
Abstract
Introduction:
The direct anterior approach (DAA) for hip arthroplasty has gained popularity in recent years with numerous articles suggesting that short-term outcomes are advantageous over alternative approaches. The ‘bikini’ inguinal crease line incision is a novel variant of the DAA, which reduces the scar.
Methods:
We conducted a retrospective cohort study to assess functional and general health outcomes and complications of the two different surgical incisions used in DAA total hip arthroplasty (i.e. ‘bikini’ and longitudinal incisions).
Results:
We found no statistical difference between the novel bikini incision and the traditional DAA hip arthroplasty.
Conclusion:
This approach offers a cosmetically improved scar with no compromise in outcomes.
Introduction
The direct anterior approach (DAA) total hip arthroplasty (THA) has gained popularity over recent years with numerous studies, suggesting that DAA patients have a faster recovery, reduced post-operative pain, earlier mobilisation and lower rates of dislocation than those with operated through alternative approaches. 1 –5 These benefits have been attributed to the muscle-sparing nature of the procedure and the intervascular and internervous plane used. 6 Detractors of the DAA suggest that the operation has a long learning curve, greater blood loss and higher complications than alternative approaches. 7
One of the frequently cited criticisms of the DAA is that because the skin incision runs perpendicular to Langer’s lines, it leads to widening and discomfort of the scar. 8 The oblique ‘bikini’ incision for the DAA was developed by Leunig et al. to tackle this problem. 6 By placing the incision within the inguinal skin fold, the scar runs parallel with Langer’s lines resulting in a narrower and more subtle scar. 8 Cosmesis is subjectively and objectively improved with this approach 6 and so advantageous for patients conscious of aesthetics. In addition, initial articles show this technique to be safe with no difference in lateral femoral cutaneous nerve symptoms. 6
There are no sizeable studies so far that compare outcomes of ‘bikini’-incision DAA with longitudinal-incision DAA THAs. This article addresses this by comparing the functional outcomes, general health outcomes and complication rates of ‘bikini’ and longitudinal incision DAA THAs at 6 months post-operatively.
Methodology
Patient selection
We conducted a retrospective cohort study to compare the two different surgical incisions used in DAA THAs (i.e. ‘bikini’ and longitudinal incisions). All the patients who underwent THA in our centre between January 2013 and July 2015 were included. Information on patient and operation details as well as Oxford hip scores and EuroQol scores was previously recorded within a cloud-based medical records platform ‘iMedDoc’ and so was easily extractable. We excluded all the patients who underwent an approach other than longitudinal or bikini DAA, had an incomplete follow-up at 6 months and had missing preoperative scores or underwent revision surgery.
Clinical features and treatment option
The database was interrogated for the following: age, sex, date of surgery, surgical approach, incision type, preoperative and 6-month Oxford hip and EQ-5D scores. To minimise potential bias, all patients in both groups were operated on by the same surgeon. The surgeon started performing the ‘bikini-incision’ DAA in March 2014, prior to which all THAs were performed via a longitudinal DAA. Initially, the surgeon selected thin-female patients for the ‘bikini-incision’, but over time, he used the bikini incision for all THAs.
Operative description
The longitudinal-incision DAA was performed as has been described by previous authors. 9 The bikini-incision DAA is performed on a standard table with the pelvis placed at the break to enable extension. Both legs are draped, with the non-operative leg placed on a mayo table to allow adduction of the operative leg. A line is drawn between the anterior superior iliac spine and the fibular head. A 3–5 inch incision is made in the inguinal crease line, with one-third medial and two-third lateral to the previously drawn line. Subcutaneous tissues are incised with diathermy and the fascia covering the tensor fascia lata was incised longitudinally. Blunt dissection is performed between the sartorius and tensor fascia lata until the lateral aspect of acetabulum can be palpated. The deep fascia of the tensor fascia lata is incised longitudinally and a capsular flap created. With the femoral head still in the acetabulum, a femoral osteotomy is performed and the femoral head was removed with a corkscrew. The preparation of the femur and insertion of the stem are done with the foot lowered to extend the hip to 10–30°. Both cemented and cementless cups are used dependent on patient age and bone quality. The foot-end is then raised back to neutral, which allows full visualisation of the entire capsule. The labrum is removed, the acetabulum reamed with a straight reamer and the acetabular cementless cup inserted. An alignment rod is used to aid assessment of inclination of the acetabular component. The stability of the hip is assessed intraoperatively, and the wound is closed in layers; skin closure is performed with staples. No drains are used.
