
Abstract
Background:
Ankle foot orthoses (AFOs) are usually used for patients with incomplete spinal cord injury (ISCI) to provide support in walking.
Objectives:
The aim of this study was to compare the effect of AFOs, with and without ankle hinges, on specific gait parameters during treadmill training by subjects with ISCI.
Study Design:
Quasi-experimental.
Methods:
Five patients with ISCI at the thoracic level participated in this study. Gait evaluation was performed when walking 1) barefoot 2) wearing a solid AFO and 3) wearing a hinged AFO.
Results:
The mean step length when walking barefoot was 26.3 ± 16.37cm compared to 31.3 ± 17.27 cm with a solid AFO and 28.5 ± 15.86 cm with a hinged AFO. The mean cadence for walking barefoot was 61.59 ± 25.65 steps/min. compared to 50.94 ± 22.36 steps/min. with a solid AFO and 56.25 ± 24.44 steps/min with a hinged AFO. Significant differences in cadence and step length during walking were only demonstrated between the barefoot condition and when wearing a solid AFO. Significant difference was not observed between conditions in mean of ankle range of motion.
Conclusion:
The solid AFO was the only condition which improved cadence and step length in patients during ISCI gait training.
Clinical relevance
A solid AFO could be used permanently to compensate for impaired ankle function or it could be used while retraining stepping.
Background
Patients with incomplete spinal cord injury (ISCI) do not have the ability to walk unaided. Foot clearance is difficult to achieve because of reduced hip, knee and ankle motion during swing phase of gait resulting in a drop foot condition.1-4 These problems are a commonly demonstrated pathology during walking after an ISCI.1,5
Reduced muscle power and spasticity may also be observed in ISCI patients post-injury, which also adversely affects walking patterns. Appropriate ankle joint motion forms an important part in normal walking, 6 and feedback from the ankle joint mechanoreceptors is important in the control of human gait,7-8 but individuals with ISCI unfortunately demonstrate abnormal ankle kinematics. 9 Due to the important role that the ankle joint has in the control of gait, it is therefore critical to provide adequate and appropriate support to the ankle joint during gait training for these patients.
To facilitate the rehabilitation of ISCI patients, powered gait orthoses utilizing treadmills have been developed for clinic environments.10-12 The main part of rehabilitation training involves the task-specific practice of walking with as normal a gait pattern as possible to restore gait recovery.10,12 Training with a body weight support mechanism has demonstrated improvements in gait patterns, walking speed and endurance.11,13-15 However, these types of assistive device designed for gait training only assist the knee and hip joints, and commonly offer no support for the ankle. Support and guidance of the foot and ankle is commonly applied by therapists via manual assistance during treadmill walking of SCI subjects.
The rehabilitation of walking for ISCI patients mainly involves mechanical orthoses, which are designed to control the range of motion (ROM) in the impaired joints or limb.16,17 An ankle foot orthosis (AFO) is one type of orthosis which may also be used to provide walking assistance by decreasing plantarflexion and providing dorsiflexion at the ankle joint.18-20 This type of orthosis could prove beneficial when used in powered gait orthoses for gait training purpose in rehabilitation of walking of ISCI patients. Furthermore, improvements in gait parameters, 21 walking performance, confidence and safety, 22 have also been reported with an AFO.
Few studies have identified the effect of AFOs during walking on the lower limb kinematics of spinal cord injury (SCI) patients when performing gait training. Gregory et al. reported that a powered AFO provided approximately 50% of normal peak ankle torque during gait, and also that the ankle angle at push-off during stance phase increased as compared to walking with a passive-orthoses in five ISCI patients. 23 Nair et al. reported that hip extension, ankle plantarflexion and plantarflexor power were all significantly reduced during late stance when healthy subjects walked with ankle foot orthoses. However, hip flexion and ankle plantarflexion increased and the loading rate and braking force reduced significantly during swing-to-stance transition. 24 They therefore suggested that an AFO could improve transition phase kinematics and kinetics in ISCI patients.
The aim of this study was therefore to ascertain the effect of two designs of AFO on facilitating gait improvements during treadmill training. The aim was to evaluate the effect of AFOs with and without ankle hinges on the gait parameters of ISCI subjects during this activity. To study these effects, customized solid AFOs and hinged AFOs with plantar flexion stops were constructed for each volunteer subject. The two AFO designs to be compared were chosen in preference to other designs (such as the use of ground reaction AFOs) because the two AFO designs could be manufactured with similar trimlines, superstructures and footplate designs for each volunteer SCI subject. Therefore, the alteration and the effect on the outcome measures chosen could be isolated to the lack of intimate contact around the malleoli areas and provision of ankle ROM adjustment via the orthotic ankle joints in the articulating AFOs when compared to the solid AFOs.
