
Abstract
Low energy peri-trochanteric fractures may happen in the presence of a retrograde nail in the femur. The management of these peri-implant fractures are very rarely reported. This is a series of seven cases from a level one trauma centre in Hong Kong. All fractures arose from low energy falls and were either inter-trochanteric or subtrochanteric. Removal of previous implants to allow cephalo-medullary fixation of the new fracture could be considered, but this is often difficult, time-consuming, and may inflict damage to the articular cartilage. Furthermore, this is not an option if the distal fracture is not yet well healed. Six of the seven fractures presented here were treated operatively with an extra-medullary device fixed to the proximal shaft with cerclage cables. The choice of fixation implants were based on the fracture type and available space above the proximal end of the retrograde nail. All seven fractures healed with no implant failure and major complications. There were no thirty-day and one-year mortality. A treatment algorithm is proposed for the management of these uncommon but difficult cases.
Keywords
Introduction
With the increased use of retrograde nails in the treatment of distal femoral fractures, peri-trochanteric fractures proximal to long retrograde femoral nails are not rare, but few cases had been reported in the literature. We present a case series of seven peri-implant fractures proximal to long retrograde femoral nails, six were treated with extra-medullary devices and one with removal and cephalo-medullary nailing.
Materials and methods
A retrospective, single centre case series study was conducted at a level one trauma centre. All consecutive patients treated for peri-implant femur fractures proximal to a long retrograde nail from December 2003–December 2019 were reviewed. Exclusion criteria were patients with multiple injuries, open fractures, pathological fracture and incomplete medical or radiological records.
A retrospective chart review was conducted, data collected include patients’ demographics, mobility, mechanism of injury, fracture pattern, operative data and clinical outcome. The fractures were classified according to the AO/Orthopaedic Trauma Association classification.
Results
Seven patients were identified. Patient demographics, data of the initial femur fracture, proximal peri-implant fractures, fixation device and outcome data were summarized in Table 1.
Patient demographics, previous femur fracture characteristics, proximal peri-implant fracture characteristics and outcome.
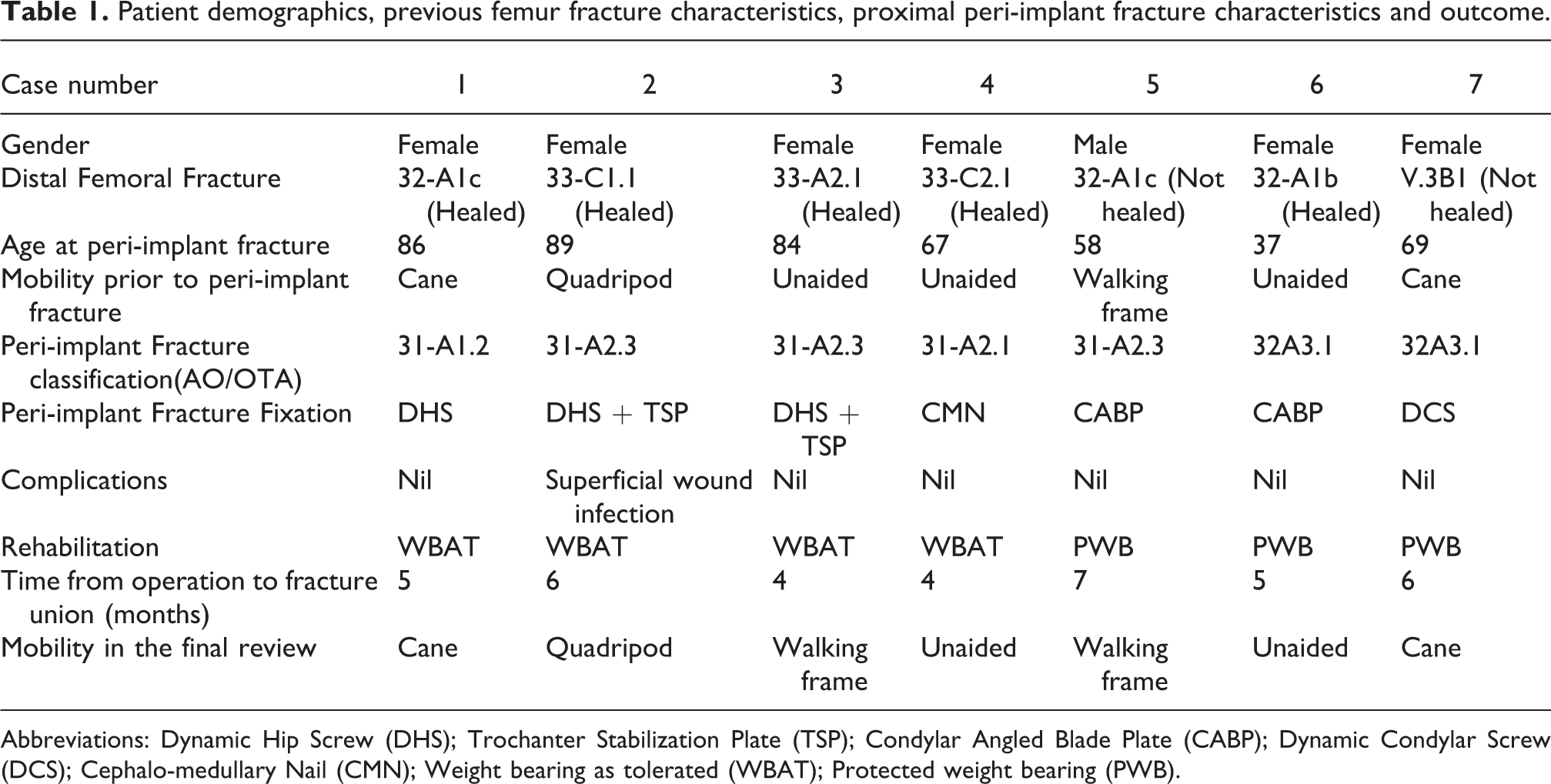
Abbreviations: Dynamic Hip Screw (DHS); Trochanter Stabilization Plate (TSP); Condylar Angled Blade Plate (CABP); Dynamic Condylar Screw (DCS); Cephalo-medullary Nail (CMN); Weight bearing as tolerated (WBAT); Protected weight bearing (PWB).
