
Abstract
Objective:
Acute rupture of the distal biceps tendon is relatively uncommon, and surgical repair is advocated for acute injuries to restore strength and function. Numerous techniques are described in the literature, with no true consensus regarding the optimal method of fixation. The aim of this study was to evaluate patient-reported outcome measures, clinical outcomes and complications for patients undergoing distal biceps tendon repair using two fixation techniques: cortical button and suture anchor.
Methods:
A retrospective single-unit case series of 51 cases (50 patients) underwent distal biceps tendon repair, comprising 19 cortical button and 32 suture anchor fixations. Patients were assessed using the Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire and overall satisfaction. Clinical outcomes and complications were reviewed from patient records.
Results:
Thirty-eight (76.5%) patients responded to DASH questionnaires with a mean follow-up of 189 weeks (11.5–425 weeks). Mean DASH scores for cortical button and suture anchor groups were 6.2 (0–30.8) and 3.3 (0–16.7), respectively (p = 0.21). Eight patients (16%) reported lateral cutaneous neuropraxia in the early post-operative period. All but two of these patients experienced complete resolution at the final follow-up. One patient had heterotrophic ossification, which did not require any further intervention. There was one re-rupture (suture anchor), but the patient declined further surgical intervention.
Conclusion:
There were no statistically significant differences in the patient-reported outcome measures, overall satisfaction and complication rate between patients undergoing either method of fixation.
Level of evidence:
III
Introduction
Rupture of the distal biceps tendon is relatively uncommon with a reported incidence of 0.9–1.8 per 100,000 people per year. 1 The dominant arm is affected in the majority of cases, with a greater prevalence in males aged 30–50 years. 2 The usual mechanism of injury is a rapid eccentric contraction with the elbow flexed, usually against a heavy load, although commonly there is evidence of pre-existing tendinopathy. 3
Surgical repair is advocated for acute injuries to restore strength and function, particularly of forearm supination, although rarely non-surgical management may be advocated in patients with low functional demand. 4 The aim of surgery is anatomical reconstruction of the biceps tendon. Numerous techniques are described in the literature, with no true consensus regarding the optimal method of fixation. 5 Commonly reported methods include suture anchors and cortical buttons, with many studies reporting comparable outcomes. 6 –8
While it is clearly desirable to restore strength and function following this injury, there are inherent risks to surgery. The reported surgical complications include infection, neuropraxia of the lateral cutaneous and posterior interosseous nerves, and less commonly, heterotrophic ossification (HO) and re-rupture. 9
The aim of this study was to compare the clinical and functional outcomes of cortical button and suture anchor fixation for anatomical surgical fixation of distal biceps rupture. The hypothesis was that there would be no significant difference in the clinical and functional outcomes between the two methods of fixation.
Methods
All patients who had undergone surgical repair of distal biceps tendon in a single district general hospital (DGH) were identified retrospectively via the computerised theatre records system (ORMIS TM). Cases were identified from data between January 2010 and December 2017. Criteria included acute primary distal biceps repair, with complete rupture usually confirmed by magnetic resonance imaging/ultrasound (MRI/US) imaging.
Surgical information and clinical outcomes were collated via the clinical records system (CWS). Functional outcomes were obtained via telephone interview. The Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire was used. All patients who were contacted by telephone gave verbal consent to taking part in this aspect of the study. The DASH outcome measure is a validated 30-item, self-report questionnaire designed to assess the patient’s health status during the previous week. The items enquire about the degree of difficulty in performing different physical activities because of arm, shoulder and hand problems (21 items), the severity of each of the symptoms of pain, activity-related pain, tingling, weakness and stiffness (5 items) and the impact of the problem on social functioning, work, sleep and self-image (4 items). Each item has five response options. The scores are then used to calculate a scale score ranging from 0 (no disability) to 100 (most severe disability). 10
Patients were also asked to rate their overall satisfaction on a numerical rating scale (NRS), where 0 was least satisfied and 10 was most satisfied.
Exclusion criteria included other ipsilateral upper limb injury at the time of surgery, tears requiring allograft or autograft, tears which were found to be irreparable at the time of surgery and significant reported pre-existing ipsilateral upper limb pathology such as ipsilateral cerebrovascular accident (CVA) or musculoskeletal disorder, which may have influenced functional outcomes. No patients were excluded using these criteria.
Surgical methods
All of the patients underwent surgery under general anaesthesia. Surgery was undertaken with the patient supine, with an armboard to position the affected limb in elbow extension and supination. A tourniquet was used in all cases.
A single incision technique was utilised in all cases. The incision was transverse, just distal to the antecubital crease, and was extended proximally and distally as required. The ruptured end of the tendon was identified, and released as required to allow the tendon to be mobilised. Debridement and freshening of the tendon was performed as deemed necessary. The radial tuberosity was identified under direct vision.
In cases using cortical button fixation, a 1.8-mm guide pin was drilled into the radial tuberosity, and the position was confirmed using the image intensifier. The cortical button (EndoButton, Smith and Nephew TM) was sutured to the tendon using a Krakow suture technique using number 2 Ethibond (Ethicon TM). The tuberosity was reamed to 4.5 mm over the guidewire, and the cortical button was passed through the tunnel and flipped. The final position was confirmed with imaging.
In cases using suture anchor fixation, a 2.4-mm hole was drilled into the radial tuberosity, and the 2.4-mm Super Anchor (Depuy Synthes TM) suture anchor was inserted. The integral sutures were then attached to the tendon using a Krakow technique, and the sliding mechanism of the suture anchor was used to pull the tendon down to the tuberosity, which was then tied.
All wounds were closed in layers and a plaster of Paris backslab was applied in flexion and supination. Follow-up was at 2 weeks for wound check and then as deemed clinically appropriate. Graduated mobilisation was allowed in all cases to protect the repair and reduce elbow stiffness.
Results
Demographics
A total of 51 cases (50 patients) were identified and screened to ensure they met the inclusion criteria. All patients were male, with a mean age of 41 years (24–61 years). The mean time from rupture to surgery was 12.6 days (1–46 days). Nineteen patients underwent fixation with cortical button, while the remaining 32 underwent suture anchor fixation. There were no reported intraoperative complications in either group. Key demographics are listed in Table 1.
Demographic findings.

Clinical outcomes
The duration of clinical follow-up ranged between 11.5 weeks and 425 weeks (mean 189 weeks). All but the most recently operated had either been discharged from clinical follow-up with a clinically satisfactory outcome (42) or had not attended their last planned clinical review and, subsequently, were lost to follow-up (8). One patient had ongoing pain and underwent US-guided injection of bupivacaine and triamcinolone to the biceps tendon, which had subsequently led to a resolution of symptoms.
The review of clinical documentation from the last appointment confirmed that all patients who were formally discharged were happy with their symptoms and function, and there were no clinical concerns identified.
Functional outcomes
Thirty-eight (76.5%) patients responded to the DASH questionnaire. The interval from surgery ranged from 12.7 weeks to 425 weeks with a mean follow-up of 183 weeks.
The mean DASH scores for the cortical button and suture anchor fixation groups were 6.2 (0–30.8) and 3.3 (0–16.7), respectively (p = 0.21), as presented in Table 2.
DASH scores.
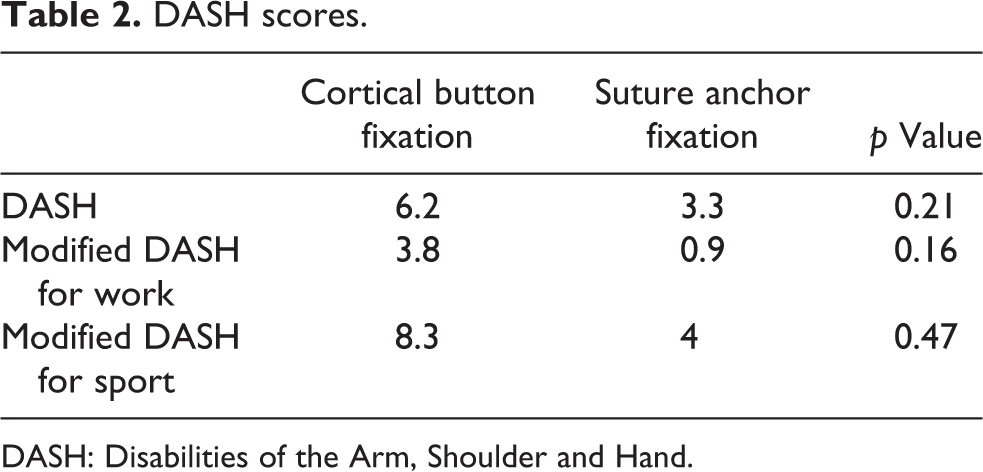
DASH: Disabilities of the Arm, Shoulder and Hand.
The optional mean DASH scores for the working population for the cortical button and suture anchor groups were 3.8 (0–25) and 0.9 (0–12.5) (p = 0.16). The optional mean DASH scores for athletes and musicians were 8.3 (0–43.8) and 4 (0–25) (p = 0.47). All patients were able to return to previous work, sports and playing of musical instruments.
The overall patient reported satisfaction was 9.4/10 on NRS.
Complications
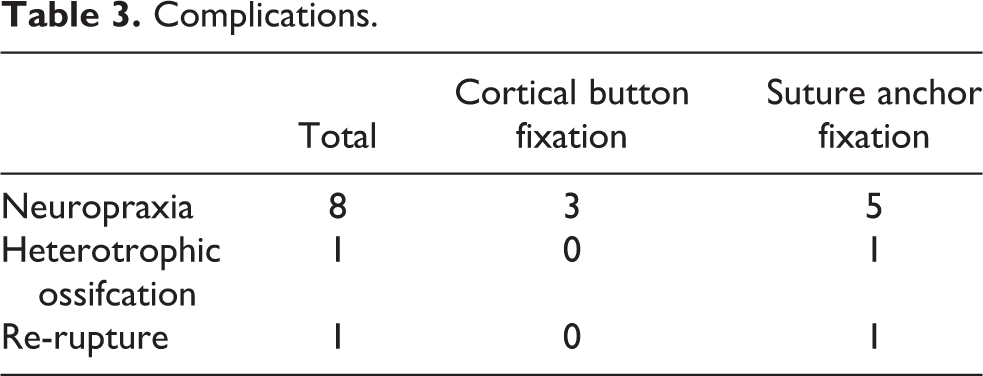
Eight patients (16%) reported lateral antebrachial cutaneous nerve neuropraxia in the early post-operative period: five in the suture anchor fixation group and three in the cortical button group. They all described paraesthesia in the distribution of the lateral cutaneous nerve. All but two of these patients experienced complete resolution by the final follow-up (one in each group). Of the two patients with ongoing symptoms, both reported no loss of function and no further intervention was planned. No posterior interosseous nerve injuries were documented.
One patient had heterotrophic ossification on plain radiograph, but as this was asymptomatic no further intervention was required (suture anchor). There was one re-rupture (suture anchor), but the patient declined further surgical intervention due to other medical conditions. There were no superficial or deep wound infections documented. Table 3 demonstrates these findings.
Complications.
Discussion
This article reports the clinical and functional outcomes of a cohort of patients undergoing primary repair of distal biceps tendon rupture in a DGH, using two methods of fixation.
The cohort studied is representative of the typical demographic of distal biceps rupture. 2 Two patients, both in the endobutton group, underwent fixation at 32 and 46 days, respectively, which may be considered outside of the range for acute repair. However, this did not cause any statistical significance in the time-to-surgery between the groups, and these cases were included in analysis as it was felt to be representative of pragmatic clinical practice. No other significant differences in baseline demographics were identified between the cortical button and suture anchor fixation groups. There were no statistically significant differences in the patient-reported outcome measures (PROM), overall satisfaction and complication rate between patients undergoing either method of fixation.
These functional results are in line with other papers comparing similar groups of patients. 5,11,12 The mean DASH score in this cohort was 4.9; a DASH score ranging from 0 to 29 is considered to be the point where patients were no longer considered their upper limb disorder a problem. 10 In their retrospective sample of 28 patients with a mean follow-up of 3 years, Reichart et al. report mean DASH scores of 14.39 in the cortical button group and 23.01 in the suture anchor group. 5 Similarly, in a case series of 46 patients, 93% were satisfied with the results and more than 80% of patients had regained their premorbid function in both recreational and occupational activities. 11 This article adds further evidence that surgical repair of ruptured distal biceps reliably restores upper limb function.
Complications of surgery can be classified as major, such as re-rupture, posterior interosseous nerve palsy, reoperation and symptomatic heterotrophic ossification requiring intervention, and minor, such as superficial wound infection and temporary paraesthesia of the lateral cutaneous nerve of the forearm. 13 A large retrospective case review examined 970 cases over a 12-year period, performed at a single site by multiple surgeons. The authors reported a 7.5% major complication rate and 4.5% reoperation rate overall. 14
One re-rupture was identified in the cohort, which occurred at 7 days post-operatively, and confirmed with imaging. As no form of radiological investigation was routinely undertaken to confirm tendon integrity post-operatively, in line with routine clinical practice, it is possible that patients who were not contactable for DASH scores could have moved out of the area and subsequently re-ruptured. This would not be known due to the study data collection methods.
Re-rupture occurred in a patient in the suture anchor fixation group. Cadaveric biomechanical studies have shown variable outcomes of fixation strength. Some papers report that cortical button fixation can withstand greater loads before failure; 15 others found that suture anchors demonstrate the ability to tolerate greater load before failure. 16 The sample size in this cohort is too small to draw any conclusions regarding fixation failure rates between the two methods of fixation.
An overall 16% incidence of early lateral antebrachial cutaneous neuropraxia was observed, although this completely resolved in all but two patients. These remaining two patients did not undergo any further intervention related to this. This rate compares with an incidence of 9.8–14% reported in the literature. In a meta-analysis of 87 papers, incorporating 1283 patients, lateral antebrachial neuropraxia was observed in 9.8% of patients who underwent repair using a single incision technique, although symptom duration or resolution is not clearly stated in this article. 9 The duration of symptoms in the two patients in this cohort, and whether complete resolution occurred, is unknown, as both patients were discharged with ongoing symptoms as they were unconcerned with their presence. This is a limitation of this type of retrospective study.
Other papers have also noted that the single incision repair technique, used in all cases in this cohort, is associated with greater rates of lateral antebrachial cutaneous neuropraxia. 14 This may explain the rate at the higher end of that described by other papers. 9,14,17 There were no reported posterior interosseous nerve injuries.
The rate of HO (0.5%) was considerably lower than that reported in the literature at 2.9–7.2%, 9,13 although the actual incidence may be underestimated in this series. HO in asymptomatic cases would not have been identified as routine post-operative radiographs were not undertaken, in line with common clinical practice. It is reported to be higher in cases where a double incision technique is used. 9 As the single incision technique was used in this cohort, this may explain the lower rate.
There are limitations to this study, particularly the study design. This was not a randomised study, it was single blinded, and data collection was retrospective without a consistent follow-up schedule. The retrospective data collection may have a reduced bias. Additionally, data regarding clinical assessment of outcome such as strength testing, or radiological confirmation of tendon healing or heterotrophic ossification, has not been obtained. Although physical assessment of clinical outcomes such as strength testing was not undertaken, a robust PROM was undertaken in a significant proportion of patients. The outcomes of a clinical intervention obtained by the patient, that is, patient-reported outcomes are deemed to be of more importance in future than any other outcomes. 18
Despite these limitations, however, this study is both pragmatic and representative of the clinical practice in smaller hospitals. It is a large sample size with a significant period of follow-up and a validated, robust PROM.
In conclusion, in this case series, both methods of fixation resulted in similar satisfactory clinical outcomes and a complication rate similar to that reported in the literature. Therefore, both techniques can be recommended for primary repair of distal biceps rupture, and patients can be counselled appropriately.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.