
Abstract
Background and purpose:
Considering dissatisfaction rates of around 10% after total hip arthroplasty (THA), this study aimed to investigate the role of pain catastrophising (PC) on functional outcomes, pain, and quality of life following THA in a large prospective study. PC is the tendency to focus on and exaggerate painful stimuli combined with a decreased ability to deal with pain.
Patients and methods:
A prospective comparative study was performed with 531 patients undergoing primary unilateral THA between 2019 and 2020. Patients were considered PC with a preoperative score ⩾30 on the PC Scale, resulting in 57 (11%) PC-patients. Patient-reported outcome measures (PROMs) were collected preoperatively, at 3 months, 1 year, and 2 years postoperatively and consisted of Hip disability and Osteoarthritis Outcome Score–Physical Function (HOOS-PS), Oxford Hip Score (OHS), pain (NRS), and quality of life (EQ-5D), including minimal clinical important differences (MCIDs) and patient acceptable symptom state (PASS), as well as length of stay and aseptic revisions.
Results:
PC-patients reported inferior preoperative scores on all PROMs and had longer hospital stay (p = 0.02). Although PC-patients had more improvement in all scores and a higher proportion generally reached MCID, they still reported lower OHS, more pain, and lower EQ-5D at 2-year follow-up (all p < 0.03), and fewer PC-patients reached PASS for OHS and EQ-5D at final follow-up. No difference in aseptic revisions was seen (p = 0.95).
Conclusions:
PC-patients had worse preoperative subjective function and more pain. Although they showed more improvement than non-PC patients at all outcomes, less patients reached PASS for OHS and EQ-5D at 2-year follow-up.
Keywords
Introduction
Total hip arthroplasty (THA) is 1 of the most performed orthopaedic procedures,1,2 and considered a reliable procedure with excellent implant survivorship and patient-reported outcomes.3–5 It has been projected that the number of patients undergoing THA will dramatically increase over the next decades, and it is therefore important to better understand the risk factors of unsatisfying outcomes and revision surgery. 1
Psychological factors have been the topic of research on patients undergoing total joint replacement, with 1 of these factors being pain catastrophising (PC). PC is described as the tendency of patients to focus on and exaggerate painful stimuli combined with a decreased ability to deal with pain. 6 In 2012, a systematic review on the role of psychological factors on the outcomes of total joint arthroplasty concluded that there was insufficient evidence for THA patients. 7 Since then, several studies have assessed whether patients with preoperative PC have increased pain or prolonged opioid use or decreased sleeping quality compared to patients without PC.8–14,41 These studies are often limited by maximum 1-year follow-up, retrospective study designs, and small sample sizes, which may explain the conflicting and unclear results. Furthermore, none of the studies have assessed revision rates as an outcome. Sufficient sample sizes and large cohort studies are especially needed as the incidence of PC is estimated to be only between 10 and 30% in cohort studies,15–17 and revision rates following THA are generally low.3,8,18,19
Therefore, the goal of this study was to assess the role of PC on the outcomes of THA in a prospective large cohort of patients with minimum 2-year follow-up. While previous studies reported conflicting findings, it was hypothesised that preoperative PC would be significantly associated with inferior preoperative and postoperative pain and subjective function, and higher aseptic revision rates.
Methods
This prospective cohort study was performed in a high-volume teaching hospital between 01 January 2019, and 30 September 2020, with predefined outcome measures and follow-up points. Institutional review board approval (L019-075) was obtained prior to the study. The Reporting of studies Conducted using Observational Routinely-collected health Data (RECORD) statement and the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline were followed.20,21 Patients were eligible for inclusion if they: (1) were scheduled for unilateral primary THA for the indication of end-stage osteoarthritis (OA) (Kellgren-Lawrence 3 or 4); (2) mastered the Dutch language; (3) completed the preoperative questionnaires; and (4) provided informed consent to participate in the study. Patients were excluded at the end of follow-up if they had not completed the 2-year follow-up questionnaires after 2 automatic reminders, or if they decided to drop out of the study at an earlier point.
Outcome measures
The primary outcome measures of this study were patient-reported subjective function, pain, and quality of life following THA. These were assessed using the following patient-reported outcome measures (PROMs): the Hip disability and Osteoarthritis Outcome Score – Physical Function Shortform HOOS-PS, 18 Oxford Hip Score (OHS), 19 numeric rating scale NRS for pain 22 and the 5-level EuroQol-5-dimension (EQ-5D-5L) index for quality of life (the Dutch tariff).23,24 Differences in these measures between PC patients and non-PC patients were evaluated at baseline, 3 months, 1 year, and 2 years postoperatively. Additionally, to determine clinically relevant improvement after THA, it was evaluated whether the improvements between preoperative and any of the follow-up moments exceeded the minimal clinical important differences (MCIDs). Furthermore, it was assessed whether patients reached a patient acceptable symptom state (PASS). The primary null-hypothesis for this study was that there are no differences in subjective function, pain and quality of life outcomes between patients with and without PC symptoms preoperatively.
The secondary outcome measures included the rate of aseptic revisions and length of hospital stay. The secondary null-hypotheses were that there are no differences in revision rates and no differences in length of hospital stay, between patients with and without PC symptoms preoperatively.
Data collection
Preoperatively, PC was assessed using the Pain Catastrophizing Scale (PCS) (Appendix 1).25,26 The PCS is a validated questionnaire consisting of 13 statements regarding feelings and thoughts during experiencing pain.27,28 Patients rate these statements on a 5-point Likert scale ranging from “not at all” to “all the time” with the total score ranging from 0 (no catastrophising) to 52 (severe catastrophising). A score of ⩾30 is considered clinically relevant catastrophising,8,27 as such, patients were considered PC or non-PC patients.
