
Abstract
Introduction:
Minimal invasive fixation of fragility pelvic fracture is feasible with advancement of computerized navigation. However, the clinical outcomes compared with conservative care were seldom mentioned.
Method:
This is a retrospective study comparing the outcomes of elderly with stable pelvic fracture treated conservatively or operatively using computerized navigation. Outcome parameters included pain score, analgesics requirement, length of hospital stay and complication(s), if any.
Result:
Operations were performed in 15 patients from July 2017 to November 2018. A retrospective cohort of 37 patients who were treated conservatively was recruited. In the operative group, it showed a statistically significant reduction in analgesics consumption at 4-week time only. There was significant improvement in pain score at 1-week, 4-week and 3-month time. Patients showed earlier return to premorbid walking status. No major surgical complication was noted.
Conclusion:
Treating fragility pelvic fracture with computerized navigated screw fixation achieve better pain control, reduction in analgesics requirement and earlier mobilization.
Introduction
Most pelvic fractures sustained in the elderly occur from low energy trauma. Osteoporosis, fragility, and propensity to fall appear to be associated with increased risk of pelvic fracture in this age-group of patients, which is different from the younger population who usually result from high energy trauma.
In the past, elderly who suffered from mechanical stable and uncomplicated pelvic fracture pattern were usually treated conservatively with analgesics and bedrest. 1 –3 However, suboptimal pain control is common. 4 Delayed mobilization always leads to complications, including hospital related illnesses, thromboembolism and even death. 5
Operative management is usually required in patients with mechanical unstable and complicated pelvic fracture. Open reduction and internal fixation or external fixation is needed. However, it is associated with lots of complications as well, including high operative risks, significant amount of blood loss, implants problem, wound complications, etc. 6 Traditionally, screws fixation is assisted mainly by intraoperative fluoroscopy, but it is difficult to ensure the correct trajectory of the screws. There are potential risks of neurovascular 7 or pelvic organ injuries given the narrow pelvic corridor. 8,9 With the recent advancement of computerized navigation, minimal invasive procedure has become a popular option in treating osteoporotic fracture.
Many literatures have reviewed the surgical details, feasibility and also the safety issues of the navigation technique in pelvic fracture, 10,11 but seldom has discussed about the clinical outcomes, including the pain control, analgesics requirement and also the rehabilitation in terms of mobilization status.
The aim of the study is to evaluate and compare the outcomes between patients undergoing navigation assisted screw fixation and those treated conservatively. The null hypothesis is that the outcome between the two groups (i.e. interventional group and conservative group) is the same.
Methodology
This is a retrospective cohort study.
There are two groups of patients in this study (i.e. the operative group and the conservative group). All patients were admitted consecutively through the Accident and Emergency Department in North District Hospital (NDH) to the Department of Orthopedics and Traumatology Department, NDH from July 1 2017 to November 1 2018.
Inclusion and exclusion criteria for operations are shown in Figure 1.
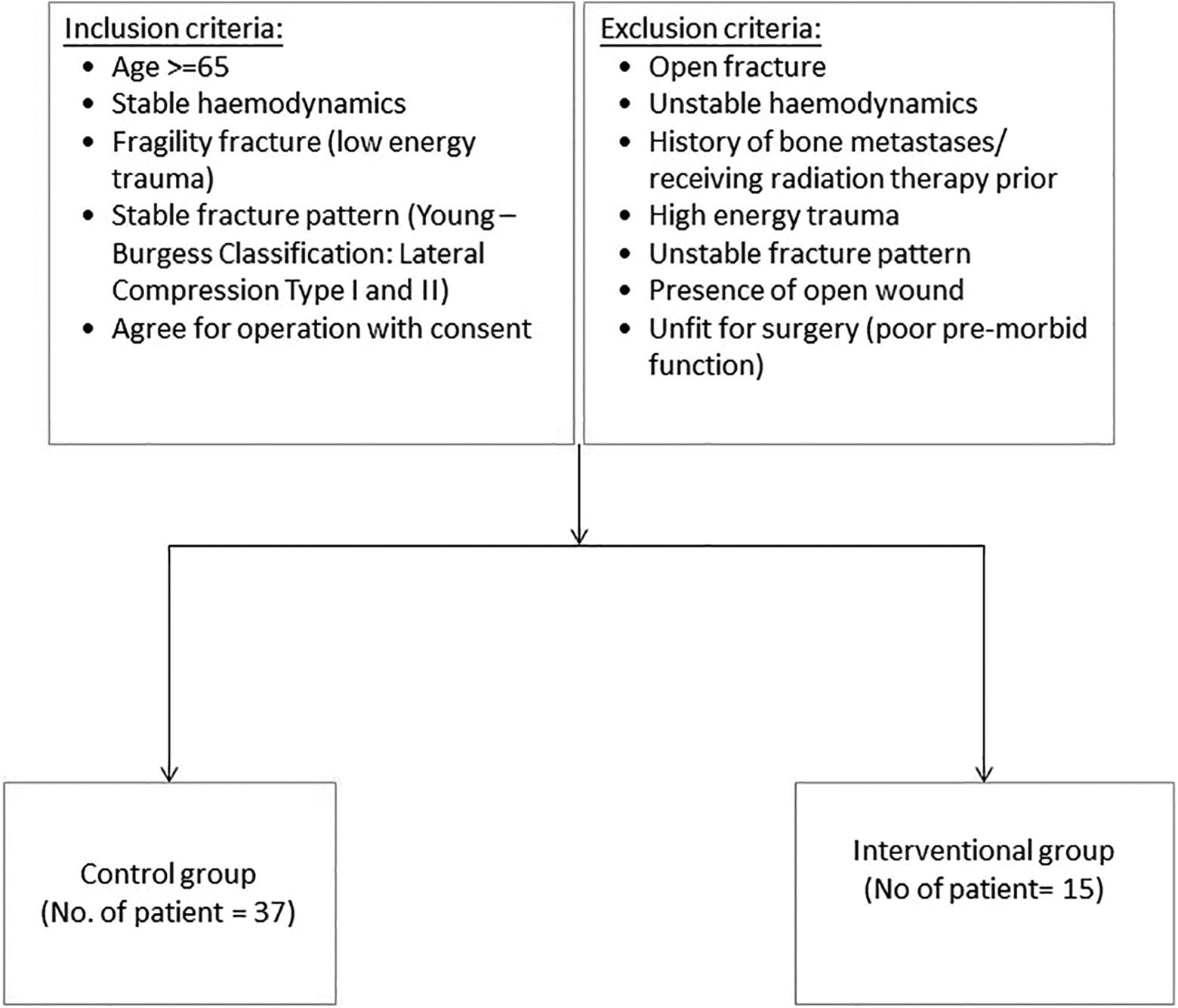
Flowchart showing inclusion and exclusion criteria for operations.
