
Abstract
Background/Purpose:
Chronic symptoms related with hip osteoarthritis (OA) can negatively affect health-related quality of life (HRQoL). The purpose of this study was to examine factors related to a HRQoL measure that considers an Asian lifestyle in Japanese patients with hip OA.
Methods:
Forty-seven female subjects participated. The dependent variable was the Japanese Orthopaedic Association Hip Disease Evaluation Questionnaire (JHEQ), which assessed HRQoL. Potential factors were measured as independent variables. After screening, potential variables were entered into a multiple regression analysis to determine which variables were related to HRQoL.
Results:
In the regression model, knee extension muscle strength on the unaffected side and hip flexion range of motion (ROM) on the affected side were associated with HRQoL. Higher strength and higher ROM were related to greater HRQoL.
Conclusion:
Results can help health-care providers develop appropriate rehabilitation programs for improving HRQoL in patients with hip OA.
Introduction
Hip osteoarthritis (OA) is a common musculoskeletal condition, and the prevalence of hip OA in the general population is 2.4% in Japan, 4.7% in France, and 10.1% in the United Kingdom. 1,2 Patients with hip OA typically develop hip pain, joint stiffness, and muscle weakness over months to years rather than acutely. 3 These chronic symptoms can negatively affect health-related quality of life (HRQoL) in these patients. 4,5
In rehabilitation clinical practice and research, HRQoL is an important outcome and is measured frequently. A previous study found that HRQoL of patients with hip OA was related to patient satisfaction after total hip arthroplasty (THA). 6 Loza et al. 7 examined the direct and indirect OA-attributable costs in 1071 patients with OA and demonstrated that worse HRQoL scores, as assessed by the Western Ontario and McMaster Universities Osteoarthritis index (WOMAC), related to higher total medical costs. Furthermore, age, radiological severity, contralateral hip OA, low back pain (LBP), leg length discrepancy (LLD), hip pain, range of motion (ROM), strength, and walking ability were previously shown to be related to HRQoL in patients with hip OA and/or THA. 8 –12 However, most studies were completed in Western countries, and it is unclear whether results can be generalized to non-Western countries since HRQoL may reflect the lifestyles of each country, region, or culture.
Factors that relate to HRQoL in Asian patients compared to Western patients with hip OA may differ due to cultural differences. For instance, squatting position or sitting on the floor is an important part of many Asian cultures. Fujita et al. 13 revealed that Japanese patients who underwent THA had difficulty performing postures requiring deep hip flexion and these movements related to their HRQoL. However, few studies have examined factors that relate to HRQoL measures that include important aspects of Asian lifestyle in patients with hip OA. Therefore, the objective of this cross-sectional study was to examine factors related to a HRQoL measure that considers an Asian lifestyle in Japanese patients with hip OA. We hypothesized that hip ROM would be significantly related to the HRQoL since substantial hip ROM is required for squatting, which is an important position for Asian lifestyle.
Methods
Study design and subjects
The cross-sectional study was conducted in a hospital in Kurashiki City, Japan. Data were collected between August 2015 and August 2016. Subjects with hip OA scheduled for a THA were recruited. Hip OA was diagnosed based on the guidelines proposed by the Japanese Orthopedic Association’s committee of medical doctors. 14 This study recruited only females because the incidence of hip OA is higher in female than in male. 1,2 Exclusion criteria included under 50 years of age, rheumatoid arthritis, neurological problems, cancer, and previous THA or hip osteotomy. The study complied with the principles of the Declaration of Helsinki and was approved by the institutional review board of the authors. Subjects provided written informed consent.
