
Abstract
Introduction:
Total knee arthroplasty has been adopted to be the most successful treatment for advanced knee osteoarthritis. The adoption of multimodal periarticular analgesic (MPI) has been shown to have satisfactory pain control after surgery. However, there is relatively lack of data investigating whether this mode of pain control is effective in enhancing rehabilitation.
Method:
This is a prospective randomized control trial from July 2017 to June 2018, including 82 patients, in which 43 of them had MPI injection and 39 of them had no MPI injection. Primary outcome measures included the number of days required to perform straight leg raise, length of hospital stay, and Insall knee score upon discharge. Secondary outcome measures included total dose of patient-controlled analgesia (PCA) consumption postoperatively and visual analog scale (VAS) at rest and on motion during postoperative days 1–4.
Result:
The MPI group performed significantly better than the femoral nerve block (FNB) group in terms of early functional outcome, namely the number of days required to perform straight leg raising and length of hospital stay. The total postoperative PCA consumption and VAS score on motion during postoperative day 1 were also significantly better for MPI group. There was no difference in Insall knee score upon discharge between these two groups.
Conclusion:
Compared to FNB, MPI depicts a faster inpatient rehabilitation, accounted by its quadriceps-sparing, and better pain relief especially in the early postoperative period.
Introduction
Total knee arthroplasty is currently the most successful operative treatment for advanced knee osteoarthritis. It also constitutes one of the most common elective operations in orthopedics and is expected to experience a sixfold increase from 2005 to 2030. 1 For patients receiving the treatment, the adoption of multimodal periarticular analgesic (MPI) has greatly improved postoperative pain during hospital stays. 2,3 Compared with femoral nerve block (FNB), MPI offers the theoretical advantage of a quadriceps-sparing effect. 4 Pain relief achieved with MPI may also be comparable or even superior on postoperative day 1. 5
There is a paucity of extant literature, however, examining the effect of MPI on inpatient functional rehabilitation of patients undergoing total knee replacement. Our study aims to compare inpatient clinical outcomes of using MPI versus FNB in a Chinese population. With inputs from a multidisciplinary team, the clinical results can facilitate future patient education and guide expectations concerning pain management related to the operation.
Patients and methods
The current study is a prospective randomized controlled trial investigation, lasting from July 2017 to June 2018. The study was approved by the Regional Ethics Committee, Kowloon West Cluster, Hong Kong, in June 2017 (record number 111-06).
A total of 82 Chinese patients receiving total knee replacement operations in Caritas Medical Centre were recruited for participation in the study. Inclusion criteria were as follows: aged 80 years old or less and scheduled for total knee arthroplasty for tricompartmental osteoarthritis of the knee under spinal anesthesia. Exclusion criteria comprised the following: allergy to analgesic agents, history of cardiovascular disease or arrhythmia, impaired renal function, or gastrointestinal bleeding. Patients having excessive knee ligamentous laxity and requiring extensive ligamentous balancing and constraint implant for total knee arthroplasty were also omitted.
Patients fulfilling the inclusion criteria of the study were recruited in preassessment clinics for total knee replacement in Caritas Medical Centre. After receiving a thorough explanation concerning the study, the patients provided informed written consent for participation. Patients were randomized to receive either MPI (case group) or FNB (control group) during the operation by the study coordinator, using the method of drawing lots in the Hospital Authority Operative Theatre Management System.
A study protocol for MPI and FNB was adopted with reference to a similar study carried out by Wall et al. 6 In the MPI protocol, infiltration agents included 10 mL of 0.5% levobupivacaine, 1 mL (30 mg) ketorolac, and 5 mL of 1:10,000 epinephrine, diluted with 0.9% normal saline to a total volume of 100 mL. The agent was injected into the posterior capsule, periosteum of both medial and lateral femoral condyles, periosteum of proximal medial and lateral tibia, and subcutaneous tissue along the main wound, respectively, after irrigation and prior to implant placement. 7 A lamina spreader was placed between the femur and tibia to increase the knee joint space and to expose the posterior capsule. The knee was maximally flexed to displace the popliteal artery further posteriorly to avoid injury during MPI injection. 8 Aspiration was also performed before the injection to ensure that the popliteal artery was not punctured.
In the FNB protocol, the femoral nerve was identified by an anesthetist under ultrasound guidance. As the needle tip was inserted adjacent to the nerve, a small dose of local anesthetic was administered to confirm position. Following visualization of the local anesthetic distributing around the nerve, the complete 10 mL of 0.5% levobupivacaine was injected.
Postoperatively, both groups of patients received an identical rehabilitation regime. The same patient-controlled analgesia (PCA) and oral analgesia regime (i.e. 1 week of Panadol 500 mg four times daily and Arcoxia 90 mg once daily) were administered. Physiotherapy, including walking exercise, knee range of motion (ROM) exercise, and muscle strengthening, commenced after the wound drain was removed on the first postoperative day. Patients were discharged on fulfilling hospital discharge criteria.
Data collection was carried out in preoperative clinics, in the first few days of in-hospital stay, and at discharge. Data collection was performed by case medical officers, nurses, physiotherapists, and occupational therapists, who were blind to patient group allocation. All staff involved in data collection had no communication with the chief operating surgeon and anesthetist concerning the mode of intraoperative analgesia.