All seven patients had long retrograde nail fixation of a distal femoral fracture prior to the current peri-implant fracture at the upper end of the nail. All patients regained independent mobility after the previous retrograde nail fixation. The proximal peri-implant fractures occurred 3 months to 4 years after the previous fractures, all of them were inter-trochanteric or subtrochanteric closed fractures sustained after low energy falls.
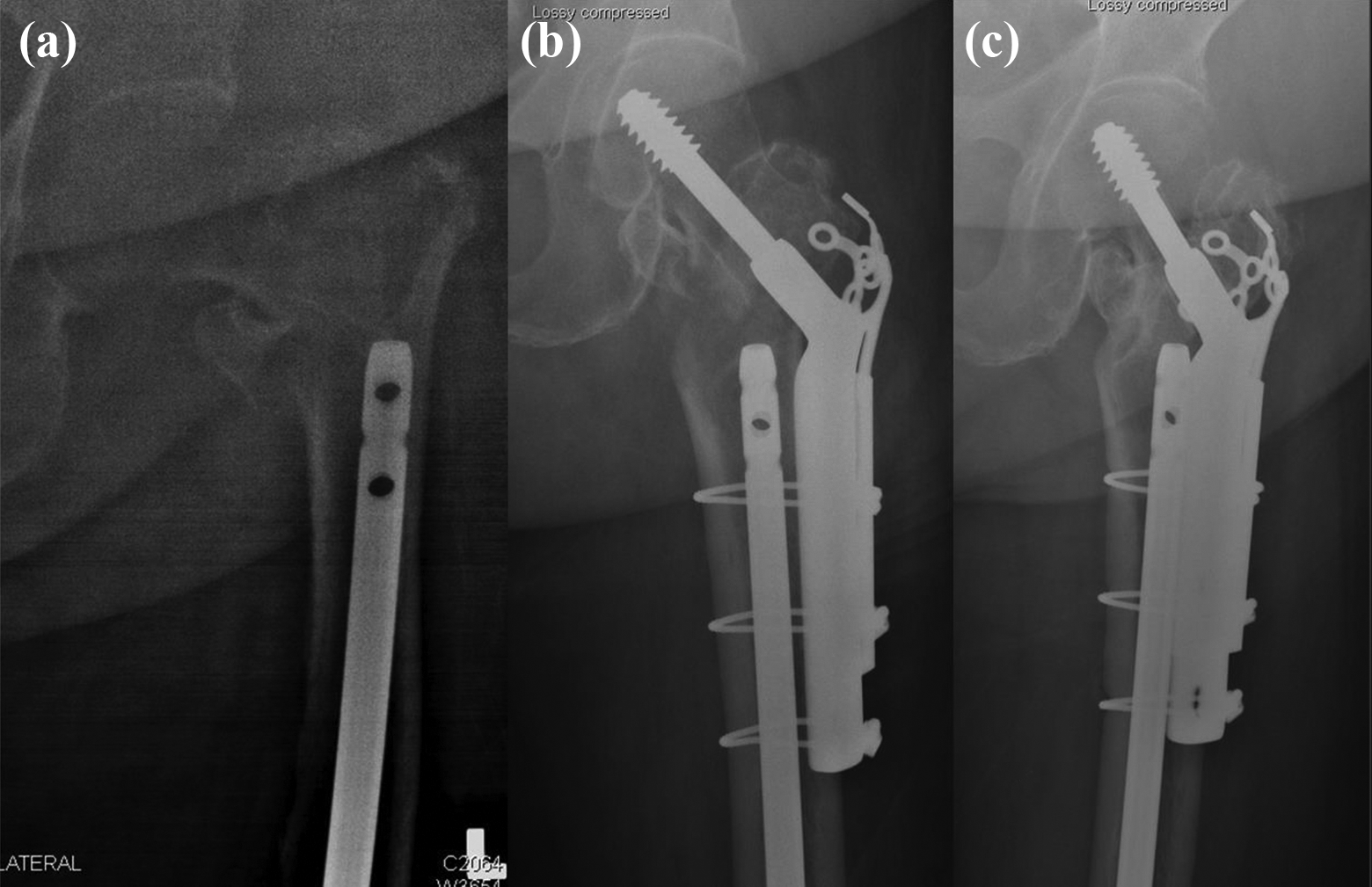
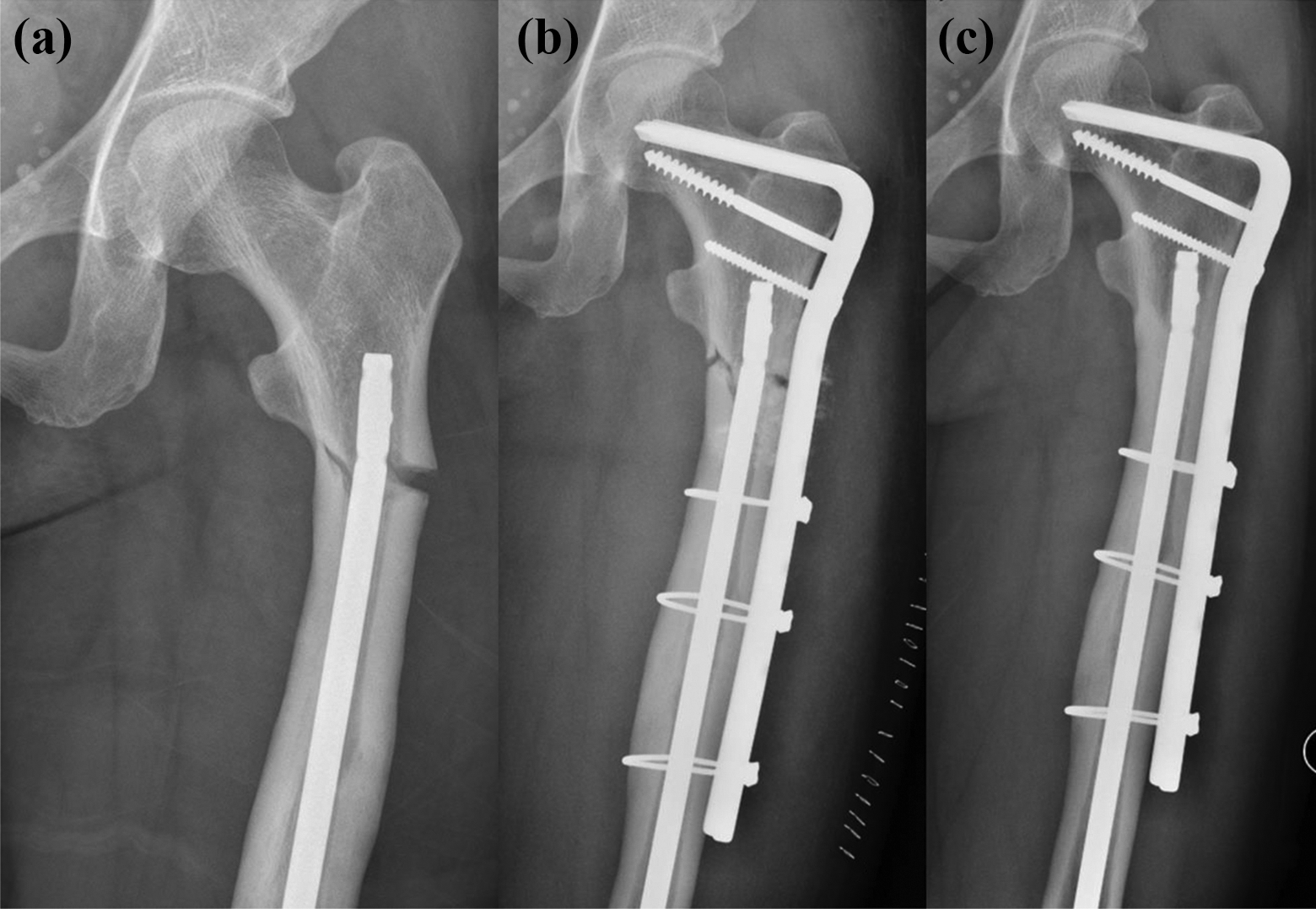
The choice of implant for fixation of the peri-implant fracture depended on the peri-implant fracture configuration, and the available space above the retrograde