
Abstract
Bipolar hemiarthroplasty has been a well-established treatment for femoral neck fractures. We report a case of spontaneous dissociation of bipolar cup in a 68-year-old female with edge of the bipolar shell notched onto the femoral stem. Revision surgery to total hip arthroplasty was performed with acetabulum and bipolar cup component replaced and notched stem retained. While bipolar cup dissociation has been reported in case series, this associated notching from bipolar cup dissociation onto femoral stem has rarely been reported. We reviewed the current literature on dissociation of bipolar hip hemiarthroplasty regarding the pattern, risk factors, as well as its salvage options.
Introduction
Bipolar hemiarthroplasty has been a well-established treatment for femoral neck fractures. We report a case of spontaneous dissociation of bipolar cup in a 68-year-old female with edge of the bipolar shell notched onto the femoral stem. Revision surgery to total hip arthroplasty was performed with acetabulum and bipolar cup component replaced and notched stem retained. While bipolar cup dissociation has been reported in case series, 1 –3 this associated notching from bipolar cup dissociation onto femoral stem has rarely been reported. 4 We reviewed the current literature on dissociation of bipolar hip hemiarthroplasty regarding the pattern, risk factors, as well as salvage options. Although rare, surgeons should be aware of this possible prosthesis related complication, and formulate individualized treatment plan.
Case report
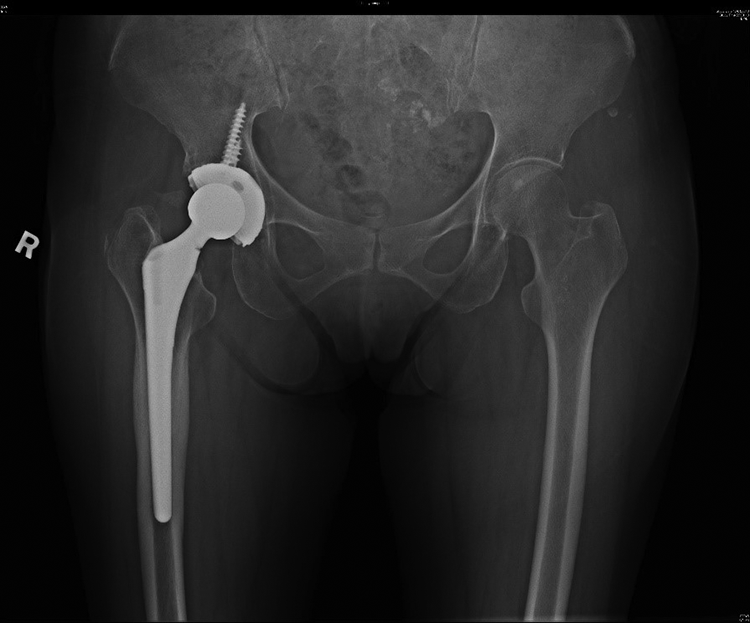
The patient is a 68-year-old woman with small body build. She has medical history of hypertension, impaired fasting glucose, depression and bronchiectasis. She suffered from a fracture neck of right femur after a fall. She was treated with bipolar hemiarthroplasty of right hip, using a cementless proximal coated size 6 Stryker Secur-Fit Max femoral stem with 39 mm DePuy Synthes self-centering bipolar cup. A 28 mm cobalt-chromium femoral head with 5 mm offset was implanted (Figure 1). The index surgery was uneventful, and she was symptom-free after the operation. She could walk unaided with exercise tolerance more than 1 hour.
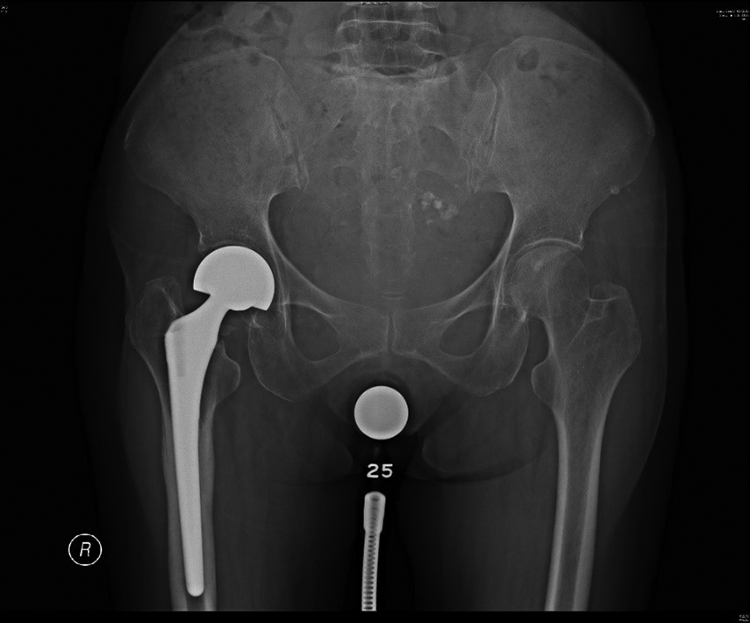
Plain radiograph of the pelvis after the index surgery, showing a bipolar hemiarthroplasty of the right hip.
However, she was admitted through the Accident and Emergency Department for one-month history of spontaneous right hip pain 5 years after the index surgery, at the age of 73. She complained of severe right hip pain upon hip flexion, which limited her hip range of movement and greatly reduced her mobility. There was no resting pain. She needed to walk with a stick due to right hip pain. She reported no history of trauma. She also had no fever or constitutional symptoms.
Physical examination showed no hip deformity or abnormal posturing. The right hip joint was non-tender on palpation. There were no erythema or warmth over the right leg. However, there was significant reduction in both active and passive range of movement of right hip flexion to 0–40 degrees only, compared to 0–130 degrees of the left hip. The lower limb pulses were strong, and distal limb movement was normal.
Plain radiograph of the pelvis and right hip showed a varus mal-positioning of the bipolar cup within the acetabulum, impinging onto the neck of the femoral stem (Figure 2). The femoral head was in an eccentric location within the bipolar cup. There was no sign of loosening of the femoral stem. Laboratory investigations showed normal white cell count, C-reactive protein and erythrocyte sedimentation rate.
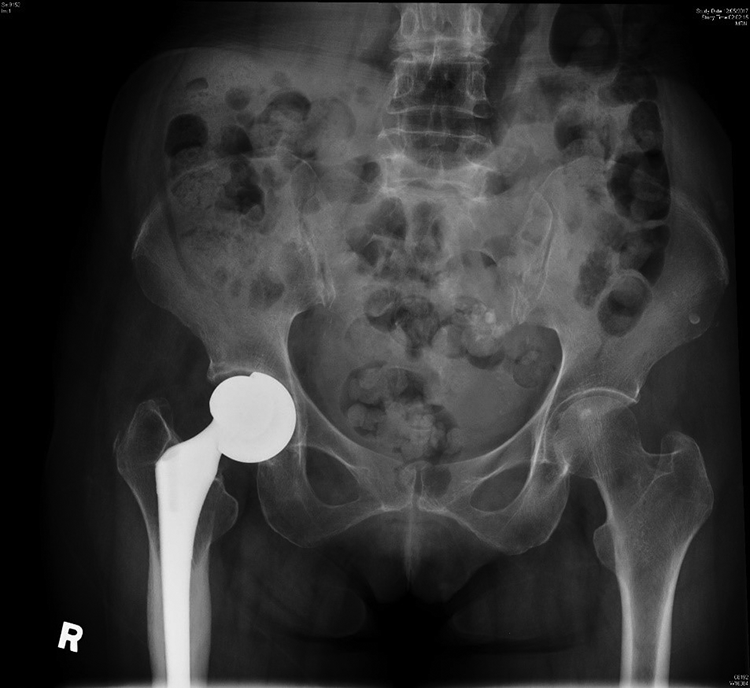
Plain radiograph of the pelvis 5 years after the index surgery, showing a varus aligned bipolar cup with an eccentrically located femoral head.
Revision total hip arthroplasty was scheduled. Intra-operatively, the bipolar locking ring was noted to dissociate from the polyethylene insert (Figure 3). The polyethylene insert was freely moving within the bipolar shell, allowing the bipolar shell to rotate into varus position and thus impinging onto the neck of the femoral stem. There was no macroscopic wear of the articulating surface of the polyethylene insert. Upon retrieval of the bipolar component, a notching over the postero-inferior aspect of the neck of the femoral stem was noted. It measured 2 mm deep and involved one-third of the femoral stem neck circumference (Figure 4). Metallosis in the right hip joint was evident. The femoral stem was well fixed without evidence of loosening. Revision surgery to total hip arthroplasty was performed with replacement of disassembled bipolar cup by a 44 m Stryker Trident acetabular shell with X3 highly crosslinked polyethylene insert. A new 28 mm cobalt-chromium femoral head with 5 mm offset was implanted. The notched femoral stem was well fixed thus was retained. Postoperatively, the patient was free of right hip pain. She regained mobility and was able to walk with a stick, with exercise tolerance of 1 hour. Latest plain radiograph at 3 years post-operatively showed well fixed femoral and acetabular components without progression of notching over femoral neck or catastrophic failure (Figure 5).