The hypothesis was that ankle joint kinematics, step length and cadence, (the most important gait parameters which define ambulatory ability during gait training by SCI subjects) would all be improved when walking with AFOs which either blocked sagittal plane ankle motion, or only allowed ankle dorsi flexion, when compared to a non-orthosis condition.
Methods
Patients were referred with a diagnosis of incomplete spinal cord injury by an orthopedic surgeon to the orthotics and prosthetics department of University of Social Welfare and Rehabilitation Science. Three males and two females (height 169 ± 0.07 cm; weight 68.6 ± 7.4 kg; age 28 ± 8.68 years; mean ± SD) with ISCI at the thoracic level with American Spinal Injury Association (ASIA) grades C-D participated in this study. According to the ASIA scale, in patients with grade C, motor function is preserved below the neurological level and more than half of key muscles below the neurological level have a muscle grade less than 3. In grade D, motor function is preserved below the neurological level and at least half of key muscles below the neurological level have a muscle grade of 3 or more.
Participants were required to be older than 18 years of age, be more than 6 months post-injury with no history of orthopedic complications, and to have a walking disability. Subjects read and signed a prepared consent form. The Ethics Committee of University of Social Welfare and Rehabilitation Sciences approved the study.
Two types of custom fitting AFOs (solid and hinged with a plantar flexion stop) were constructed for each patient using negative and subsequent positive casts of the leg and foot in order to potentially reduce gait anomalies and improve gait by increasing step length and increasing toe clearance. The AFOs were manufactured from 4 mm polypropylene and the hinges were of the adjustable type with a capability of providing a plantarflexion stop function (Karino Company, Iran). The trimline of the solid ankle foot orthoses was anterior to the apex of the malleoli to add some rigidity (Figure 1).
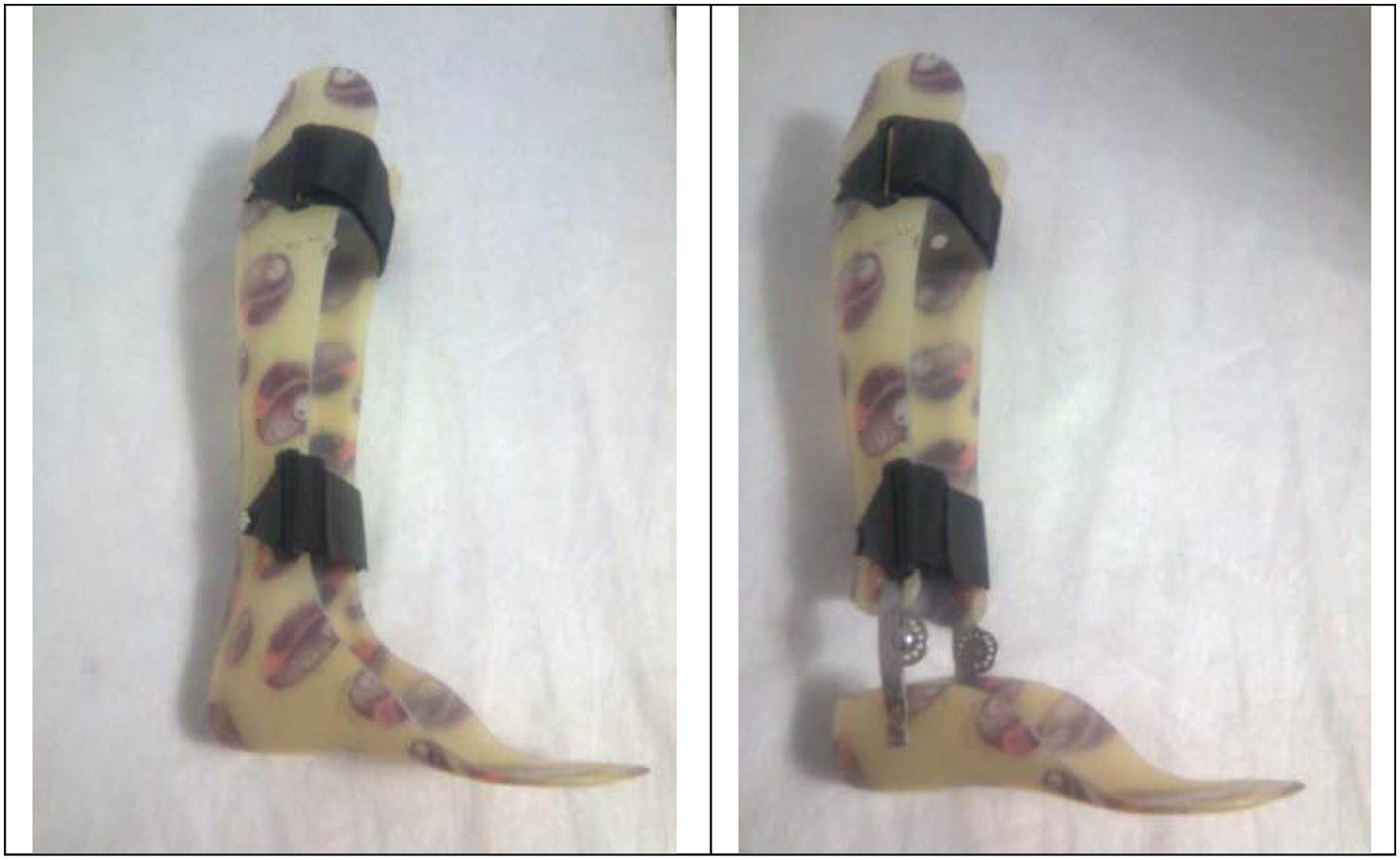
The solid ankle foot orthosis (AFO) and the hinged AFO (with a plantarflexion stop capability) used in this study.
According to the patient’s weight, a harness was used to support 60% of the subjects’ body weight to provide balance and support during the walking trials when using a treadmill. The treadmill was set at a constant speed of 0.54 m/s for all subjects. Three analyzing situations were considered: (1) without an orthosis (barefoot), (2) when wearing a solid AFO, and (3) when wearing a hinged AFO which was designed to prevent ankle plantarflexion but allow dorsi flexion. The AFOs were worn bilaterally during the walking trials. The