
Abstract
Introduction:
As the geriatric population increases, the incidence of intertrochanteric fractures (ITF) has also increased significantly. There are various modalities to treat these fractures. In this study our aim is to analyse outcomes of Proximal Femoral Nail (PFN) in comparison to those of Dynamic Hip Screw (DHS) for the treatment of ITF.
Materials and Methods:
This study was carried out during 2017–20. 150 patients of unstable ITF (AO type 31-A2, 31-A3) in elderly were randomly divided into two groups of 75 each and were treated either by DHS or PFN and were followed up regularly.
Results:
The results were compared between the groups and statistical analyses were performed. The results were assessed with Harris Hip Score(HHS) & Parker Palmer mobility score (PPMS) which were better in PFN group.
Conclusion:
PFN is a better fixation device for unstable ITF (31 A2 and 31 A3) in elderly patients.
Keywords
Introduction
With the growing geriatric population, the intertrochanteric fractures are on rise. About 50% of these fractures are unstable. 1 –3 Poor bone quality with complex fracture pattern makes these fractures challenging to treat. The greatest challenges for treatment of these fractures are instability and osteoporosis, and the complications of fixation that may arise from them. The goal of surgery in such type of fracture is to provide a stable construct to restore early mobility while decreasing the risk of complications associated with long term recumbency and restoring the patient to preoperative status. Both DHS and PFN have shown good result in such complex situations. The risk of implant failure is lessened in DHS with fixed angle locking side plate and is valuable in unstable fracture with osteoporosis. 4
PFN provides a more biomechanically stable construct by reducing the distance between hip joint and implant. 5 –7 PFN prevents lateral translation of the proximal fragment and its intramedullary location at the junction between the nail and lag screw resist the bending force and thus, allows early weight bearing in unstable ITF. 7 –9 But PFN remains comparatively more costly than DHS. The results of review of literatures shows no significant advantage of PFN over DHS in terms of complications and functional outcomes. 10,11 In spite of several benefits of PFN, it is associated with technical failures. 12 –14
This prospective randomized study was designed to look for the outcome of PFN or DHS in unstable intertrochanteric fracture.
Materials and methods
A prospective randomized controlled study was conducted at our level I trauma centre between September 2017 and January 2020 to evaluate the surgical outcome of unstable intertrochanteric fracture. A total of 202 patients with age more than 50 years with unstable ITF (AO type 31-A2, 31-A3) were enrolled in our study. Out of the 202 patients enrolled for our study, 27 patients were unfit for surgery and 25 cases were lost to follow up. A total of 150 patients were evaluated (Figure 1). Pathological fracture or compound fractures were excluded from our study. The patients were assigned to one of the two treatment groups based on a computer generated randomization table with Group A patients (n = 75) were treated with PFN and Group B with DHS (n = 75). Institutional Ethical Clearance was obtained before patient recruitment. All patients gave written consent to be included in the study.
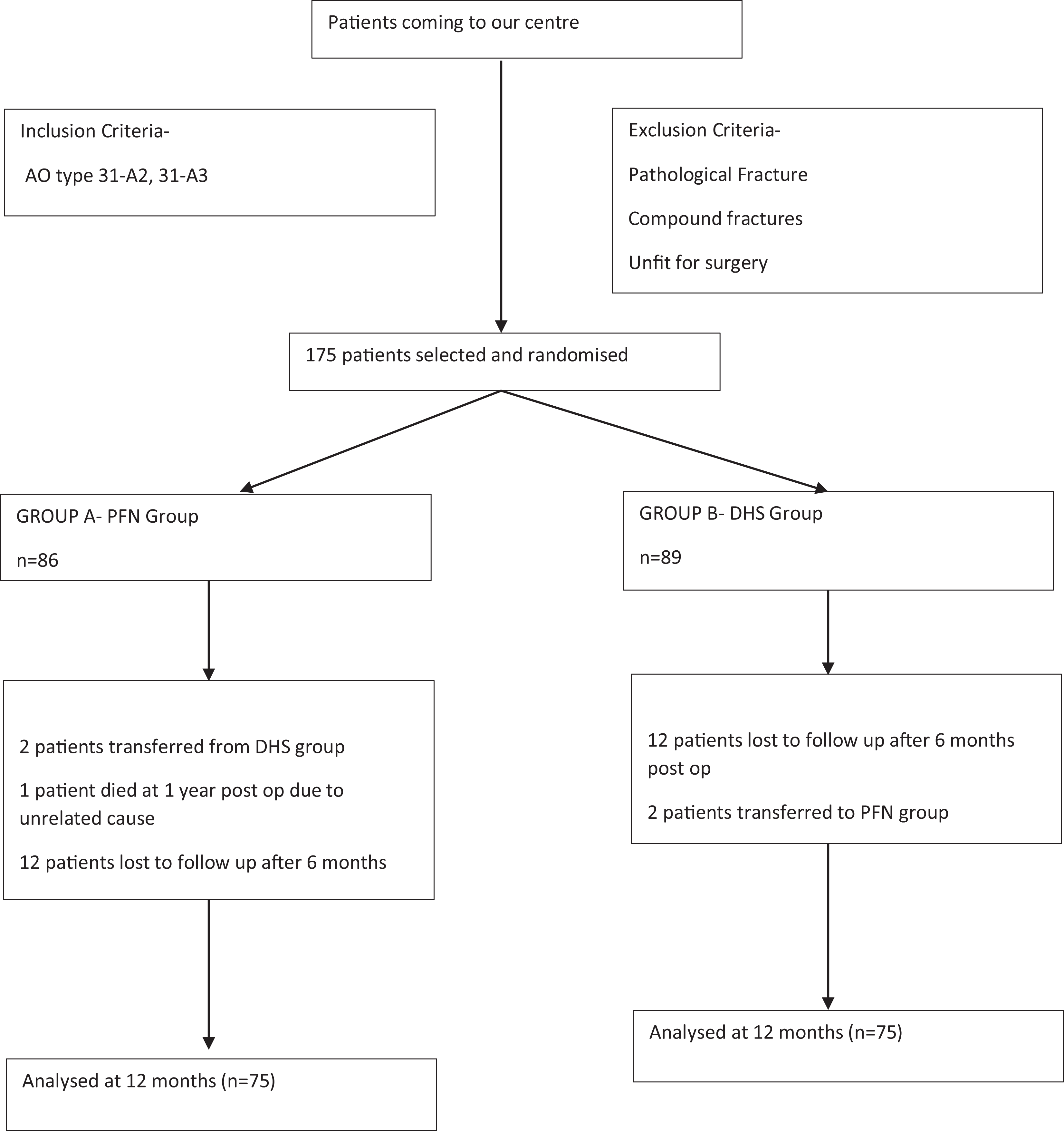
Flowchart demonstrating the inclusion, exclusion criteria along with details of loss of follow up.
The demographic details, radiographs and functional assessment (walking ability grades described by Sahlstrand) at 3 month, 6 month, 1 year and 2-year follow up was collected. All surgeries were performed by the same orthopaedic surgeon under regional anaesthesia after patient was fit for surgery. The patient was placed on a traction table and the fracture was reduced by closed manipulation under image intensifier. The length of compression screw for DHS was measured from Antero Posterior view radiograph by subtracting magnification. The neck-shaft angle and length of side plate were measured using Antero Posterior view radiographs of the unaffected side. The diameter for PFN were measured from diameter of the femur at the level of isthmus. The neck-shaft angle for PFN were measured on the unaffected side on AP X-ray. A standard length PFN (250 mm) was used in all our cases. The average blood loss was calculated using method by Brecher et al. 15
Post-operative rehabilitation protocol was uniform. Isometric quadriceps exercise, knee bending, sitting by side of bed and abductor strengthening exercise were advised immediately after surgery. Non-weight bearing/Toe touch walking (NWB/TTW) was allowed with help of the walker/axillary crutches from the second/third post-operative day depending upon general condition and pain tolerance of the patient. The patients were discharged 5–7 days following surgery with instruction to walk NWB/TTW with help of walker/axillary crutches. The patients were followed up at 6 weeks, 3 months, 6 months, 1 year and at 2 years. Fracture union, malunion and functional ability [Harris Hip Score, Parker and Palmer Mobility Score (PPMS), Visual Analogue Scale (VAS)] were evaluated at each follow up. Radiologically, the presence of at least three of the four cortices with bridging callus formation and crossing trabeculae in AP and lateral radiographs were considered as osseous healing. Malunion was considered when varus angulation was greater than 10 degrees.