nail. Sliding Hip Screw (SHS) was the implant of choice in cases with inter-trochanteric fractures (Figure 1), with the addition of trochanter stabilization plate (TSP) for enhanced stability and to prevent excessive medialization of the femoral shaft in cases where the lateral wall was thin (Figures 2 and 3). If there was inadequate space above the proximal end of the retrograde nail to accommodate a SHS, removal of the retrograde nail should be considered in order to insert a cephalo-medullary nail (CMN) (Figure 4). In this case, removal of the retrograde nail took 2 hours. If removal and CMN fixation is contraindicated, a 95° device (Condylar Angled Blade Plate (CABP) or Dynamic Compression Screw (DCS)) would be used (Figure 5). For subtrochanteric fractures, the implant of choice would be a 95° device (CABP or DCS) (Figure 6 and 7).
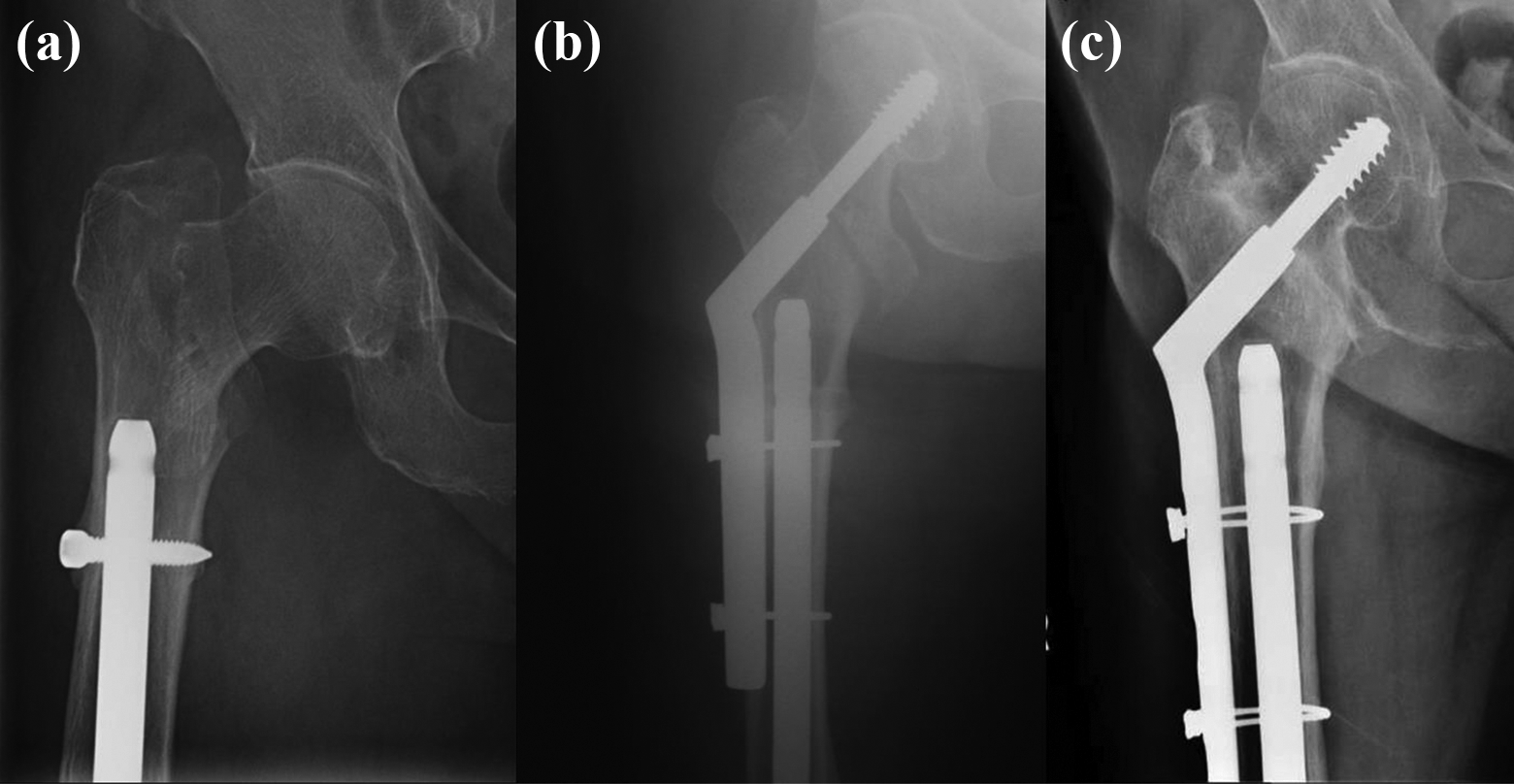
Case 1, female 86. Peri-implant inter-trochanteric fracture (a), fixation with DHS (b), and radiograph taken 3 years post-fixation (c).
Case 2, female 89. Inter-trochanteric peri-implant fracture with thin lateral wall (a), fixation with DHS + TSP (b), and radiograph taken 3 years post-fixation (c).
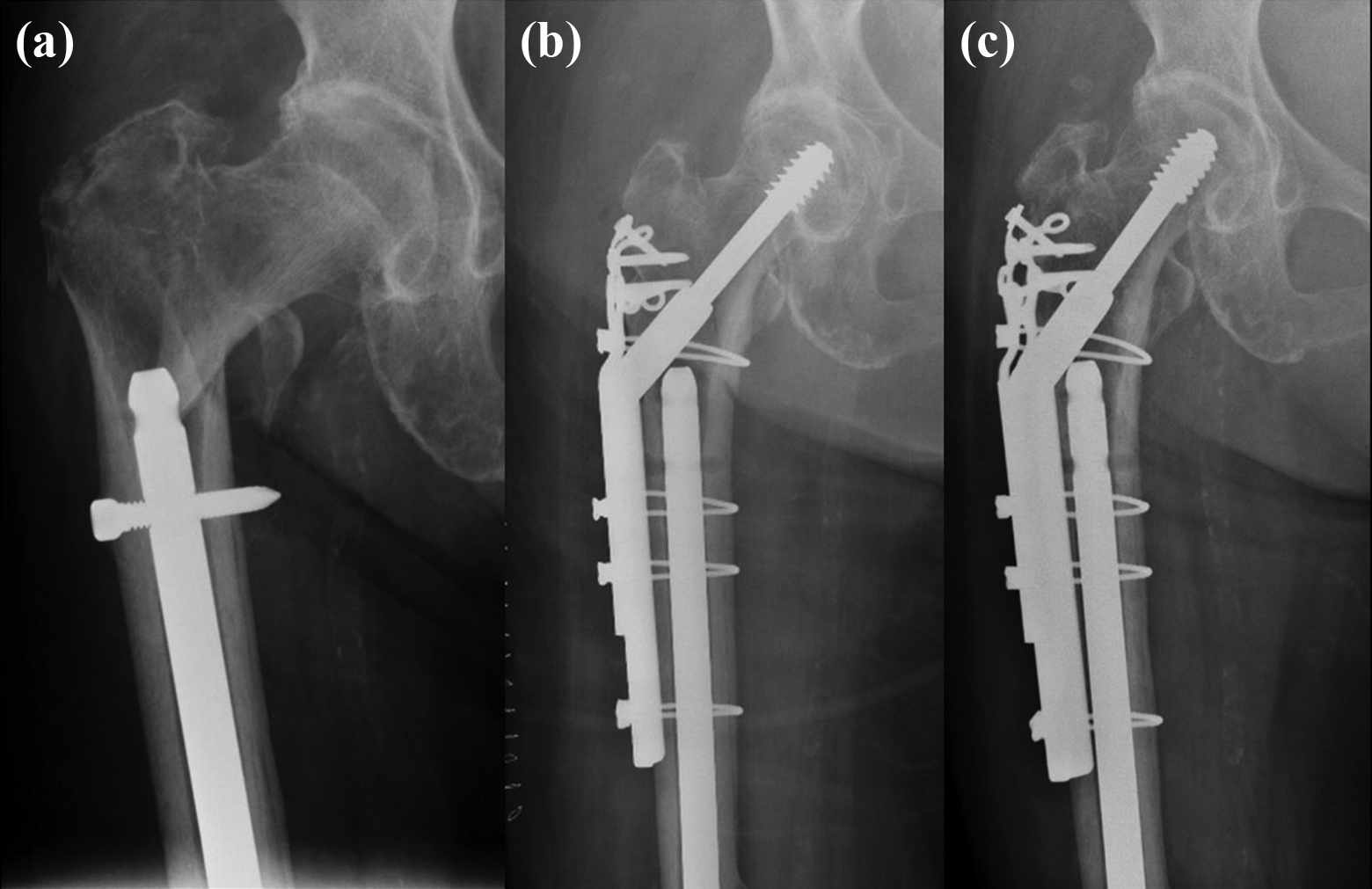
Case 3, female 84. Inter-trochanteric peri-implant fracture with thin lateral wall (a), fixation with DHS + TSP (b), radiograph taken 2 years post-fixation (c).