Primary outcome measurements comprised length of hospital stay, Insall knee score upon discharge, and days to Modified Functional Ambulation Classification-5 (MFAC-5). Quadriceps power was assessed by days to straight-leg-raising (SLR) and by Medical Research Council (MRC) grading prior to the operation and in the first four days postoperation. Quadriceps power in kilograms before the operation was measured by a dynamometer, with the patient sitting and knee in 90° flexion, to be extended actively against the device.
Combined ROM were performed in a supine position using a goniometer device at postoperative day 1 to day 3 and upon discharge. Knee circumference (KC) in centimeters (cm) was measured by a soft measurement tape, leveled at the mid-patella. The percentage of KC increase was measured as the increase in KC divided by the original KC. Secondary outcome measures included pre- and postoperative pain according to the visual analog scale (VAS) and PCA consumption up to 24 hours postoperatively.
Statistical analysis
Statistical analyses were conducted using SPSS (version 23.0) for Windows (SPSS Inc., Chicago, Illinois, USA). Data entry was performed by a research assistant who was blind to patient grouping. Baseline equivalence, including demographic background, was analyzed using the paired t-test. To assess the effect of MPI on functional outcomes over time, two-way repeated-measures analysis of variance (ANOVA) was utilized. Post hoc analyses were carried out when any significant difference was identified in any outcome variable. Bonferroni correction was employed to adjust the α levels. Three independent sample t-tests were performed to examine the group differences for PCA consumption, hospital stay, and day of SLR, respectively. The p value <0.05 was considered statistically significant. Preliminary assumptions of the statistical tests, including data normality using the Shapiro–Wilk test (all p-values >0.05) and homogeneity of variance using the Levene test (all p-values >0.05) for the ANOVAs, were met.
Sample size
From a similar study conducted by Chen et al., 9 Cohen’s d value ranged from −3.98 to −1.05, and mean values of clinical parameters were provided. In the current study, the mean value of the effect size (d = −2.52) was used to calculate the requisite sample size. With a 5% level of significance and attrition rate of 20%, a sample size of 12 (six per group) was required to achieve a power of 90% for an interaction effect. We adopted a sample size of approximately 40 patients per group to augment the generalizability of the findings.
Results
The complete results are presented in Table 1.
Statistical data analysis of case versus control groups, presented by mean ± standard deviation. The p-values between groups were analyzed.
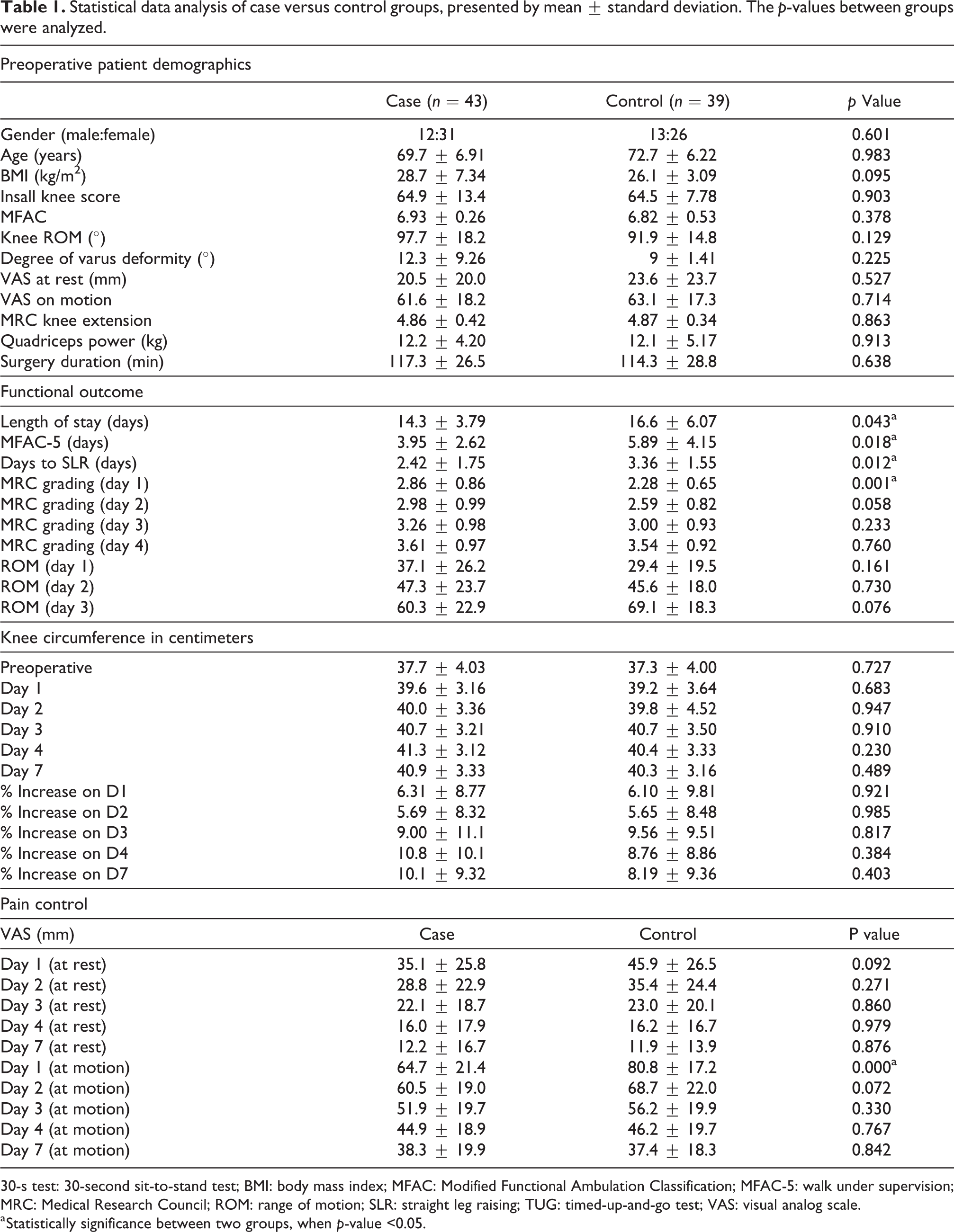
30-s test: 30-second sit-to-stand test; BMI: body mass index; MFAC: Modified Functional Ambulation Classification; MFAC-5: walk under supervision; MRC: Medical Research Council; ROM: range of motion; SLR: straight leg raising; TUG: timed-up-and-go test; VAS: visual analog scale.