ankle joint ROM hinges in the articulating AFOs were set individually, so that for each subject, the ankle was free to dorsiflex, but plantarflexion was prevented. This allowed a comparison to be made between AFOs allowing unfettered dorsi flexion, and those designed to prevent it. The walking speed selected was the same for each participant in order to be able to isolate the effect of the AFO conditions rather than having an additional variable of walking speed which may have had an additional influence on the selected outcome measures. The constant walking speed selected was similar to that typically used for adult walking training by SCI patients.
The order of testing for the conditions was randomized and all the subjects completed all three experimental tests. Each patient had 2 months of gait training time on the treadmill with the body weight support system when wearing footwear but without orthoses before the trials were commenced in order to become acclimatized with the experimental tests. All the patients wore the same style and make of shoes to ensure constant shoe pitch and heel height during all of the walking trials. However, it was necessary to increase the shoe size by one size for each subject while walking with the AFOs. Breaks were permitted after each experimental trial or when the patient needed a rest. Break times were variable and varied between 3 and 5 minutes.
Walking data were acquired using a six-camera VICON 640 system (Oxford Metrics, Oxford, UK). The data were processed at 100 Hz with VICON BodyBuilder (Oxford Metrics, Oxford, UK) using the standard model of the lower limbs included with the software. The data derived using the standard BodyBuilder model were then analyzed using MATLAB (MathWorks, Natick, MA). Fourteen markers were used in the lower extremities. Markers were placed bilaterally over the position of the ASIS, greater trochanter, lateral condyle of the femur, head and lateral malleolus of the fibula, the second metatarsal and the calcaneus.
Repeated measures one-way (by situations) analysis of variance tests (ANOVAs) were used to evaluate for differences in sagittal plane ankle ranges of motion, cadence and step length for all four patients (JMP IN software, SAS Institute, Inc.). We used Tukey Honestly Significant Difference (THSD) post-hoc tests to identify specific differences between groups. SPSS 16 was used for data analysis. The significant level considered was α = 0.05.
Results
The condition profiles of the patients with ISCI are reported in Table 1. The patients included in the study had injury levels between T5 to T12 and the mean time post-injury in these patients was 43.2 ± 12.29 months. According to the ASIA, all patients were ISCI with level C and D.
Patient information.