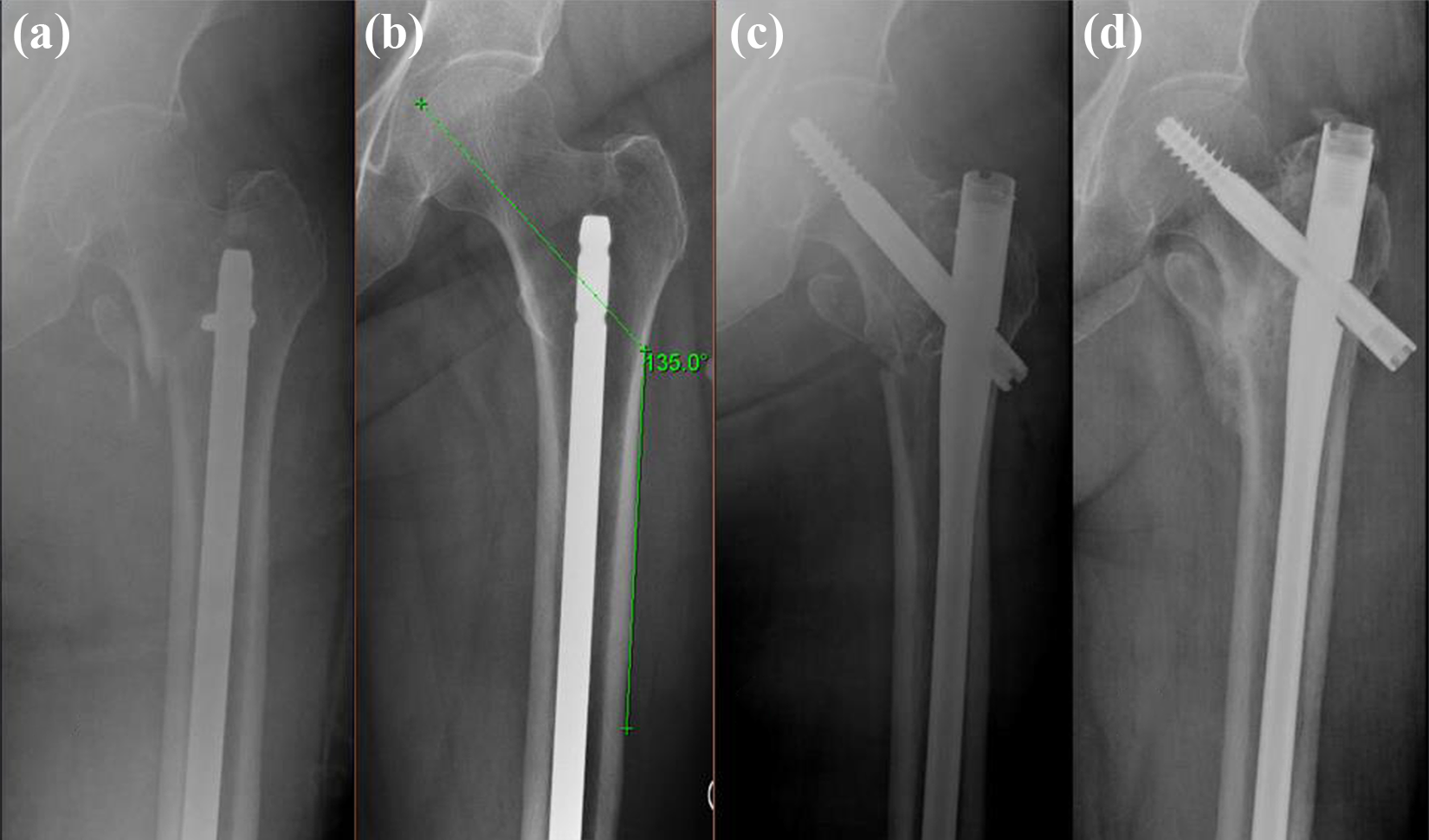
Case 4, female 67. Peri-implant inter-trochanteric fracture (a), pre-fracture radiograph showing inadequate space for a 135° device (b), removal of retrograde nail and insertion of long cephalo-medullary nail (c), and radiograph taken 4 months post-fixation (d).
