
Abstract
Introduction:
Currently there is no gold standard clinical test or investigation available to diagnose piriformis syndrome. We have found a pose used by the patients to describe the pain in the gluteal region in cases of suspected piriformis syndrome. This pose in our study has been described as ‘hand on hip sign’ (HHS). In this study, we aim to assess the significance of this sign in screening of patients with piriformis syndrome.
Materials and methods:
Seventy patients presenting with pain in the gluteal region with radiculopathy between the age group of 18 years and 60 years were included. All patients were asked to locate the site of the pain in the gluteal region. The demonstration of pain by the patients was noted. If the description matched the description of HHS, it was considered to be positive, else it was considered negative. All patients were subjected to four piriformis-specific confirmatory clinical tests. Considering that there is no single confirmatory test, any patient in whom any two piriformis-specific signs were elicited was considered as a case of piriformis syndrome. Using the data, sensitivity, specificity and positive and negative likelihood ratio of the HHS in the diagnosis of piriformis syndrome were calculated. Inter-test comparison was also made using Cohen’s kappa statistic.
Results:
HHS was found to have a sensitivity of 86% and a specificity of 75%. It also has a high positive predictive value of 94% and a positive likelihood ratio of 3.44. Inter-test reliability comparison showed that there was a fair to moderate agreement between HHS and other confirmatory piriformis-specific tests.
Conclusion:
HHS serves as an effective screening test in the identification of piriformis syndrome.
Introduction
Piriformis is a flat pyramidal muscle which arises from the anterior surface of the sacrum, passes through the greater sciatic notch and is inserted on the tip of the greater trochanter. 1 Piriformis syndrome is a form of non-discogenic sciatica, occurring as a result of sciatic nerve impingement below the piriformis muscle. 1 –3 Piriformis syndrome has for long been a difficult condition to diagnose. Few studies believe it to be under-diagnosed while others suggest that it is over-diagnosed. 4,5 There are two important reasons for the difficulty in diagnosis of this condition. First is the varied symptoms that the patients present with. The symptoms include gluteal pain and paraesthesias in the back, groin, perineum, hip, calf and foot. 6 Some patients have pain while defecation while others have reported to have sexual dysfunctions in the form of dyspareunia and impotency. 2,6,7 In presence of these myriad of symptoms, it is difficult for the treating physician to identify and treat the condition. The second reason is that currently there is no gold standard clinical test or investigation available to diagnose this condition. 8 We have identified a specific pose, described as ‘hand on hip sign’ (HHS), in which the patient describes the pain in the gluteal region in cases of suspected piriformis syndrome, which can be confirmed by other confirmatory tests.
In the typical form of this pose, the patient is standing erect with the shoulder slightly abducted, elbow flexed, wrist resting over the greater trochanter, fingers pointing anteriorly and the thumb pointing towards the sacrum (Figure 1). We found that patients describe the pain to be originating from the point where the tip of the thumb is pointing at. We assume that when the wrist is resting on the tip of the greater trochanter, the tip of the thumb can be easily used to point towards the tender point in the piriformis muscle. Patients also describe the radiculopathy separately using the palm and moving it across the back of the thigh and calf. This classical description was not found in other causes of gluteal pain. The ‘C’ sign which is described in femoroacetabular impingement syndromes is similar, but the pain in these conditions is pointed anteriorly at the hip joint using the fingers, whereas in HHS the pain is pointed posteriorly using the thumb.