The primary outcome measures were assessed through the aforementioned PROMs, the Dutch language versions of the HOOS-PS, OHS, NRS, and the EQ-5D-5L. Patients were invited to complete questionnaires prior to surgery and at 3 months, 1 year and 2 years postoperatively with 2 automatic reminders in case of non-completion. Furthermore, the achievement of MCID and PASS thresholds for each PROM was assessed. Respectively, the MCID and PASS for HOOS-PS were 23 and 88, 29 for OHS 5.2 and 39,19,30 for NRS pain 18.6 and 21.6,31,32 and for EQ-5D-5L 0.31 and 0.77,29,33 although pain PASS was based on hip arthroscopy. 32 As for secondary outcomes, revision rates were determined through electronic health records up to 2-year follow-up, and cross-referenced with the National Dutch Arthroplasty Registry (LROI) to ensure completeness. LROI has a 100% coverage of hospital and 96% completeness for revisions nationally. 34 Length of hospital stay was recorded in days from admission to discharge. Baseline demographics and intraoperative characteristics were also prospectively collected through the electronic health records preoperatively and postoperatively, respectively.
Study cohort
A total of 693 patients fulfilled the inclusion criteria of which 162 were excluded because they dropped out of the study (90 dropouts at 3 months, 32 dropouts at 1 year, 40 dropouts at 2 years) leading to a cohort of 531 patients (Figure 1). Response rate was 88–100%. Overall mean age was 70 years, 65% were female, mean body mass index (BMI) 27 kg/m2 (Table 1). 57 patients (11%) were classified as PC-patients. Baseline demographics and intraoperative characteristics differed insignificantly except for gender, BMI, and ASA.
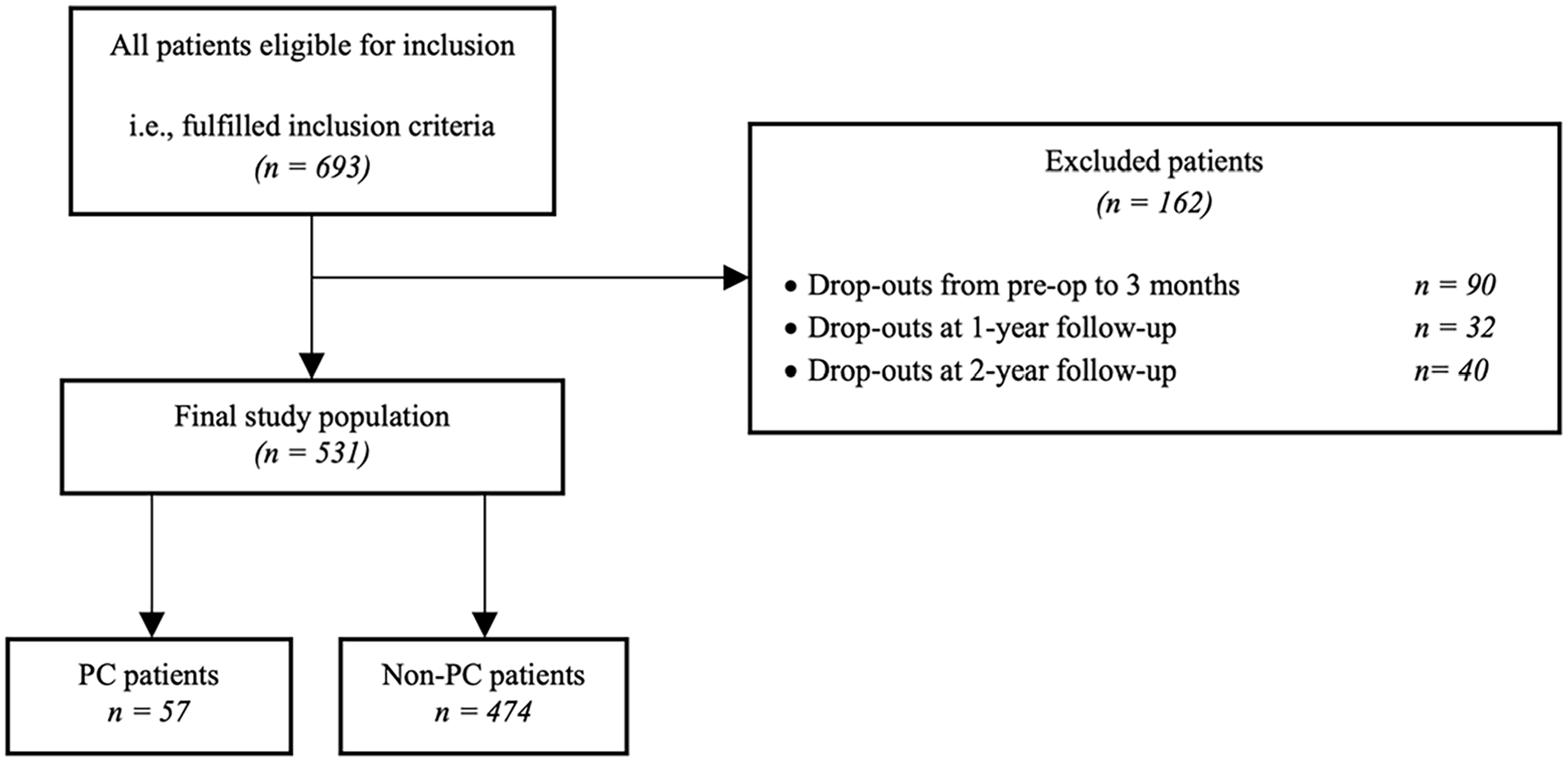
A flowchart of the study population, including the number of drop-outs i.e., excluded patients during the inclusion period.
Preoperative and intraoperative patient demographics and short-term outcomes of length of stay and aseptic revisions of all patients and of patients stratified by catastrophising.