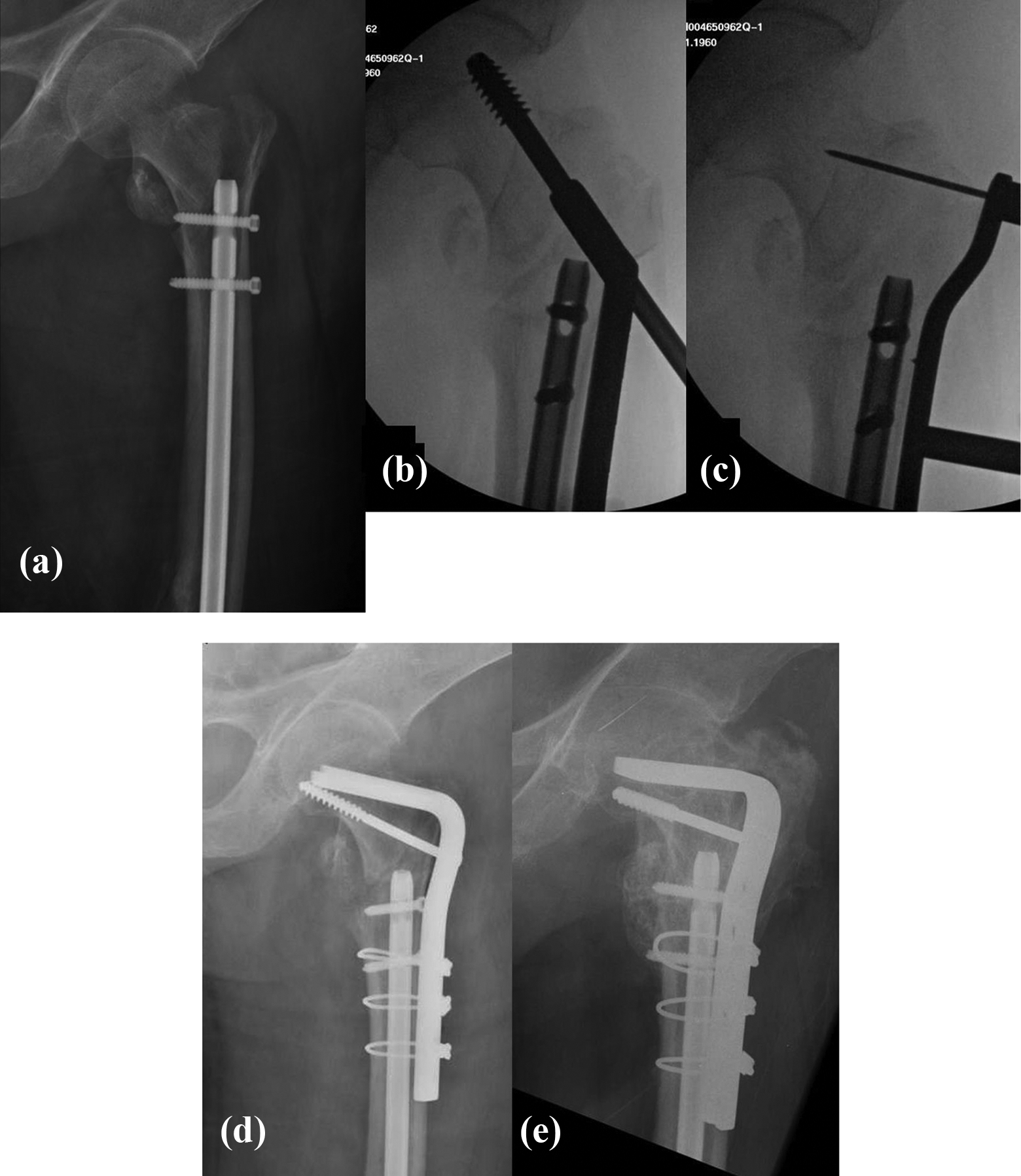
Case 5, male 58. Peri-implant inter-trochanteric fracture 4 months after retrograde nail fixation of a distal shaft fracture (a). After closed reduction, AP view with DHS overlapped (b), and 95° angle guide from DCS set overlapped (c). Fixation with 95° CABP (d) and radiograph taken 7 months post-fixation (e).
Case 6, female 37. Subtrochanteric peri-implant fracture (a), fixation with 95° CABP (b), and radiograph taken 6 years post-fixation (c).
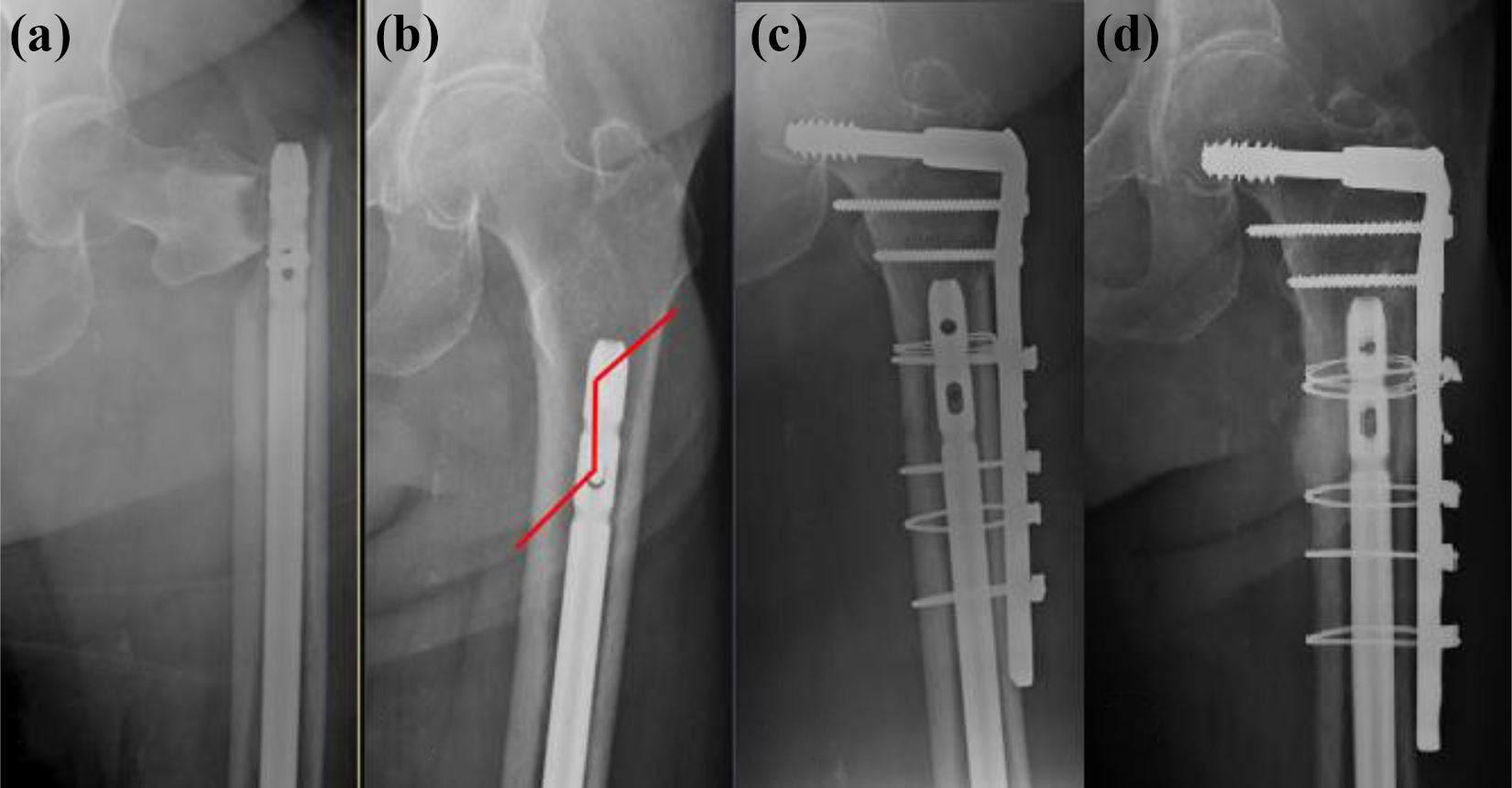
Case 7, female 69. Subtrochanteric peri-implant fracture 3 months after retrograde nail fixation of a distal femoral fracture (a), fracture line marked on pre-fracture film (b), fracture reduction utilizing cerclage wire loop and fixation with DCS (c), and radiograph taken 7 months post-fixation (d).