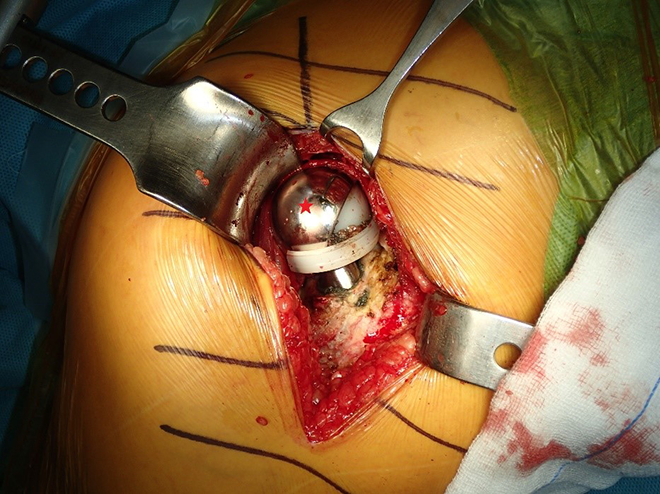
Intra-operative photo during revision surgery, showing the subluxed bipolar shell over the polyethylene insert and dislodged polyethylene locking ring (Asterisk: bipolar shell).
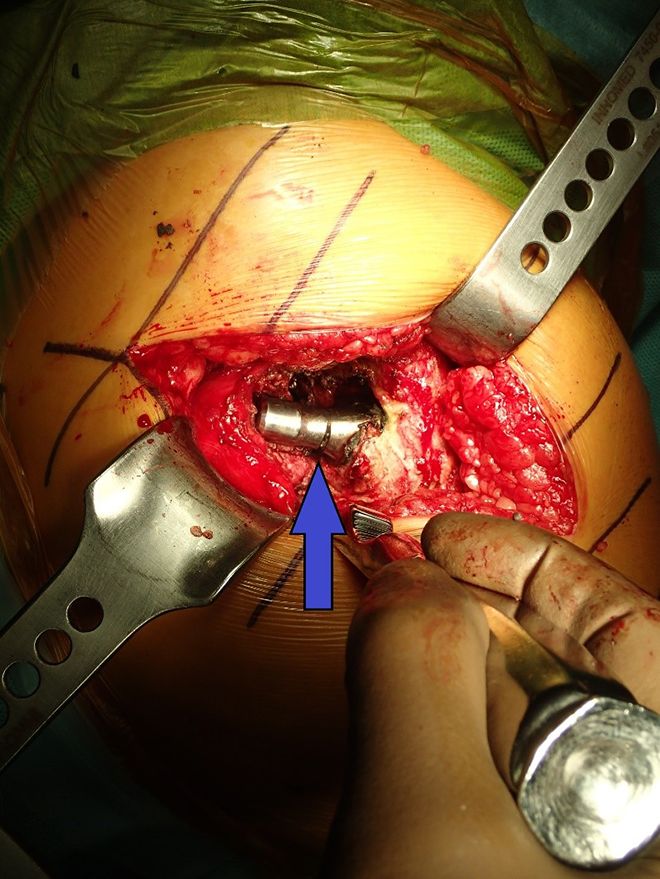
Intra-operative photo during revision surgery, showing the notched femoral stem neck after removal of the bipolar component (Arrow: notch).
Plain radiograph of the pelvis 3 years after revision surgery, showing static notch over inferior side of the femoral stem neck without progression or catastrophic failure.
