
Abstract
A 63-year-old man collided with a vehicle while riding a motorcycle. At an emergency hospital, he was diagnosed with cerebral concussion, incomplete cervical cord injury, C6 fracture, facial bone fractures, and lacerations. Radiographical findings indicated that his neck was forced into an extended position. At our rehabilitation hospital, we evaluated the patient’s hoarseness and dysphagia 1 month posttrauma and determined the diagnosis to be due to “traumatic right recurrent laryngeal nerve palsy (RLNP).” We followed the patient’s RLNP during admission and at our outpatient clinic. His right RLNP gradually recovered and finally disappeared 6 months after the accident. We describe this case within the context of a review of the literature.
Introduction
Acute traumatic central cord syndrome is the most commonly encountered subtype of incomplete spinal cord injury and is characterized by worse sensory and motor function in the upper extremities compared with the lower extremities. It is commonly seen in the setting of trauma such as motor vehicles or falls in elderly patients. 1 There are several reports regarding dysphagia after acute traumatic spinal cord injury using videofluoroscopy. 2,3
The etiologies of adult vocal paralysis vary according to the site of the lesion as well as the extent and cause of the damage. Most large studies point to the surgical cases of cervical spine, 4 aortic aneurysm, 5 or neoplasm 6,7 regarding the causes for recurrent laryngeal nerve palsy (RLNP). In the case of RLNP related to trauma, the literature reports a case of laryngeal blunt trauma 8 and a case of skull fracture involving the bilateral jugular foramen. 9 However, a case of unilateral RLNP caused by a traction mechanism has not been reported, thus far. We describe such a case within the context of a review of the literature.
Case report
A 63-year-old man who was riding a motorcycle collided with another vehicle at an intersection. He was taken to an emergency hospital by an ambulance.
It was supposed that the patient’s neck had been forced into an extended position. The patient was diagnosed with cerebral concussion, incomplete cervical cord injury at the level C6 with a C6 fracture, facial bone fractures, and a facial laceration including the left canaliculus, and amputation of the right first finger at the level of the proximal interphalangeal joint. As his cervical spine was stable, his cervical cord injury as well as his cervical spine fracture was conservatively treated with neck fixation collar. No tracheal intubation was performed during the clinical course.
One month post-injury, the patient was transferred to our hospital for rehabilitation. On admission, he complained of hoarseness, dysphagia, muscle weakness in the bilateral forehands, numbness, and sensory disturbance of the bilateral C8 dermatome.
Computed tomography (CT) scan of the head, neck, and thorax revealed no apparent subcutaneous or intrathoracic mass or hematoma, or laceration caused by this injury.
The neck X-ray film showed extension of the neck at the level of C6 with fracture of the anterior lower portion of C6 spine (Figure 1).

Neck X-ray showing extension of the neck at the level of C6 with fracture of the anterior lower portion of C6 spine (arrow heads).
The neck sagittal magnetic resonance imaging (MRI) scan showed slight hyperintensity of the spinal cord from C4 to C6 spine level on the T2-weighted image and extension of the neck at the level of C6 (Figure 2). On the axial MRI scan at the level of C6 did not show any remarkable findings (Figure 3).

Neck MRI (T2-weighted image, sagittal) showing slight hyperintensity of the spinal cord from C4 to C6 spine level and neck extension at the level of C6 (arrow heads). MRI: magnetic resonance imaging.
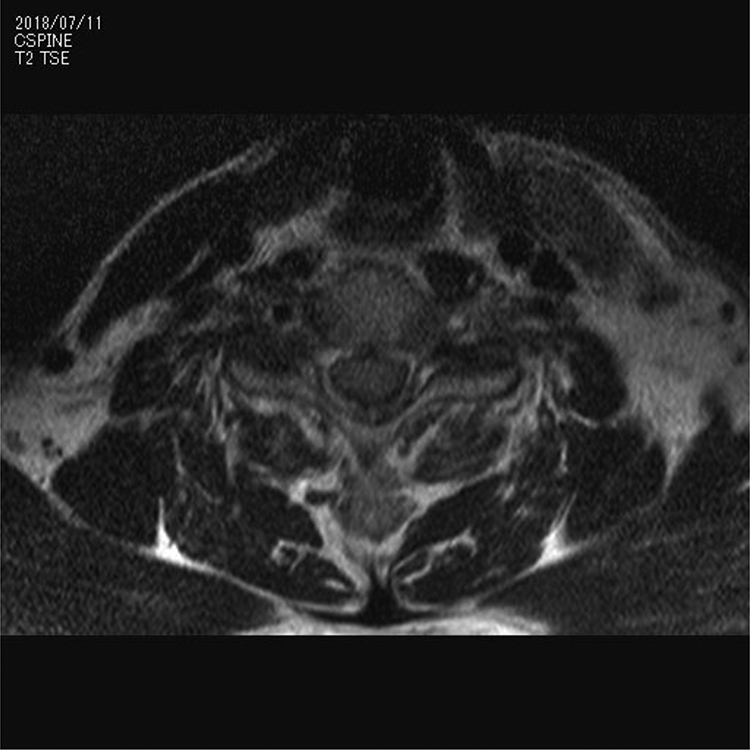
Neck MRI (T2-weighted image, axial) at the level of C6, showing no remarkable findings. MRI: magnetic resonance imaging.
