data anonymously in respect to the patients privacy.
Case 1
A 47 years old male, with history of medial meniscectomy 5 years before, due to a painful meniscal tear, presented with left knee pain (VNS 6/10), in the medial compartment, due to a grade IV Kellgren-Lawrence classification knee osteoarthritis. The pain was not significantly reduced after the combination of a conservative rehabilitation program, oral analgesics, and intra-articular viscosupplements and autologous PRP injections. The patient was proposed to cadaver meniscus transplant versus total or partial knee arthroplasty surgery. In the meantime, we performed an ultrasound-guided thermal radiofrequency ablation of the superior and inferior medial genicular nerves. At the first evaluation, 6 weeks after the procedure, the patient had returned to the practice of physical activity with hiking and bicycle (30–40 kilometers), presenting significant pain reduction, with pain of 3/10, during the more strenuous/prolonged activities. No immediate or late adverse effects were reported.
Case 2
A 72 years old male, with a previous right total knee replacement surgery, presented with right knee pain (VNS 8/10) and a limited knee flexion range of motion, partially due to arthrogenic pain inhibition. Conservative treatment with oral medications and physical therapy failed in reducing pain and improving range of motion. We performed an ultrasound-guided thermal radiofrequency ablation of the superior and inferior medial genicular nerves, superior-lateral genicular nerves and posterior articular rami of the tibial nerve. At first evaluation, 6 weeks after the procedure, the patient had returned to the practice of physical activity with hiking and presented significant pain reduction, with 50% pain reduction (VNS 4/10) during hiking. No immediate or late adverse effects were reported.
Case 3
A 46 years old Jiu Jitsu sportsman presented with bilateral hip pain (VNS 9/10) due to a grade III Tönnis classification hip osteoarthritis, as a result of a femoroacetabular impingement syndrome. This patient had a limitative pain, even to low impact sports activity. Range of motion movements were reduced in all axis. The pain was not significantly reduced after the combination of a conservative rehabilitation program, oral analgesics, and intra-articular viscosupplements and autologous PRP injections. We performed an ultrasound-guided thermal radiofrequency ablation of the articular rami of the femoral and obturator nerves at the right side (the most symptomatic side). At first evaluation, 6 weeks after the procedure, the patient had returned to the sport activity and he presented significant pain reduction (VNS 3/10), during the more strenuous activities, with no pain (VNS 0/10) during regular activities of daily living. No immediate or late adverse effects were reported.
Case 4
A 72 years old male, with degenerative poliosteoarticular joint disease and total left hip replacement surgery, presented with multiple joint pain. Globally, pain improved after physiotherapy and oral analgesics—except for the left hip pain (VNS 9/10). We then decided to perform an ultrasound-guided thermal radiofrequency ablation of the articular rami of the femoral and obturator nerves. At first evaluation, 6 weeks after the procedure, the patient had returned to the practice of physical activity with gardening and hiking and presented significant pain reduction (VNS 2/10). No immediate or late adverse effects were reported.
Case 5
A 66 years old male, with a medical history of Charcot-Marie-Tooth type 1 neuropathy, presented with right hip pain (VNS 8/10) due to a grade III Tönnis Classification hip osteoarthritis. The pain was not significantly reduced after the combination of a conservative treatment with oral analgesics and physical therapy. We performed an ultrasound-guided thermal radiofrequency ablation of the articular rami of the femoral and obturator nerves. At first evaluation, 6 weeks after the procedure, the patient had returned to his normal daily activities and started hiking activities. He presented significant pain reduction (VNS 4/10), during the more strenuous activities of hiking with no pain (VNS 0/10) during normal activities of daily living. No immediate or late adverse effects were reported.
Case 6
A 80 years old female, with multiple degenerative join disease, with right total hip replacement and right osteotomy for valgus knee surgeries, presented severe (VNS 9/10) left knee pain in relation to a medial compartment grade IV Kellgren-Lawrence classification knee osteoarthritis. The pain was not significantly reduced after the combination of a conservative rehabilitation program, oral analgesics and intra-articular corticosteroid and viscosupplement injections. The patient was proposed to total knee arthroplasty surgery, but she was completely reluctant to another orthopedic surgery. We then decided to perform an ultrasound-guided thermal radiofrequency ablation of the superior and inferior medial genicular nerves. At first evaluation, 6 weeks after the procedure, the patient had no pain (VNS 0/10) during normal activities of daily living. No immediate or late adverse effects were reported.