Dependent variable
HRQoL was the dependent variable. The Japanese Orthopaedic Association Hip Disease Evaluation Questionnaire (JHEQ) was used to asses HRQoL. The JHEQ is a patient-reported outcome measure that includes questions concerning common Asian-lifestyle movements, such as using a squatting pan toilet or getting up from the floor; both movements require deep flexion of the hip joint. 15 The JHEQ consists of pain (seven questions, 28 points), movement (seven questions, 28 points), and mental (seven questions, 28 points) subscales, with higher scores indicating a better HRQoL (maximum 84 points). In this study, the composite measure of JHEQ was used for analyses. A previous study demonstrated that the JHEQ was a reliable and valid tool for evaluating hip diseases. 16
Independent variables
Independent variables were selected because they have previously demonstrated a relationship to HRQoL in patients with hip OA or after THA. 8 –12 Age was recorded from medial charts. The radiological severity of developmental hip OA was assessed using the disease stage of hip OA proposed by the Japanese Orthopedic Association’s committee. 14 This stage is classified into one of the four stages (i.e. pre-OA stage, initial stage, advanced stage, and terminal stage). All subjects had either advance or terminal stage severity since subjects were undergoing THA. Hips were classified as advanced stage with partial disappearance of the joint space and evidence of cystic radiolucencies and osteophytes (coded as 0). Terminal stage was classified when almost a total disappearance of the joint space and marked osteophyte formation (coded as 1). Previous study indicated good inter- and intra-observer reliability of this measurement method. 17 Contralateral hip OA was assessed using X-ray by medical doctors and subjects who had bilateral hip OA were coded as 1. For the presence of LBP, subjects were asked “do you feel LBP now, please answer as the presence or absence of LBP.” Subjects with LBP were coded as 1. To avoid measurement bias, we excluded possible confusion between LBP and hip pain by palpation of painful areas in each subject. LLD was measured using anteroposterior X-ray in a standing position. The LLD was defined as the difference in the perpendicular distance in millimeters between a line passing through the lower edge of the teardrop points and the tip of the lesser trochanter. This measurement method has been demonstrated to show high reliability. 18 Hip pain was measured using the visual analog scale (VAS) after subjects walked 10 m. A systematic review 19 revealed that VAS was applicable for unidimensional assessment of pain intensity in most settings. The subjects were given the following standard instruction: “please rate your hip pain after you walk 10 m, 0 would mean no pain and 10 would mean worst possible pain.” If subjects had bilateral hip OA, the side with the greater pain intensity was considered as the study limb.
Body functions such as hip and knee muscle strengths, hip ROM, and walking ability were also measured as independent variables. Bilateral maximum muscle strength was assessed using a hand-held dynamometer (µTas F1, ANIMA, Japan) with a fixed band during isometric contraction for hip flexion, extension, abduction, and knee extension. Subjects completed two repetitions for each direction, and contractions were held for 3 s. The force sensor was placed at 5 cm from the distal end of the segment. Torque was calculated by multiplying force by the lever arm (distance between the force sensor and the center of the groin for hip flexion, the ischial tuberosity for hip extension, the greater trochanter for hip abductor, and the level of the tibial plateau for knee extension). Torque was expressed as a percentage of body weight (Nm/kg), and the average of the two trials was determined. These measurement methods have been demonstrated to show high reliability in a previous study. 20 Bilateral ROMs were measured for hip flexion and extension, based on the method described by Norkin and White, 21 with a goniometer in 5° increments. Subjects were instructed to lie supine on a treatment table with their hips and knees straight and arms folded beside their trunk for measurement of hip flexion. To measure hip extension, subjects were instructed lie prone position. If the hip extension ROM did not reach 0°, they were instructed to lie on their side to measure hip extension. Walking ability was assessed using the 10 m walking speed (10 mWS) test at maximal speeds in a long corridor with a flat surface. The 10 mWS was chosen because previous studies found that 10 mWS was related to activities of daily living in patients with hip OA. 22 The 10 mWS consisted of a 20-m liner walking path with a 5-m acceleration zone, a central 10 m timed zone, and a final 5 m deceleration zone. The 10 mWS started from the moment the subject’s lower limb crossed the starting line in the central timed zone and ended when the subject crossed the end line. The subjects were given the following standard instruction: “walk as fast as you can to the 20 m line.” Subjects were allowed to use walking assistive devices during this measurement. The 10 mWS was conducted twice and the faster value was utilized in analyses and expressed in m/min.