a Statistically significance between two groups, when p-value <0.05.
Demographics
From July 1, 2017 to June 30, 2018, a total of 82 Chinese patients (25 males and 57 females) were recruited, including 43 MPI (case group) and 39 FNB (control group) patients. Demographics comprised age, gender, body mass index, preoperative Insall knee score, VAS, MFAC, combined knee ROM, and quadriceps power in both MRC grading and in kilograms. All parameters did not show statistical significance. Preoperative knee alignment and duration of surgery also exhibited no significant difference, indicating that the scale of surgery was similar for both groups.
Functional outcomes
Length of hospital stay
A significant difference was found for length of hospital stay in the case group (mean 14.3 days) versus the control group (mean 16.6 days), with a p-value of 0.043 (Figure 1).
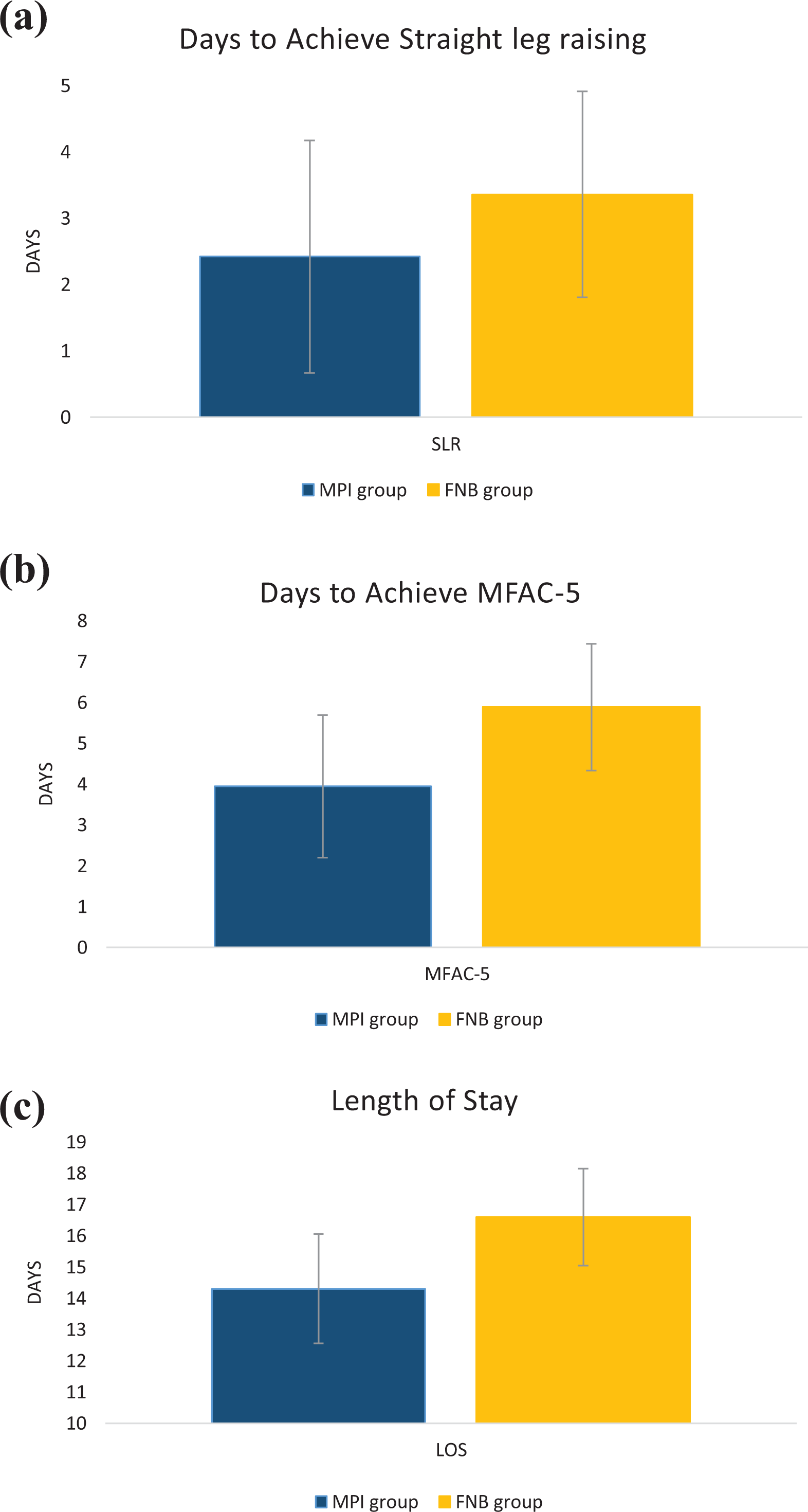
Functional performance during in-patient rehabilitation: (a) Days to achieve SLR, (b) MFAC-5 (walk under supervision), and (c) LOS. Statistical significance was noted on days to SLR, MFAC-5, and LOS. SLR: straight leg raising; LOS: length of stay; MFAC: Modified Functional Ambulation Classification.