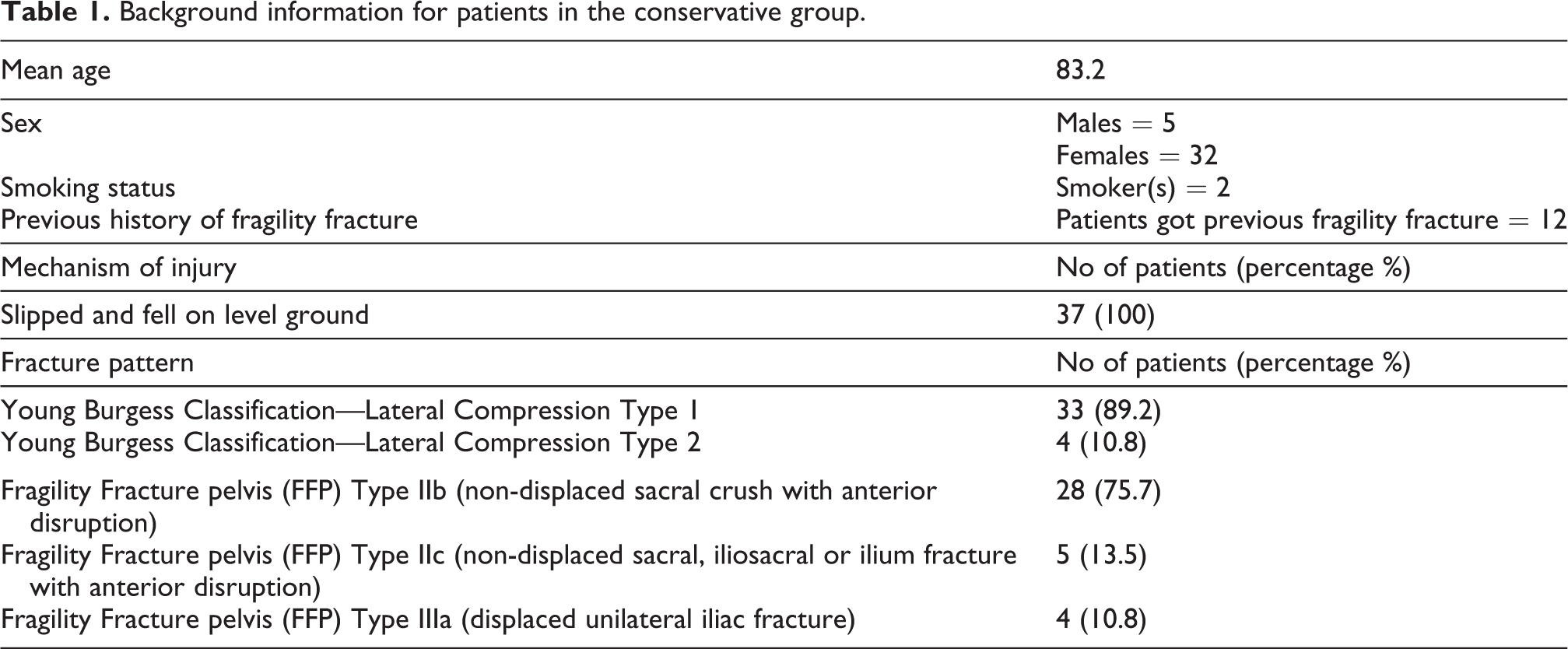
On admission, patients were studied on The demographics (including the age, sex, smoking status, previous history of fragility fractures—fracture distal radius, geriatric hip fracture, osteoporotic vertebral collapse, if any); The fracture pattern and The mechanism of injury
The chief classification system of pelvic fracture used in this study is Young Burgess classification, which was classified according to the mechanism of injury. Another supplementary classification system—“Fragility Fracture pelvis (FFP)” published originally by Rommens and Hofmann in 2013 12 —was also employed in this study in which it was mainly based on the degree of instability regarding the fracture pattern.
Patients in the operative group were offered Plain Computed Tomography (CT) of the pelvis to investigate the pattern of fracture. A Digital Imaging and Communications in Medicine (DICOM) disc file would be prepared for pre-operative planning. Stryker NAV3I navigation system was used, combining surgical navigation and pre-operative imaging. Screws length and their optimal trajectory were then evaluated.
Navigation set-up and execution
Patients were offered CT Pelvis upon admission to evaluate the pattern of fracture. A DICOM disc file would be prepared for surgeon’s planning. For un-displaced pelvic fracture, the pre-operative CT imaging would be used for planning directly, determining the best screws length, width and the trajectory. While for patients with displaced pelvic fracture, pre-operative CTs were also done for references which guided our planning during the operation. The acquired anatomical image was then stored in the computer memory for operative use.
Intraoperatively, patients were under General Anesthesia (GA)/Spinal Anesthesia (SA), they were positioned supine on the radiolucent table with cushion support and the Stryker NaV3I system was placed at the caudal side with connection to the Simens Arcadis Orbic 3D C-arm where the calibration cage was installed. Navigation reference tracker was anchored on the iliac crest of the patients for registration (Figure 2). Patients with un-displaced pelvic fracture would undergo intraoperative CT directly. After registration of the pelvic geometry, the images would be merged to the pre-operative one accurately before navigation execution (Figure 3). For those displaced pelvic fracture cases, closed reduction was first carried out by joystick manipulation by pins and then being temporarily fixed with an external fixator. Intraoperative 3D image was generated by intraoperative computed tomography, followed by careful operative planning of screws before execution.
Reference tracker was anchored to the rigid drill sleeve and calibration was then carried out. Stab wound incisions were made for guide pins insertions. Guide pins insertion was executed via the drill sleeve with the aid of real time navigation for confirmation of locations (Figure 4). Serial plain radiographs (X-rays) were made to confirm guide pins in situ before screws fixation. All screws used were 6.5 mm partially threaded cannulated screws with or without washers, they were subsequently inserted and tightened sequentially (Figure 5), with all guide pins being removed afterward. Final X-rays were checked before wound closure.
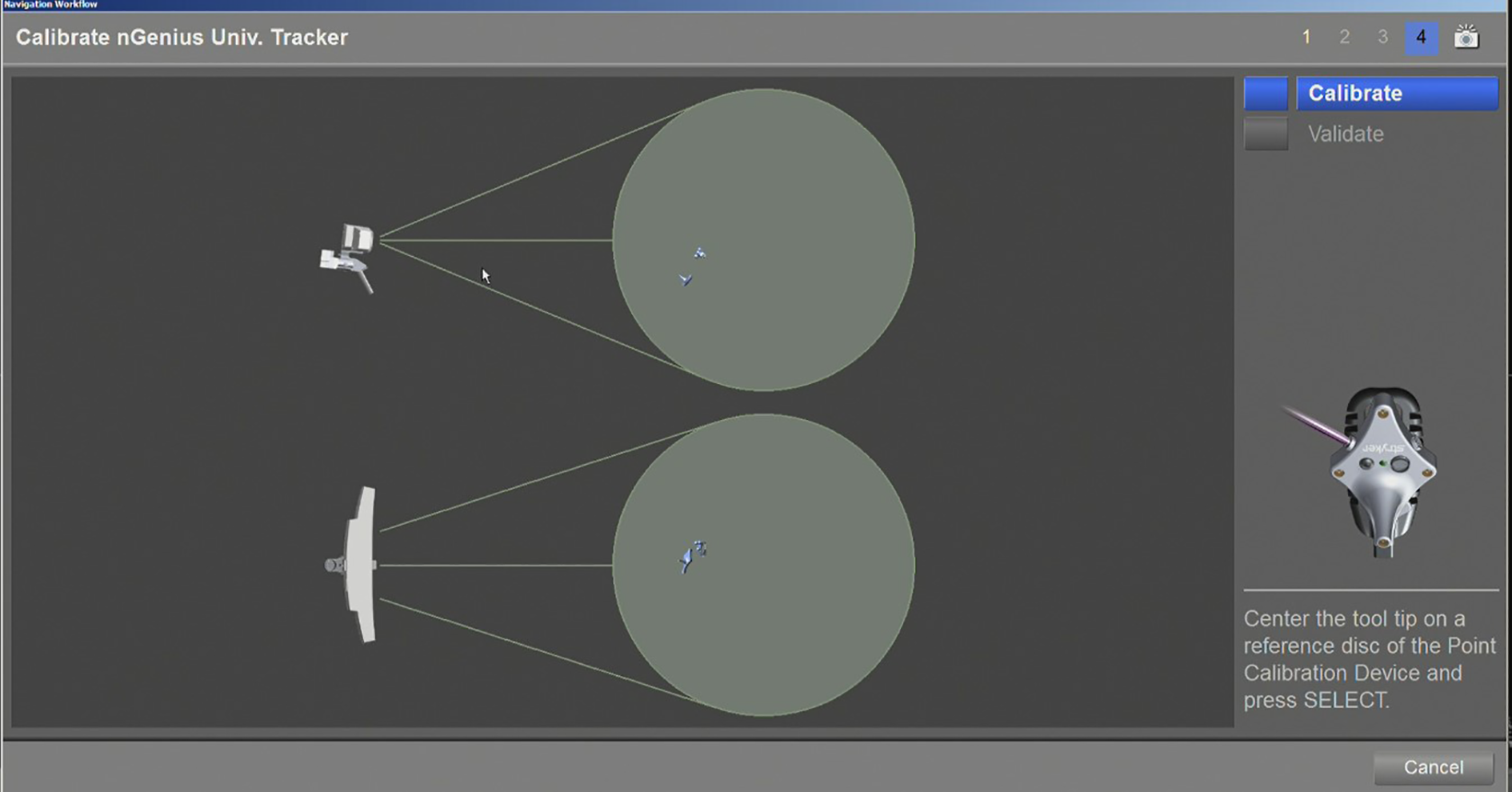
Calibration with the tracker.
