
Abstract
Hydrogen peroxide (H2O2) is a commonly used chemical agent in orthopaedic practice for antisepsis, haemostasis and preparation of bone bed for cementation. However, the associated risks of H2O2 usage are not widely known. We report a case of suspected air embolism after use of H2O2 during drainage of a septic arthritis of the shoulder.
Upon our literature review, we were able to demonstrate H2O2 to be beneficial in antisepsis and care of chronic wounds. However, it has not been proven to be superior to other antiseptics commonly used in orthopaedic surgery. Regarding its use in cementation, there is evidence to show it is more effective than saline however, the use of pulsatile lavage appears to be the most important factor affecting the quality of cementation. H2O2 has not been shown to be helpful with haemostasis. Prior to the use of H2O2, one should be cautious and understand its associated risks and precautions.
Introduction
Hydrogen peroxide (H2O2) is commonly used in our daily orthopaedic practice because of its antiseptic and haemostatic effects. Common examples include incision and drainage, debridement and preparation of bone bed during cementation procedure. 1 However, despite its common use, its potential risks are often overlooked. We report a case of subcutaneous emphysema and suspected air embolism to illustrate the risks associated with the use of H2O2 and discuss the potential benefits and disadvantages of H2O2 in orthopaedics.
Case report
A 71-year-old lady with a history of carcinoma in the left breast 20 years ago and currently in remission was admitted for left shoulder pain with swelling for 2 days. Upon initial examination, she was afebrile. However, her left shoulder joint was swollen with marked pain and had limited motion. Her white cell count was normal, and X-ray of her left shoulder revealed no osteomyelitis or gas collection (Figure 1). In view of these findings, we performed a left shoulder arthrocentesis, and the joint fluid was mildly turbid. Urgent Gram smear revealed the presence of Gram-positive bacteria, and the definitive culture in both the joint fluid and blood yielded methicillin-sensitive Staphylococcus aureus. Her computed tomography (CT) showed a rim enhancing collection over her left shoulder joint with multiple air pockets in the joint space which was suspicious of septic arthritis with concomitant osteomyelitis (Figure 2). In view of these findings, shoulder arthroscopy was performed with 40 mL of pus drained. Penicillin group antibiotics was then started in accordance to the culture sensitivity results.

X-Ray of the left shoulder upon admission.
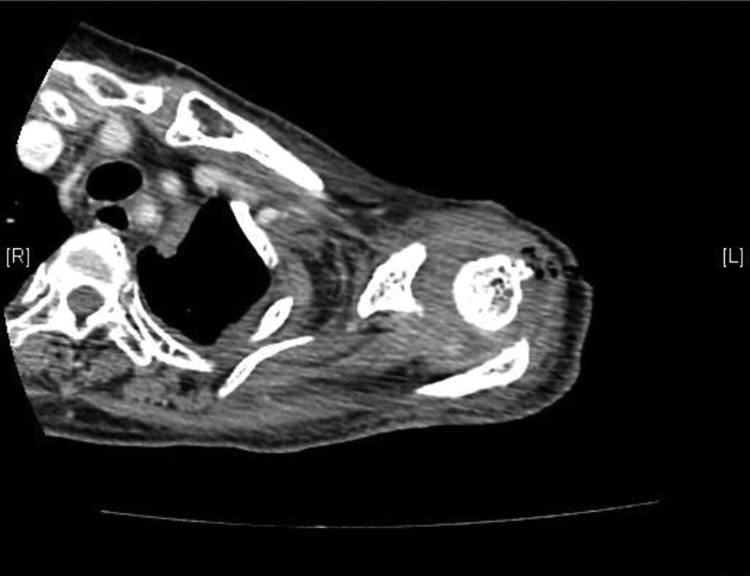
Computed tomography (CT) showing collection over the left glenohumeral joint.
Her subsequent treatment required prolonged antibiotics and repetitive debridement due to persistent signs of infection including fluctuating fever, elevated inflammatory markers, continual pus discharge and findings of residual collection on serial imaging.
Upon her last debridement, persistent loculation and turbid fluid was found within her shoulder joint. After adequate drainage and debridement, the wound was irrigated with H2O2 (Banitore hydrogen peroxide solution) using a syringe. During H2O2 irrigation, the patient’s blood pressure suddenly dropped to 50/30 mmHg with a heart rate of 70 beats/min. There was also an associated loss of end tidal CO2. Her electrocardiogram (ECG) was initially unremarkable, however she rapidly developed pulseless electrical activity with cardiopulmonary resuscitation initiated and return of spontaneous circulation 1 minute later. Post-operatively, she was transferred to our intensive care unit (ICU) for further care.