Fracture table was used in all cases to achieve closed reduction of the proximal femoral fracture. The hip was slightly abducted to relieve the pressure of the perineal pole onto the medial vascular structures. All extra-medullary fixation devices (SHS, TSP, DCS, CABP, Synthes) were introduced through a lateral approach to the proximal femur. Every effort was made to minimize stripping and devitalization throughout the operation. The devices were fixed to the proximal femoral shaft with multiple 2.0 mm cables from the Dall-Miles Recon and Trauma Cable System (Stryker). Cable passers were used carefully to minimize soft tissue stripping and prevent neurovascular injuries. Cables were not anchored to the screw holes with cerclage positioning pins.
All operations were targeted at achieving stable fixation. Immediate weight bearing was allowed in the geriatric patients, except in case 5 and 7 as they were segmental fractures. The young patient with subtrochanteric stress fracture (case 6) arising from a SMAD3 gene mutation was advised to have restricted weight bearing for 4 weeks.
All seven cases of proximal peri-implant fractures healed with no implant failure or major complications, thirty-day and one-year mortality. No cases required any subsequent operation after the index fixation of peri-implant fracture.
Discussion
Retrograde nailing is a proven method for fixation of distal femoral fractures. Commonly reported complications include malunion, nonunion and complications that occur around the knees. Other complications around proximal region of the nail include neurovascular injury and femoral fracture. There have been few reports on femoral fractures at the proximal ends of the retrograde nail. 1 –3 Mounasamy et al. 1 presented two cases treated with removal of the retrograde nail followed by antegrade CMN fixation. Among the case series of 60 peri-implant fractures published by Chan et al. 2 in 2018, there was only one such fracture. O’Mara et al. 3 reported one case treated with CABP. Apart from those, little had been said about the management of this difficult scenario. The current case series is the largest ever described.
As removal of a retrograde nail might risk damaging the articular cartilage in the knee, this should only be considered if the peri-implant fracture could not be adequately fixed with an extra-medullary device, or if there is a separate indication for removal of the retrograde nail such as nail protrusion into the knee. The authors propose a treatment algorithm as in Figure 8 based on the fracture type, the available space above the retrograde nail, and the condition of the previous fracture.
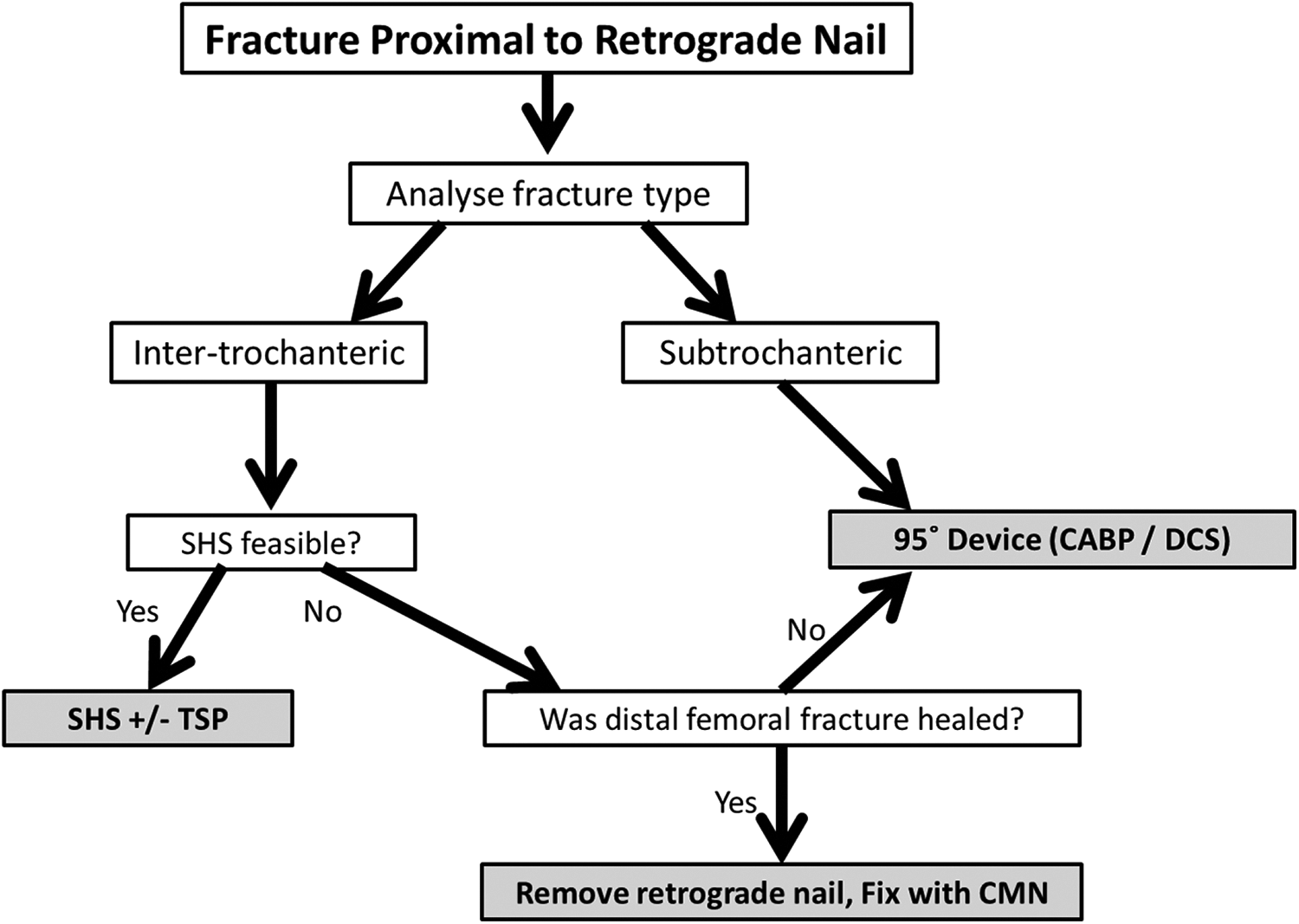
Algorithm for the management of peri-implant fractures proximal to a long retrograde femoral nail.
1. Fracture type
Inter-trochanteric fractures should preferably be managed with slidable devices (CMN or SHS), unless this is not feasible. Current literatures do not support routine removal of hardware. 4 The retrograde nail should be retained unless there are other indications for its removal, such as inadequate space for a 135° SHS. If a conversion to CMN is chosen, a long CMN reaching the femoral condyles would help prevent a subsequent peri-implant fracture down the shaft.
SHS remained the gold standard for fixation of stable (A1) inter-trochanteric fractures. A TSP should be added in those with thin lateral walls (A2) to prevent medialization of the distal fracture fragment and cut-out of the lag screw. 5
Non-comminuted subtrochanteric fractures are well managed with the use of 95° extra-medullary devices (CABP and DCS) 6,7 (case 6, 7), thus removal of retrograde nail does not offer much advantage, unless the nail blocks the proper positioning of the 95° device. The CABP has theoretical advantages over 95° DCS, 8 but the application of CABP could be technically more demanding than that of a DCS. The available surgical expertise should be taken into consideration when choosing between the two. For subtrochanteric fractures with medial cortical comminution, a careful balance must be made between an extra-medullary device and a CMN.
2. Available space above upper end of retrograde nail
Assessment is made on AP radiographs of the proximal femur taken before the peri-implant fracture to assess whether there is enough space above the retrograde nail for proper placement of SHS (for inter-trochanteric fractures) or 95° devices (for subtrochanteric fractures). 135° or 95° lines could be drawn on the AP image to visualize if a DHS or CABP could be comfortably accommodated (Figure 4(b)). In cases where a good pre-fracture AP radiograph is not available, similar assessment could be made on table after reduction of the fracture by placing the implant over the hip as a template for overlapped fluoroscopy (Figure 5(b) and 5(c)). If there is not enough space for the appropriate extra-medullary device, consideration is made as to whether removal of retrograde nail is preferred.
3. The condition of previous fracture
When there is insufficient space for the insertion of the desired extra-medullary device, healing status of the previous distal femoral fracture had to be assessed by both clinical (lack of pain on weight bearing and tenderness on palpation) and radiological (absence of visible fracture lines and gaps, sometimes bridging trabeculae lines, CT) features. The anatomical position of the previous distal femoral fracture needs to be taken into consideration as distal shaft fractures could be stabilized within the distal locking screws of the long CMN but not so in distal metaphyseal fractures. When healing status and anatomical position of the previous distal fracture are favourable, removal of retrograde nail per se could still risk damage to the knee articular cartilage. If the healing status and anatomical position are not favourable, another choice would be to replace the retrograde nail with a slightly shorter nail, combined with insertion of the desired extra-medullary device for the proximal fracture. The pros and cons of these alternative strategies must be carefully considered before a decision is made.
As the case series demonstrated, proximal peri-implant fractures proximal to a retrograde nail can be successfully treated without removal of the retrograde nail. The authors do not advocate routine removal of the retrograde nail unless the proper positioning of a SHS for fixation of an inter-trochanteric fracture was blocked by the upper end of the nail. Case 4 in the current series illustrates this scenario. Case 5 showed a scenario in which the distal fracture condition was not amenable to long CMN fixation, whereas the much preferred SHS was obstructed by the proximal end of the retrograde nail. A difficult decision had to be made between A. conversion to a shorter retrograde nail and use of SHS, and, B. use of 95° device which runs a higher risk of fixation failure in this inter-trochanteric fracture.
In the process of selecting an appropriate fixation device, analogy had been drawn from the management of inter-trochanteric and subtrochanteric fractures not complicated with the presence of a pre-existing intramedullary device. In the presence of pre-existing intramedullary device, the extra-medullary devices have to be fixed with cerclage cables or obliquely applied screws instead of bicortical screws. There is no biomechanical proof that the cables are working just as well, and there is no study showing the number and diameter of cables required to produce equivalent fixation strength. The authors had based on their past experience that two to three well applied and spaced-out 2 mm cerclage cables are simpler and more effective than several eccentrically applied bicortical screws or uni-cortical locking screws.
As in the management of most lower extremity fragility fractures, one should aim for stable fixation in order to allow early unrestricted weight bearing mobilization. 9
The authors believe that the treatment algorithm presented in Figure 8 can streamline the decision making in the management of this rare but complex proximal peri-implant fracture.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.