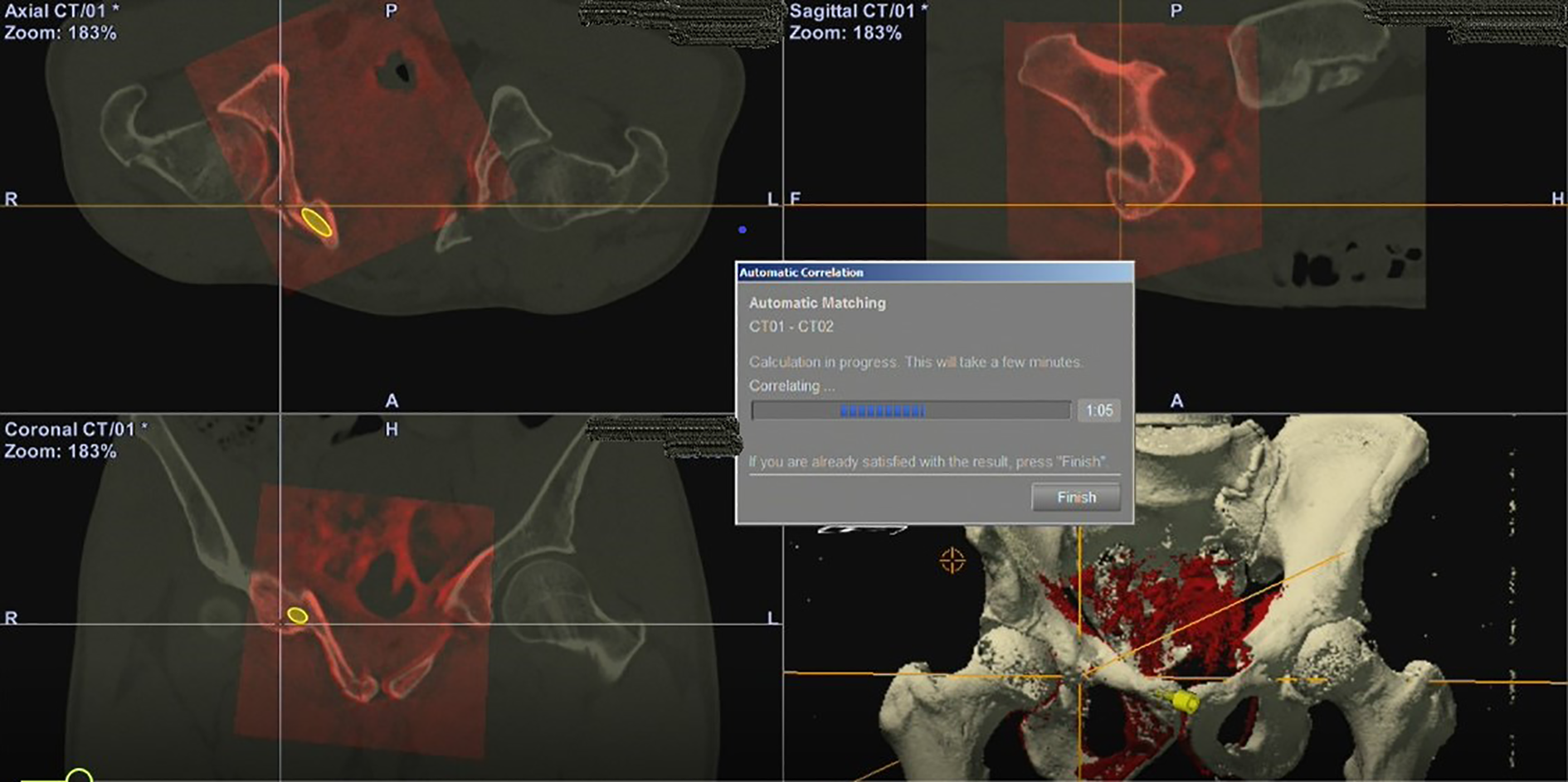
Automatic matching between the pre-operative planning images (red) and the intraoperative CT images.
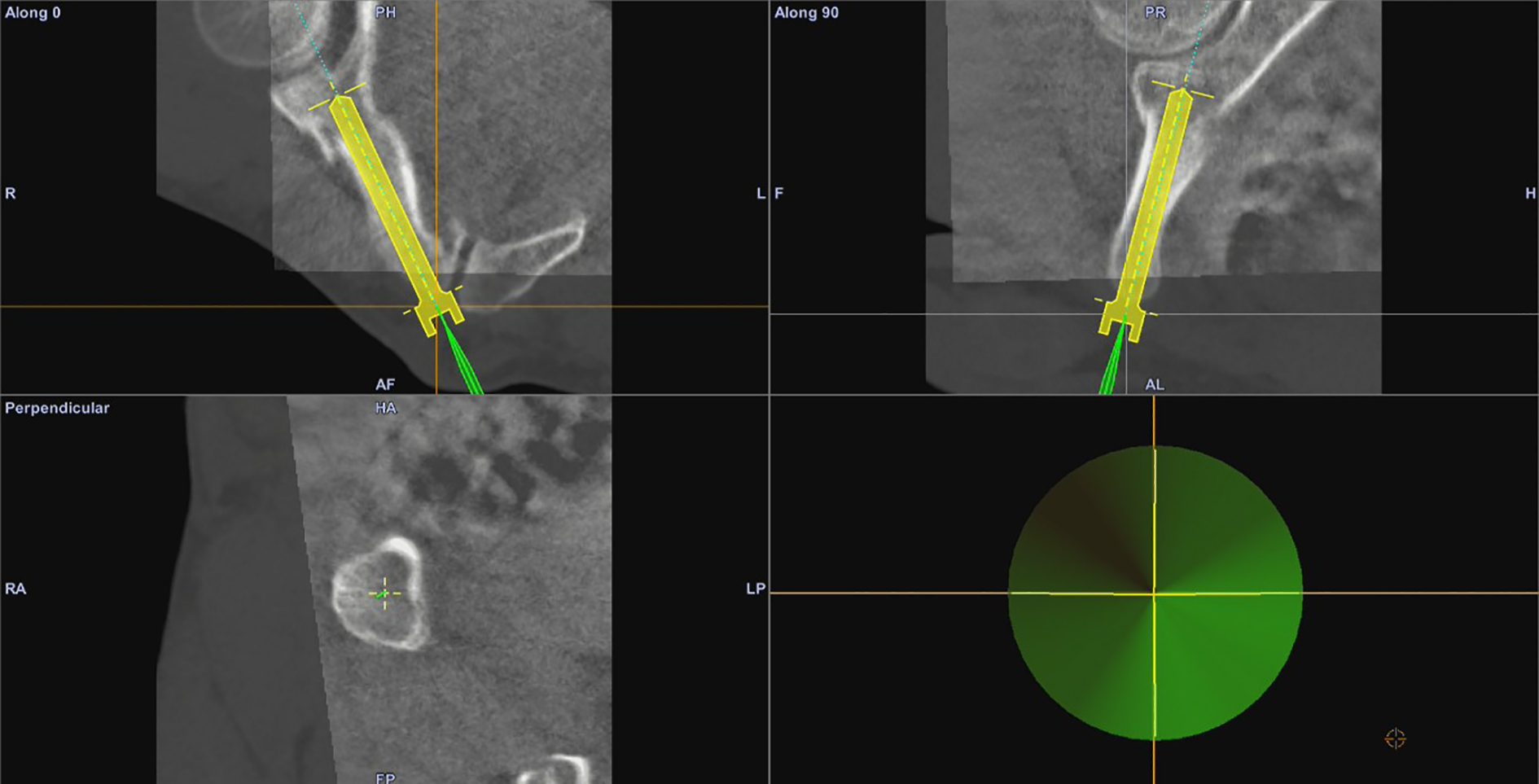
Real time navigation being carried out.