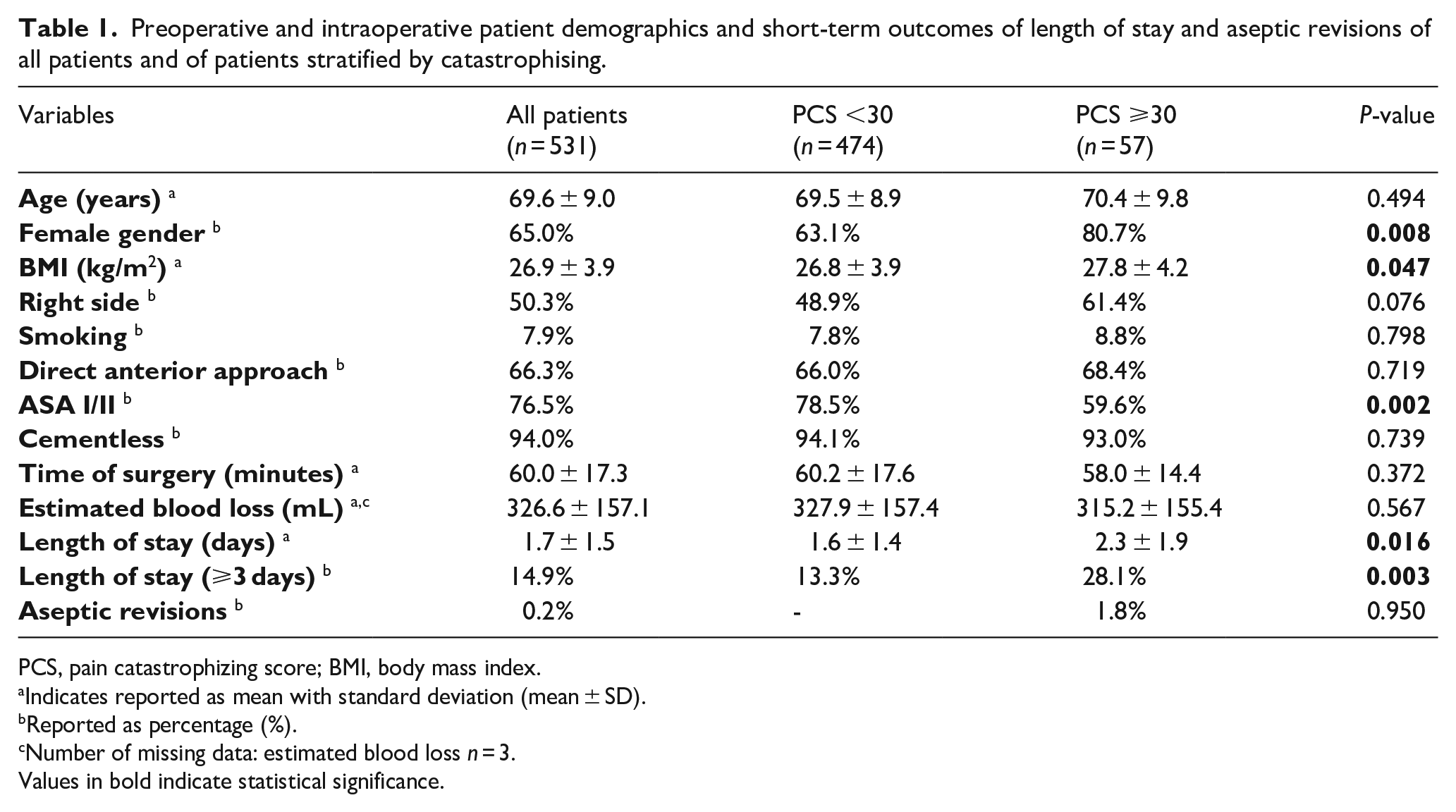
PCS, pain catastrophizing score; BMI, body mass index.
Indicates reported as mean with standard deviation (mean ± SD).
Reported as percentage (%).
Number of missing data: estimated blood loss n = 3.
Values in bold indicate statistical significance.
Surgical technique
For uncemented THA (94%), patients received the R3 acetabular cup and Polarstem system with standard highly cross-linked polyethylene liner and either an Oxynium or Cobalt Chromium femoral head, and for cemented THA (3%) the Spectron (2019) and cemented Polar system (since 2020) were used (all Smith & Nephew, London, UK). 3% had (reversed) hybrid THA, and the majority (66%) underwent THA via the direct anterior approach. Mean time of surgery was 60 ± 17 minutes (range 28–192 minutes), and estimated blood loss 327 ± 171 mL (range 75–1600 mL).
Statistical analysis
SPSS Statistics version 28 (IBM Corp., Armonk, NY, USA) was used for statistics. To compare categorical and continuous variables between PC and non-PC patients, chi-square tests and independent sample t-tests were used, respectively. Linear regression analyses were performed for all preoperative scores, 2-year follow-up, and total improvement (i.e., change from preoperative to 2-year follow-up), to correct for the between-group differences in gender, ASA, and BMI. Finally, a log rank test was used to compare aseptic revisions between both groups. A p-value < 0.05 was considered a statistically significant difference.
A power analysis was conducted before study commencement, to determine the appropriate sample size for detecting clinically significant differences in the primary outcome measures. The sample size calculation of the primary outcome (HOOS-PS) using a standard deviation 17 points and MCID threshold of 23 for HOOS-PS, 29 (based on previous literature and preliminary data), alpha 0.05, power 80%, and enrolment ratio 5:1, revealed 30 PC-patients and 150 non-PC-patients were needed to assess a statistically significant difference between both groups. 35 The term ‘Beta’ represents the regression coefficient, indicating the change in the dependent variable associated with a 1-unit change in the independent variable. For example, when referring to the HOOS-PS scores, a Beta value of −10.0 suggests a decrease of 10.0 points in the preoperative HOOS-PS for the PC group compared to the non-PC group. Additionally, a power analysis was performed for the other primary outcome measures (OHS, NRS, EQ-5D-5L, including MCID and PASS for all PROMs), confirming that the minimal sample size of 180 patients provided sufficient power to detect clinically relevant differences. However, as this study was conducted in a high-volume teaching hospital, larger sums of study participants were easy to reach. Therefore, it was chosen to recruit a larger study population than power analysis initially required. For the secondary outcome measure of revision rate, a 2% difference between groups was anticipated, requiring a total sample size of 3054 patients to achieve sufficient power. Given that our study cohort was smaller, we acknowledge the possibility of a type II error in detecting differences in revision rates.
Results
Subjective physical function
Regarding the HOOS-PS, preoperatively PC-patients reported inferior subjective function when compared to non-PC-patients but this was equivalent at 1- and 2-year follow-up (Table 2) (Figure 2(a)). PC-patients had more improvement from preoperative to all follow-up moments and a higher proportion reached MCID including at 2-year follow-up (91% vs. 73%, p = 0.003). No significant difference in PASS was seen. When correcting for baseline differences, similar findings were noted with PC as a significant factor on preoperative HOOS-PS (p < 0.001, Beta −15.6 [confidence interval (CI ) −20‒-11]) and for improvement from preoperative to 2-year follow-up (p < 0.001, Beta 13.8 [CI, 8–19]), but not for 2-year HOOS-PS (p = 0.2, Beta −1.9 [CI, −5–1]).