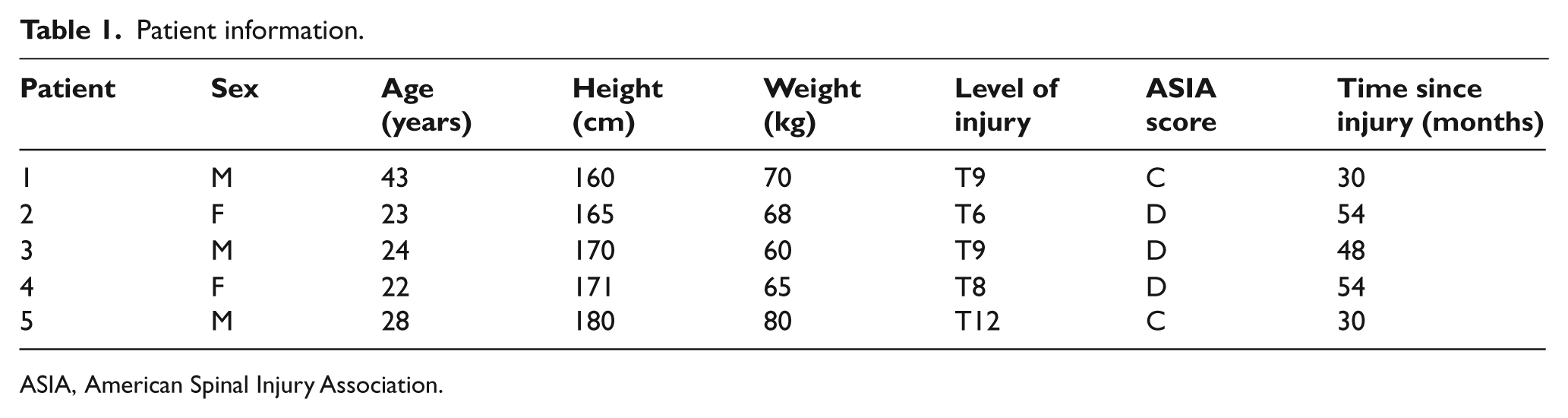
ASIA, American Spinal Injury Association.
Table 2 shows the mean and SD for the gait parameter measurements. Following confirmation that there were no significant differences between left and right lower limbs in the data acquired, results were calculated for the same number of steps for each subject (n = 30), and the steps for both sides were analyzed and averaged. The mean step length for walking in the barefoot situation was 26.3 ± 16.37 cm compared to 31.3 ± 17.27 cm with solid AFO and 28.5 ± 15.86 cm with hinged AFO. This difference in step length during walking was significantly only between barefoot and solid AFO conditions (Table 3). The mean cadence for walking in barefoot was 61.59 ± 25.65 (steps/min) compared to 50.94 ± 22.36 (steps/min) with a solid AFO and 56.25 ± 24.44 (steps/min) with a hinged AFO. This difference in cadence during walking was significantly only between barefoot and solid AFO (Table 3). The mean of ankle ROM improved when walking with orthoses, but no significant differences were shown between barefoot and orthosis types or between orthosis types (Table 3).
The mean ± SD of gait parameters with the solid AFO, hinged AFO and bare foot conditions.

AFO, ankle foot orthosis; ROM, range of motion.
Comparison of gait parameters between walking situations.
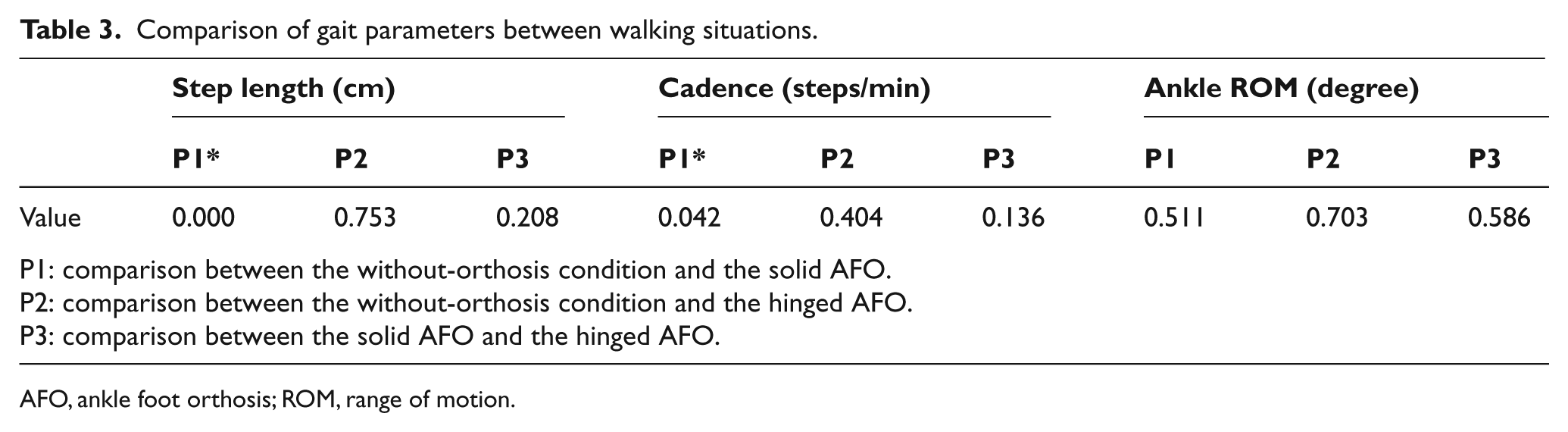
AFO, ankle foot orthosis; ROM, range of motion.