Analgesia and physiotherapy regimes are the same for both groups. Local anaesthetic is infiltrated into the wound during the operation and oral post-operative analgesia provided. Physiotherapy is commenced at day 1 post-operatively in both groups and patients encouraged to fully weight bear. Discharge is considered once deemed safe by physiotherapists and doctors.
Clinical evaluation
Functional and general health outcomes were recorded using validated Oxford hip and EQ-5D scores. 10,11 These were patient-completed and collected by an outcome nurse during the patient’s preoperative and 6-month post-operative assessments.
The Oxford hip score is a functional score to assess hip function. It is made up of 12 questions each with a score of 0–4, it has a maximum score of 48 (i.e. perfect function). 11 The EQ-5D score is a health-related life quality score that measures five key tenants: mobility, self-care, usual activities, pain or discomfort and anxiety or depression, which can be graded as ‘no problem’, ‘a moderate problem’ or an ‘extreme problem’. 12 EQ-5D range is from −0.594 to 1, where 1 is full health and 0 equates to being dead (negative values are valued as worse than being dead). 13 These measurements have been shown to be valid and reliable. 10 We used the change between preoperative and 6-month Oxford hip and EuroQol scores as a proxy for the level of functional and general health improvement after a THA. 11
Complications were collected by a standardised telephone pro forma led consultation. This included asking about myocardial infarctions, stroke, deep vein thrombosis, pulmonary embolus, deep and superficial infections, nerve palsy, hip dislocation and further surgery up to 2 years post-operatively. Any patient reported complications were verified with the patient’s general practitioner.
Statistical analysis
We used statistical software SPSS 17.0 software (SPSS Inc., Chicago, Illinois, USA) for statistical analysis. Mean values are presented with their corresponding standard deviations. Normal distribution of continuous variables was tested using the Shapiro–Wilk test. Differences between non-parametric variables were analysed using the Mann–Whitney U-test. The results were considered significant when two-tailed p values were <0.05.
Results
Patient demographics and clinical features
A total of 273 patients underwent THA via the DAA between January 2013 and September 2015, with 214 fulfilling our inclusion criteria (Figure 1). Of these, 90 were performed via a bikini-incision and 124 via a longitudinal-incision. There were no significant age and sex differences between the two groups (Table 1).
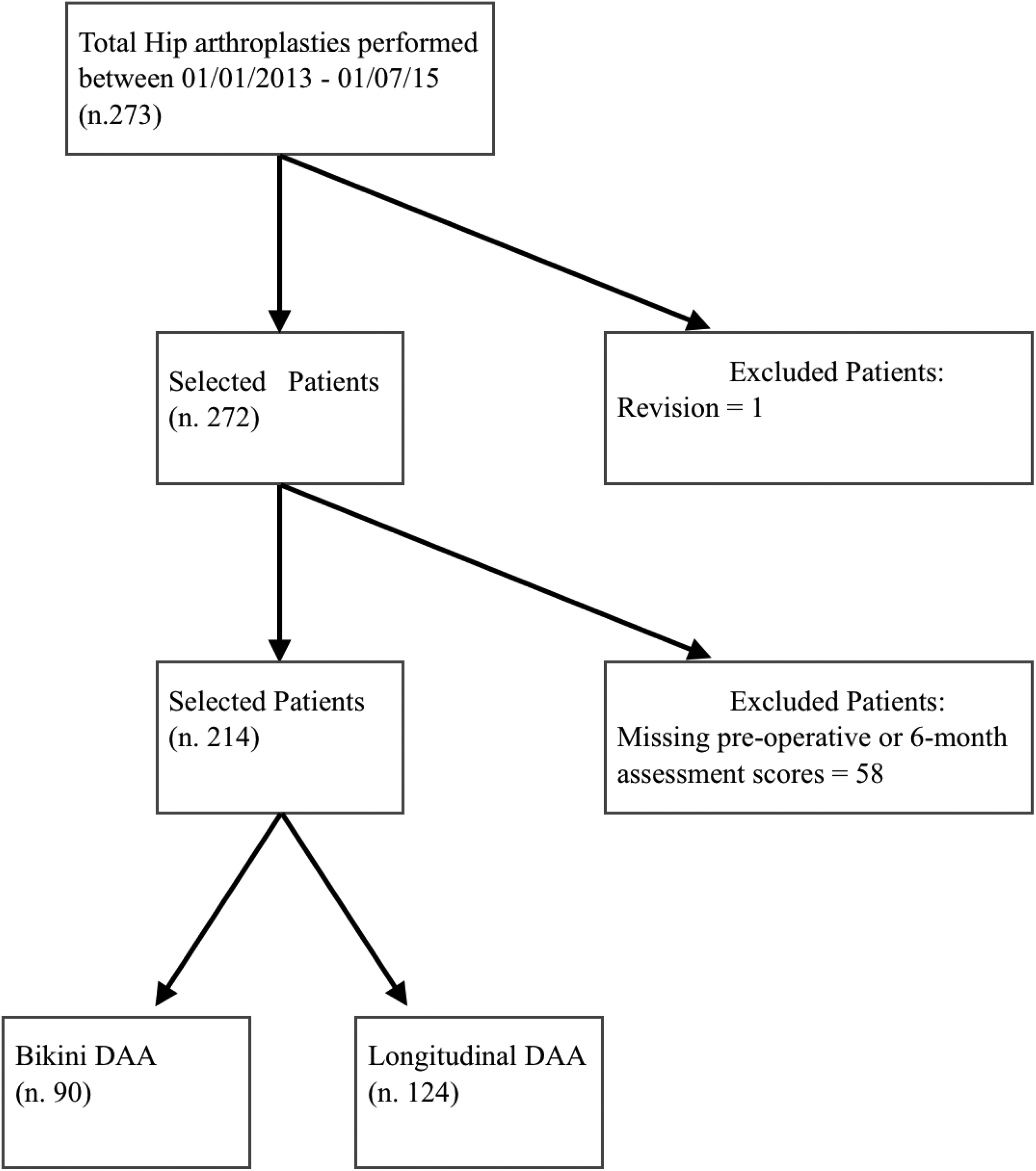
Patient selection.
Demographic features; bikini versus non-bikini incision.a
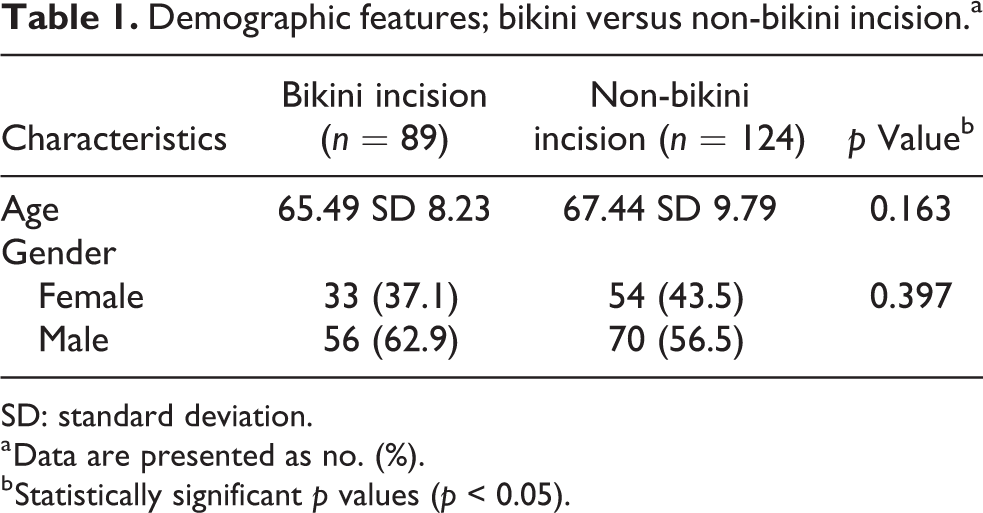
SD: standard deviation.
a Data are presented as no. (%).
b Statistically significant p values (p < 0.05).