The neck bone CT scan revealed a teardrop fracture of C6 body as well as a fracture of the left transverse process (Figure 4(a) and (b)).
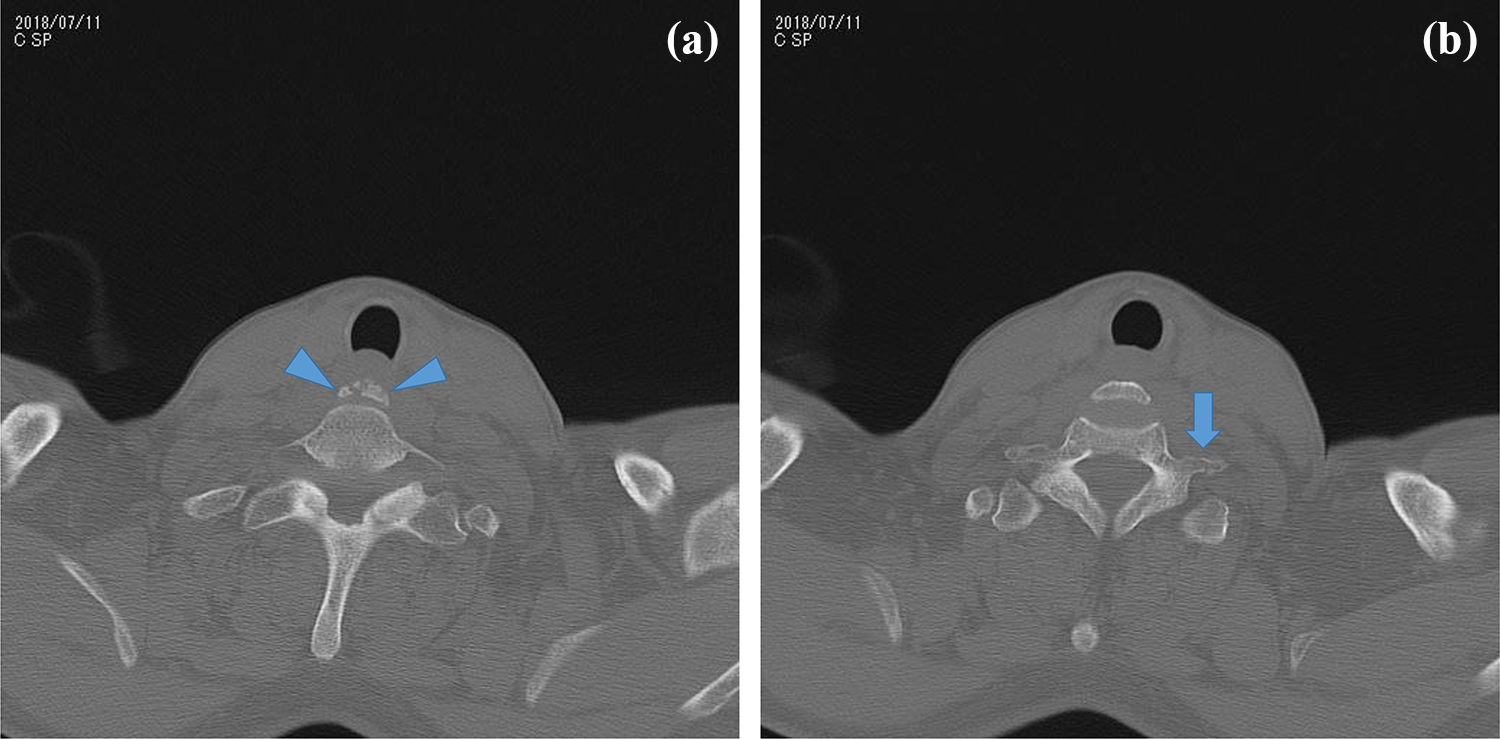
(a and b): Neck bone CT scan, revealing a teardrop fracture of C6 body (arrow heads) as well as a fracture of the left transverse process (arrow). CT: computed tomography.
Videoendoscopic evaluation (VE) of swallowing revealed saliva and food residue in the pyriform sinus and vallecula of the epiglottis. The right vocal cord was located centrally. It did not move adequately and smoothly, indicating right unilateral RLNP (Figure 5). Also, curtain sign was positive, suggesting inadequate movement of the right pharynx.
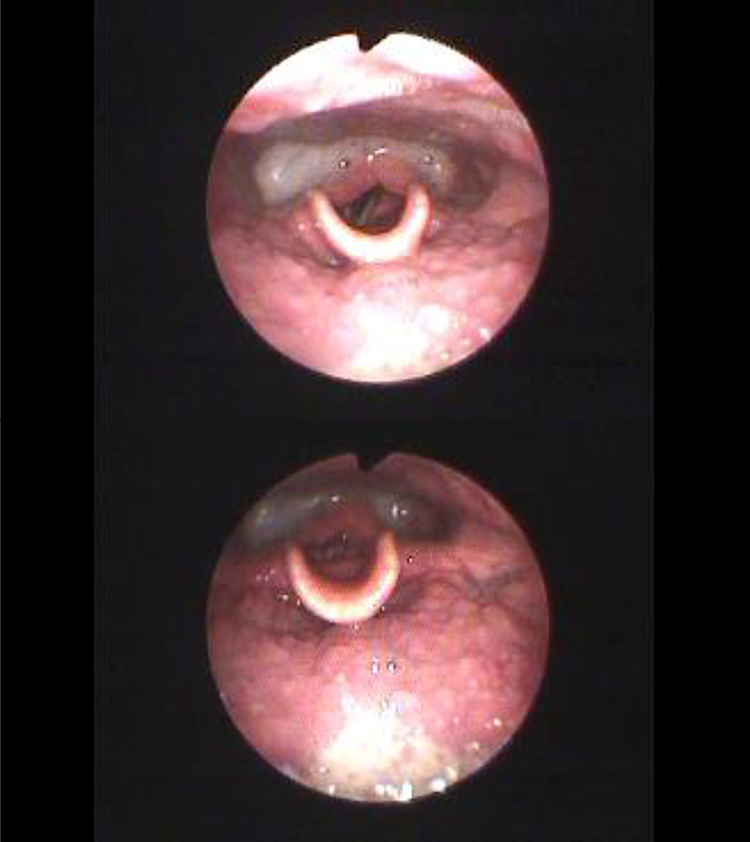
VE of swallowing, showing paralysis of the right vocal cord, as well as over-adduction of the left arytenoid. Upper: inspiration; lower: vocalizing. VE: videoendoscopic evaluation.
Videofluoroscopic examination of swallowing (VF) showed inadequate opening of the upper esophagus. Additional water swallowing was effective, while additional saliva swallowing was not. This patient’s RLNP resulted in hoarseness and occasional coughing while eating. The latter may be caused due to intra-swallowing aspiration of food.
Except for the above-mentioned signs and symptoms of the right RLNP, there were no other symptoms of right vagal nerve (the Xth nerve) dysfunction.
The patient had a history of hypertension, hyperlipidemia, and duodenal ulcer, for all of which he required medication.
After discharge, the patient’s right RLNP gradually improved and disappeared 6 months after the accident.
Discussion
The patient’s hoarseness and swallowing disturbance were typical signs and symptoms of unilateral RLNP. Also, there was no other X cranial nerve signs such as vertigo or orthostatic hypotension. Moreover, right RLNP was confirmed and evaluated by VE. Finally, the patient had recovered from RLNP at 6 months after the accident. This clinical course is also consistent with the suspected etiology of “incomplete damage to the right recurrent laryngeal nerve by physical extension force.”
Regarding the suggested mechanism of the unilateral RLN injury in this case, several findings support the physical extension force mechanism: (1) The existence of a facial laceration which suggests that the patient received an impact, at least, to the face; (2) the neck X-ray revealed the fracture of the lower portion of the C6 spine suggesting the extension of the neck (Figure 1); (3) also, the cervical MRI findings showed the existence of extension injury at the level of the C6 vertebra (Figure 2) (it is a well-known fact that neck extension injury frequently causes incomplete cervical cord injury 1 ); (4) moreover, there were no other causes of RLNP revealed by the X-ray, MRI, and CT scans of the head, the neck, and the chest. No tracheal intubation or no cervical fixation surgery was performed. Therefore, it is suspected that the patient’s right RLNP was caused by neck extension.
However, it is possible that RLN was compressed by the teardrop fracture itself or by the edema of the surrounding tissue. Moreover, it is also possible that RLN was damaged by the direct compressing force to the neck. The third mechanism is more likely if the laryngeal nerve course takes “nonrecurrent” type. Nonrecurrent inferior laryngeal nerve (NRILN) has been reported as a potential risk for the intraoperative injury of RLN in thyroid or cervical spine surgery. Although NRILN is rare (0.52%), it is found almost exclusively on the right side. 10 So, if there is NRILN, direct damage of the nerve is also possible. In our case, the existence of the transverse process fracture on the left side (Figure 4(a) and (b)) suggests that the impulsive force was more severe on the left side rather than on the right side. This fact also supports the aforementioned mechanism of indirect extension force to the right RLN.
So far, there have been no reports of unilateral RLNP caused by neck extension. Furthermore, there has been no reported case of traumatic RLNP in which the clinical course was carefully followed using VE and VF.
As the elderly population increases, so does the number of cases of incomplete cervical cord injury. Thus, it is predicted that more cases of RLNP caused by this mechanism may be found in the future. And, in that case, it is very important to check the existence of RLNP using VE and/or VF.
Footnotes
Acknowledgements
The authors especially thank all the nursing and rehabilitation staff for their devoted and capable nursing care and rehabilitation. The authors appreciate Dr Mari Nakao for her very useful comments on the VE findings.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.