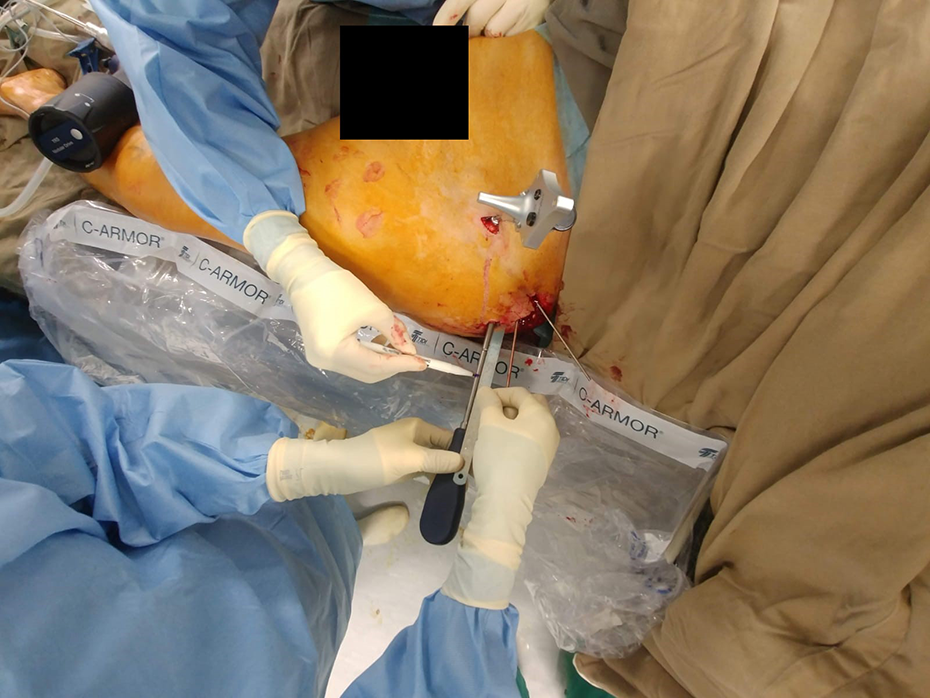
Insertion of screw (screw length marked beforehand to avoid overshoot).
All surgeries (navigation assisted screw fixation) are carried out by the same group of surgeons and navigation assisted screw fixation is used as the standard operative management. Post-operatively, patients would be closely monitored and X-Rays were taken to evaluate the screws position.
The outcomes to be studied for each patient in the operative group were: Pain—Visual Analog Scale (VAS) (pre-operative, post-operative immediate, 1-week, 4-week and 3-month); Number of analgesics used (pre-operative, post-operative immediate, 1-week, 4-week and 3-month); Time for operation; Intraoperative blood loss; Mode of Anesthesia (GA/SA); Total number of screws inserted; The time to achieve premorbid walking status; Length of hospital stay (including acute hospital, rehabilitation hospital, and total length of stay); Surgical complication(s), if any; Percentage reduction in number of analgesics used based on the amount in immediate post-operative, post-operative 1-week, 4-week and 3-month compared with pre-operative amount.
The outcomes to be studied for each patient in the conservative group were: Pain—Visual Analogue Scale (VAS) (on admission, post-injury 1-week, 4-week and 3-month) Number of analgesics used (on admission, post-injury 1-week, 4-week and 3-month); The time to return to premorbid walking status; Length of hospital stay (acute hospital, rehabilitation hospital, and total length of stay); Complication(s) if any during the in-hospital stay; Percentage reduction in number of analgesics used based on the amount in post-injury 1-week, 4-week and 3-month compared with admission amount.
They were either discharged directly or transferred to Tai Po Hospital (TPH) for further rehabilitation if necessary. They were regularly followed up in our Specialist Out-patient Clinic.
Summary of the treatment algorithm for the interventional and conservative group is shown in Figure 6.
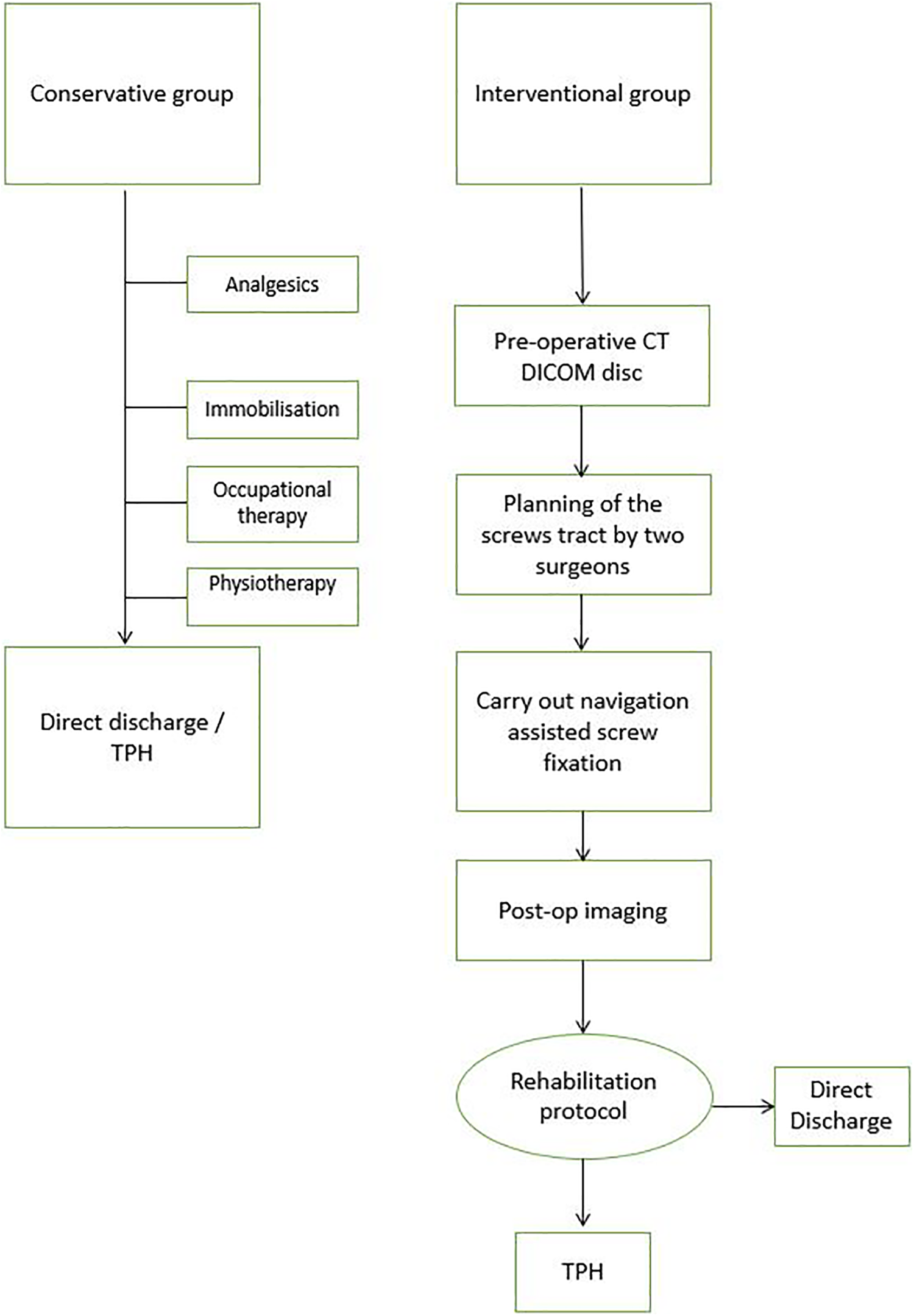
Treatment algorithm of the interventional and conservative group.
Statistical analysis
In this study, statistical software (IBM SPSS version 13) was used for all statistical analyses. Analgesics requirement and VAS score on admission and at various time periods for each group were analyzed using paired T-test. The mean percentage reduction in analgesics requirement, mean VAS score, mean length of stay and the mean number of days required for returning to premorbid walking status for the two groups were compared using independent T-test. A 5% significance level was applied for all tests (P < 0.05).
Results
We reviewed 15 (13 females, 2 males) consecutive patients with pelvic fractures undergoing computerized navigated screw fixation and 37 (32 females, 5 males) consecutive patients with pelvic fractures treated conservatively.
Conservative group
Background information for the conservative group is shown in Table 1.
Background information for patients in the conservative group.
The mean VAS score for the conservative group of patients is shown in Table 2. It decreased from 7.95 on admission to 2.92 at post-operative 3-month.
Paired T-test to compare with VAS score between the value on admission and at various time periods for the conservative group.
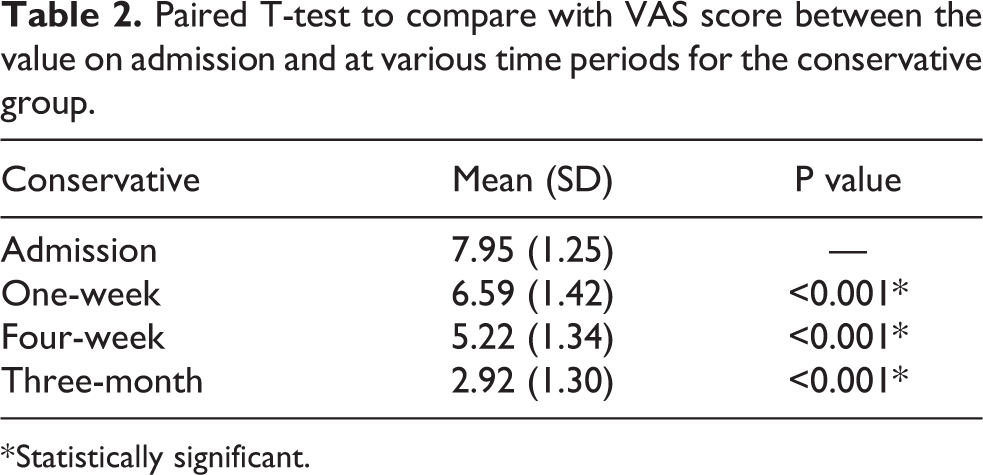
* Statistically significant.
Majority of them consumed acetaminophen (Panadol) and/or tramadol, with four of them required additional analgesics (e.g. Diclofenac Sodium or Indomethacin) on top of these. The mean percentage reduction of analgesics between the dosage on admission and at various time periods is shown in Table 3 for the conservative group.
Paired T-test to compare with mean percentage reduction in analgesic requirement between the dosage on admission and at various time periods for the conservative group.
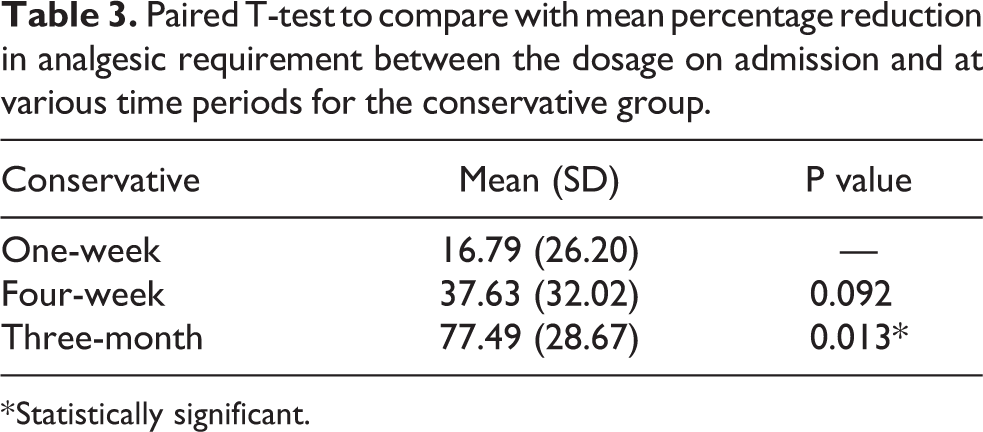
* Statistically significant.
The mean total length of stay in this group of patients was 20.54 days, which included a stay of 6.46 days in acute hospital and 14.08 days in the rehabilitation hospital. The mean number of days required to return to premorbid walking status was 49.00 days.
There were complications arising from this group of patients during the in-hospital stay. Two of them got chest infection in the rehabilitation hospital which required a course of antibiotics treatment with subsequent good recovery. None of them got urinary tract infection, deep vein thrombosis or side effects arising from the prolonged use of analgesics.
Operative group
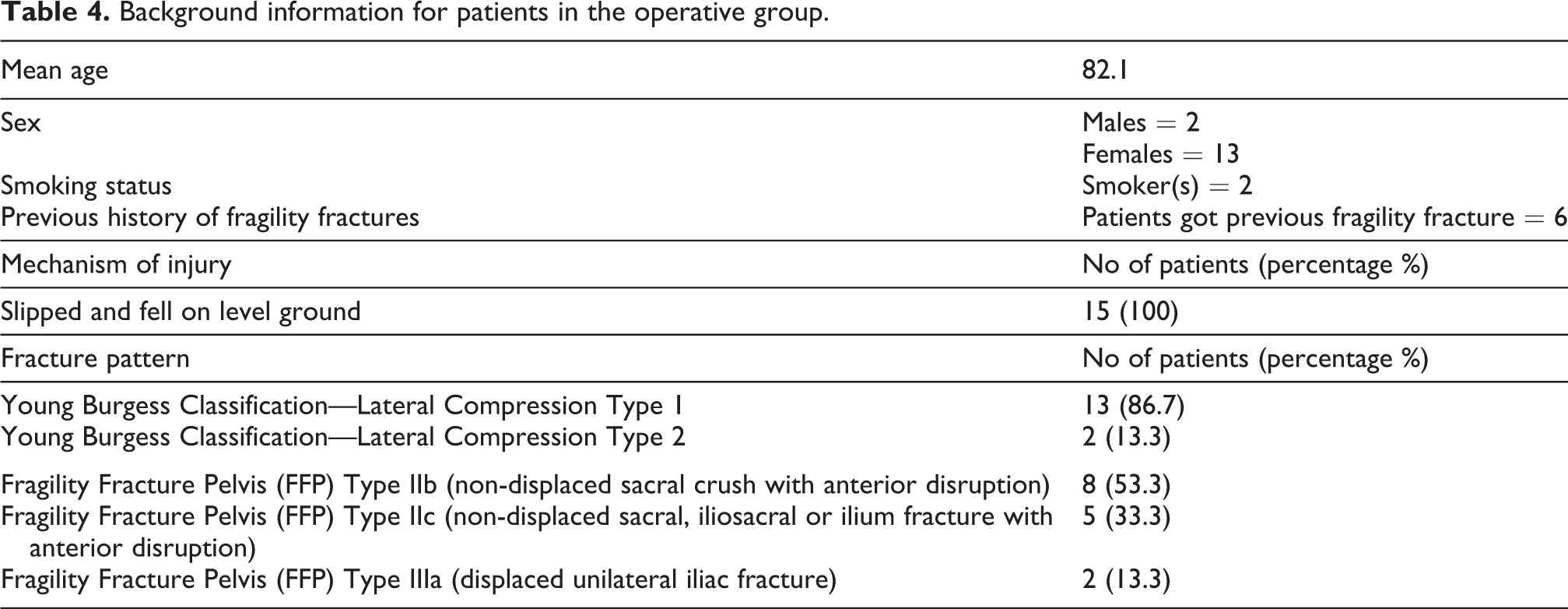
Background information for the operative group is shown in Table 4.
Background information for patients in the operative group.
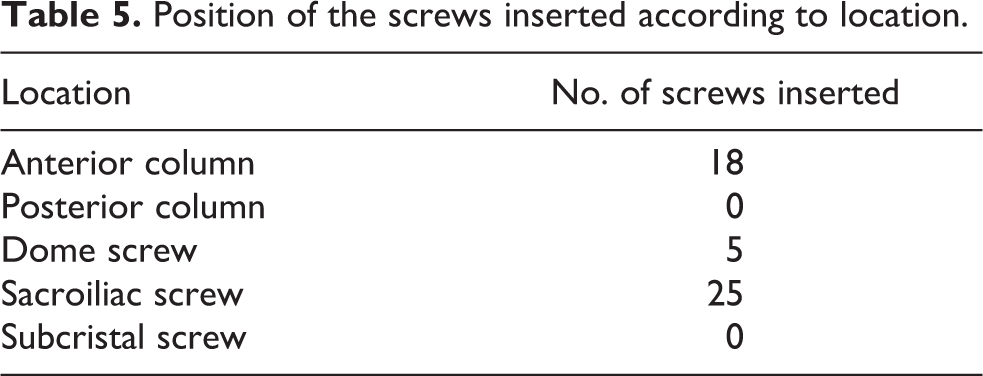
The operations were either carried out under GA (n = 12) or SA (n = 3). The mean operation time was 120.5 minutes and the mean blood loss during the operation was 56 ml. We inserted a total of 48 screws (with location of the inserted screws shown in Table 5), with all of them successfully inserted under the navigation system as planned pre-operatively. Fourteen of them required only one stage operation, from fracture reduction to navigation assisted screws fixation carried out within the same session, while one required a two stages operation with the first stage being executed on external fixation, and a second stage operation was carried out on fixing the iliac wing and acetabulum.
Position of the screws inserted according to location.
The mean VAS score of the group at various periods of time was listed in Table 6.
Paired T-test to compare with VAS score between the value on admission and at various time periods for the operative group.
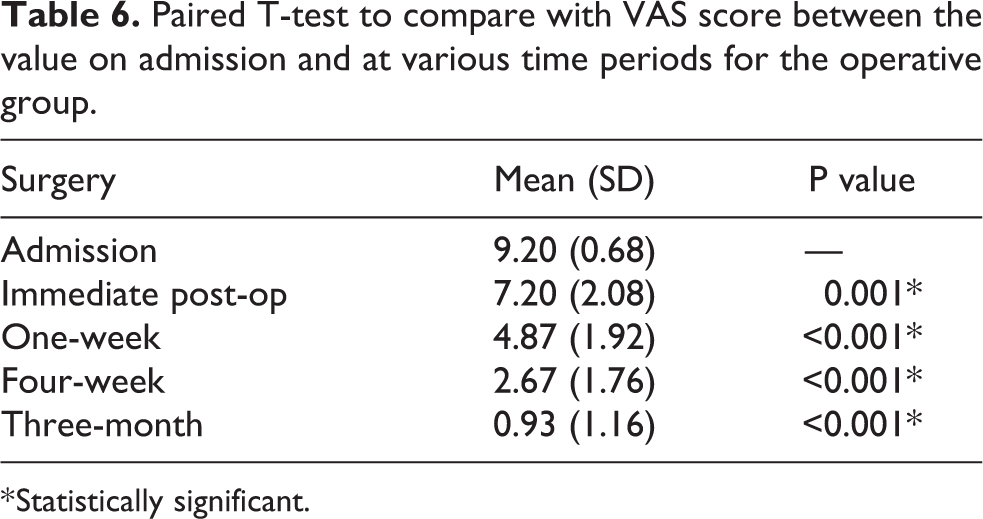
* Statistically significant.
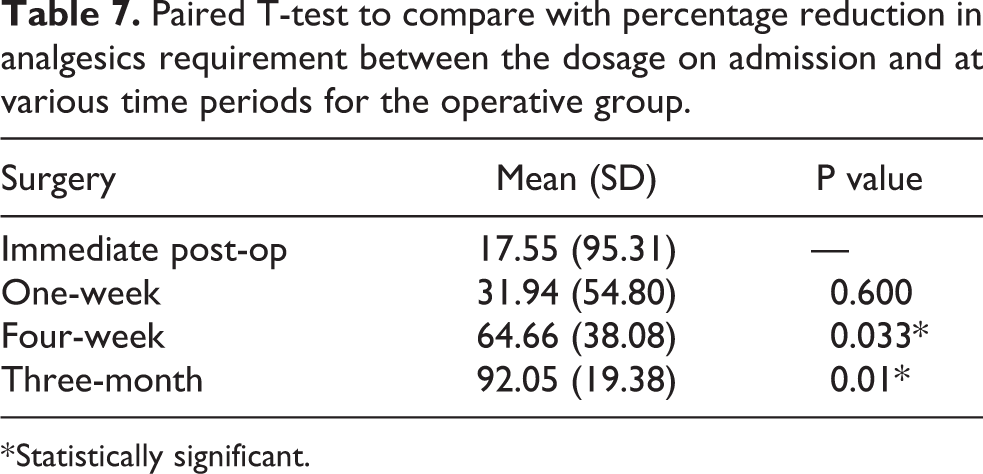
All of the patients in the group consumed acetaminophen (Panadol) and/or tramadol. The mean percentage reduction of analgesics requirement between the dosage on admission and at various time periods is shown in Table 7. At immediate post-operative period, it already showed a 17.55% decrease in the analgesic requirement, with further decrease in subsequent time periods.
Paired T-test to compare with percentage reduction in analgesics requirement between the dosage on admission and at various time periods for the operative group.
* Statistically significant.
The mean length of stay in this group of patients was 29.00 days, which included a stay of 13.27 days in acute hospital and 15.73 days in rehabilitation hospital. The mean number of days required to return to premorbid walking status was 25.77 days.
There was no major complication at immediate or early post-operative period. However, minor complication (i.e. screws backout) occurred in 2 out of the 15 patients. Both got radiological diagnosis of screws backout with the superior pubic rami screws. None of them was symptomatic and the fracture sites with screws had already healed with callus shown in subsequent X-rays. All patients in the operative group were still followed up in our Specialist-Out-Patient Clinic.
Parameters comparison between conservative group and operative group
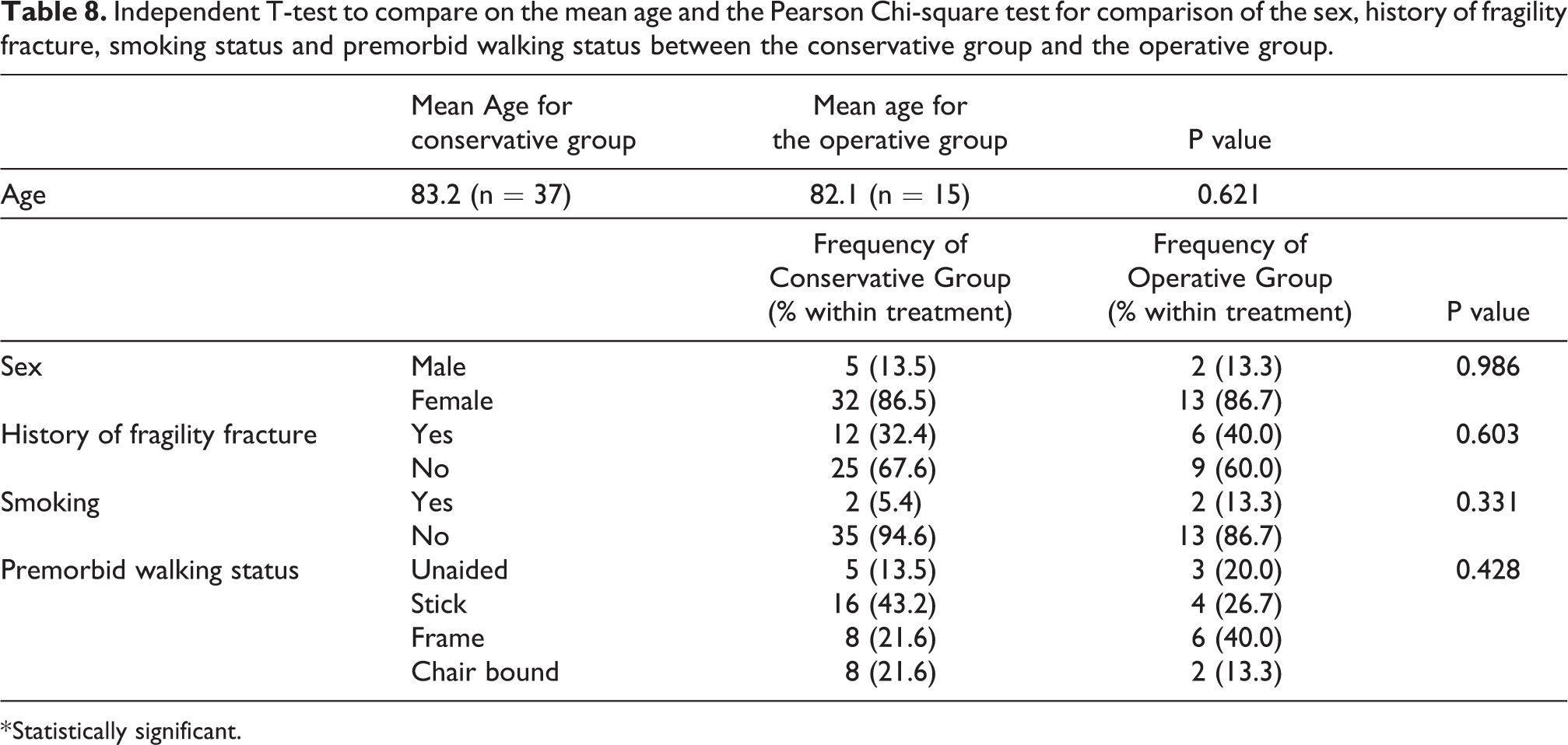
There was no significant difference regarding the background data between the two groups including the mean age, sex, previous history of fragility fracture, smoking status and premorbid walking status as shown in Table 8.
Independent T-test to compare on the mean age and the Pearson Chi-square test for comparison of the sex, history of fragility fracture, smoking status and premorbid walking status between the conservative group and the operative group.
* Statistically significant.
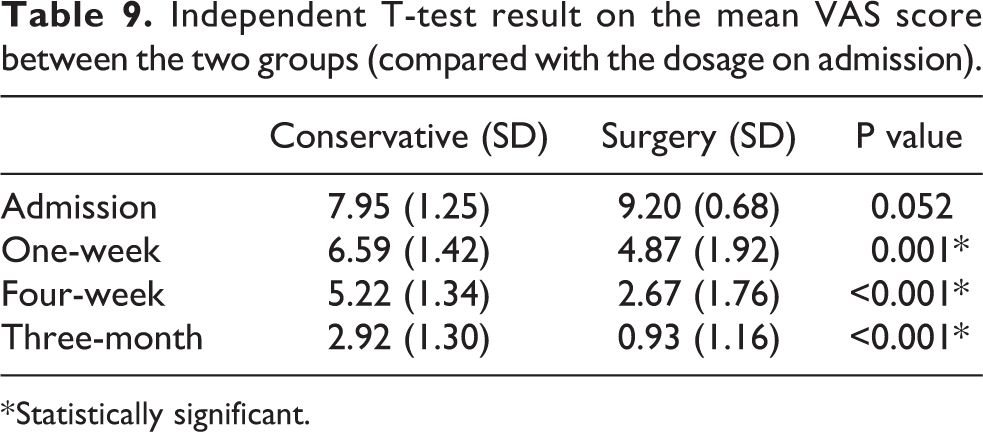
The mean VAS score also showed significant improvement in 1-week (4.87 vs 6.59, p = 0.001), 4-week (2.67 vs 5.22, p < 0.001) and 3-month time (0.93 vs 2.92, p < 0.001) for the operative group, with details being shown in Table 9.
Independent T-test result on the mean VAS score between the two groups (compared with the dosage on admission).
* Statistically significant.
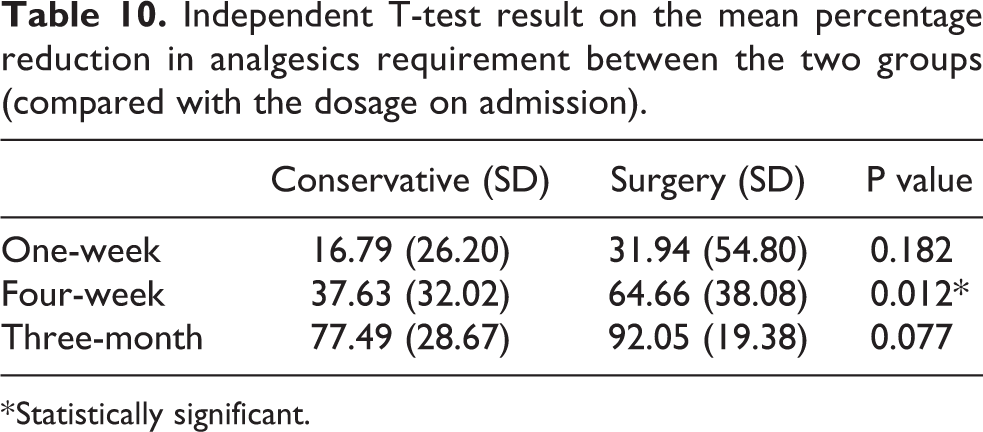
Table 10 showed a statistically significant percentage reduction in analgesics consumption in 4-week time (64.66% vs 37.63%, p = 0.012) for the operative group. However, there is no significant reduction in 1-week and 3-month time.
Independent T-test result on the mean percentage reduction in analgesics requirement between the two groups (compared with the dosage on admission).
* Statistically significant.
Patients in the operative group were able to have an earlier return to their premorbid walking status with statistical significance (Table 11). However, there was no significant difference between the two groups in terms of mean length of stay in hospital (Table 12).
Independent T-test result on the mean number of days required for returning to premorbid walking status between the two groups.