Discussion
The TRA of the joint sensory nerves has progressively gained interest as an intervention for refractory knee and hip pain, in patients who have failed conservative and surgical treatments or are not suitable to surgical interventions. The procedure is manly described in literature using fluoroscopic guidance to target the nerves, by relying on bony landmarks and it is more used in the knee joint. This approach fails not overtaking anatomical variations and also not providing visualization of vascular structures. 15,16 For these reasons, the efficacy may be lower than expected and vascular injuries (the formation of pseudoaneurysm, arteriovenous fistula, hemarthrosis, and/or bone osteonecrosis) can occur. 15
In respect to knee pain, the published data points out that more than 60% of patients have pain relief for as long as 6 months or more in knee osteoarthritis. 11,12 Considering hip pain, the TRA is more infrequently used and less literature data are available, despite some evidence of the effectiveness and safety. 17 Furthermore, some studies used pulsed radiofrequency ablation and not TRA 13 and include only patients with various comorbidities and for that reason consider to be nonsurgical candidates 14 and not patients that simply failed other therapeutical interventions. A case report by Kim et al. 18 showed a significant reduction in pain and increase in functionality at 2 weeks, 4 weeks, 6 months and 2 years after TRA in a patient with persistent hip pain after total hip arthroplasty.
Our case series of six patients treated with TRA showed a significant reduction in experienced pain, with all of them with over 50% of pain reduction. The three patients with refractory hip pain were consider the ones with the greater benefit—higher initial pain score, the bigger percentage of pain reduction. All patients returned to usual/previous interrupted activities and were satisfied with the procedure.
Intending to surpass the limitations of fluoroscopic guidance, we used ultrasound guidance. In this approach, we visualize the nerves and, in any doubt, we visualize genicular arteries that are always along the nerves. We performed the intervention closely visualizing tube trajectory till the nerve and then, in all patients, we placed the active thermogenic needle tip right next to the nerve (Figures 1, 2 and 3). The results presented in literature take into account all approaches (fluoroscopic and ultrasound-guided). We believe and hypothesize that more accurate nerve identification and needle placement can give more time of pain relief until myelinization and nerve sprouting occur, with no adverse effects in the majority of patients.
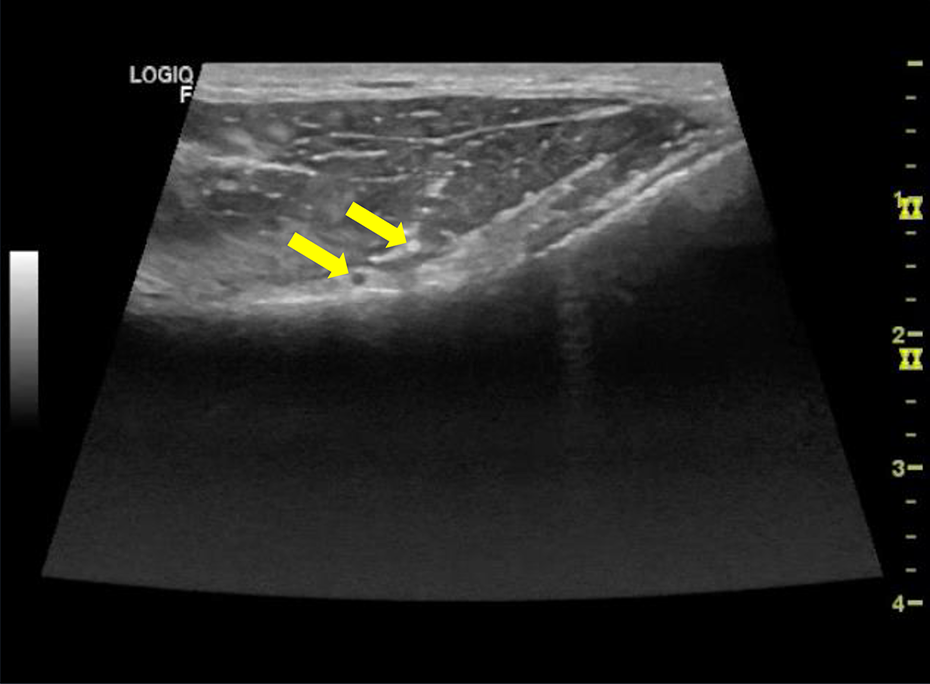
Genicular nerve and artery.