The results were compared between the groups. The statistical analyses were performed using SPSS 20 (SPSS, Inc., IL). P values were calculated with independent samples t-test and with cross-tabulation using Student t-test; values of p < 0.0001 were considered as significant.
Results
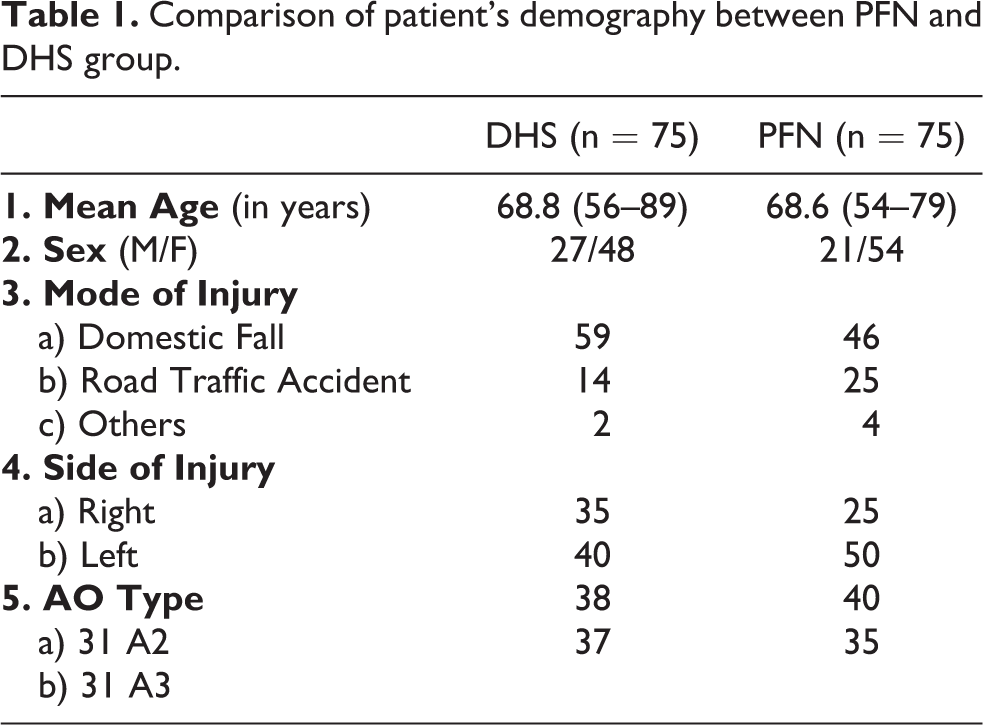
The mean age of the patients was 68.8 years (range 54 to 89 years). The average delay of surgery was 3.2 days (range 2 to 8 days). In PFN group there were 54 females and 21 males, while in DHS group there were 48 females and 27 males. In total, 78 were 31-A2 (DHS-38, PFN-40) and 72 were 31-A3 (DHS-37, PFN-35). Ninety (60%) patients had fractures on the left side. The Singh’s index for osteoporosis showed 88 (58.67%) patients were grade 4 and above. 105 (70%) fractures were due to domestic fall, 39 (26%) were due to road traffic accident and 6 (4%) fractures were of other etiology. The preoperative and perioperative comparison are presented in Table 1 and Table 2. Closed reduction was achieved in all cases in both groups except two cases in PFN and 4 cases in DHS group where open reduction was carried out. Patients treated with PFN required an average 6.64 cm shorter incision than DHS (p < 0.0001). Fluoroscopy time for DHS group was significantly less as compared to PFN group (p < 0.0001). The mean duration of surgery was significantly shorter for the PFN as compared to DHS (p value <0.0001). Duration of surgery in DHS group was almost same for each AO type but in PFN group it increased with the instability from A2 to A3 type fractures.
Comparison of patient’s demography between PFN and DHS group.
Perioperative comparison between PFN and DHS groups.
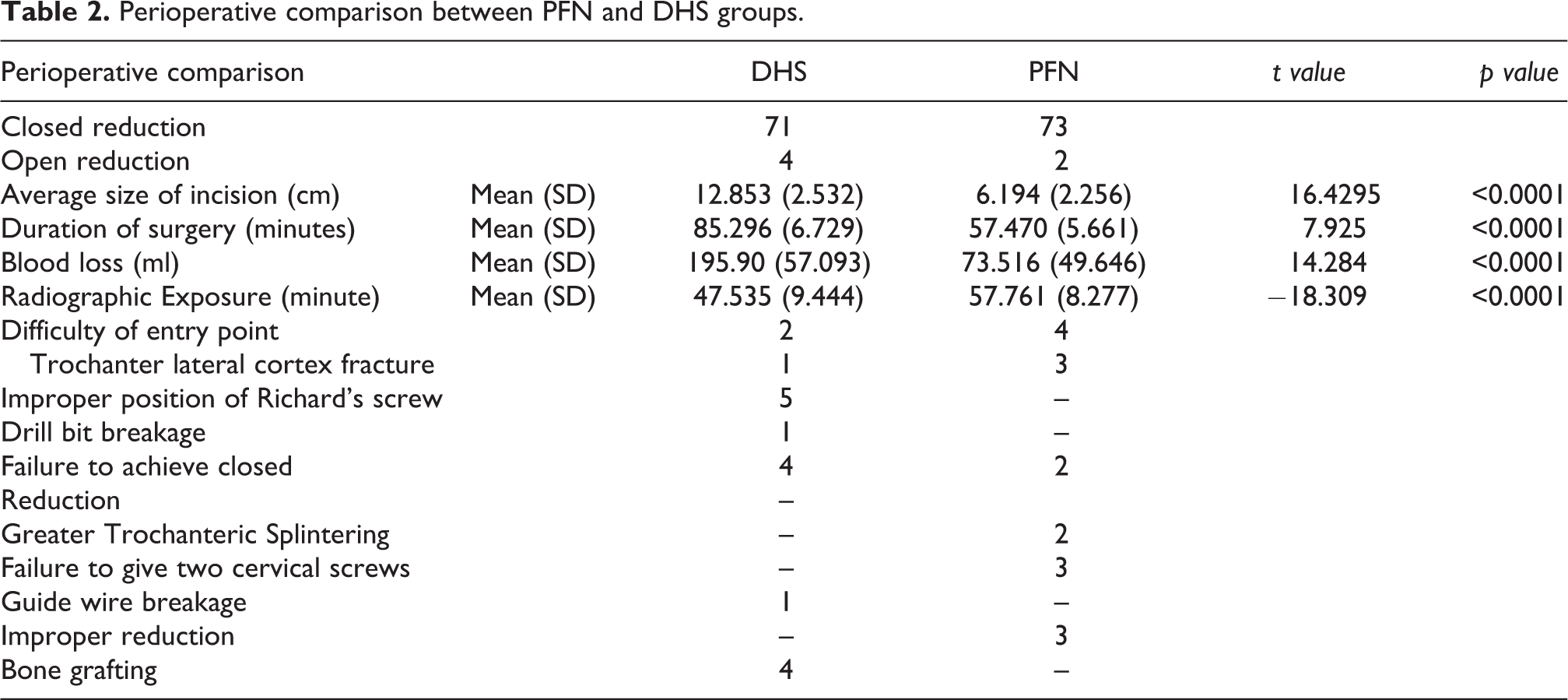
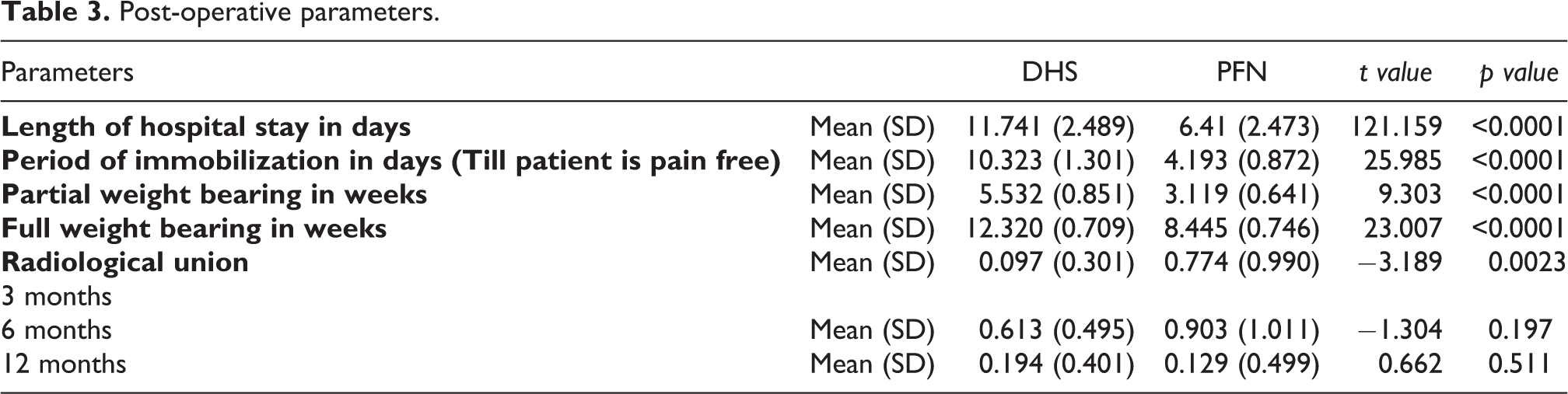
The average blood loss in the PFN group was 74 ml and in the DHS group was 195 ml (p value <0.0001). Intraoperative blood loss was greater in A3 as compared to A2 type unstable fractures. Blood transfusion was essential in 11 of 75 DHS patients, either intra or post-operatively, but PFN patients needed no blood transfusion. There were two preoperative and two iatrogenic fracture of lateral cortex which was augmented either with a cerclage wire or an additional screw. We failed to put hip screw in three cases as it could not be accommodated in the neck after putting neck screw. There was one guide wire cut during reaming and one case of drill bit breakage in DHS group. The greater trochanter splintering was encountered in two patients in PFN group which united well without complication. Location of entry point was difficult in four obese patient treated with PFN and two in the DHS group due to proximity of fracture near the entry point. Improper placement of Richard’s Screw was found in five cases. Entry point was difficult in two reverse oblique fractures as the fracture line extended to the screw entry site and we had to switch to PFN, these patients were considered with PFN group. Post-operative parameters are presented in Table 3. Average duration of stay in hospital was 6.5 days for PFN (5–10 days) and 11.8 days (8–15 days) for DHS (p value <0.0001). Period of immobilization till the patient is pain free was significantly less in PFN group. The mean PWB from the day of surgery was 5.52 weeks in DHS and 3.12 weeks in PFN group (p value <0.0001) and the mean FWB was 12.32 weeks in DHS and 8.45 weeks in PFN (p value <0.0001). At the end of 12th to 14th week all patients in either group were found bearing full weight with the help of walker/crutches. There was no significant statistical difference found between two groups while walking without support at 16th, 20th and 24th weeks (p value 0.437, 0.681 and 1.000 respectively). Radiological outcome were assessed at 3, 6 and 12 month post-operatively (Figures 2 and 3).
Post-operative parameters.
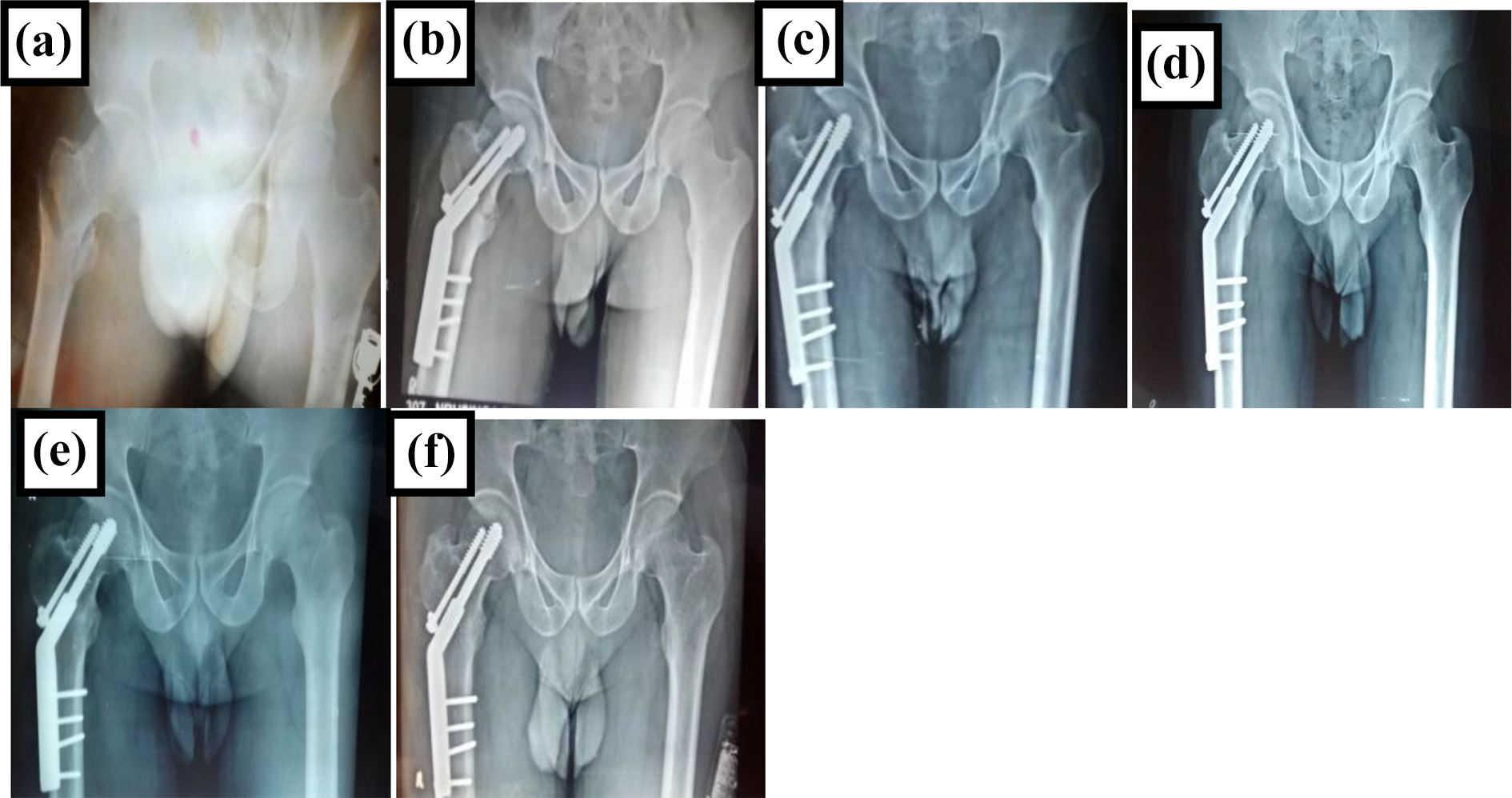
Radiographs of a case treated with DHS: A. Preoperative Trochanteric fracture; B. 4 weeks post-op; C. 8 weeks post-op; D. 12 weeks post-op; E. 6 months; F. 1 year.
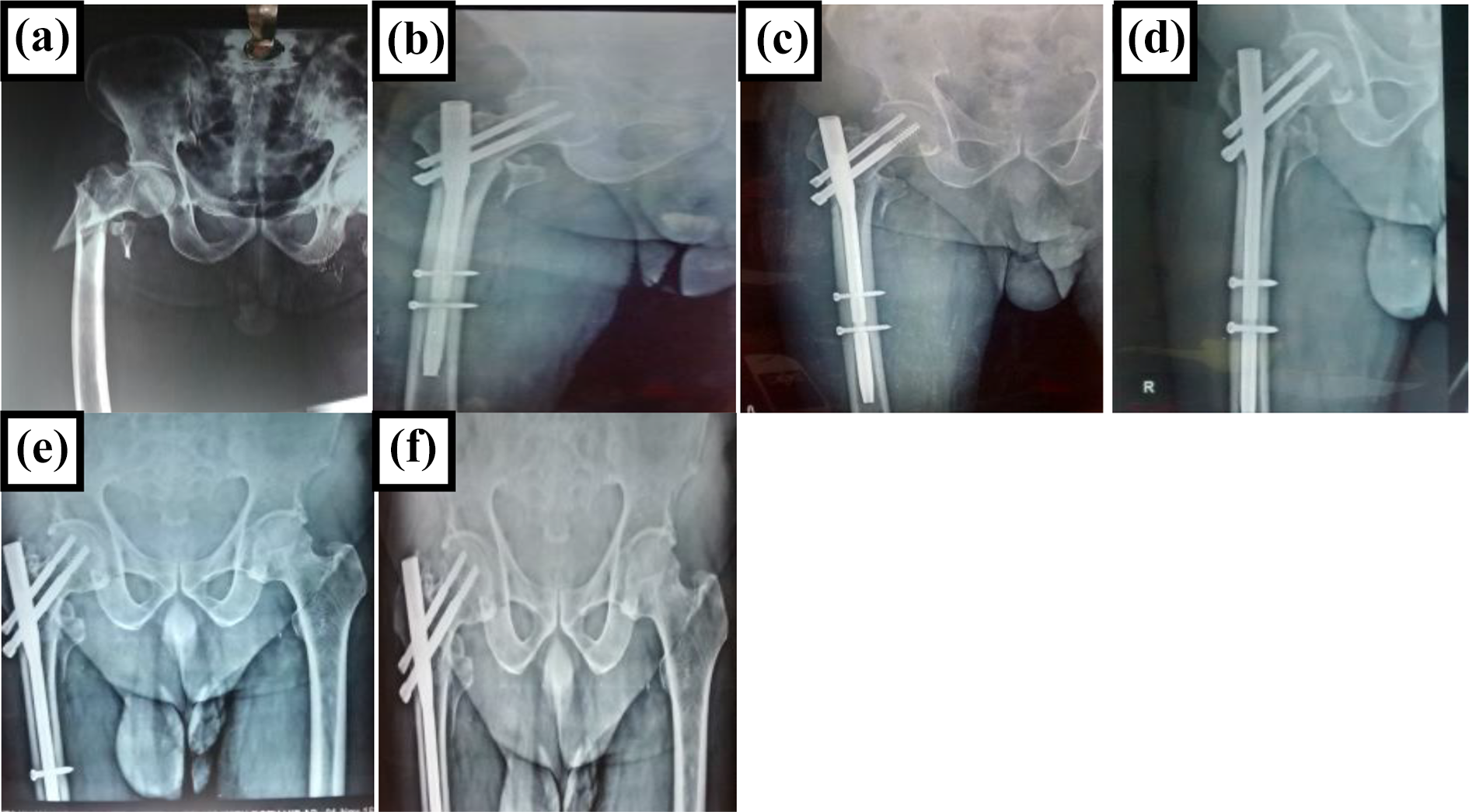
PFN: Radiographs of a case treated with A. Preoperative Trochanteric fracture; B. 4 weeks post-op; C. 8 weeks post-op; D. 12 weeks post-op; E. 6 months; F. 1 year.
In our study the mean radiological union at the end of 3 months in DHS was 0.097 and 0.774 in PFN (p < 0.0001). However, the p value was insignificant at 6 and 12 months. In the PFN group, patients had a better fracture union. At 12 months post-operatively, all patients in the DHS and PFN groups had complete union of the fracture site with eight patients in DHS group continued to unite in varus deformity, which did not progress. A significant difference was found in the post-operative pain in the two groups with 13 (14.3%) cases in the DHS group were pain free (VAS-0) at the 3 months of follow up as compared to 44 (58.7%) in the PFN group, which increased to 40 (53.3%) in DHS group as compared to 62 (82.7%) cases in PFN group at the end of 6 months. There was severe pain (VAS ≥ 6) in 6 (8%) of cases in the DHS as compared to 1 (1 .3%) in PFN group. Complications encountered post-operatively are summarized in Table 4, Table 5 and Figure 4. There were five cases of superficial and one deep infection in the
Complications.
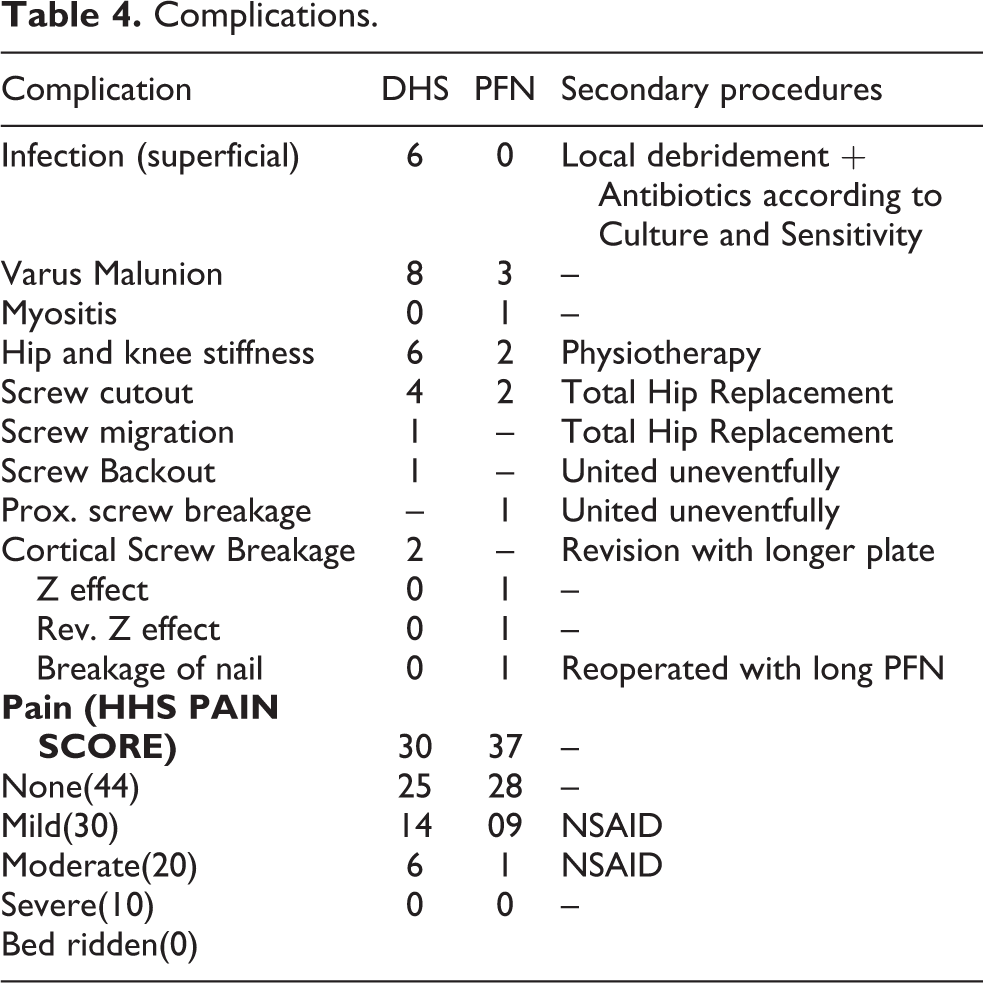
Complications.

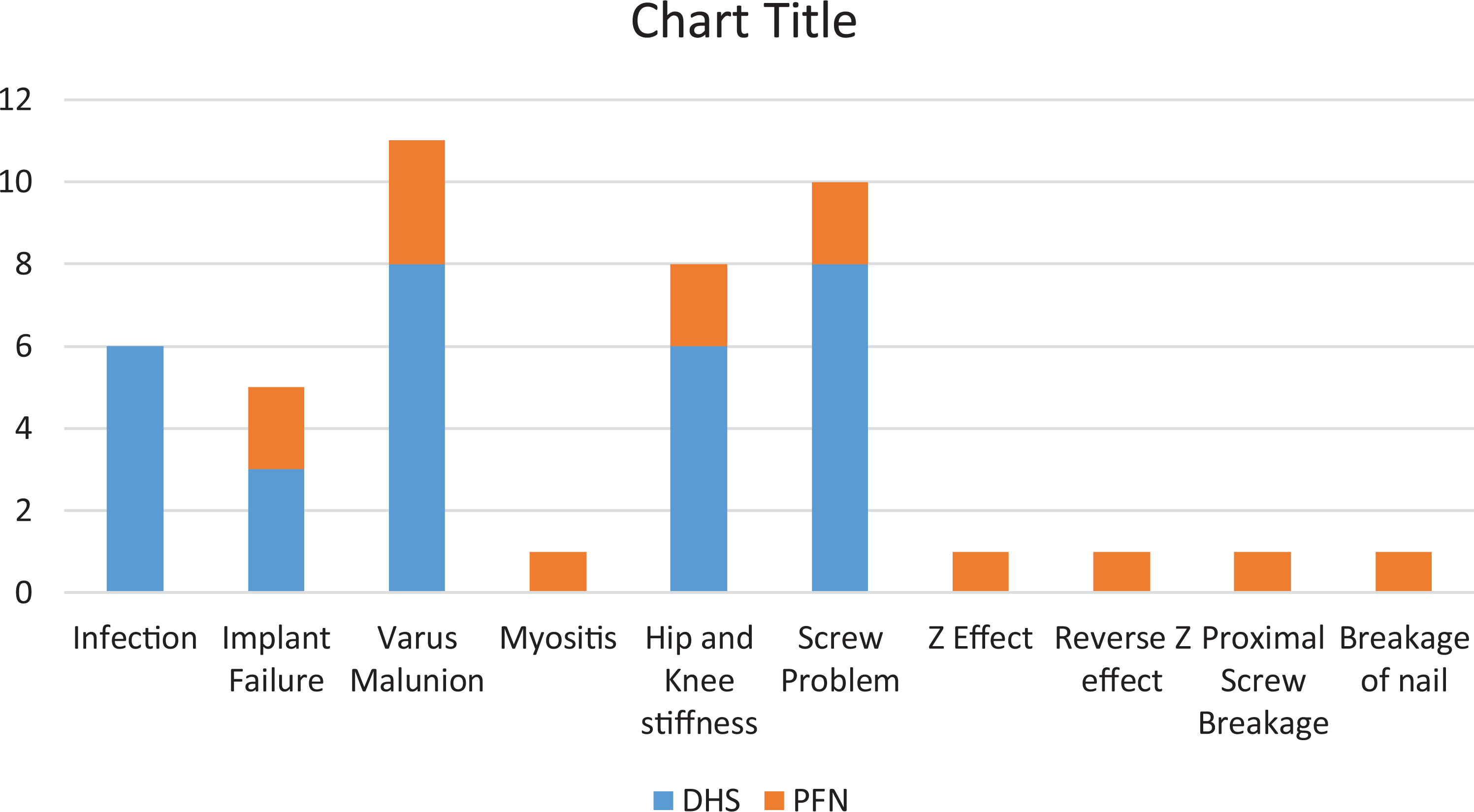
Complications
DHS group which was treated by local debridement and antibiotics as per culture and sensitivity. No implant was removed due to infection. We didn’t encounter any infection in PFN group. There was an average of 8.70 mm of shortening of the femoral neck in the DHS group as compared to 3.41 mm in the PFN group at the end of 1 year (p < 0.0001).The average femoral shortening in the DHS group was 9.961 mm as compared to 5.901 mm in the PFN group (p value 0.0001). Femoral neck-shaft angle difference as compared to opposite side was 14.610 in DHS group and 8.810 in PFN group (p value <0.0001).In PFN group we had one Z-deformity, one reverse Z-deformity and one case of screw breakage. One patient had stem breakage after fall for which revision was done with long PFN. Two patients have screw cut out (Figures 5 and 6). We had one case of myositis and three cases of varus malunion of 125° to 130° in PFN group. In the DHS group we encountered four hip screw cut outs, one screw migration, one screw back out and two cases of cortical screw breakage/pull-out (Figure 7). Total hip replacement was done in four screw cut out/migration cases (Figure 8). Longer locking plate was used in two cortical screw breakage/pull-out cases while retaining the Richard’s screw and were followed up till union (5 months post-operatively).
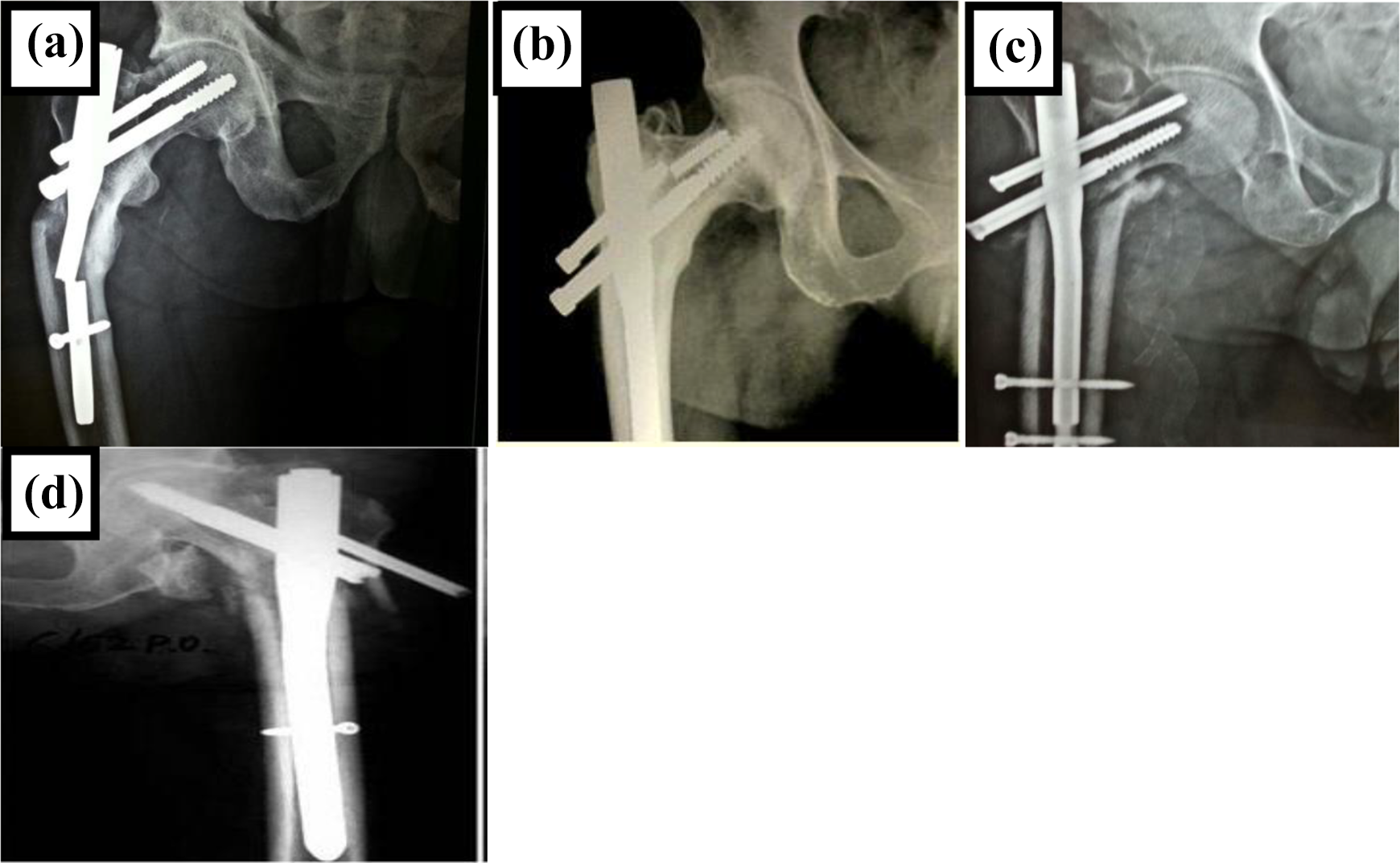
Complications seen in patients treated with PFN: A. Broken implant in OTA 31-A3 B. Broken hips screw in OTA 31-A2 C. Z effect in OTA 31-A2 D. Reverse Z effect in OTA 31-A3.
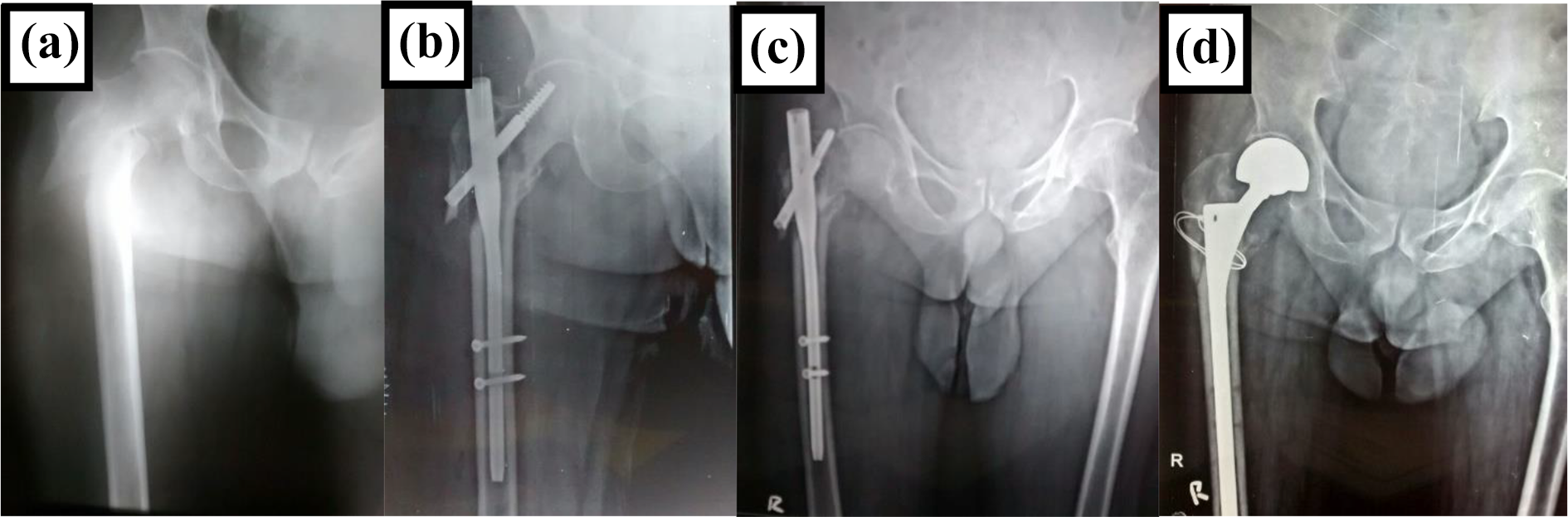
Radiographs of Failed PFN converted to Bipolar Hemiarthroplasty. A. Preoperative Radiograph B. Immediate Post-operative C. Shows Screw cut out. D. Conversion to Bipolar Hemiarthroplasty.
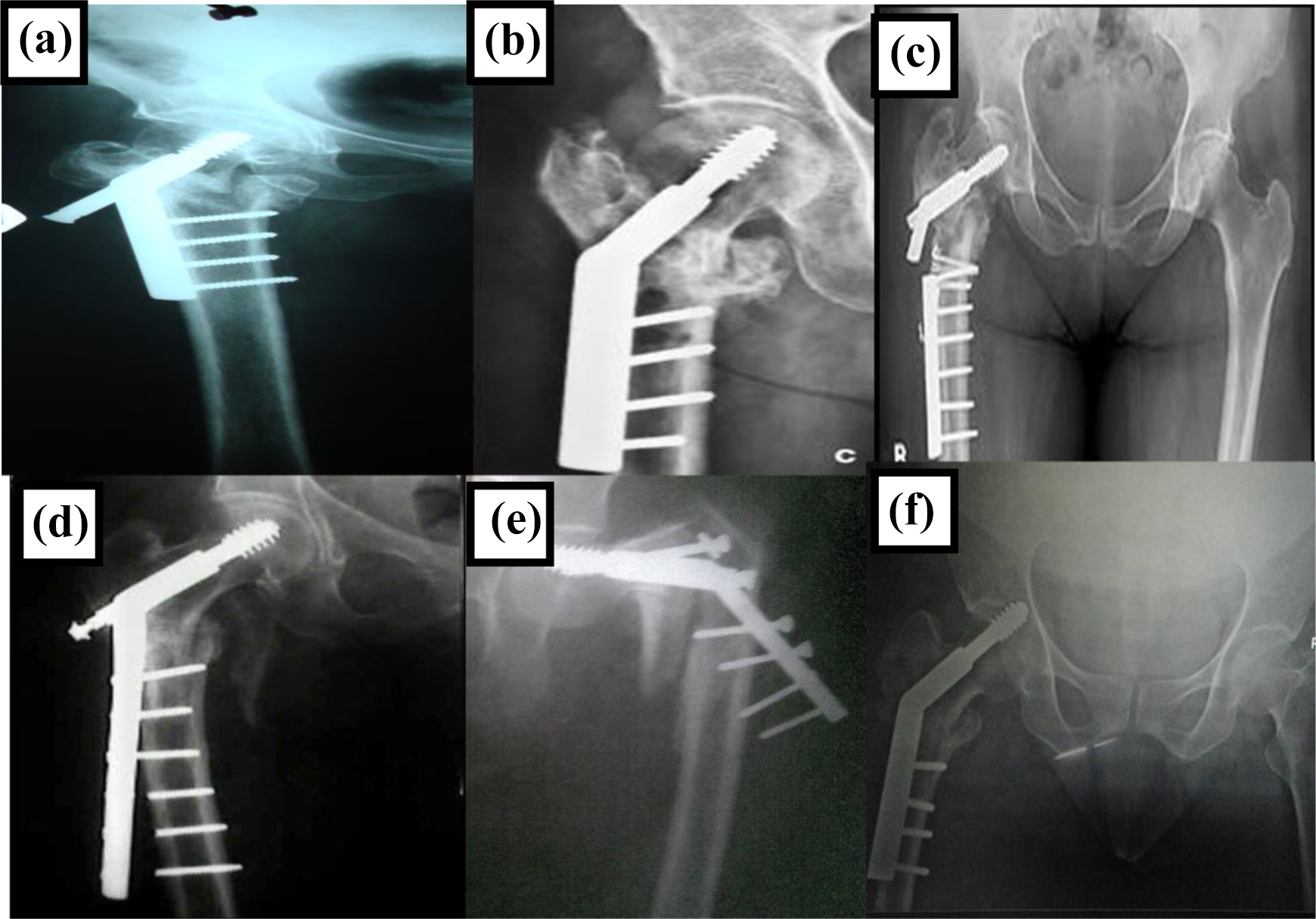
Complications seen in patients treated with DHS: A. Screw backout in OTA 31-A2; B. Malunion in OTA 31-A2; C. Implant breakage nonunion in OTA 31-A3; D. Cortical screw break in OTA 31-A3; E. Implant failure and non-union in OTA 31-A2; F. Screw migration in OTA 31-A2.
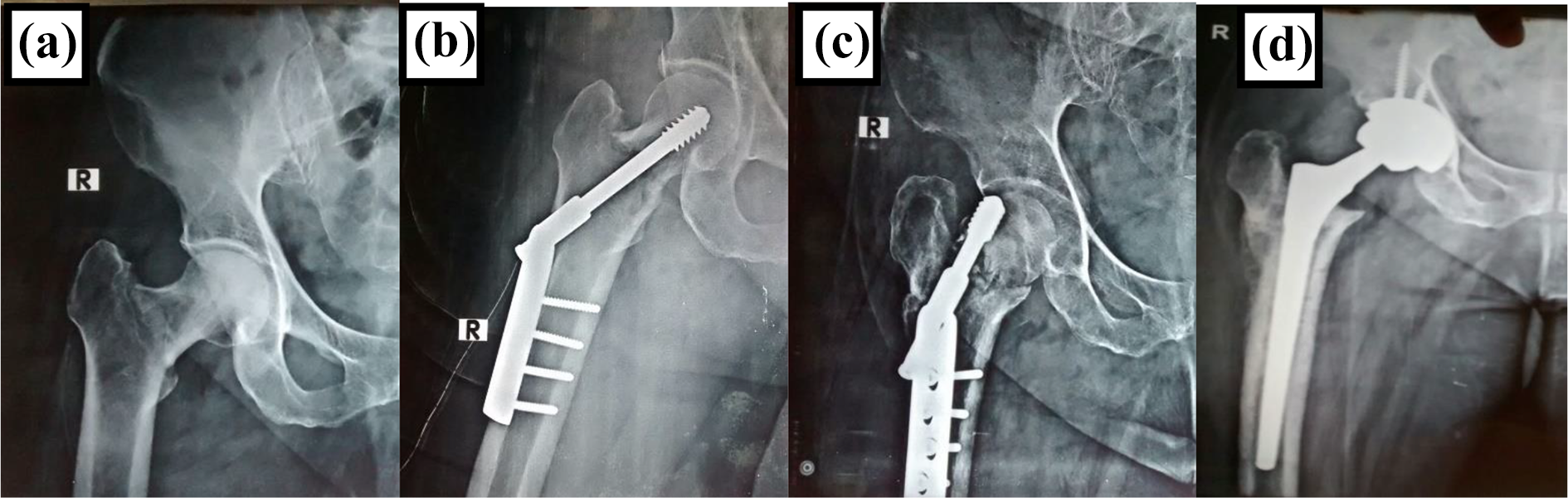
Radiographs of Failed DHS converted to Total Hip Arthroplasty. A. Preoperative Radiograph B. Immediate Post-operative C. Shows Screw cut out. D. Conversion to Total Hip Arthroplasty.
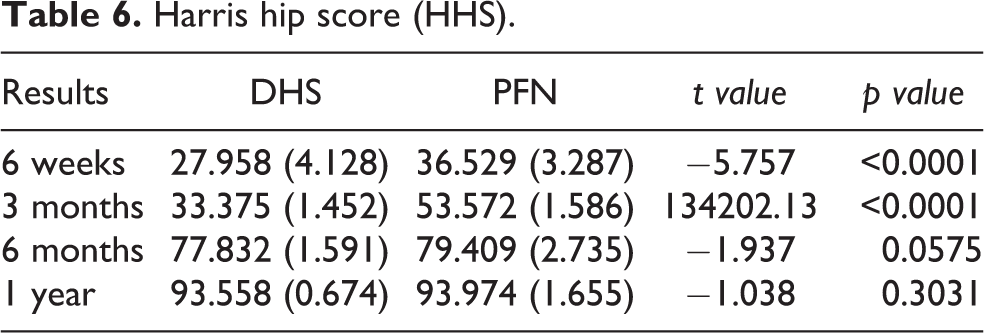
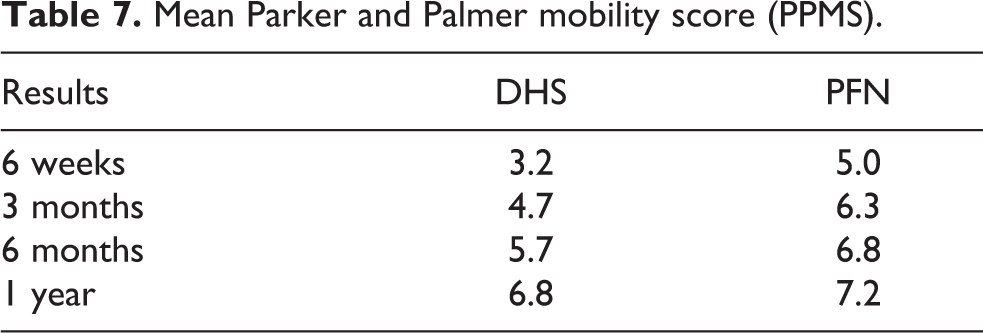
Patient with screw back out had varus malunion but didn’t have difficulty in walking. Eight patients had varus malunion of 120° to 125° due to excessive collapse in DHS group. The functional outcome results were analysed according to HHS and PPMS (Tables 6 and 7) and Figure 9. The mean HHS at 6 weeks for DHS was 27.96 as compared to 36.53 in PFN (p < 0.0001) which increased to 33.37 and 53.57 for DHS and PFN group respectively (p < 0.0001) at end of 3 months. Scores again increased to 77.83 and 79.41 for DHS and PFN group respectively at the end of 6 months (p < 0.0001) but this difference disappeared at the end of 1 year to 93.56 in DHS as compared to 93.97 in PFN group (p value = 0.30). The mean preoperative PPMS in both groups was 8.8 and after 1 year it was 6.8 in DHS and 7.2 in PFN. HHS was excellent in 42 (56%), good in 14 (18.7%), fair in 13 (17.3%) and poor 6 (8%) in DHS group as compared to excellent in 52 (69.3%), good in 20 (26.7%), fair in 2 (2.7%) and poor in 1 (1.3%) cases in PFN group (Table 7).
Harris hip score (HHS).
Mean Parker and Palmer mobility score (PPMS).
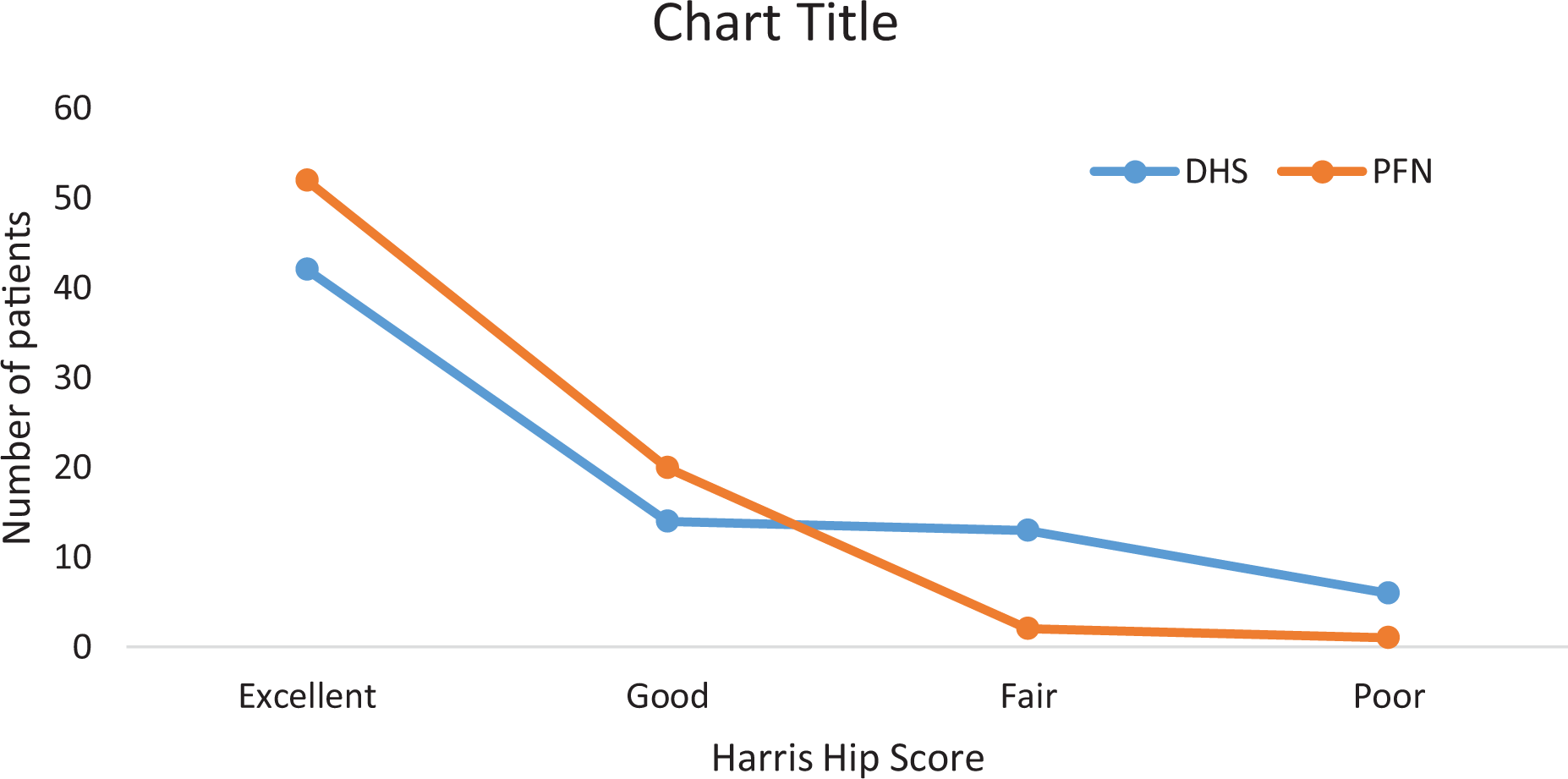
Results of Harris Hip Score (HHS). The data represents the number of patients in each category at 1 year post-op.
Discussion
The development of DHS in the 1950’s revolutionized the management of unstable intertrochanteric fractures. 16,17 Larger exposure, increased operative time, increased blood loss, excessive collapse with shortening and mechanical failures made it unsuitable for unstable fracture in the elderly with co-morbidities. 17 The common causes of fixation failure are osteoporosis, instability, improper anatomical reduction, failure of fixation device and improper placement of the Richard’s screw. 18 In early 90’s, PFN was developed with biomechanical and biological advantage over DHS and has become more prevalent in use. 1 –3,19,20 The moment arm of PFN is shorter than in DHS, because the load is transmitted to the axis of nail which is more medial which minimizes the amount of femoral neck collapse. The PFN compensates the function of the medial column. It is documented that, to initiate sliding of hip screw requires increased force in PFN as compared to DHS. 21 The longer the barrel length the lesser the forces required for initiation of sliding of screw. DHS are not well fixed in an osteoporotic bone. The intramedullary location of PFN prevents significant shortening at fracture site and its buttressing effect prevents medialization of the femoral shaft. 5,22
In our study most of the fractures occurred at home from a simple fall in elderly females. In our study, A2 (52%) was the most common type of fracture followed by A3 (48%). We used Singh’s index to measure osteoporosis, though the accuracy of the Singh index has been questioned by several authors. 23 In our study 88 (58.67%) cases were with grade 4 and above according to the Singh’s index. The ideal fixation device for unstable IT fractures is still controversial. 10,11 Due to the complexity of this fracture, not a single device is suitable for all fracture patterns. The treatment of unstable ITF is a challenge for the surgeon either due to fracture geometry or unavailability of suitable implant to overcome the stress at the fracture site. In our series there were no instances of femoral shaft fractures or extension of the fractures either intra-operatively or post-operatively. Mechanical failure of PFN still remains a major concern which can be significantly reduced by placing screws in ‘safe zone’. 24 In our study, we had significantly lesser length of incision, duration of surgery, blood loss (measured by method described by Brecher et al.) except fluoroscopy time in PFN which corroborated with other studies. 4,13,15,25 In another study duration of surgery was similar in both groups. 7 Recent studies showed no significant difference between the groups. 10,11
There were one preoperative and two iatrogenic fracture of lateral cortex in PFN group which was augmented either with an additional screw or cerclage wire. Recent articles stated that lateral femoral wall fracture in addition to posteromedial fragment here the main predictor for a reoperation after an intertrochanteric fracture fixation. 25,26 PFN group had significantly less pain, less incidence of deep infection and better range of motions compared to DHS group. Patients regaining the pre-injury walking ability was better in the PFN group significantly as in other studies. 27 We had five cases of superficial and one deep infection in the DHS group but didn’t encounter any infection in PFN group. In our series there was lesser cases of implant failures in PFN as compared to DHS group which was in concordance with other study. 27 In our study, the screw complications were seen more in the DHS group as compared to PFN group which was similar to other studies. 10 In this study reoperation rate was higher in DHS group. In another study, rates of reoperation in the two groups were alike. 6 The conversion to the total hip arthroplasty after failed PFN was more demanding than DHS. We didn’t had any conversion to arthroplasty in PFN group to prove its authenticity. In this study, the average limb length shortening in DHS group was higher than the PFN group, which was due to greater fracture impaction resulting from increased sliding the lag screw. 1,28 DHS group had more number and degree of malunion as compared to the PFN group where all fractures united with lesser varus angulation (<10°). In PFN group the fracture healing was not affected by lesser compression at the fracture site. 11 No difference in persistent pain in both groups was found in another study. 29
In our study both PWB and FWB were started significantly early in PFN. Pre-injury walking ability was statistically insignificant in both groups, but the PFN group surpassed the DHS group in the number of patients retaining their pre-injury walking ability at 3 and 6 months post-operatively corroborating the previous studies. 28 However, another study reposed DHS may allow more patients to return to their previous level of activity. 29 Indeed, PFN was superior to DHS as per the duration of surgery, rates of fixation failure, intra operative blood loss, lesser requirement of post-operative blood transfusion and overall complications in contrast to another study, which revealed that PFN had the same effectiveness as DHS regarding need for blood transfusion, infection, mortality and reoperation. 30 Probably these conflicting results were due to heterogeneity of the described trials. This study could help concluding that PFN is superior to DHS as a procedure for unstable intertrochanteric fractures in elderly, corroborating other previous studies. 6,8,9 In the long term both the implant had almost similar functional outcomes. 6
Drawbacks – In our study patients with age between 54 years to 89 years were considered which is a very wide range. The patients on extremes of this range have contrasting bone density and hence the outcomes will vary.
Advantages – A low drop-out rate, large number of patients, management and description of complications in the follow up period are some of the advantages of our study.
Conclusion
PFN being a load sharing device with a better biomechanical advantage offers biological indirect reduction, concomitantly allowing early mobilization and weight bearing with comparatively lesser complications and superior functional outcomes, in comparison to DHS particularly in unstable intertrochanteric fractures in the elderly with osteoporosis.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.