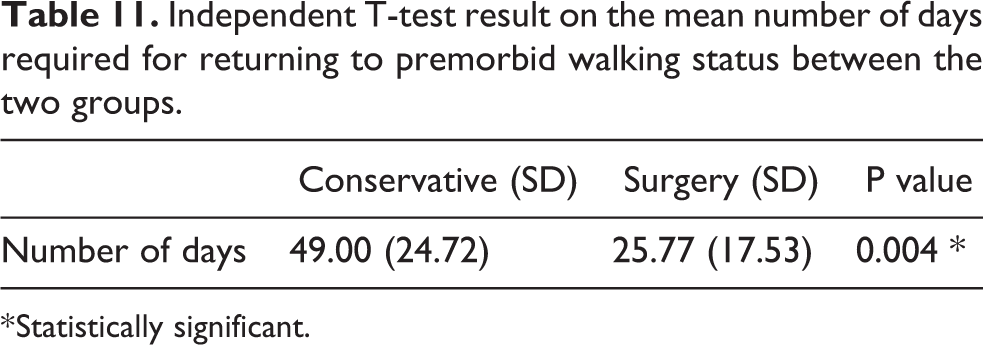
* Statistically significant.
Independent T-test result on the mean length of stay (LOS) between the two groups.
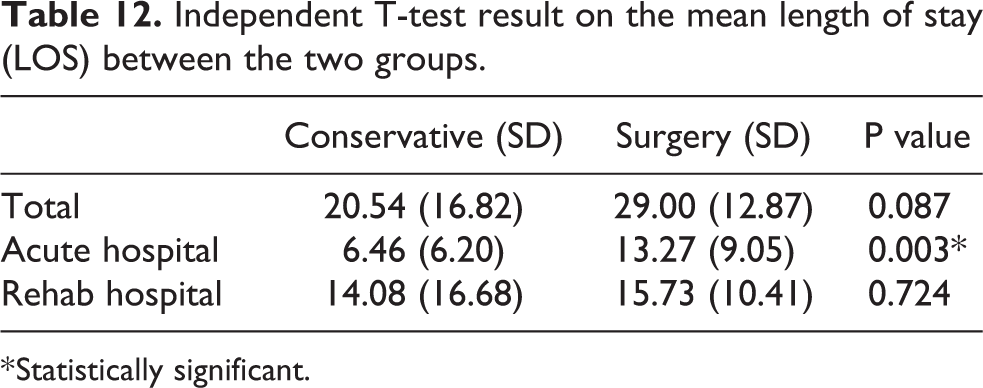
* Statistically significant.
Discussion
Traditionally, patients with mechanical unstable and complicated pelvic fracture usually required open reduction and internal fixation or external fixation. 13 However, it is associated with high incidence of complications. Actually, the complications arising from the surgery depend on many factors, including the fracture type, method of management, presence of any associated injuries, patients’ factors including age and bone quality, etc. Pavelka T and his group 6 grossly summarized the distinguished complications as three main types (i.e. intraoperative, early and late) and described in detail in his article. These complications render open pelvic surgery a highly risk operation.
Computer-assisted surgery was first introduced in orthopedic surgery in 1995. 14 The very first application was spine and pelvic surgery. Stockle and his team 15 were the first to report a clinical series of patients who employed navigation technique to insert sacroiliac screws in pelvic fracture. They inserted a total of 36 screws, with 35 of them placed correctly while the remaining one got perforated into the anterior cortex of sacrum without neurological consequences. They found that CT based navigation is more beneficial in screw fixations for minimally displaced pelvic fracture while fluoroscopic one is more advantageous in sacroiliac screws fixation in traumatic or degenerative instabilities, which required update of images intraoperatively. With the recent advancement and advocation of navigation technology, more and more working groups practiced on the new techniques. In 2013, Peng et al. 16 demonstrated a high accuracy for percutaneous iliosacral screw placement with integration of intraoperative CT, at the expense of higher effective dose compared with the fluoroscopic method. In Hong Kong, the Queen Elizabeth Hospital (QEH) has employed the minimal invasive percutaneous screw fixation (MIS) since 2015 for pelvi-acetabular fracture and have demonstrated a very good result. 17
Interpretation of data
Our center has started to employ the navigation technique for screw fixation in pelvic fracture since 2017. We had 15 patients undergone this type of operation since then. Reviewing the result, the pain score of any individual patient showed improvement with time, regardless of the group patient belonged to. This could be explanatory due to the continuous use of analgesics and fracture healing as time goes. However, the operative group showed consistent significant improvement in pain score in the selected time-frames compared with the conservative group. This concluded screw fixation was more superior in terms of pain control.
In terms of reduction in analgesics requirement, the operative group showed significant reduction in number of analgesics consumption in 4-week time only, but not in 1-week time. This could probably be attributed to the presence of post-operative wound pain noticed in early post-operative period. The mean number of days required for patients to return to premorbid walking status showed statistically significant improvement in the operative group. This concluded that navigated assisted screw fixation could achieve a better pain control and earlier mobilization for our patients.
Our department tried to facilitate the rehabilitation protocol and minimize the length of hospital stay by arranging the operations for our patients in the next available operation session (i.e. usually within 2–3 days). However, the operative group showed no reduction in the mean total length of stay in hospital, with even statistically significant increase in stay in acute hospital when compared with the conservative group. This could be attributed by two reasons. Firstly, we aimed at observing for the wound conditions for a longer period of time. Since the operative wounds were quite near to the perineum, and they could easily get contaminated. Education was given to the nursing staff for proper wound management. Patients were also educated on the wound care prior discharge. Secondly, since it was a new technology in our center, we did spend a lot of resources in the post-operative management and rehabilitation. These included post-operative X-rays for assessment of the screw positions, discussion with physiotherapists for individual progress of every patient, analgesics adjustment, etc. With accumulation of experience, standardization of the treatment protocol and increased familiarity with the system, the mean length of stay for consecutive patients in the operative group was found to have a decreasing trend. This parameter will further be evaluated in our upcoming study. Importantly, there was no major complication reported in the operative group.
Limitations
There were some limitations to this study. First of all, we only had limited number of patients in the operative group for analysis. Despite this a pilot study, we might need larger sample for carrying out a large-scale study for comparison. Secondly, analgesics used in both groups of patients should be standardized. Due to the fact that there may be potential misleading in the number of analgesics requirement if one chose to use more potent analgesics such as non-steroidal anti-inflammatory drugs (NSAIDs). In view of this, our center had just launched a protocol in the end of 2018 which standardized the type of analgesic consumed. The group of surgeons would review the analgesics requirement every day for both the conservative and operative group of patients and make any adjustment accordingly. Also, for all our operative cases, no patient-controlled analgesics (PCA) were employed in the post-operative period. Thirdly, there might be potential selection bias happened because patients who refused operation would be allocated to the conservative group. In the coming future, we will carry out a large-scale randomized controlled trial which tries to randomize the selected patients into different groups in order to minimize the potential selection bias.
Besides, there was also no immediate post-operative CT imaging to compare the screws position with the expected trajectory. Another potential drawback of this study was that the radiation exposure in each operation was not being measured. Although Kraus et al. 18 found out in his study that the effective dosage received was nearly fivefold greater for non-navigated operations than navigated operations for sacroiliac screw insertion, still it was an essential cost to be measured for the operation.
Education of the navigation techniques and future thoughts
Navigation surgery is more popular nowadays. Its accuracy for screws placement, risk reduction of implant related and neurovascular complications have been well documented. 19 Undoubtedly, surgeons’ and scrubbed nurse experiences, together with the assistance from the operating technical staff are essential for a safe, effective and successful operation to be executed. 20,21 Konrad G et al. emphasized the importance of training and pointed out that the complication rate is actually dependent on the surgeon’s experience. 22,23 Therefore, steep learning curve is a major obstacle to be confronted. Other obstacles needed to be faced include the huge costs of machine, software incompatibility between generations and maintenance problems. However, judging from the current progress and the atmosphere of promoting imaging guided surgery, there is no doubt that navigation or 3D imaging technique will be a standard of care in the coming years.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.