Post-operatively, her blood gas showed metabolic acidosis with a pH of 7.27, her lactate was elevated at 3.4 mmol/L (normal value 0.7–2.1 mmol/L). Cardiac workup showed a mildly elevated troponin level of 46.4 ng/L (normal value <14ng/L), however serial ECG did not show any evidence of arrhythmia, myocardial infraction or pulmonary embolism. Moreover, bedside echocardiogram showed a mildly dilated right ventricle with a preserved ejection fraction of 50% with no gas bubbles detected in the cardiac chambers, and there were no features to suggest myocardial infarction or ischaemia. CT pulmonary angiogram was performed, which revealed a small right upper lobe subsegmental thrombus pulmonary embolism with a large amount of subcutaneous emphysema over the left shoulder (Figure 3).

Computed tomography (CT) showing subcutaneous emphysema over the left shoulder and a small right upper lobe subsegmental thrombus pulmonary embolism.
Based on the history and clinical findings, our intensivist managed the patient with the working diagnosis of air embolism. She later developed multi-organ dysfunction and was placed on inotropic support, temporary haemodialysis and ventilator support. Her vitals and blood parameters later improved, and she was able to wean off life support 2 days after admission to ICU.
She was eventually discharged to the general ward with continual management of her residual left shoulder wound with intravenous antibiotics and wound dressing. Her inflammatory markers normalized after 6 weeks of antibiotics and her wound eventually healed after a bedside excision of the residual sinus tract at 3 months after discharge from ICU.
Discussion
Despite gas bubbles were not detected from our patient’s echocardiogram and CT, our anaesthetist and intensivist had felt that the cause of this patient’s intraoperative deterioration was most likely air embolism as a result of administration of H2O2 based upon the timing of events and the presence of subcutaneous emphysema on her post-operative CT. Another possibility that can account for her sudden deterioration includes pulmonary embolism by thrombus. However, this is unlikely since the thrombus on the CT was small and only occluded a single peripheral artery. Commonly, a major trunk of the pulmonary vasculature has to be occluded by a large thrombus to trigger a cardiac arrest. Furthermore, such cardiac arrest by thrombus occlusion is unlikely to revert as quickly as in our case due to the time required for thrombus resolution. 2 One can argue that a primary cardiac event (not a result of air embolism or thrombus pulmonary embolism) could be accountable for her deterioration based on her troponin elevation, however we must note that she had a relatively normal ECG and echocardiogram thus making it unlikely.
Application of H2O2 to human tissue causes it to rapidly decompose into oxygen and water. 2 –5 It has been reported that as little as 1 mL of 3% H2O2 can release up to 10 mL of oxygen. 4

Infection
It is theorized that H2O2 exerts its antiseptic effect via its cytotoxic effects to bacteria and also mechanical removal of debris when oxygen bubbles are formed. 1,2,6 It has been shown to be especially potent against Gram-positive organisms and bacteria without catalase; it has been reported to be effective in the reduction or even complete removal of bacterial biofilm. 1,6 H2O2 acts in a synergistic manner with other commonly used antiseptics such as chlorhexidine and povidone iodine. 1,6 Despite prior evidence to date, there is still no trial comparing the antiseptic efficacy of H2O2 versus other types of commonly used antiseptic agents.
Wound healing
H2O2 has been shown to be helpful in the treatment of chronic wounds. Mohammadi et al compared the skin graft uptake and healing rates in chronic infected burn wounds with or without the use of H2O2. He showed debridement of chronic infected burn wounds followed by intraoperative H2O2 dressing and then skin grafting was statistically superior to debridement with skin grafting alone. In his cohort of 98 limbs, none showed any irritative dermatitis. It has also previously been shown that H2O2 stimulates angiogenesis, thus promoting healing. 7
Bone cementation
Classically, H2O2 has also been used for bone bed preparation prior to cementation. It is thought that its ability to mechanically remove debris (fats, marrow and blood clots) and haemostasis allows cement to interdigitate deeper and thus better quality of cementation. 8 Ackland conducted a study comparing the quality of cementation using different methods of femoral canal preparation; he used pulsatile lavage followed by H2O2 gauze packing, pulsatile lavage with saline, H2O2 gauze packing alone or saline irrigation alone. He was able to show that pulsatile lavage alone regardless of whether it was with or without H2O2 had the most significant effect on the quality of cementation. Interestingly, in his study, he noted that the pull out force of the cemented stem in the H2O2 gauze packing group was more than that of the saline irrigation group (2017.9 N versus 947.1 N), but it was not statistically significant. 8
Haemostasis
With regard to haemostatic effect in dogs, Hankin et al. compared the blood loss of per unit area of trabecular bone in bones which were treated with either gauze soaked in H2O2 or saline. He calculated blood loss by weighing how much blood was soaked up from the trabecular bone after exposure of H2O2 or saline and divided it against the cross-sectional area of the bone. He concluded that there was statistically significant decrease in blood loss in those treated with H2O2. 9 To date, no one is certain by what mechanism H2O2 exerts its haemostatic effect. 9
Bannister uses a similar method of calculating blood loss as Hankin et al., however he performed his study on human subjects undergoing total hip replacement. He concluded that H2O2 was not superior to room temperature saline in haemostasis. 3 Another controlled trial performed by Chen et al. in humans comparing transamine, H2O2 and saline wash in total knee replacement failed to show any significant difference in the post-operative haemoglobin level and total blood loss between the saline and the H2O2 groups. 10 The haemostatic benefits of H2O2 in humans are doubtful.