Walking status
Number of days to supervised walking (MFAC-5) was 3.95 versus 5.89 for the case group versus the control group, showing statistical significance (p = 0.018) (Figure 1).
Quadriceps activity
The number of days for the case group (mean = 2.42 days) to perform SLR was significantly shorter than that for the control group (mean = 3.36 days) with a p-value of 0.012 (Figure 1).
The mean values of MRC grading on knee extension for both groups are shown in Figure 2. Post hoc multiple comparisons with Bonferroni adjustments demonstrated that knee extension power in the case group was significantly higher than that of the control group over postoperative day 1 (p = 0.001), but the difference between the two groups was no longer significant in the next three days.
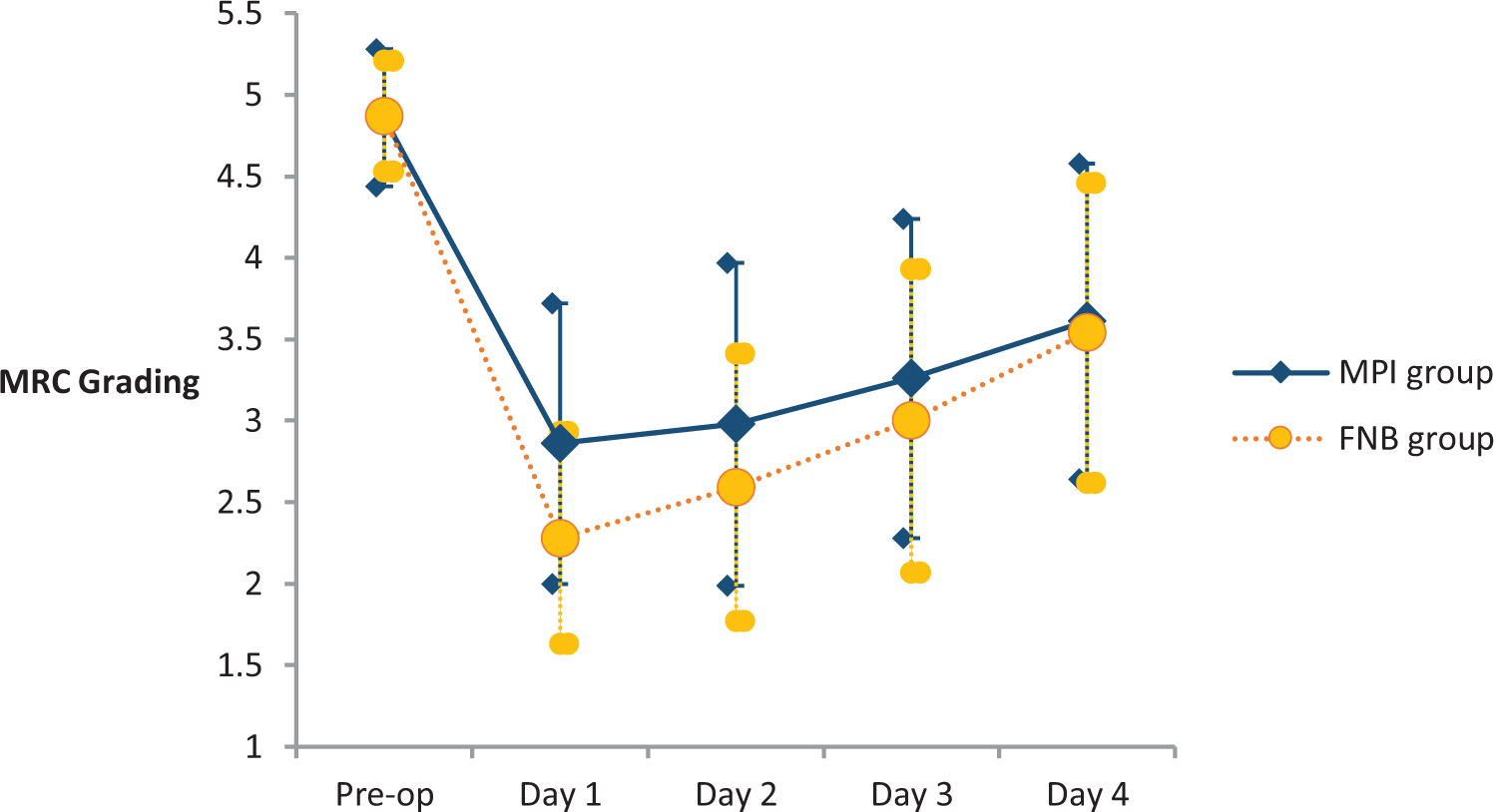
MRC of quadriceps muscle power: preoperative and postoperative days 1–4. Statistically significant difference upon day 1 for MPI versus FNB group was observed. MRC: Medical Research Council; MPI: multimodal periarticular analgesic; FNB: femoral nerve block.
Combined knee ROM and KC
No significant differences were identified in combined ROM (Figure 3) and KC (Figure 4) between the case group and the control group.
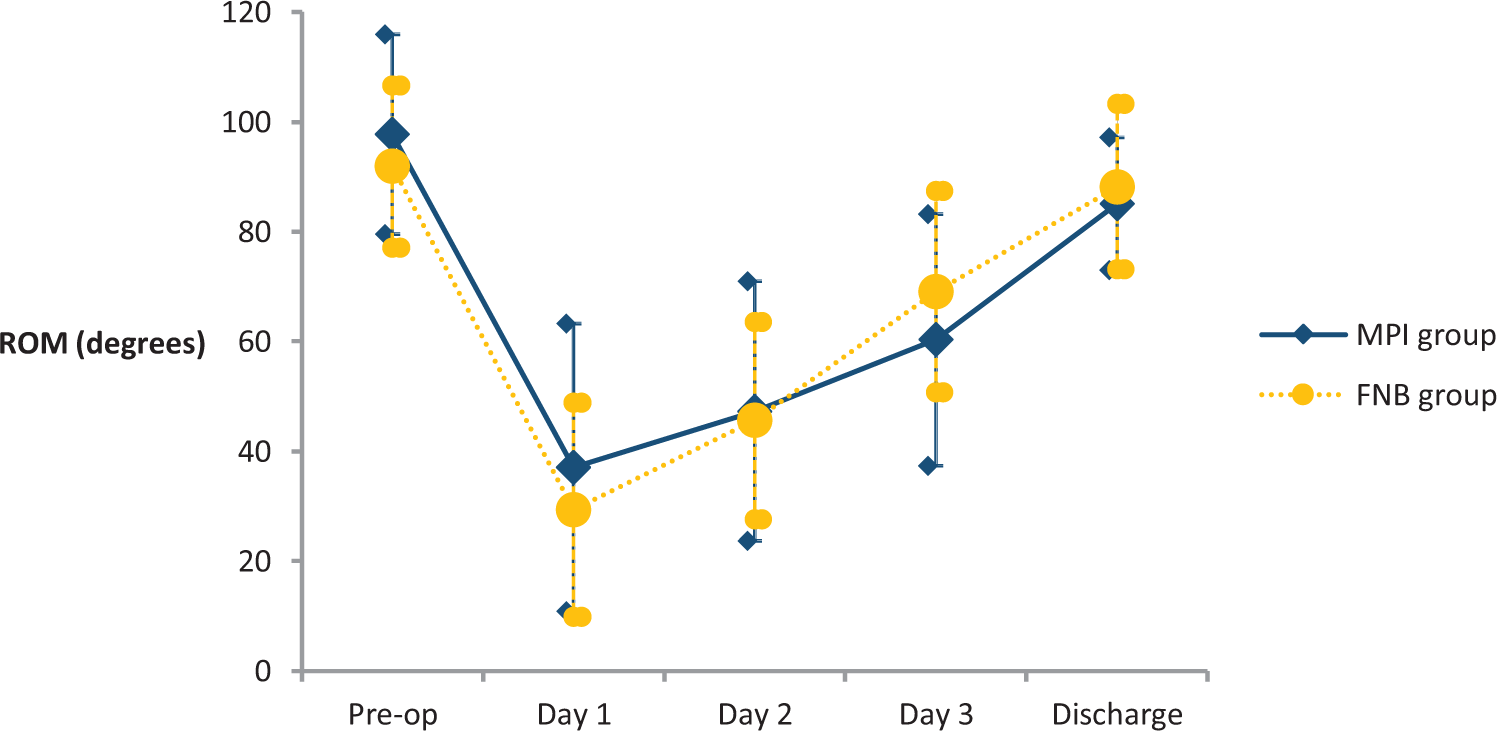
Combined ROM: preoperative, postoperative days 1–3, and upon discharge. ROM: range of motion.
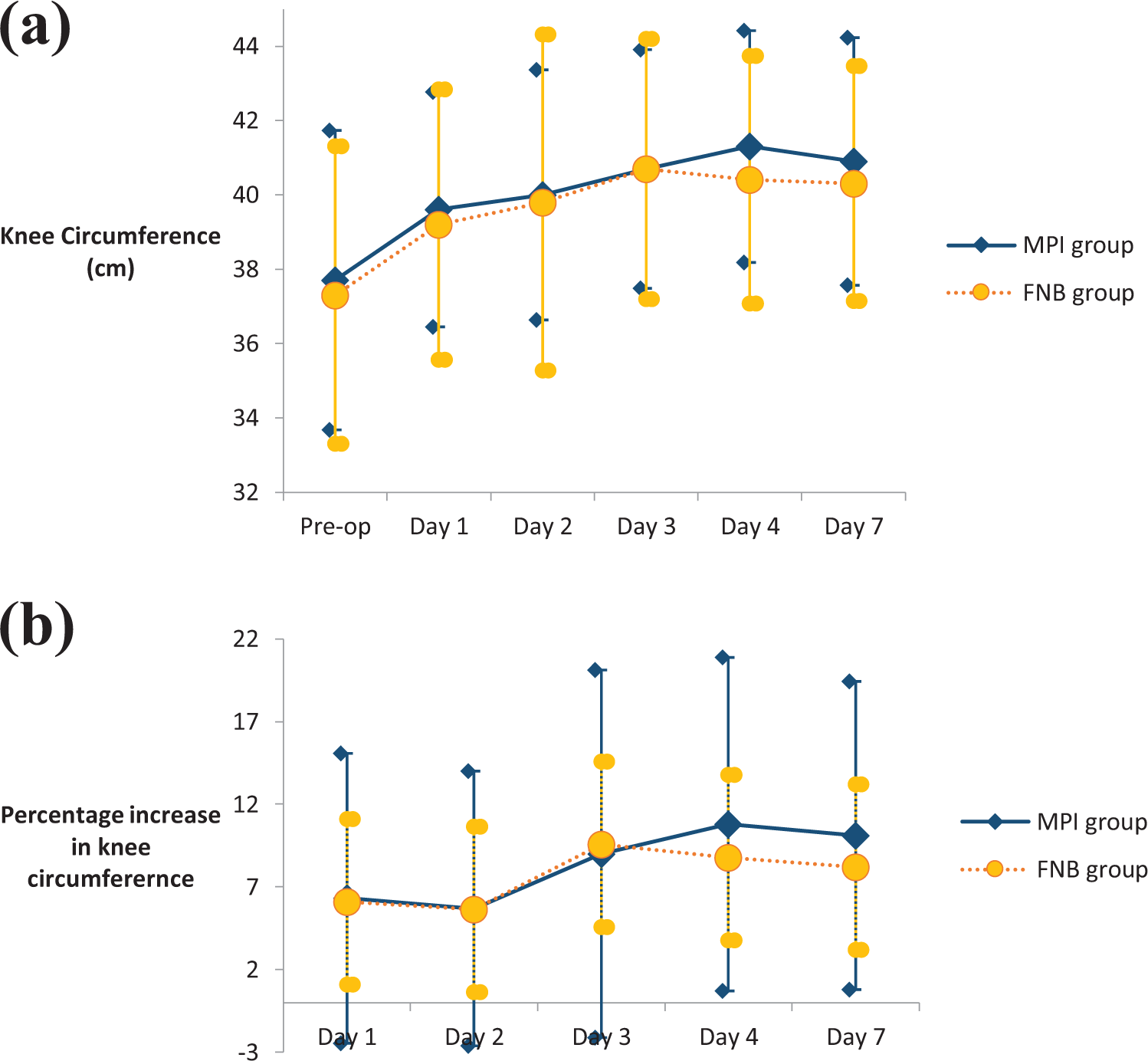
(a) KC in centimeters: preoperative, postoperative days 1–4, and day 7. (b) Percentage increase in KC. KC: knee circumference.
Pain control
As shown in Figure 5, the case group had a significantly lower VAS score on motion than the control group on postoperative day 1 (p = 0.000). There were no significant differences between groups for VAS scores at rest and VAS scores on motion on postoperative days 2–4 and 7. In Figure 6, average PCA consumption over 24 hours was 12.8 mg for the MPI group and 20.0 mg for the control group, and this difference was statistically significant (p = 0.040).
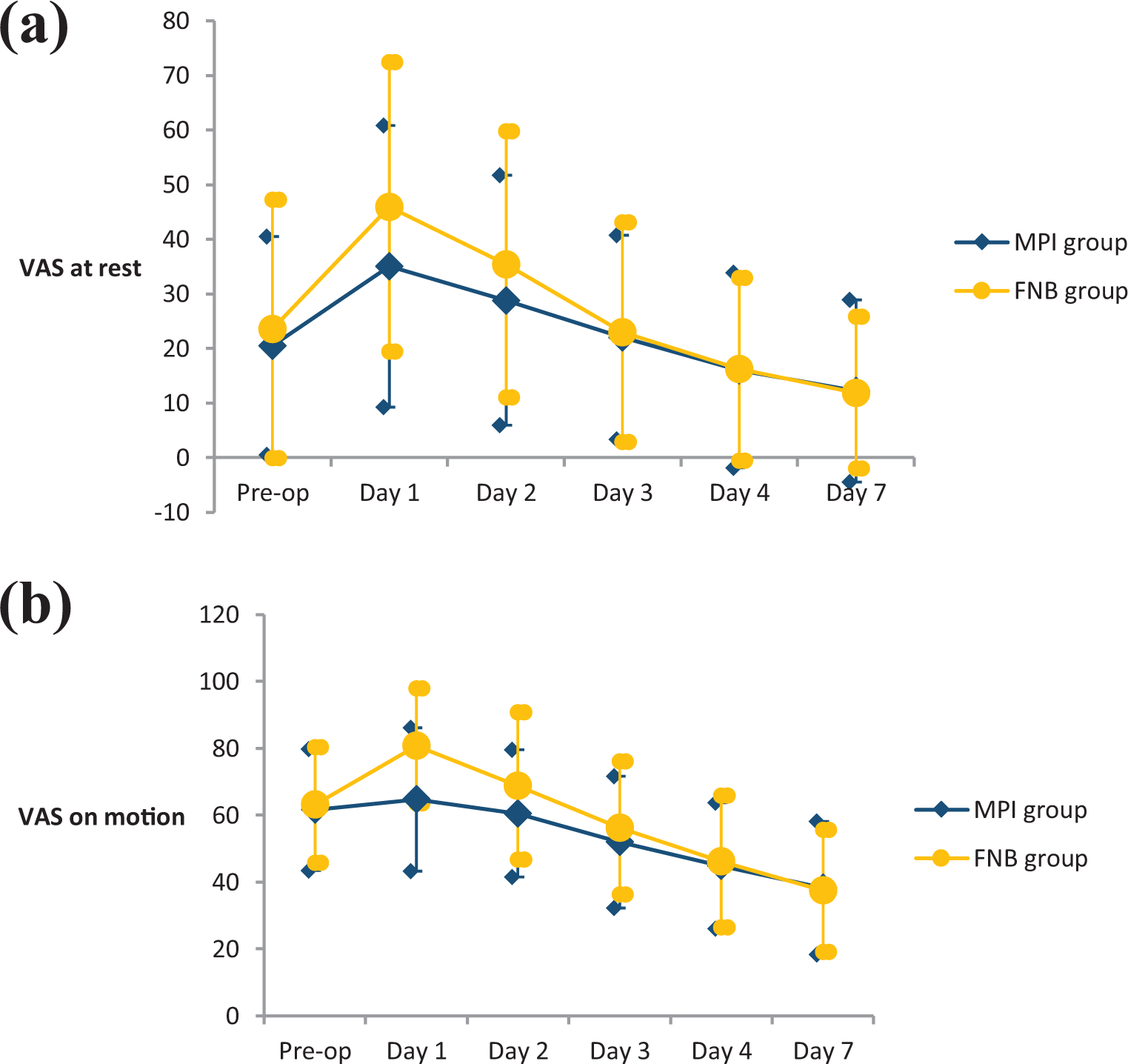
VAS for pain measure: preoperative, postoperative days 1–4, and day 7. (a) VAS at rest. (b) VAS on motion. Statistically significant difference was noted for VAS on motion on day 1. VAS: visual analog scale.
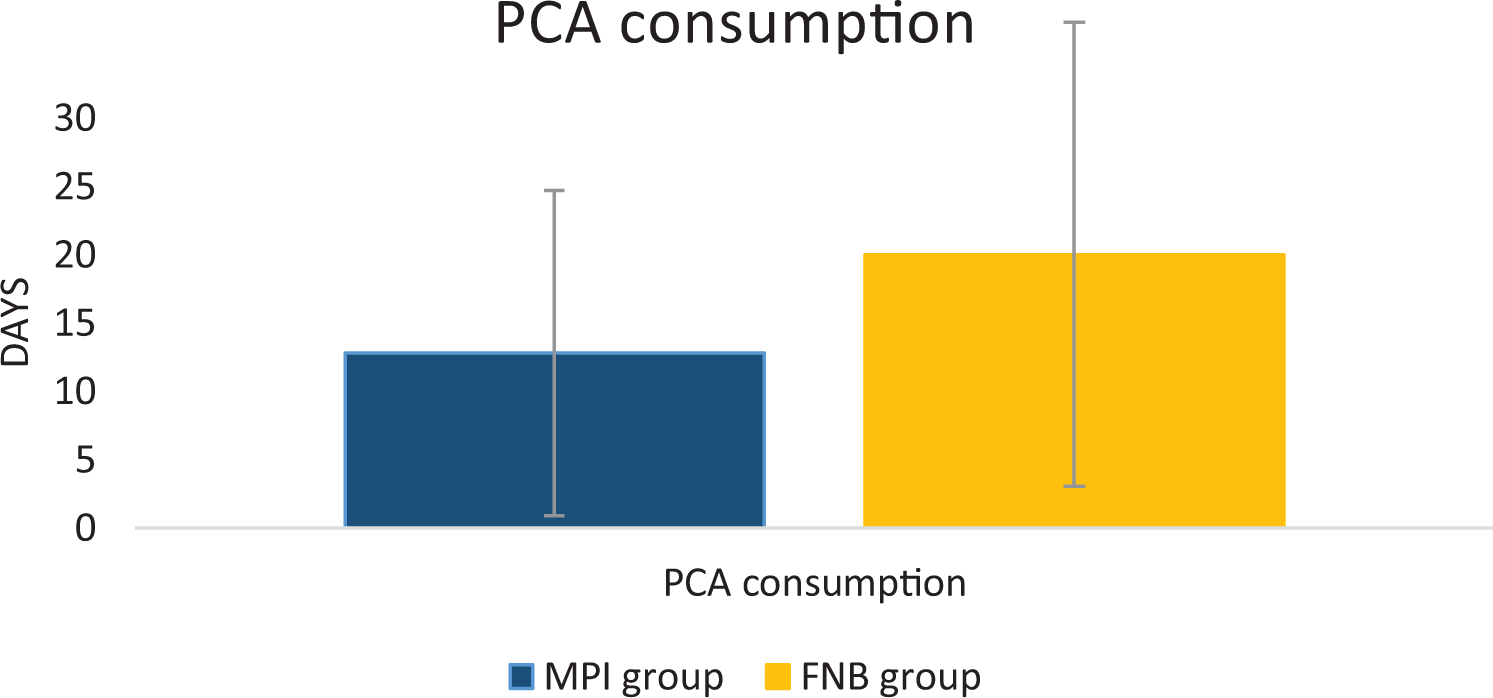
MPI group had a lower postoperative PCA consumption than FNB group, which showed statistical significance. MPI: multimodal periarticular analgesic; FNB: femoral nerve block; PCA: patient-controlled analgesia.
Discussion
Total knee arthroplasty significantly reduces mechanical pain in advanced knee osteoarthritis. Nevertheless, inpatient functional rehabilitation can be delayed due to postoperative pain and swelling. Currently, there are two common methods of perioperative pain control. The recent trend in favor of MPI over FNB is attributable to MPI’s quadriceps-sparing effect, as FNB can cause motor paralysis of the femoral nerve leading to quadriceps impairment. 4
A number of studies have demonstrated equivalent pain control of both MPI and FNB methods. However, these investigations focused mainly on pain control, which were initiated by anesthetists, 2 –4 and lacked description of soft tissue condition and functional outcome during in-hospital stays. The most common description of functional assessment was quadriceps function via SLR. For example, several kinds of research reported better SLR on days 1–2, 10 –13 which is in accordance with our findings of better knee extension power on day 1. In addition, although knee functional recovery was measured by ROM and knee flexion in some studies, these ranges were assessed after patient discharge. A significant difference was found by Fu et al. at postoperative 15 days, 10 while no differences were identified by Joo et al. 14 and Busch et al. 15 at 2 and 6 months postsurgery, respectively. Furthermore, in two of our local studies, the primary outcome measure focused primarily on pain relief via 42- to 72-hour morphine consumption. 16,17
Our study included a comprehensive assessment by surgeons, nurses, and allied health professionals. MPI delivered the benefit of reduced length of hospital stay, which is consistent with some investigations, 13 but not others. 15 In our study, the length of stay was reduced by 2.3 days. Length of stay can be influenced by multiple factors, including physical, psychological, and social factors. Our study was constrained by a lack of assessment of psychological and social factors. Concerning the physical factor, however, we observed a more rapid patient rehabilitation journey, reflected by a statistically significant reduction of MFAC-5 by 1.94 days, due to improved pain control and better quadriceps recovery. Despite a shorter patient journey, indicative parameters upon discharge, including Insall knee score, MFAC, quadriceps power, and combined ROM, were equivalent in both groups. This demonstrated that patients had achieved optimal recovery prior to discharge, following a standardized discharge protocol.
Additionally, in our study, no wound complications occurred in both groups. Although knee swelling was significant throughout the first postoperative week, the MPI group did not exhibit a significant effect on knee swelling. Moreover, for both the case group and the control group, VAS at rest returned to baseline at approximately day 3 and VAS on motion at day 2.
Pain was assessed as a secondary outcome measure. In our study, 24-hour PCA consumption and VAS upon motion on day 1 favored the use of MPI over FNB. Indeed, both observations concur with other local 16,17 and overseas investigations. 13,15 The analgesic effect of MPI is more pronounced because of its extensive coverage to the knee soft tissues. FNB injection, on the other hand, focuses only on the anterior aspect of the knee, which is innervated by the femoral nerve. As a consequence, the posterior aspect of the knee, which is innervated by the tibial nerve, remains unblocked.
Certain limitations exist concerning this prospective randomized control trial study. Firstly, since the operations were performed by different surgeons, variation of surgical and injection techniques may have affected postoperative pain control, rehabilitation, and final surgical outcome. Secondly, data collection was carried out by different medical officers in-charge instead of a single investigator. Consequently, even though the data collection methods were standardized, some interobserver variation may have been inevitable. Thirdly, the psychological and social status of the patients, which might have influenced the length of stay, were not taken into account. Fourthly, the patients were blinded in the study, but the chief operating surgeon was not. Therefore, bias could not be avoided since this is a single-blinded study.
Conclusion
The current study demonstrated that MPI delivers a more rapid inpatient rehabilitation journey compared to FNB, ascribed to MPI’s superior quadriceps power return and pain relief, especially in the first few postoperative days. Overall, MPI constitutes a safe procedure and possibly contributes to a shorter hospital stay for patients undergoing total knee arthroplasty.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.