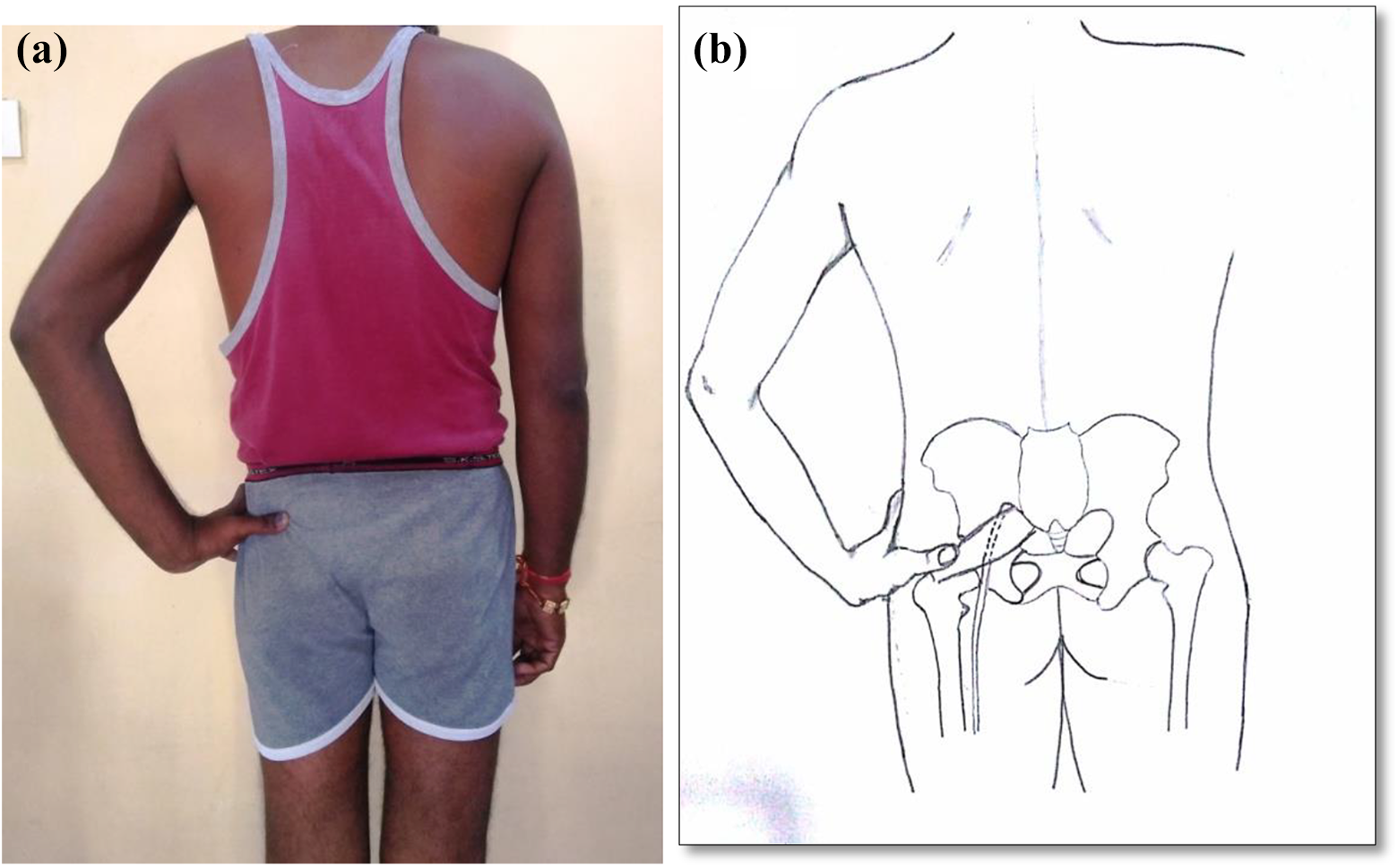
(a) Clinical representation of HHS and (b) anatomical relation of HHS with the piriformis muscle. HHS: hand on hip sign.
Materials and methods
The aim of the study is to assess the sensitivity, specificity, positive predictive value, positive and negative likelihood ratio and diagnostic odds ratio of the HHS in the diagnosis of piriformis syndrome. This prospective study was conducted in the department of orthopaedics outpatient department between May 2016 and May 2018. Institutional ethical committee clearance (ESIC Ethical Committee) was obtained and all the patients provided written consent before enrolling in the study. The study was conducted according to the ethical standards of the Helsinki Declaration of 1975, as revised in 1983. Sample size was calculated based on the systematic review conducted by Hopayian et al. 2 The authors reported a frequency of most of the piriformis-specific signs to be below 25%. Accordingly, considering a prevalence of 0.2 and precision of 0.10, a sample size of 61 patients was derived. Considering some random screening errors, the total sample size was rounded off to 70 patients.