Statistical analysis
Descriptive statistics were calculated for the variables. Independent t-tests compared JHEQ score between the unilateral and the bilateral hip OA, between the subjects with and without LBP, and between the advanced stage and the terminal stage. Pearson correlation coefficient examined bivariate relationships between variables. In accordance with previous studies, 23,24 each independent variable was subjected to an initial screening of its relationship with the dependent variable using analyses such as t-test and Pearson correlation. The level of significance was set at p < 0.20 to ensure that the independent variables were included at this stage. 25 In addition, the variables that showed multicollinearity among the independent variables were excluded from the independent variables. As the results of these screenings, eight independent variables (hip pain, hip flexion ROM on the affected side, and bilateral muscle strengths of hip flexion, hip extension, and knee extension) were chosen as the potential variables for entering the multiple regression analysis model. Potential variables were entered into a multiple regression analysis with backward stepwise selection method to determine the most accurate set of variables for the relationship of JHEQ. Regression coefficients with 95% confidence intervals and associated t-test, and standardized coefficients were examined. To examine the appropriateness of the regression analyses, residuals were examined for normality, variance inflation factors (VIFs) were used for judging multicollinearity among independent variables of the model and the Durbin–Watson ratio was used for autocorrelation in the model. All statistical analyses were conducted using SPSS version 25 software for Windows, and the significance level was set at p = 0.05.
Sample size
The α value was set at 0.05, and the power was set at 0.80. Based on a previous study, 9 the hypothesized explained variance adjusted for the degrees of freedom (R 2 ) was 0.43. Consequently, it was estimated that total 43 cases were required in this study for the 8 potential variables. 26
Results
A total of 47 female subjects participated in this study. Baseline characteristics of the subjects are listed in Table 1. The mean JHEQ score was 25.6 points, and its maximum value was 76 points. There were no significant differences in JHEQ score between contralateral and bilateral hip OA (p = 0.48), between with and without LBP (p = 0.37), and between advanced stage and terminal stage severity (p = 0.67). The JHEQ was significantly correlated with hip flexion ROM on the affected side, bilateral hip flexion and abduction muscle strength, bilateral knee extension muscle strength, and hip extension muscle strength on the affected side (Table 2).
Values of the measured variables (n = 47).