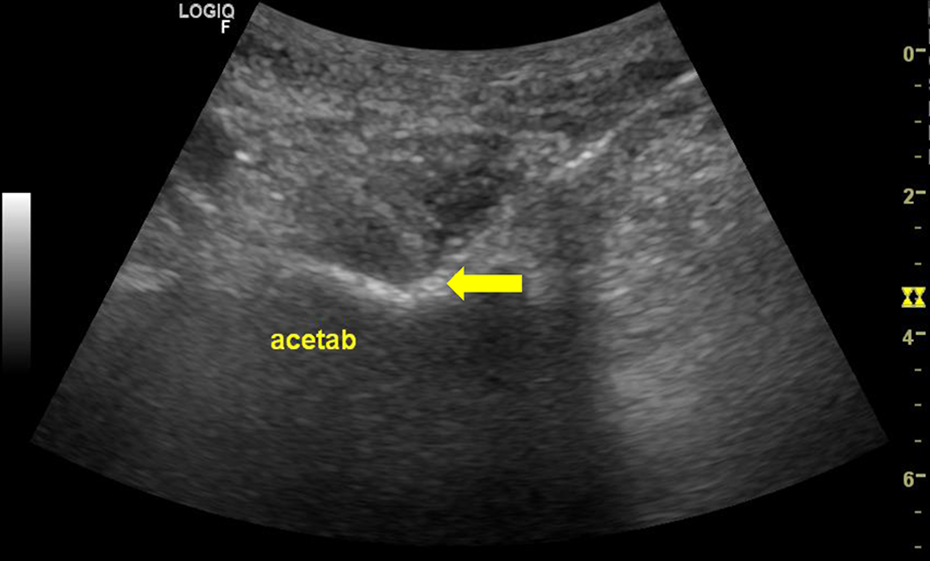
Hip articular rami (acetab - hip acetabulum).
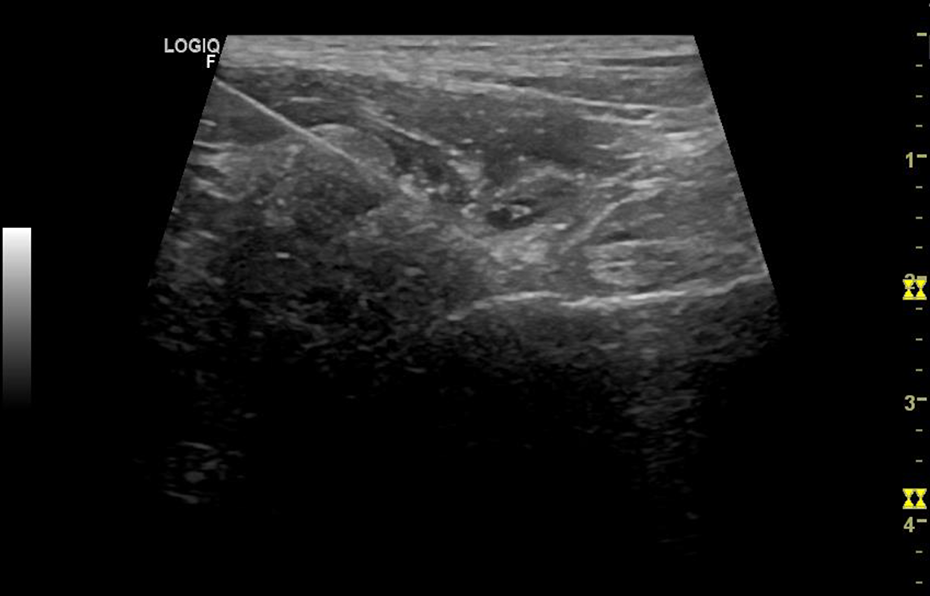
Thermogenic needle. Hip Joint.
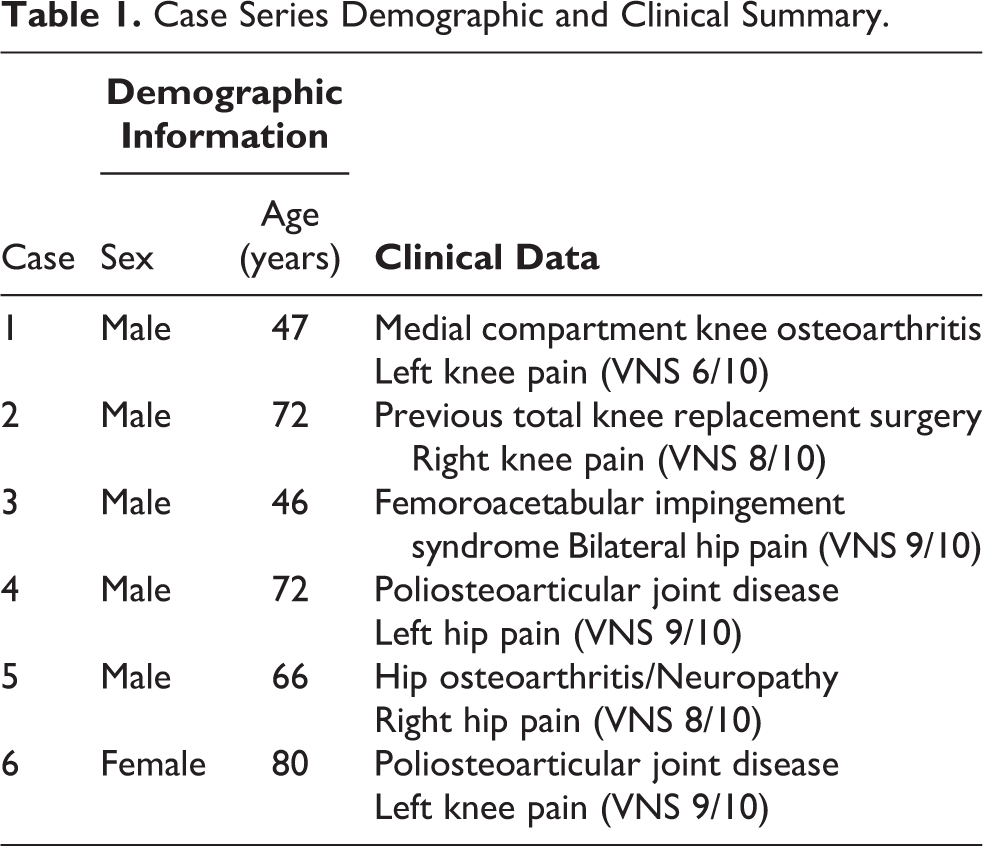
Case Series Demographic and Clinical Summary.
In the treatment of knee pain, we performed a different nerve selection in different patients. This was based on the patient condition. When there was a medial compartment pathology, as in the medial comportment knee osteoarthritis, medial genicular nerves were chosen and, when there was a more diffuse pathology, all approachable genicular nerves were intervened.
Our results are in line with literature data, demonstrating that geniculate nerve TRA is superior to nonsurgical treatment of knee pain with no frequent adverse effects, as opposed, for example, to the known neurological, cardiovascular, gastrointestinal, hepatic and renal effects of some oral analgesics (manly NSAIDs and opioids) or accelerated cartilage loss and periprosthetic infection of corticosteroid injections. In respect to hip pain treatment, the lack of studies imposes difficulties comparing our results. Nonetheless, hip pain patients were the ones with the greatest pain relief and no adverse effects were reported.
Some important limitations need to be notice. We used the VNS and took into account the return to previous activities but objective measures were not assessed. We consider that a systematic approach with validated and reliable objective measures are needed in the future.
As authors, we believe these results will contribute to the knowledge and impulsion of this relatively new pain management procedure.
Future considerations
We present the preliminary data, intending to continue the cohort of patients and following patients in a schedule follow-up, to evaluate long-term results of pain relief and late adverse effects.
We agree that more studies are needed to evaluate the short- and long-term benefits of this procedure, as so immediate and late adverse effects. It is important to evaluate pain relief, but also the return to the previous suspended or limited activities and to measure quality of life before and after the procedure. The economic impact of time pain relief are also an important component to evaluate prospectively. Furthermore, comparative studies of the approach are needed to ascertain the more effectiveness strategy.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.