Patients presenting with pain in the gluteal region which is aggravated upon sitting and associated radiculopathy were included in the study. A questionnaire was prepared to record the important details including the age group, occupation and history of preceding trauma. The same question was asked to all the patients, that is, ‘Can you locate the exact site of pain in standing position’? If the patient assumed the pose of HHS as described above, it was considered as HHS present. If the pose was not assumed, then it was considered as HHS absent. All the patients were subjected to piriformis-specific confirmatory tests, the details of which are given in Table 1. If any two of the piriformis-specific tests were positive, it was considered as ‘Piriformis syndrome confirmed’, else it was considered as ‘Piriformis syndrome ruled out’. All the patients with confirmed piriformis syndrome received a dose of ultrasound-guided intramuscular steroid. The response to the drug was also recorded. All the results were tabulated and a 2 × 2 contingency table was plotted to assess the sensitivity, specificity, positive predictive value and likelihood ratio of the HHS in the diagnosis of piriformis syndrome. The algorithm followed in the study has been shown in Figure 2. All the statistical analyses were performed using SPSS version 23.
Description of the piriformis-specific clinical tests, commonly used in the diagnosis of piriformis syndrome.
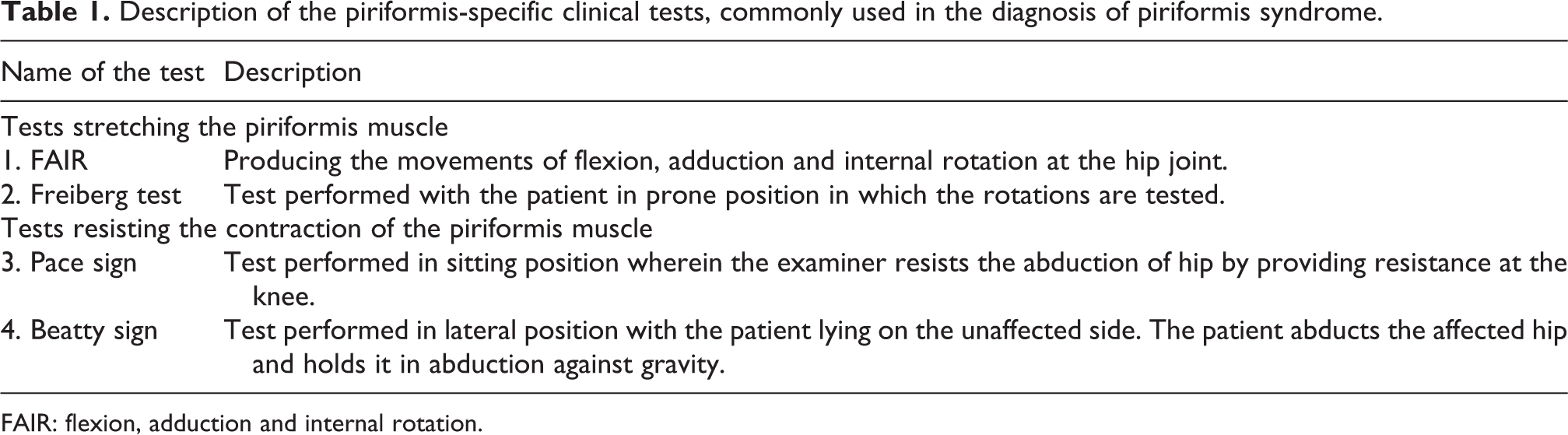
FAIR: flexion, adduction and internal rotation.