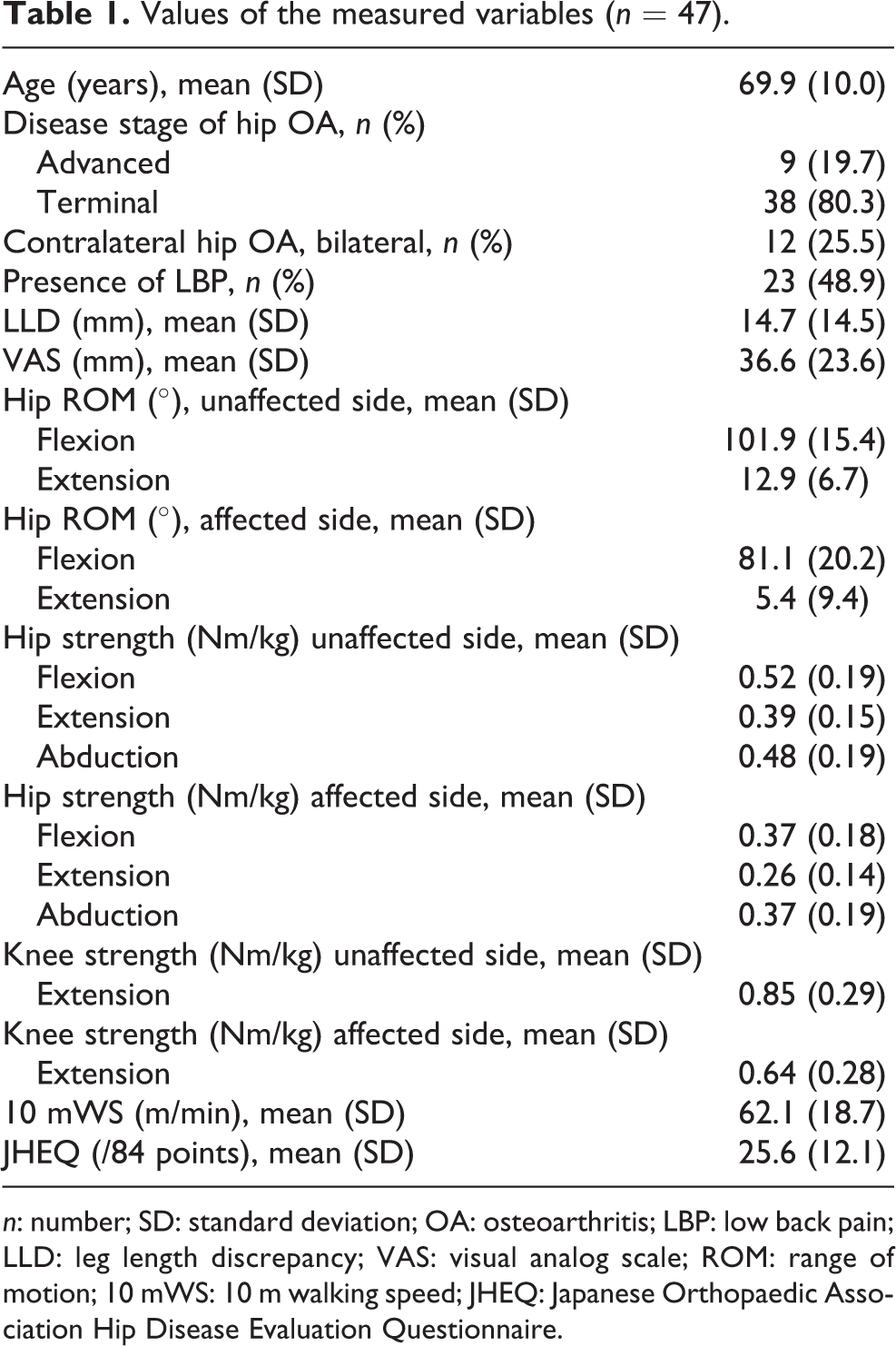
n: number; SD: standard deviation; OA: osteoarthritis; LBP: low back pain; LLD: leg length discrepancy; VAS: visual analog scale; ROM: range of motion; 10 mWS: 10 m walking speed; JHEQ: Japanese Orthopaedic Association Hip Disease Evaluation Questionnaire.
Pearson coefficients for correlations between JHEQ and other factors.
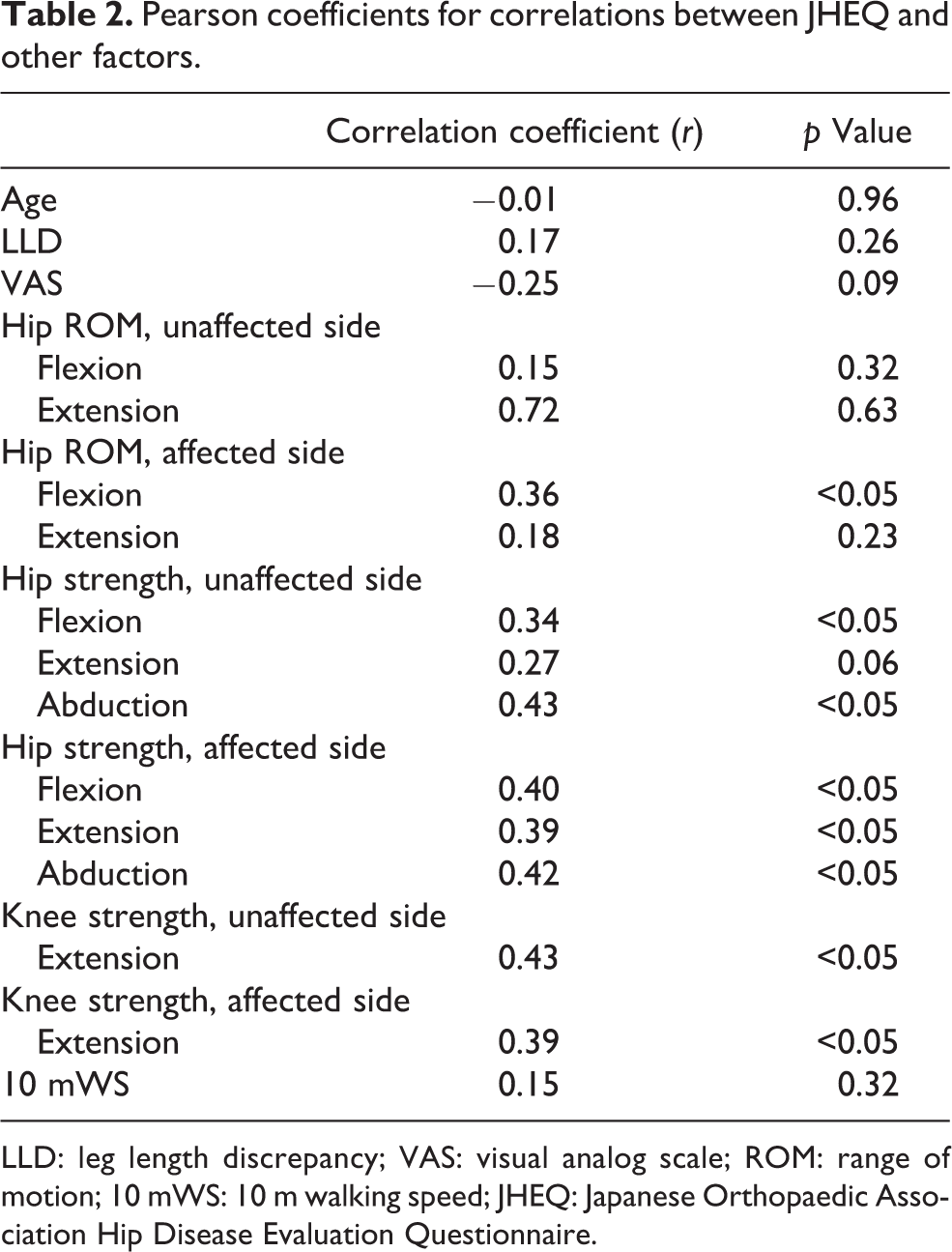
LLD: leg length discrepancy; VAS: visual analog scale; ROM: range of motion; 10 mWS: 10 m walking speed; JHEQ: Japanese Orthopaedic Association Hip Disease Evaluation Questionnaire.
Results for the regression analysis explaining the variance in JHEQ are available in Table 3. In the regression model, knee extension muscle strength on the unaffected side (standardized partial regression coefficient: β = 0.37) and hip flexion ROM on the affected side (β = 0.28) were associated with JHEQ. Higher JHEQ scores (greater HRQoL) were associated with higher hip flexion ROM and higher knee extension strength. All assumptions for regression analysis were met, and the analysis were deemed appropriate. Residual was normally distributed. The VIF of above model was 1.052, and it was judged that there was no significant multicollinearity in the model. The Durbin–Watson ratio of the above model was 1.900. There was no autocorrelation in the sample.
Result of the multiple regression analysis.
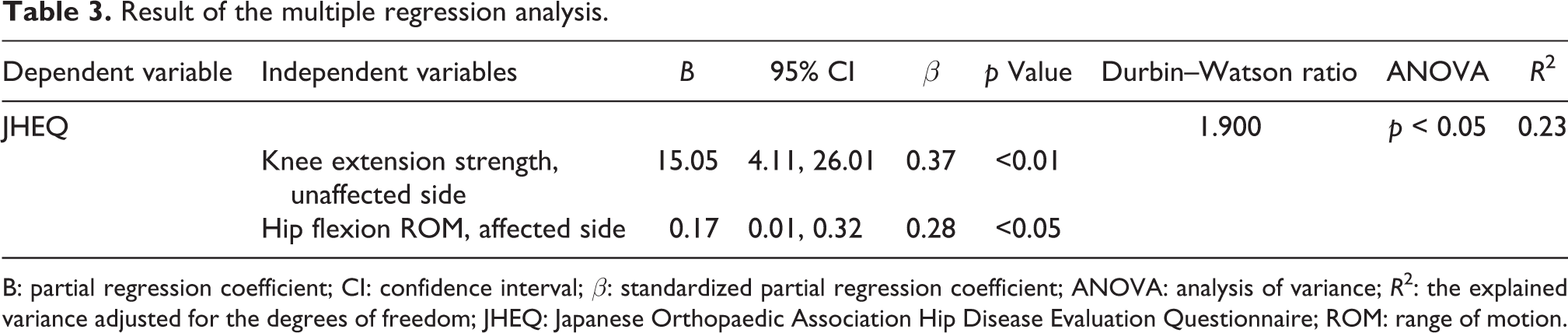
B: partial regression coefficient; CI: confidence interval; β: standardized partial regression coefficient; ANOVA: analysis of variance; R 2: the explained variance adjusted for the degrees of freedom; JHEQ: Japanese Orthopaedic Association Hip Disease Evaluation Questionnaire; ROM: range of motion.
Discussion
This study examined factors associated with HRQoL in Japanese patients with hip OA. Higher knee extension muscle strength on the unaffected side and higher hip flexion ROM on the affected side were related to higher HRQoL scores. To the best of our knowledge, this study is the first to examine factors related to a HRQoL, measure (JHEQ) that considers Asian lifestyle in Japanese patients with hip OA. Result can be used to support health-care providers to develop appropriate rehabilitation programs for improving HRQoL in patients awaiting THA.
Knee extension muscle strength on the unaffected side was most strongly related to HRQoL. This factor was significant because JHEQ reflected an Asian lifestyle which requires squatting or sitting on the floor. Findings are similar to a previous study, 12 which found significant relationships between knee extension muscle strength and self-report physical function assessed by the Short Form 36 in patients with hip OA. Squatting and sitting on the floor require substantial knee extension strength and patients with hip OA have diminished knee extension muscle strength on the affected side (Table 1). Thus, patients with hip OA may compensate with their unaffected leg to perform these movements. Findings suggest that interventions that target knee extension strengthening may be effective in improving HRQoL in patients with hip OA. In support, Foley et al. 27 showed that three exercise sessions a week for 6 weeks, which included knee extension muscle strengthening, improved HRQoL in patients with OA. Therefore, ensuring patients improve muscle strength is an important part of hip OA management.
Hip flexion ROM on the affected side was also significantly associated with HRQoL. A previous study 28 showed that hip flexion ROM correlated with the WOMAC scores, but no previous study has investigated a significant relationship with JHEQ. Hip flexion is required for daily activities such as squatting or sitting on the floor, particularly for Asian older adults who still prefer the floor for most of their activities of daily life. Mulholland and Wyss 29 investigated the hip ROM required for movement on the floor and found that hip flexion ROM of 110° was required for sitting cross-legged and 130° for squatting. In our study, the mean hip flexion ROM on the affected side was 81.1°, which is much less than what is required for those aforementioned tasks. Thus, it is not surprising that hip flexion ROM was associated with the JHEQ since this HRQoL measure includes questions concerning movements that require substantial hip flexion, such as using a squatting pan toilet or getting up from the floor.
This study had several limitations. Firstly, only 23% of the variance in JHEQ was accounted. Other factors, such as medical interventions (e.g. medications and rehabilitation), should be considered in future studies. Secondly, this study was cross-sectional, and the results should be confirmed in longitudinal designs. Finally, only females with advanced and terminal stage hip OA were recruited and the sample size was small which limits generalizability. Results should be confirmed in larger samples that include males and patients with less severe hip OA.
In conclusion, our results suggest that higher knee extension muscle strength on the unaffected side and hip flexion ROM on the affected side were associated with higher HRQoL in Japanese patients with hip OA. These factors should be assessed in clinical practice for patients with hip OA living in Asian cultures if the goal of treatment is to improve their HRQoL.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.