Patient-reported outcomes of the Hip disability and Osteoarthritis Outcome Score – Physical Function (HOOS-PS) in all patients and stratified by patient catastrophizing score.
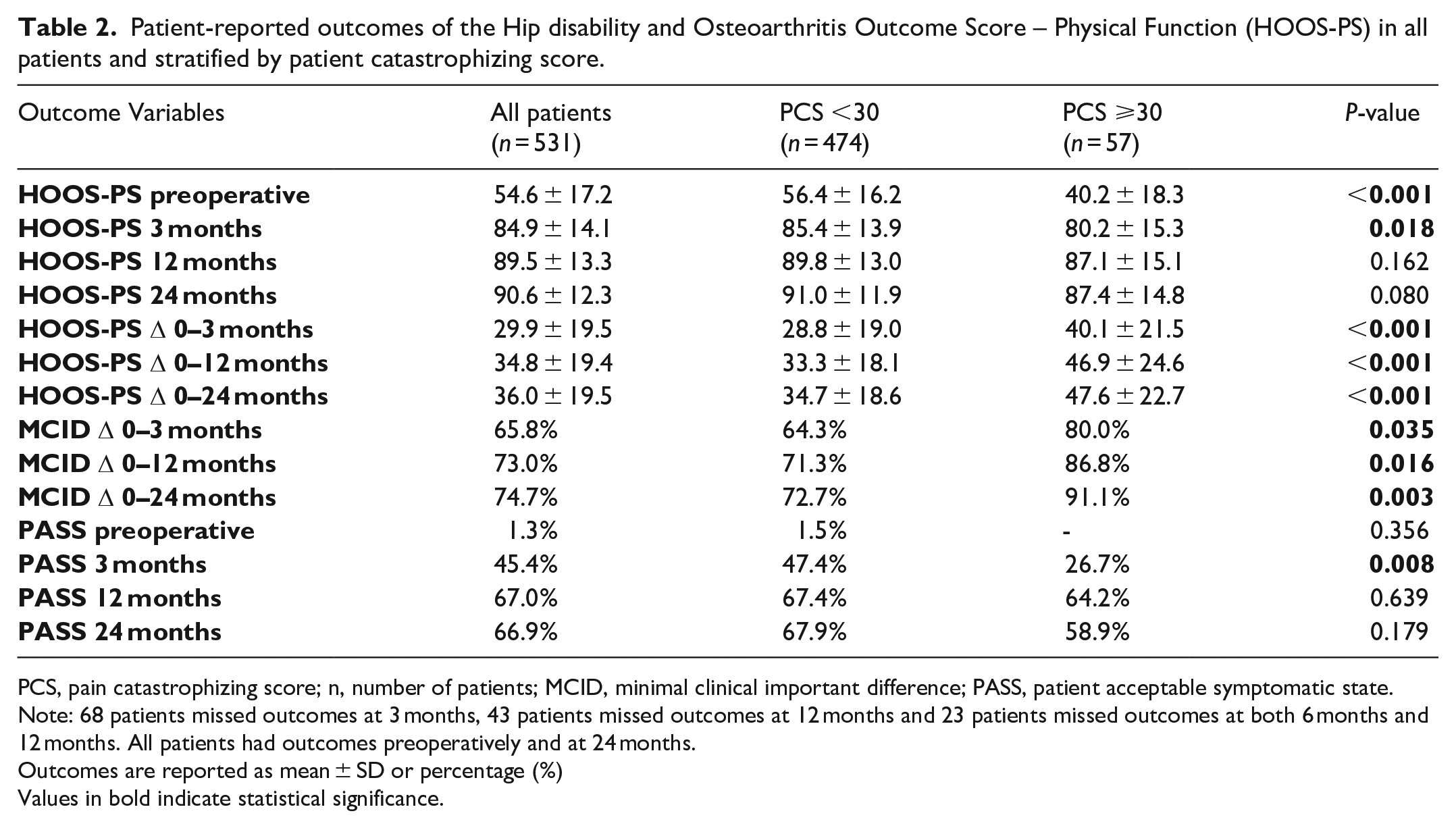
PCS, pain catastrophizing score; n, number of patients; MCID, minimal clinical important difference; PASS, patient acceptable symptomatic state.
Note: 68 patients missed outcomes at 3 months, 43 patients missed outcomes at 12 months and 23 patients missed outcomes at both 6 months and 12 months. All patients had outcomes preoperatively and at 24 months.
Outcomes are reported as mean ± SD or percentage (%)
Values in bold indicate statistical significance.
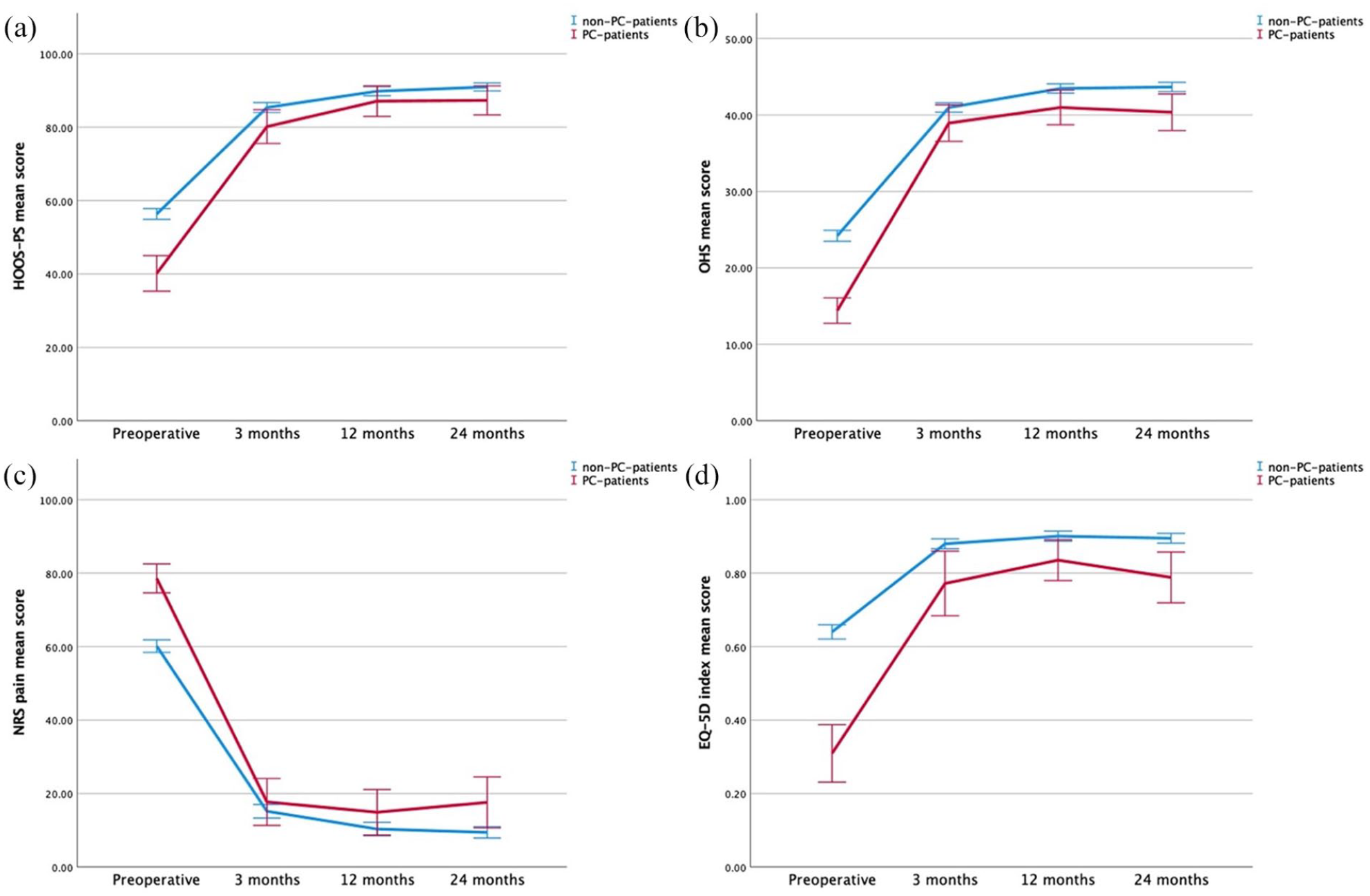
The mean and 95% confidence intervals of PC-patients (red – [darker]) and non-PC-patients (blue) with the HOOS-PS (a), OHS (b), NRS Pain (c), and EQ-5D Index (d).
For OHS, PC-patients had inferior scores preoperatively and at 2-year follow-up, although this did not exceed the MCID (Table 3) (Figure 2(b)). PC-patients had more clinical improvement from preoperative to all follow-up moments (p < 0.001) although no significant differences were seen for MCID. Less PC-patients reached PASS at 2-year follow-up (67% vs. 84%, p < 0.001). When correcting for baseline differences, similar findings were noted with PC as a significant factor for preoperative OHS (p < 0.001, Beta −8.9 [CI, −11–-7), for overall improvement (p < 0.001, Beta 6.7 [CI, 4–9]), and for 2-year OHS (p = 0.02, Beta −2.2 [CI, −4‒-0.4]).
Patient-reported outcomes of the Oxford Hip Score (OHS) in all patients and stratified by patient catastrophizing score.
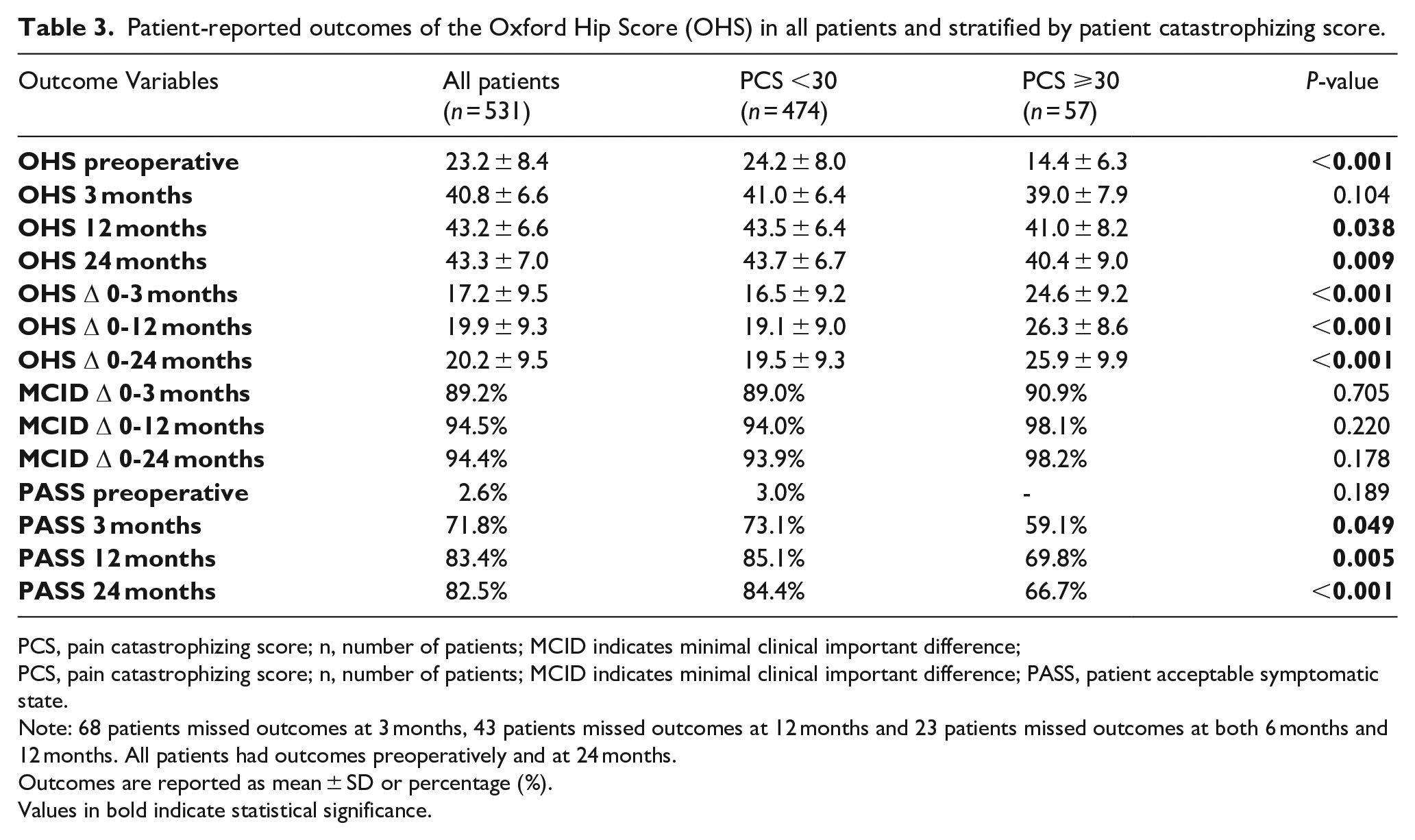
PCS, pain catastrophizing score; n, number of patients; MCID indicates minimal clinical important difference;
PCS, pain catastrophizing score; n, number of patients; MCID indicates minimal clinical important difference; PASS, patient acceptable symptomatic state.
Note: 68 patients missed outcomes at 3 months, 43 patients missed outcomes at 12 months and 23 patients missed outcomes at both 6 months and 12 months. All patients had outcomes preoperatively and at 24 months.
Outcomes are reported as mean ± SD or percentage (%).
Values in bold indicate statistical significance.
Pain and quality of life
Similar findings were also noted for pain (Table 4) (Figure 2(c)) and quality of life (Table 5) (Figure 2(d)). PC-patients reported more pain (p < 0.001) and inferior quality of life preoperatively (p < 0.001). At 2-year follow-up, PC-patients reported more pain and inferior quality of life despite more improvement for both parameters over time compared to non-PC-patients. No significant difference in reaching MCID or PASS for pain was noted although more PC-patients had their improvement exceed MCID for quality of life at 2-year follow-up (78% vs. 27%, p < 0.001). When correcting for baseline differences, PC was a significant factor for preoperative pain (p < 0.001, Beta 17.3 [CI, 12–22]) and EQ-5D (p < 0.001, Beta −0.31 [CI, -0.4‒-0.3]), for improvement up to 2 years for pain (p = 0.004, Beta −10.3 [CI, −17‒-3]) and quality of life (p < 0.001, Beta 0.23 [CI, 0.2–0.3]) and for 2-year pain (p = 0.01, Beta 6.7 [CI, 2–12]) and quality of life (p < 0.001, Beta −0.08 [CI, −0.1‒-0.04]).
Patient-reported outcomes of the Numeric Rating Scale (NRS) Pain in all patients and stratified by patient catastrophizing score.
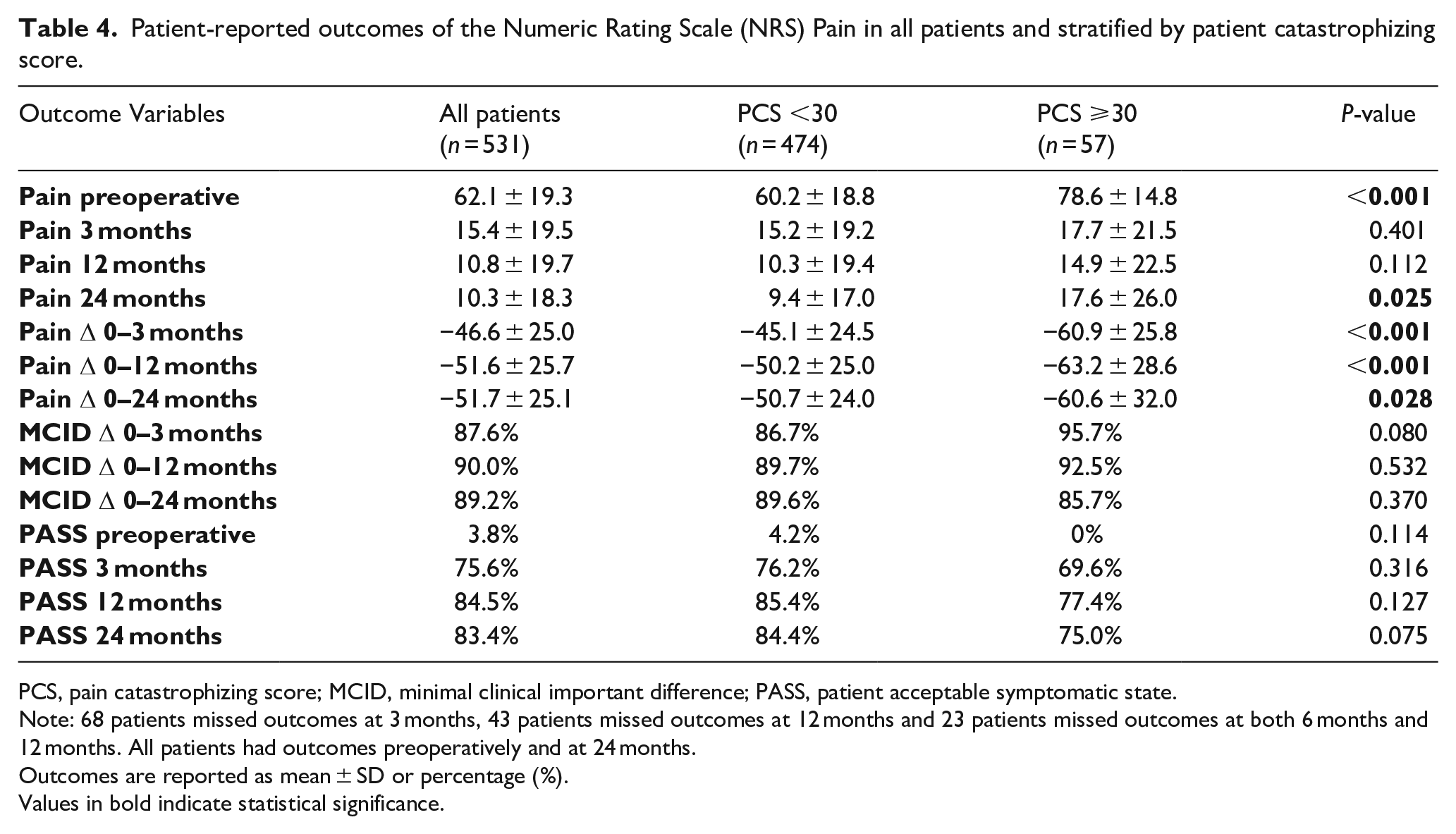
PCS, pain catastrophizing score; MCID, minimal clinical important difference; PASS, patient acceptable symptomatic state.
Note: 68 patients missed outcomes at 3 months, 43 patients missed outcomes at 12 months and 23 patients missed outcomes at both 6 months and 12 months. All patients had outcomes preoperatively and at 24 months.
Outcomes are reported as mean ± SD or percentage (%).
Values in bold indicate statistical significance.
Patient-reported outcomes of the EQ-5D in all patients and stratified by patient catastrophizing score.
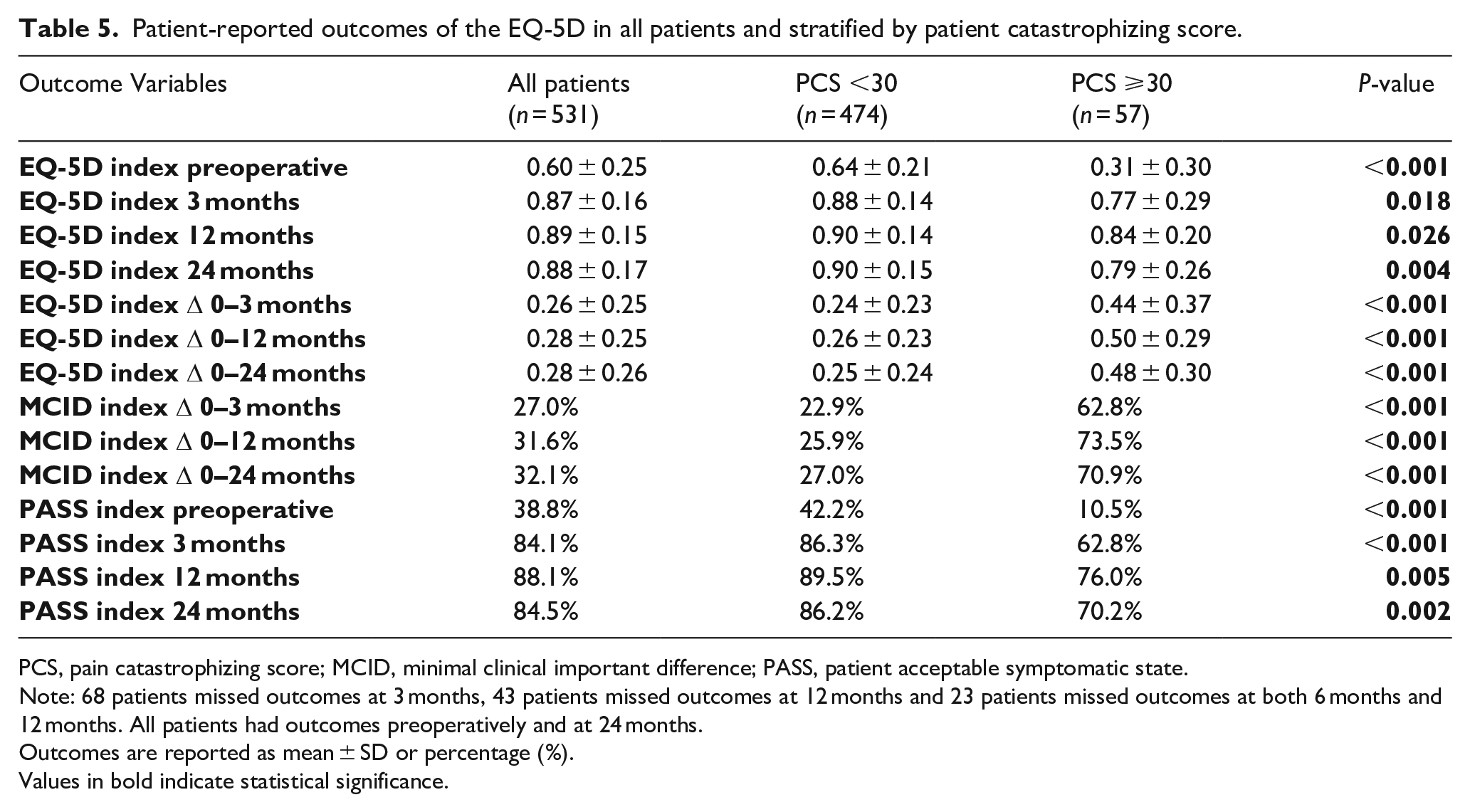
PCS, pain catastrophizing score; MCID, minimal clinical important difference; PASS, patient acceptable symptomatic state.
Note: 68 patients missed outcomes at 3 months, 43 patients missed outcomes at 12 months and 23 patients missed outcomes at both 6 months and 12 months. All patients had outcomes preoperatively and at 24 months.
Outcomes are reported as mean ± SD or percentage (%).
Values in bold indicate statistical significance.
Aseptic revision surgery
Only 1 patient underwent cup revision for iliopsoas impin-gement at 2.6 years follow-up, resulting in a total survivorship of 99.8% without baseline differences between the groups (p = 0.95).
Length of hospital stay
PC-patients had a significant longer length of hospital stay, compared with non-PC patients (2.3 ± 1.9 vs. 1.6 ± 1.4, p = 0.02).
Discussion
The goal of this study was to assess the role of PC in patients undergoing THA in a large prospective study with minimum 2-year follow-up. The most important findings were that even if pain catastrophising patients reported inferior subjective function and pain preoperatively and during follow-up, they showed more improvement than their counterparts without PC. At 2-year follow-up, they had equivalent HOOS-PS, although they were noted to have inferior OHS, NRS pain and quality of life. PC-patients generally reached the MCID more often but reached the PASS equally or less often. When correcting for baseline differences, similar findings were noted.
In this study, an incidence of pain catastrophising of 11% was found and the mean PCS was 14 ± 11. When compared to the literature, the incidence of PC is lower than reported, as 2 previous studies reported an incidence of 29–30% for THA.8,11 We cannot really explain this difference, although these might be associated with geographical difference, demographic differences in the cohorts, or the presence of more resilience. 36 When reviewing the mean PCS scores, the reported values range widely in the literature from 11 to 29,10,12,13,37 and our mean PCS falls within this range.
In this study, it was noted that PC patients preoperatively reported increased pain and inferior subjective clinical function. These findings are in line with the previous study by Wood et al. 38 who reported that preoperative pain catastrophising was associated with increased pain and inferior Oxford scores, although it should be acknowledged that they combined the cohort of THA and total knee arthroplasty (TKA) patients. Most other studies assessing the role of pain catastrophising only focused on postoperative outcomes and did not incorporate preoperative pain and subjective function scores.8–14 In this study, patients were prospectively followed which allowed us to determine and compare clinical improvement between PC and non-PC patients.
With regards to subjective function, PC-patients were noted to start with inferior subjective function preoperatively but had more improvement over time than non-PC patients. These findings were both noted for the HOOS-PS and OHS and are consistent with findings by Wood et al. 38 They likewise noted inferior preoperative Oxford scores, but more clinical improvement from preoperative to postoperative, although they pooled the findings of THA and TKA. However, studies have described that different patients have different postoperative trajectories. 39 For example, a nationwide Dutch study identified 3 distinct recovery patterns after total hip arthroplasty: fast starters, who exhibit rapid initial improvement and maintain high functional scores; slow starters, who show little to no initial improvement but experience delayed recovery over time; and late dippers, who initially improve but later experience functional decline. Several patient characteristics, such as female sex, older age, obesity, higher ASA grades, and poorer preoperative EQ-5D scores, were associated with less favourable recovery trajectories. Despite these variations, all patient subgroups demonstrated overall functional improvement following surgery, highlighting the complexity of recovery patterns in orthopaedic patients. 39 Thus, although it seems that PC-patients quickly reach equivalent scores to non-PC patients, the outcome scores might suggest that PC-patients take slightly longer to reach their optimal scores. With the HOOS-PS, PC-patients are still slightly behind at 3 months but close the gap between both groups at 1 year. This was also seen for quality of life, where non-PC patients reached their ultimate score already at 3 months postoperatively, while PC-patients still improved between 3 months and 1-year follow-up, and also more PC-patients reached PASS at 1- and 2-year than 3 months follow-up.
Regarding postoperative pain, our study noted that both groups had significantly decreased pain from preoperative to all postoperative follow-up moments, and that no clinically relevant differences in pain were reported at 3 months and 1-year follow-up between the groups. PC-patients had significantly more improvement than non-PC patients. Interestingly, pain seemed to increase slightly in PC-patients between 1- and 2-year follow-up whereas this finding was not seen in the non-PC patients. Other studies with short-term follow-up reported more pain in the PC-group at 3 months and 1-year postoperatively,10,11 which was not seen in our study. No other studies with 2-year follow-up were identified to compare our findings with, but the phenomenon of slightly increasing pain at final follow-up in PC-patients is of concern and longer follow-up is necessary to see whether these patients will have increased pain and higher risk of revisions. 2 studies in the literature assessed opioid use in these patients and despite more pain in the first year, they could not find significantly increased opioid use in PC-patients.11,13
In this study, it was noted that PC-patients had a longer (2.3 vs. 1.6 days) length of hospital stay following THA compared to the non-PC group. Most studies have not assessed the role of PC on length of stay, but Hardy et al. 10 similarly noted prolonged length of stay in this group of patients. Interestingly, they found that the mean length of stay was not significantly different between both groups but that PC patients more often stayed 3 days or longer (53%) than non-PC patients (36%). Similarly in our study, PC-patients more often stayed 3 days or longer (28%) when compared to non-PC patients (13%). This is a relevant finding for institutions that want to screen patients for potential day-care treatment.
One hypothesis of this study was that PC was associated with more aseptic revisions, but this was not observed. Despite the large cohort of patients in this study, it was still underpowered to detect small differences in revision rates between groups. As THA is generally a highly successful surgery with low revision rates, it is difficult to find statistically significant differences and larger registry studies with long-term follow-up are generally needed to reveal differences in revision rates. 40
Limitations are present in our study, despite the large sample size, prospective study design, and longer follow-up than previous studies. Most importantly, the proportion of PC-patients was relatively small (11%), although our mean PCS was comparable with current literature. Second, baseline differences existed between both groups, for example ASA classification or gender proportions differed significantly, and may have influenced outcome differences between PC patients and their counterparts. Therefore, linear regression analyses were performed to correct for these confounders and revealed similar findings. Third, the preoperative grade of OA was not assessed in this cohort, as it has been previously shown that the preoperative OA grade is not associated with preoperative pain catastrophising. 36 Furthermore, all operative cases are reviewed preoperatively by the group of orthopaedic surgeons and only patients with end-stage OA were indicated for surgery. Finally, statistical analysis for revision rates was underpowered and large registry-based studies are needed to assess differences in revision rates.
Future research should focus on objectively, opposed to subjectively, investigating the differences for pain PC-patients, and exploring the benefit of a preoperative psychological intervention on THA outcomes through a controlled trial. This could include applying condensed psychological therapies, such as cognitive-behavioural therapy or acceptance and commitment therapy, during the preoperative phase. As a result, the influence can be investigated of such interventions on postoperative experiences among patients, distinguishing between those who have undergone preoperative therapy and those who have not. Lastly, the potential bidirectional relationship between PC and fibromyalgia could be interesting to further explore, as catastrophising traits are frequently observed in fibromyalgia patients, while it remains unclear whether THA patients with high levels of PC are at increased risk of developing fibromyalgia.
Conclusion
In this prospective comparative study of 531 patients with a 2-year follow-up, it was noted that patients who showed preoperative pain catastrophising reported significantly inferior subjective function and pain preoperatively and postoperatively (except for the HOOS-PS at 2 years follow-up) but more improvement from preoperative to final follow-up, with a significant difference in MCID for HOOS-PS and quality of life. Despite more improvement in PC-patients, overall, they reached PASS less often at final follow-up for OHS and quality of life. PC-patients had a longer length of stay, but no significant differences in revision rates were seen.
Footnotes
Appendix 1
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.