Risks
Despite its benefits in antisepsis and care of chronic wounds, prior literature has shown the potential risk of intraoperative use of H2O2. Cases of subcutaneous emphysema, pneumocephalus, air embolism, respiratory and cardiac arrests have been reported. 2,4 Patients with cardiac shunts (foramen ovale, atrial or ventricular septal defect) are at even higher risk of air embolism resulting in lethal cardiac or respiratory events. 5 Prior authors have cautioned the use of H2O2 in confined spaces due to increased risk of air embolization. 1,2,4 It is believed that the sudden production of gas in an enclosed area results in increased pressure, thereby forcing gas into the blood stream. This situation can be worsened if the enclosed area has poor haemostasis, providing easy access of gas into the circulatory system. 4
Air embolism from H2O2 may occur during application of H2O2 or when the limb tourniquet is removed allowing gas bubbles to reach the systemic circulation. If air embolism involves the limb, it will present with features of acute limb ischemia; if the pulmonary circulation is involved, there may be a drop in blood pressure associated with decrease in end tidal CO2 and respiratory or cardiac arrest. Multi-organ failure can occur due to the ischaemic insults from the blocked vessels as seen in our patient. 4
In the event of air embolization, immediate treatment by the orthopaedic surgeon involves cessation of H2O2 irrigation, suction of the gas bubbles and application of saline to dilute and minimize the gas-producing chemical reaction. 4 If the episode of embolism occurs after the release of the tourniquet, the tourniquet should be reinflated immediately to prevent further dissipation of gas bubbles into the systemic circulation. 5 Anaesthetic management should include discontinuation of nitrous oxide, as this has shown to increase the gas bubble up to fourfold in size 5 and to immediately institute 100% oxygen therapy. 4 The patient should be placed in a left lateral recumbent head down position (Figure 4) to prevent gas bubbles from entering the pulmonary circulation. This position also facilitates the placement of a central line to aspirate the gas bubbles in the pulmonary circulation of right heart. 4

Left lateral recumbent head down position.
Conclusion
H2O2 is effective as an antisepsis and in treatment of chronic wounds that may require skin grafting. However to date, there are no studies showing H2O2 to be superior to other commonly used antiseptics.
If H2O2 is used, several precautions should be undertaken such as avoiding its use in the following situations: confined spaces, areas with significant bleeding or poor haemostatic control. If H2O2 were to be used in a wound bed just prior to wound closure, it needs to be rinsed away quickly after its application, placement of a drain prior to wound closure for gas decompression should be considered, and the patient should be monitored closely intraoperatively and post-operatively. 1
H2O2 should not be used for its haemostatic property as its efficacy in humans remains doubtful and the existing bleeding channels provide a portal by which gas can enter into the circulatory system. During femoral canal preparation prior to cementation, the surgeon may opt to use isolated pulsatile lavage with saline rather than H2O2 to improve cementation quality. It has been suggested that oxygen liberated from H2O2 may be forced into vasculature during cementation and pressurization. 1
It is important for orthopaedic surgeons to observe safety principles regarding the use of H2O2 intraoperatively. Orthopaedic surgeons should be well versed in the risks and the acute management of H2O2-associated air embolism. Good communication between the orthopaedic surgeon and the anaesthetist is key in the safe use of H2O2.
In conclusion, H2O2 is beneficial as an antiseptic and in treatment of chronic wounds; however, it has yet been shown to be more effective than other commonly used antiseptics. Thus, given the potential risks, one may consider using alternative antiseptics. H2O2 has been shown to be more effective than saline in cementation, but the use of pulsatile lavage seems to be the most important determining factor in the quality of cementation rather than the solution used. The use of H2O2 can result in devastating complications if precautious are not observed.
Footnotes
Authors’ Note
Tao Sun Tycus Tse is now affiliated to Department of Orthopaedics and Traumatology, Pamela Youde Nethersole Eastern Hospital, Chai Wan, Hong Kong.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.