Discussion
Since its development in the 1970s, bipolar hemiarthroplasty of the hip has been a well-established surgery for treatment of femoral neck fractures. Cup dissociation is a rare and unique complication after bipolar hip hemiarthroplasty. The higher modularity of the bipolar head contributes to this unique form of dislocation. Occurrence of cup dissociation is rare and mostly exists in case series. 1 –3 Dissociation can occur 4 days to 11 years from the initial surgery. 1 Reported modes of dissociation include traumatic or non-traumatic dislocation of the implant from acetabulum, following reduction maneuver, or spontaneously. 2 Breakage of the polyethylene locking ring leads to loosening of the outer cup, which in turn leads to failure of locking mechanism between the bipolar cups and subsequent dissociation. Three types of dissociation have been described, 3 which is classified based on the location of locking ring; type I: the locking ring loosened but femoral ball is not dislocated; type II: the locking ring loosened and inner femoral head dislocated; type III: inner femoral head dislocated but locking ring remains attached to the outer cup. Varus mal-position of the bipolar cup is also proposed to be a risk factor for early dissociation. Excessive stress over superolateral part of the polyethylene lining from varus mal-positioning might predispose dissociation of femoral head and bipolar cup. Femoral stem notching due to mal-positioned bipolar cup is also rare. In the literature, it is mostly due to polyethylene liner wear over time, leading to abnormal stress loading within the bipolar cup. 5 They present as overt femoral stem loosening due to extensive osteolysis. 4
Our reported case represents a type II non-traumatic spontaneous dissociation, 3 which occurred 5 years after the initial surgery. The cause of dissociation cannot be ascertained in our case, with no aforementioned risk factors identified. The orientation of the bipolar cup was not in varus in the post-operative plain radiograph (Figure 1). Excessive polyethylene insert wear was not evident upon retrieval of the bipolar component (Figure 6). Intraoperatively, the polyethylene locking ring was found dislodged from the insert, allowing dissociation of the bipolar shell from the polyethylene insert. The reason for the locking mechanism failure was uncertain. Bipolar cup with single locking mechanism was found to be a risk factor for dissociation upon closed reduction for bipolar hemiarthroplasty dislocation. 6 The DePuy Synthes self-centering bipolar cup comprises a single polyethylene locking mechanism. As a single unit, the polyethylene insert and the polyethylene locking ring was coupled onto the femoral head, followed by coupling of the bipolar shell onto the polyethylene insert. The locking ring expands to allow coupling with the femoral head. Further expansion was blocked after bipolar shell was coupled, thus the femoral head was secured within the polyethylene insert. Upon examination of the retrieved bipolar component, macroscopic defect or wear was not identified at the slots of the polyethylene insert and locking ring that contributing the locking mechanism. Also, no defect was noted at the peripheral groove of the locking ring that allows the secured coupling of the polyethylene and the bipolar shell (Figure 6). The patient has a small body build with retrieved native femoral head measured only 39 mm in the index operation. A combination of 39 mm bipolar cup and 28 mm femoral head resulted in thin polyethylene, which may weaken the locking mechanism allowing the in vivo dissociation. A mixed component from different manufacturers was used in our case, which may contribute to the failure. We decided to implant a mixed component from different manufacturers as 39 mm bipolar cup was not available from the same manufacturer. Although there is no difference in revision rate comparing mixed and non-mixed components in total hip arthroplasty from a national arthroplasty registry, 7 similar large-scale study on bipolar hemiarthroplasty was lacking. A report of four cases of mixed components of bipolar hip hemiarthroplasty causing failure was due to different design of femoral head. 8 A retrieval analysis of the failure bipolar locking ring may be helpful to delineate the cause of failure.

Retrieved bipolar component and femoral head. From left to right: bipolar shell, polyethylene insert, polyethylene locking ring, femoral head. No defect or wear was found at the slots and groove of the polyethylene that contributed to the locking mechanism. No macroscopic wear was found at the articulating surface of the polyethylene insert.
Notching at postero-inferior neck of the femoral stem was noted intra-operatively. This was caused by scratching of the edge of the bipolar shell onto the prosthesis neck. This phenomenon is rare but has been reported. 4 With a notched femoral stem, most surgeons recommended a femoral stem revision to avoid subsequent prosthesis fracture and catastrophic failure, especially when it was associated with stem loosening. 6 However, it is possible to retain a notched femoral stem with good long term survival. 9 In the current case, the cementless femoral stem was well fixed and showed no evidence of loosening. A femoral stem revision would involve an extensile approach with potential devastating complications. Although defect at femoral stem might lead to stress riser and premature failure, 10 electron microscopy studies of fractured femoral stems demonstrates stem fracture progression from tensile anterolateral part of the stem toward posteromedial direction. 10 In our case, the notch was over postero-inferior aspect of the femoral stem neck at the compression side. Thus, we decided against revision of the femoral stem at the time of revision surgery, though this decision would be debatable. Over 3 years of follow up, the notching remained static and showed no propagation and no catastrophic failure. We postulated that the notch over inferior femoral neck is intrinsically more stability when compared with notch over superior neck, and hence less chance of propagation. A formal biomechanical study on the risk of propagation of defect in the prosthesis with regards to locations of defect would be favorable. We will continue close monitoring of any complication related to the notching in our patient.
Conclusion
Cup dissociation is an unusual and unique complication after hemiarthroplasty of the hip. While risk factors and types of dissociation has been suggested, exact mechanisms of dissociation are not well understood. Retention of a notched but well fixed femoral stem could be a viable option during revision surgery to avoid extensive stem revision. It is advisable to have regular radiographic monitoring for patients underwent arthroplasty, to detect and treat early complications, and avoid inevitable progression and catastrophic failure.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was obtained from the patient for publication of patient information and images.