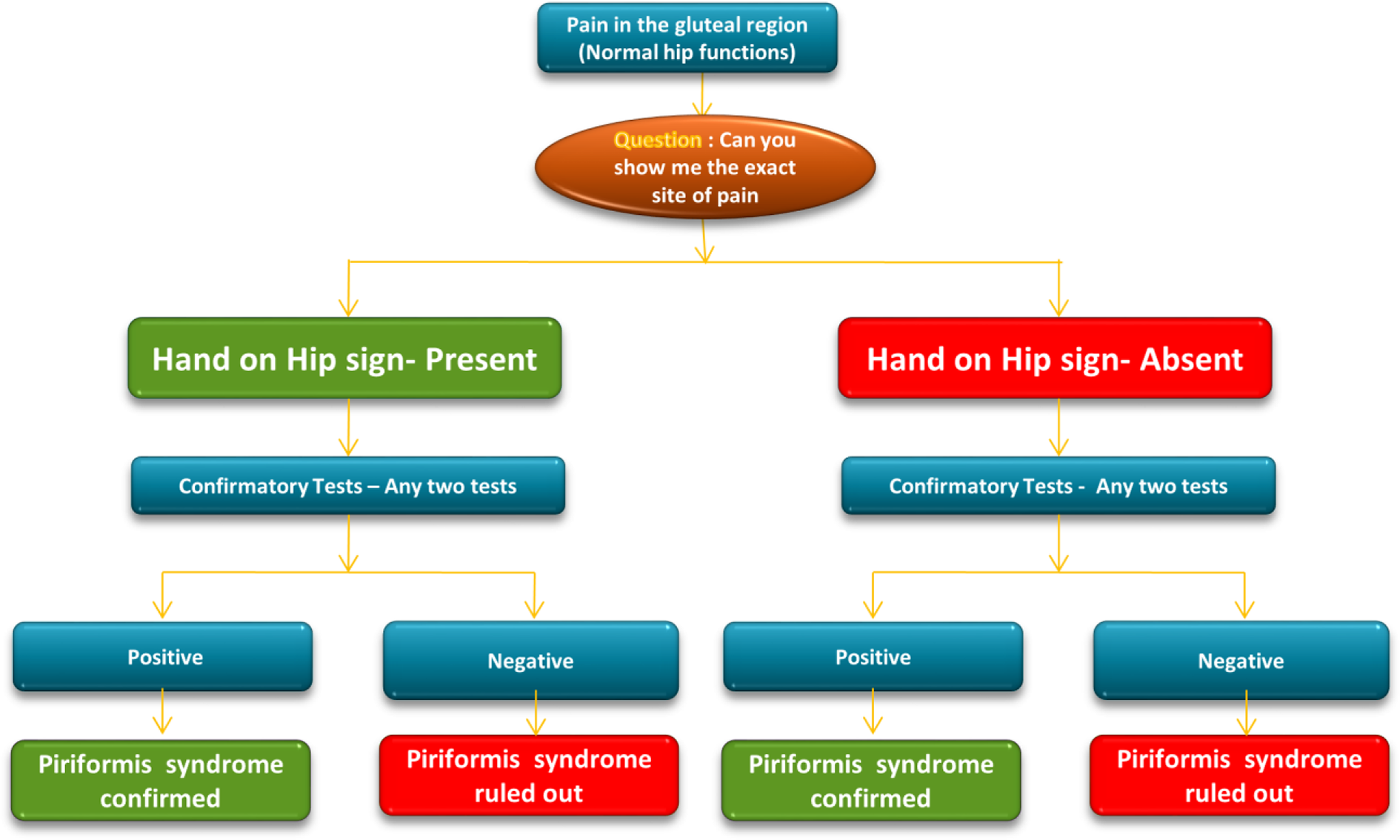
The algorithm followed in the study.
Results
Seventy patients with complaints of gluteal pain with radiculopathy were included in our study. The disease was predominantly found in females compared to males (45 females, 25 males). The most common age group was between 35 years and 50 years (n = 35). History of antecedent trauma was present in 10% of patients, while 10% of patients had a job associated with prolonged sitting. Three patients had other associated neurological abnormalities (post-polio residual paralysis, n = 1 (Figure 3); Huntington’s disease, n = 1; and Parkinson’s syndrome, n = 1).

Patient with post-polio residual paralysis of the right side, with a positive HHS on the same side. HHS: hand on hip sign.
Out of the 70 patients with gluteal pain and radiculopathy, 53 patients had a positive HHS and 17 had a negative HHS. Out of these 53 patients, piriformis syndrome was confirmed in 50 patients while it was ruled out in 3 patients. Of the 17 patients with negative HHS, piriformis syndrome was confirmed in 8 patients and was ruled out in another 9 patients. The contingency table was prepared from the above details (Figure 4). HHS was found to have a sensitivity of 86% and a specificity of 75%. It also has a high positive predictive value of 94% and a positive likelihood ratio of 3.44 and a negative likelihood ratio of 0.18. The diagnostic properties of HHS have been summarized in Table 2. We also compared the HHS with four piriformis-specific confirmatory tests and assessed the agreement using Cohen’s kappa statistic (Table 3). We found that this sign has got a moderate agreement with the flexion, adduction and internal rotation (FAIR) test and a fair agreement with the other three tests described in Table 1. All the patients with confirmed piriformis syndrome received a dose of ultrasound-guided corticosteroid injection and in all the patients the pain subsided after the injection.