Discussion
The purpose of this study was to test the effects of solid and hinged AFOs on gait parameters during treadmill training by subjects with ISCI. The assistance offered by the orthoses resulted in gait parameter improvements at a walking speed of 0.54 m/s.
Ankle plantarflexor power is critical for forward body progression. 25 However, individuals with SCI typically lose plantarflexion power, and therefore have slower limb progression than matched healthy subjects. The generation of dorsiflexion assistive torque by an AFO is designed to alleviate this. 26 A solid AFO has been shown to decrease the ability of the ankle to generate power at push-off in healthy subject walking, 24 but stiffness of the foot section of an AFO can assist this parameter in SCI patients. 27
All SCI patients demonstrated a significantly increased in-step length and cadence when they walked with a solid AFO as compared to hinged AFO. Nair et al. proposed the use of a more rigid ankle foot orthosis to improve kinematics and kinetics in the walking of SCI patients. 24 The results from this study confirm this recommendation. The articulating AFOs were adjusted to prevent plantarflexion but allow unfettered dorsi flexion. This partially reduced the ankle ROM within the orthosis by blocking plantarflexion, but the results demonstrated no significant difference between any of the test conditions during ambulation even though ankle ROM was increased when walking with the articulated AFO. This would imply that it may be beneficial to restrict ankle ROM further in these patients when using an articulated AFO with a ROM adjustment facility, rather than just blocking ankle plantarflexion.
Appropriate foot clearance is important to facilitate and restore stepping and walking in the patients with SCI. Patients with ISCI have a slow pattern of walking, and also have difficulty in extension of the hip joint.1,4 In our study, the use of solid and hinged AFOs was shown to provide the desired foot clearance and meet the functional task requirements such as loading rate previously demonstrated in healthy subjects indicating that pattern of ankle joint motion was changed and the kinematics were improved.
The walking speeds provided by the treadmill were similar to those of a previous study which observed the gait of SCI patients. 28 This speed utilized during the testing is slower than that of normal walking 29 due to the absence of active ankle push-off30-31 and the absence of an ankle moment during this phase of the walking. The AFOs reduced cadence but increased step length when walking at a very slow walking speed compared to normal, which meant that inertial effects would be reduced and the lower limb would be in swing and stance phase for longer periods compared to normal walking. This may mean that more restriction to ankle sagittal plane motion may benefit SCI patients to allow more control over lower limb and foot positions during swing. This, however, is unproven.
The results of this study suggest that more research is needed into the effects of different AFO types in clinical practice for use by ISCI subjects, and that they may have the potential to improve the energy cost of walking in gait training rehabilitation. A limitation of the study was that kinetics and kinematic effect of the AFO test conditions on the hip and knee joints were not analyzed because of patient harnessing. The participants were unable to move their hips because the harness interfered with hip joint movements. Further research in this field is therefore required.
In addition, a minimal amount of walking tests was performed to ensure that the ISCI subjects did not get too tired during the walking trials. This indeed did prove to be a factor during the walking trials. While it is appreciated that walking with the footwear in isolation would have demonstrated the effect of the shoes themselves on the gait of these subjects, to ensure patient comfort and to facilitate a repeatable number of steps without the subjects getting too tired, this condition was not tested. Sensory input can utilize to relearn a normal stepping pattern in gait training in SCI patients. The primary goal is to progressively retrain the ability to walk rather than to immediately substitute for impaired walking. The emphasis is on training without an orthotic device in step training on the treadmill.
Conclusion
The use of a solid AFO in combination with appropriate footwear improved gait parameters in patients during ISCI gait training when compared to that demonstrated when walking with a hinged AFO with the same footwear. Task-specific programs are considered to play an important role in the rehabilitation of the impaired gait of individuals with SCI. This study demonstrated that AFOs manufactured without an ankle hinge can provide an adjunct benefit to powered gait orthosis gait training for this group of patients.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors