
Abstract
Object:
This article describes the translation and cultural adaptation of the Multi-disciplinary Rehabilitation Outcome Checklist Scale in Italian and reports the procedures to test their validity and reliability.
Methods:
The forward and backward translation was conducted by specialized and certified translators, independently from each other. The scale was then reviewed by a group of 20 experts. The process of cultural adaptation and validation took place on a cohort of patients who performed a joint replacement of hip and/or knee surgery in two hospitals of Rome.
Results:
The culturally adapted scale was administered to 114 patients. It results that the interoperator reliability is equal to intraclass correlation coefficient (ICC) = 0.977 for hip and ICC = 0.97 for knee. The construct validity and the responsiveness are statistically significant.
Conclusion:
It is a scale capable of assessing the patient in a comprehensive and multidisciplinary manner at the time of hospital discharge, useful for dismissing the patient in the most appropriate timing and with the best clinical and functional conditions.
Introduction
Due to the aging of population, the number of patients with osteoarthritis of hip and knee is constantly rising, which leads to an increase, worldwide, 1,2 in the number of total arthroplasty operations of these two districts. 3 In 2015, the annual incidence of total hip arthroplasty and total knee arthroplasty in Italy was, respectively, 68,891 cases, with a progressive annual increase of 3.0%, and 65,259 cases, with an increase of 6.6%. 4
Multidisciplinary collaborative management is essential to provide effective and efficient rehabilitative care to patients affected by arthroplasty, along with the use of clinical pathways, which studies show can allow the patients outcomes to be improved and reduce the risk of complications. 5 –7
The “New Multi-disciplinary Rehabilitation Outcome Checklist” (MROC) Scale was created in 2012 by Wong et al. 8 in China, which was able to evaluate and verify the rehabilitative outcome and the general conditions in patients undergoing total primary hip and/or knee replacement surgery at the time of hospital discharge.
It is able to combine the use of clinical pathways together with the management of a multidisciplinary team, thus ensuring a coverage of observations from different disciplines and allowing a more complete and holistic assessment. It is useful in the auditing process.
The MROC Scale is composed by a range of performances and discharge criteria established by the multidisciplinary team. The listed criteria are the target outcomes aimed to achieve in patients with total primary joint replacement of hip and/or knee at discharge.
It consists of eight items, which evaluate the mobility, the Range of Motion (ROM) of knee flexion in the case of total knee arthroplasty, the carrying on in a rehabilitation structure, the self-care, the washing, the healing state of the surgical wound, the pain score, and the length of hospital stay.
The aim of this study was to translate the current MROC Scale into the Italian language, culturally adapt it and validate it, and then be able to use it specifically in subjects with total primary hip and/or knee replacement.
The purpose is to provide a valid assessment scale for the risk of discharge of patients operated on total primary hip and/or knee arthroplasty, which can be used in all Italian structures, to reduce the chances of a new hospitalization in the short term and the so-called bed blockers. 9
Materials and methods
All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1975, as revised in 2008. Informed consent was obtained from all participants for being included in the study. We certify that all applicable institutional and governmental regulations concerning the ethical use of human volunteers were followed during the course of this research.
Translation process
The translation procedure includes three steps. First, two official translators, English native speakers, independently of each other, translate the original MROC (forward translation) into Italian language. This phase involves the joint work of a translator with a technical background and one with a medical background, the latter judging the efficiency of the translation. Subsequently, two bilingual people, independent from each other and unaware of the original version, translate the Italian scale into English. These last two translations of the English-language scale are then independently translated into Italian, unaware of the original version, by two health professionals with English language certification (backward translation). The score of the questions remains the same as the original MROC. Lastly, all the translators gathered to decide the definitive translation of the MROC Scale.
Cultural adaptation
With the purpose of adapting the translated scale to Italian culture, this was reanalyzed by a group of 20 experts specialized in different medical disciplines (Appendixes 1 and 2). Experts have the opportunity to comment on the elements of translation by inserting their comments on a form. Once tested for validity and reliability, the translation judge examines this final version of cultural adaptation and approves it.
Patients and validation procedures
The validation process is based on a cohort of patients admitted to two different hospitals that provide assistance for total hip and knee arthroplasty in Rome, Italy. The transcultural validity of the scale and the test–retest reliability has been tested on all patients involved in the study.
All cases of hospitalization at the Tor Vergata Hospital and the Umberto I Hospital between April 2018 and November 2018 were examined for inclusion in the study. The study was approved by the Ethics Committee of the participating hospitals. All patients were informed about the dynamics of the study; those who underwent the study, therefore, gave their consent before being included in it. 10,11 Cases of underaged were excluded, as were patients with cognitive disabilities, those who misunderstand the Italian language, revision or nontotal arthroplasty, patients with nonorthopedic complications for which they were transferred to other departments, and those who did not agree to enter the study.
The scale was administered by two operators who were prepared for administration before starting evaluations.
To evaluate the reliability, the MROC Scale has been used as Gold Standard scales, the scales within the scale itself: the Barthel Index (BI), 12 the Visual Analog Scale for Pain (VAS), 13 and the Modified Functional Ambulation Classification (MFAC). 14
All statistical analyses were performed through Statistical Package of Social Sciences, version 18.0 for Windows. The description of the variables was made using frequency tables, averages, and standard deviations.
Administration
The version of the MROC Scale culturally adapted in Italian has been administered to all study participants by the two operators—the same physiotherapist who takes care of the study (rater 1) and a second operator, such as a trainee, a physiotherapist, a nurse, or a doctor (rater 2) —to verify that the scale works correctly and that it provides unanimous values regardless of the operator who administers it.
In the test phase, the scale was administered to all patients at the time of discharge from the hospital (T0). The scale was administered a second time, 25 days after discharge (T1) on a cohort of patients, with the so-called responsiveness, to be able to evaluate the changes recorded in this time frame. All patients after discharge were admitted to rehabilitation unit, with 3 h of daily physiotherapy (code 56) for a period of about 25 days.
Test–retest interrater reliability
A test–retest interoperator analysis was performed to evaluate the reproducibility of the MROC Scale. From the two evaluations conducted for each patient, one is chosen randomly, which is used to measure the test–retest reliability through the calculation of intraclass correlation coefficient (ICC). The scale is considered reliable when the ICC has a value greater than 0.70.
Internal consistency and construct validity
Cronbach’s αis used to evaluate and describe the internal consistency of groupings of items. A value above 0.70 is considered meaningful. Pearson’s correlation coefficient is used to evaluate the construct validity. A value above 0.70 is considered meaningful.
Results
Patients
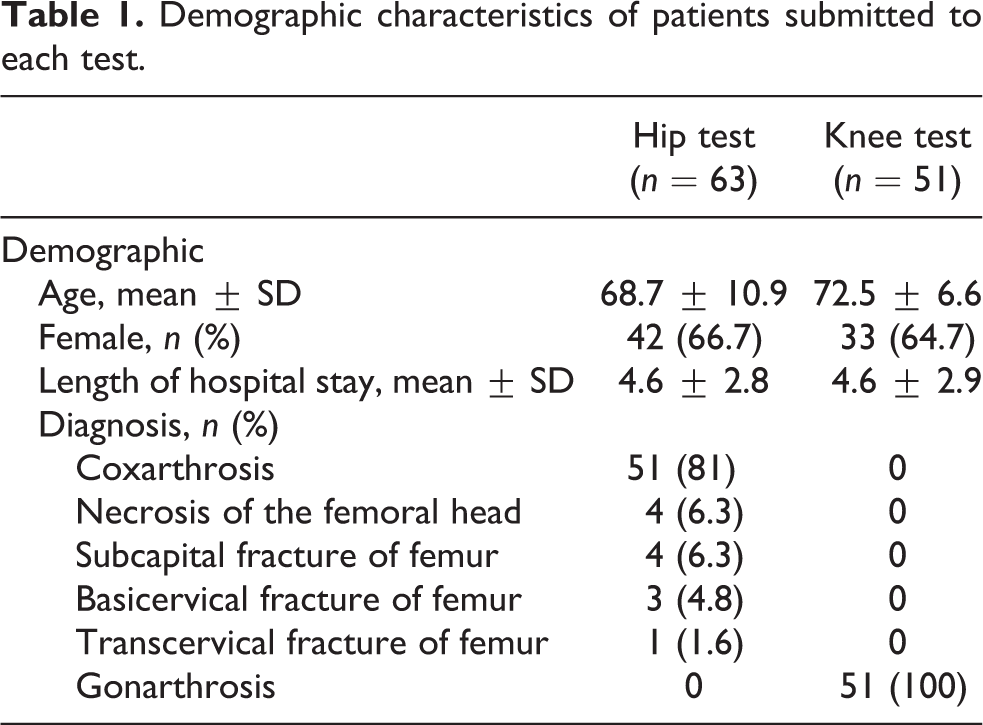
In the beginning, the patients evaluated for their inclusion in the study were a total of 141; 27 (19%) patients did not fulfill the inclusion criteria, resulting in a total number of 114 patients to whom the Italian culturally adapted MROC was administrated. Among them, there were 63 total hip replacement patients and 51 total knee replacement patients. Demographic characteristics are reported in Table 1.
Demographic characteristics of patients submitted to each test.
Reliability
Test–retest and interrater reliability
All patients participating in the study involved in the procedures for assessing the reliability of the MROC Scale. The value of the ICC in the many administrations was 0.977 (95% CI: 0.955, 0.999) for hip and 0.97 (95% CI: 0.943, 0.997) for knee, with a p < 0.01.
Construct validity
It was calculated on all 114 patients participating in the study using the Pearson correlation coefficient, to evaluate the correlation of the MROC Scale with the Gold Standard scales. Both for hip and for knee, the results show statistically significant values: BI = 0.583 for the hip and 0.542 for the knee, VAS = −0.53 and −0.57, MFAC = 0.478 and 0.53, with a p < 0.01.
Responsiveness
Responsiveness was calculated on a cohort of 33 cases, 17 for hip (mean age = 65.5 ± 9.2 years, 6 males, 11 females) and 16 for knee (mean age = 72 ± 4.4 years, 4 males, 12 females). Wilcoxon signed ranks test reveals a change between the first evaluation and the subsequent follow-up. Wilcoxon signed ranks test values are reported in Table 2.
Result of Wilcoxon signed ranks test.
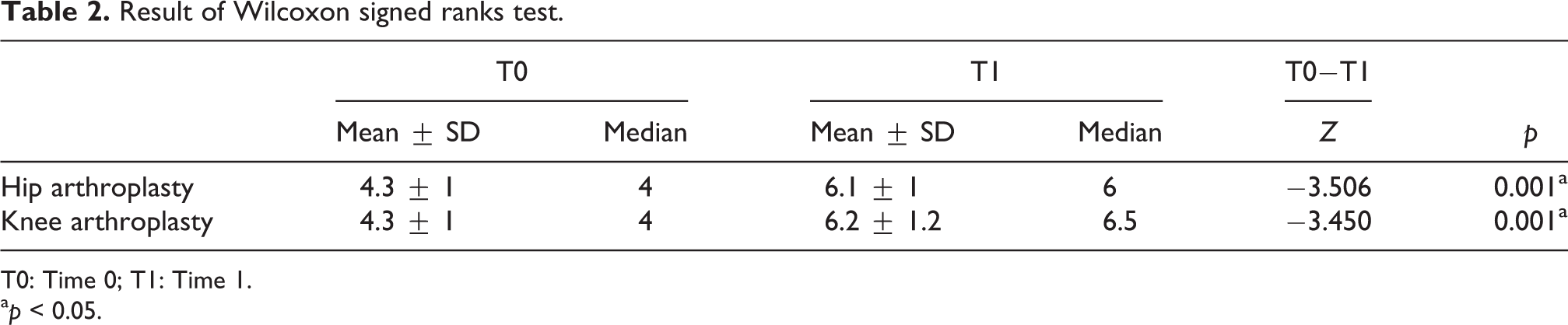
T0: Time 0; T1: Time 1.
ap < 0.05.
Discussion
The present study was conducted by health professionals of Sapienza University of Rome and ROMA—Rehabilitation & Outcome Measures Assessment Association. The research group has carried out many outcome measures in Italy. 15 –24
The purpose of this study was to translate the MROC Scale into Italian and adapt it culturally and validate it. Translation and cultural adaptation have been carried out applying internationally recognized methods, and experts have also ensured that the original meaning of the scale is maintained.
The internal consistency was calculated on all the 114 included cases. Cronbach’s α cannot be determined because some items have a continuous repetitive score of 0 or 1.
The test–retest interoperator reliability is equal to 0.977 for the hip and 0.97 for the knee, with a p < 0.01; the ICC value ≥0.70 is considered optimal to establish the degree to which repeated measurements are error free. The construct validity shows all statistically significant values. Validating that the MROC Scale proves and evaluates the same aspects evaluated by the others Gold Standard: to a high MROC score corresponds a high Barthel and MFAC score, negative because of the inverse proportionality compared to the VAS score (to a high MROC score corresponds a low VAS score).
Responsiveness shows all statistically significant values: The scale is able to evaluate patient change and improvement.
It is estimated that the number of total primary hip and/or knee arthroplasty will increase by 100% within the years 2025–2030. This is due, on the one hand, to the increase in life expectancy and to the close correlation that exists between the onset of joint pathologies and the advancing age and, on the other hand, to the continuous improvements made both by the surgical technique and to the characteristics of implanted devices, which allow to perform interventions on increasingly younger patients.
It is therefore necessary for the existence of a scale in Italy that can help hospital facilities in the management of these prosthetic patients, to be able to discharge them in the most appropriate times with the best possible clinical and functional conditions.
Limitations of the study
This study presents some limits. Limits concerning the standardization of the MROC Scale at the level of the Italian population, which led to the impossibility of calculating a precise cutoff. It is due to the criteria established by the original scale, conceived in China, where there are different ranges of values compared to those present in the Italian reality. A limit is represented by the length of the hospital stay, whose value is ill-suited to the Italian reality (duration 3–7 days) making the data less sensitive for the analysis of the data, such as the impossibility of calculating Cronbach’s α.
This implies a modification of the assessment, at the time of discharge, of the different functional abilities of the patient, since the greater Chinese hospitalization times favor a functional recovery of a higher entity. It is therefore necessary to make changes to the scale translated into Italian to adapt it to the parameters of the nation, ensuring greater precision and effectiveness.
Conclusions
The study is the validation of an instrument in Italian for the assessment of the risk of discharge of patients with total hip and/or knee replacement, a scale that aims to assess the outcome of the prosthetic patient in a multidisciplinary manner in its entirety. The MROC Scale has also proved to be a valid, reliable, acceptable scale, easy to understand, and quickly administrable in Italy.
It is able to evaluate the patient’s change and improvement in an optimal manner, excellent for assessing the risk of discharge of orthopedic patients—to prevent risks that could lead to early discharge—and to be able to direct patients to an appropriate rehabilitation path and with the most appropriate aids.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Appendix 1
Italian cultural-adapted MROC—Total knee replacement
Appendix 2
Italian cultural-adapted MROC—Total hip replacement