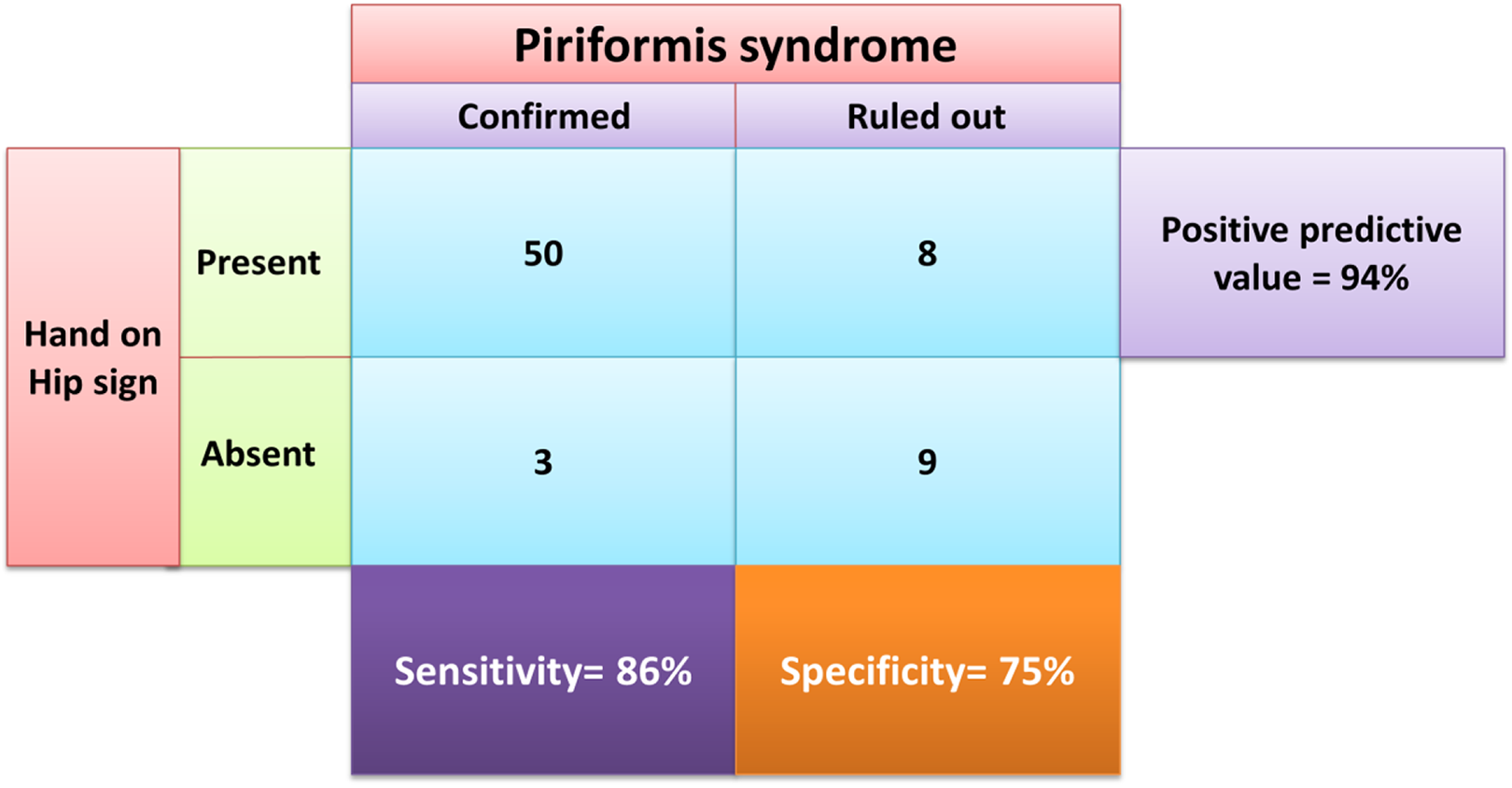
The 2 × 2 contingency table showing the sensitivity, specificity and positive predictive value of HHS in the diagnosis of piriformis syndrome. HHS: hand on hip sign.
Diagnostic properties of HHS in the diagnosis of piriformis syndrome.
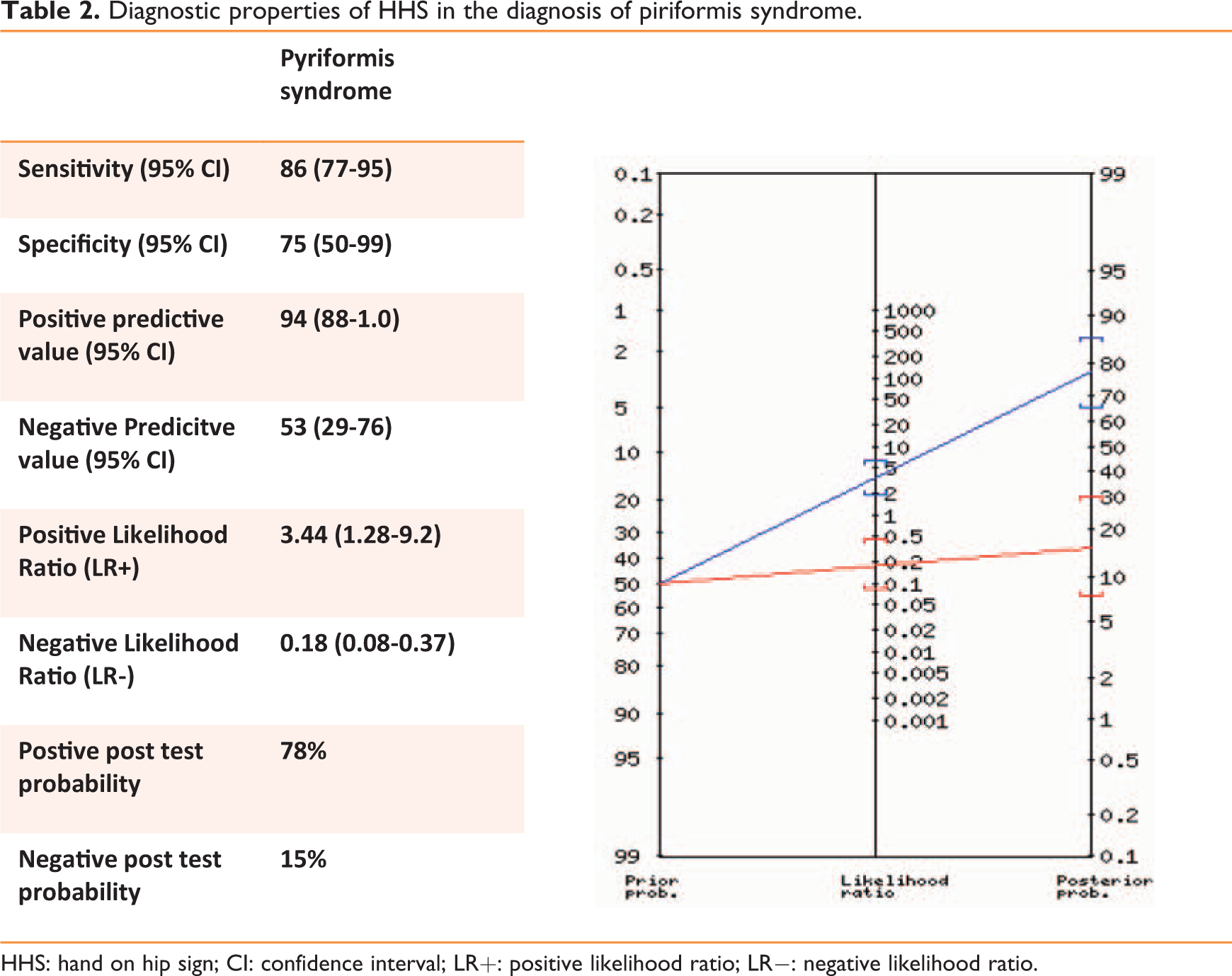
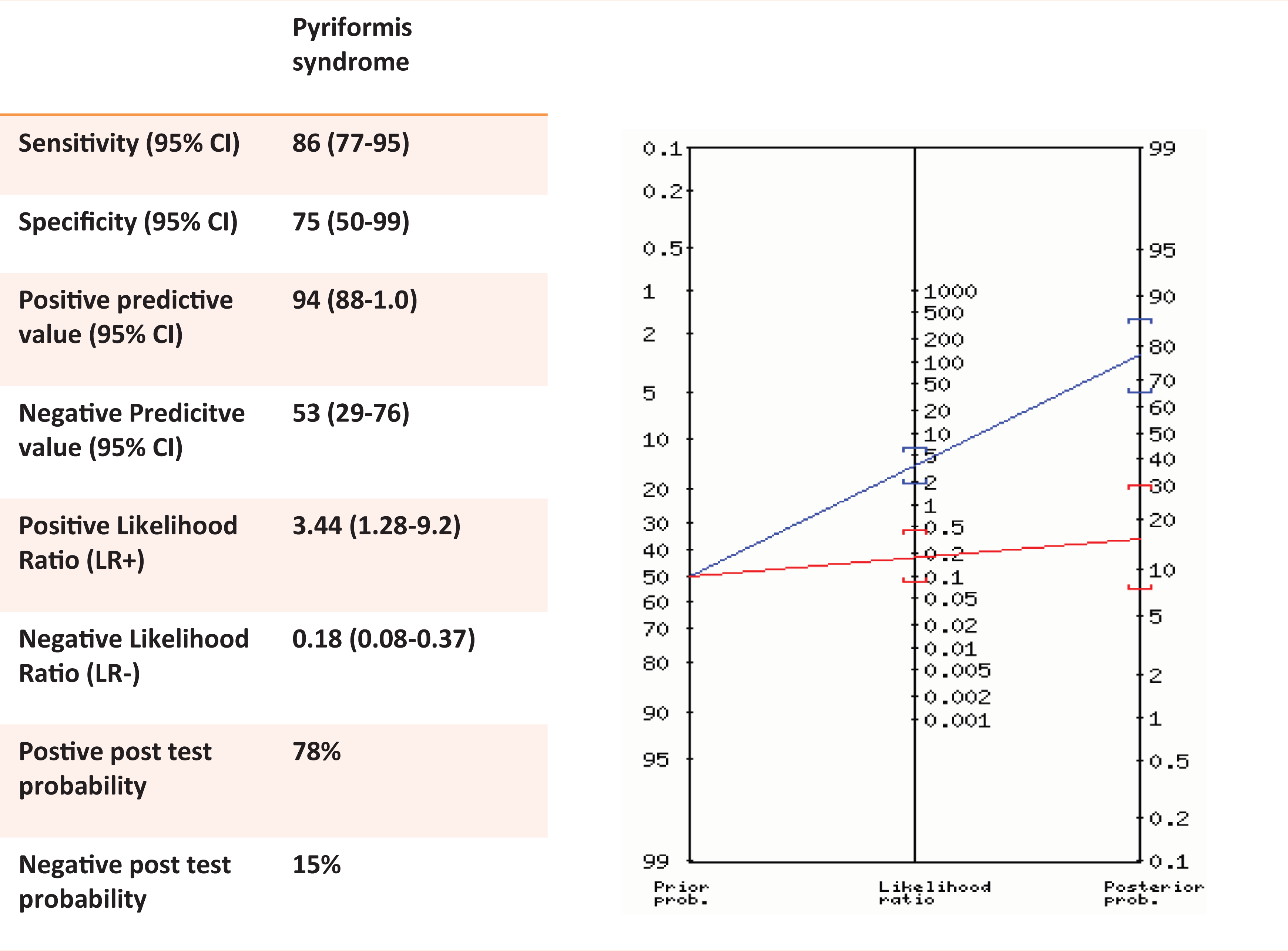
HHS: hand on hip sign; CI: confidence interval; LR+: positive likelihood ratio; LR−: negative likelihood ratio.
Comparison of the agreement between HHS and the other piriformis-specific signs using the kappa statistic.
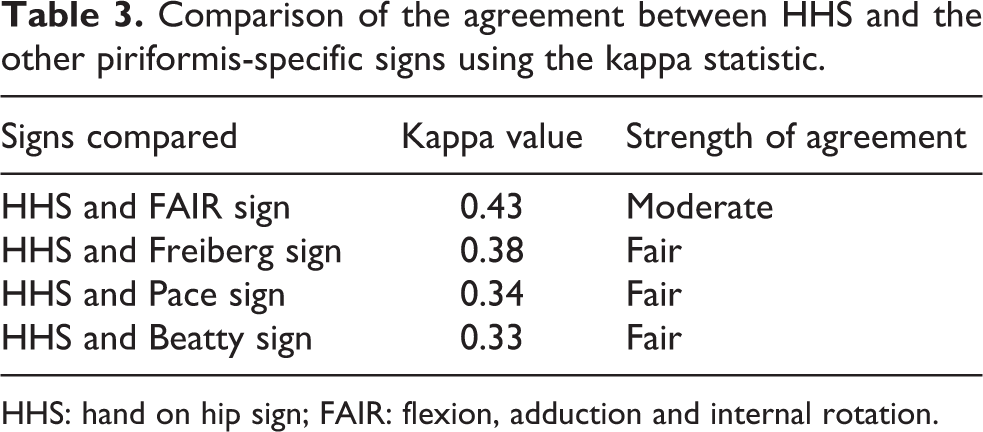
HHS: hand on hip sign; FAIR: flexion, adduction and internal rotation.
Among the patients with false-positive and true-negative HHS (n = 12), six patients had a positive straight leg raise test (SLR), four patients had tenderness over the ipsilateral sacroiliac joint with a positive Patrick’s test and two patients had lumbar paraspinal tenderness without positive SLR or Patrick’s test.
Discussion
Piriformis syndrome is a form of entrapment neuropathy occurring as a result of compression of the sciatic nerve at the greater sciatic notch, by the piriformis muscle. 1,2 About 6–8% of the cases of sciatica are reported to be caused by piriformis syndrome. 9 The term piriformis syndrome was first coined by Robinson in the year 1947. 10 Very little has been understood about its etio-pathogenesis and it has been considered as a diagnosis of exclusion only after other causes of radiating pain in the buttock have been ruled out. 11 There is no gold standard clinical test available for the diagnosis of piriformis syndrome. 8 The currently available tests can be broadly divided into tests stretching the muscle and tests resisting the contraction of the muscle. The details of these tests are described in Table 1. All these tests are meant to reproduce the radiating pain as a result of sciatic nerve compression. 8,12 –15
Hopayian and Danielyan conducted a systematic review to evaluate all the existing signs and symptoms in the diagnosis of piriformis syndrome. 7 They found that the common symptom in patients with piriformis syndrome was radiating pain along the ipsilateral lower limb (77%), followed by buttock pain (56%). Considering that only about half of the patients with piriformis syndrome report it as buttock pain, suspecting piriformis syndrome in all patients with buttock pain is an over-exaggeration. In this situation, HHS, which has a high sensitivity, serves as an effective screening test in patients with piriformis syndrome.
Robinson first described the six-point diagnostic criteria to identify piriformis syndrome. These criteria were considered to be overly specific identifying only a fraction of the cases. Considering these problems, Michel et al. devised a 12-point scoring system based on patients’ symptoms and the available clinical tests. 8 The probability of piriformis syndrome is high if the score is more than or equal to 8. HHS can act as a forerunner in the screening of piriformis syndrome on whom this 12-point scoring system can be applied. They also found that neither electromyography nor magnetic resonance imaging showed any significant changes in the piriformis group patients. Thus they did not include any radiological investigations in their scoring system.
In our study, we found that the HHS has a high sensitivity of 86% and a positive predictive value of 75%. The positive likelihood ratio of the test was 3.4 and the negative likelihood ratio was 0.18. This test serves as an important screening tool to identify the patients with piriformis syndrome which can be further confirmed with the other confirmatory tests. We also compared this sign with the other piriformis-specific signs that have been described using the kappa statistic. We found that there was a moderate agreement between HHS and the FAIR test, while there was a fair agreement with the other three piriformis-specific signs.
The lack of an effective radiological investigation is an important hurdle in the diagnosis of patients with piriformis syndrome. To be able to confirm the diagnosis, we need to evaluate the patient with the available clinical tests. Although pain in the buttock is the second most common symptom in patients with piriformis syndrome, it is difficult to suspect it in all patients with buttock pain. The HHS is of particular importance in this scenario as it serves as an effective screening sign with a high positive predictive value in the identification of piriformis syndrome.
The study is limited by its small sample size and reliability on the other clinical tests in the diagnosis of piriformis syndrome. This can be overcome by future research which can evaluate the significance of this test over a large population and also assess the reliability and validity by a multi-observer study.
Conclusion
HHS is a very good screening test in the diagnosis of piriformis syndrome. It is easy to identify and has a very high positive predictive value. Its importance lies in helping the physicians identify the condition and avoid unnecessary investigations and cut the treatment cost for the patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.