Quality of life and functional scores
The preoperative mean Oxford hip scores were in keeping with moderate–severe osteoarthritis in both groups. 11 There were no statistical differences in baseline Oxford hip scores between the two groups, as presented in Table 2. At 6 months of follow-up, we observed significant differences in the Oxford hip scores between the two study groups; however, no statistically significant differences in overall change in the Oxford hip were observed between the two groups (Table 2).
Functional outcome according to the Oxford hip score; bikini versus non-bikini incision.a
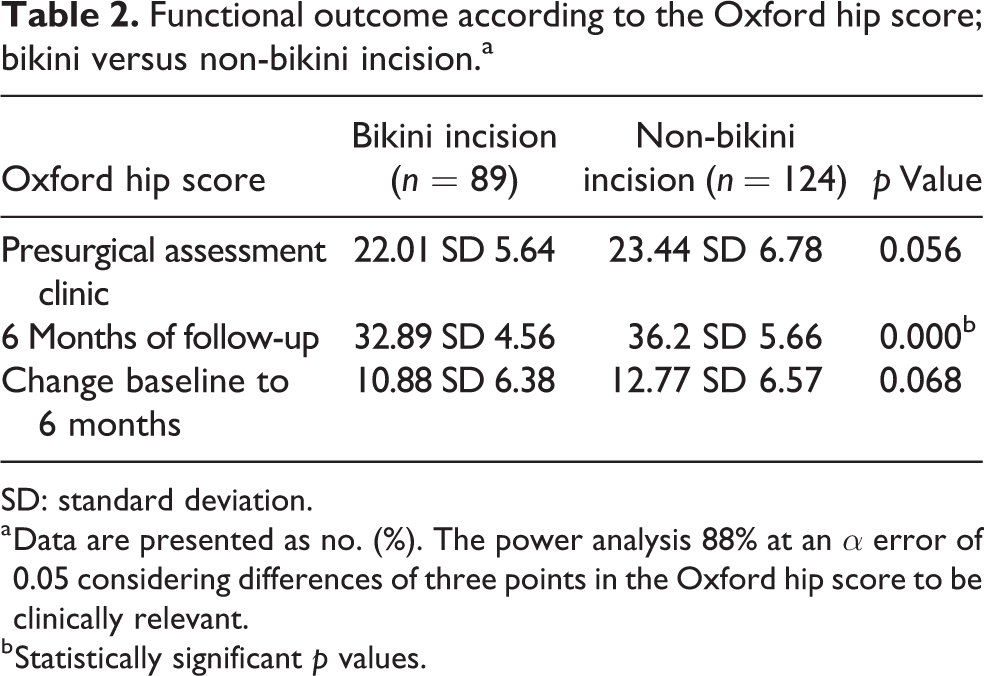
SD: standard deviation.
a Data are presented as no. (%). The power analysis 88% at an α error of 0.05 considering differences of three points in the Oxford hip score to be clinically relevant.
b Statistically significant p values.
The Bikini-incision group’s baseline EuroQol score was significantly lower than the non-bikini group (Table 3). At 6 months post-operatively, the bikini-incision group had a mean EQ-5D score of 0.71 compared with 0.75 for the longitudinal DAA group. The EQ-5D change from baseline to 6 months was statistically larger in the bikini-incision than the longitudinal-incision group (0.49 vs. 0.43).
Functional outcome according to the EuroQol 5D; bikini versus non-bikini incision.a
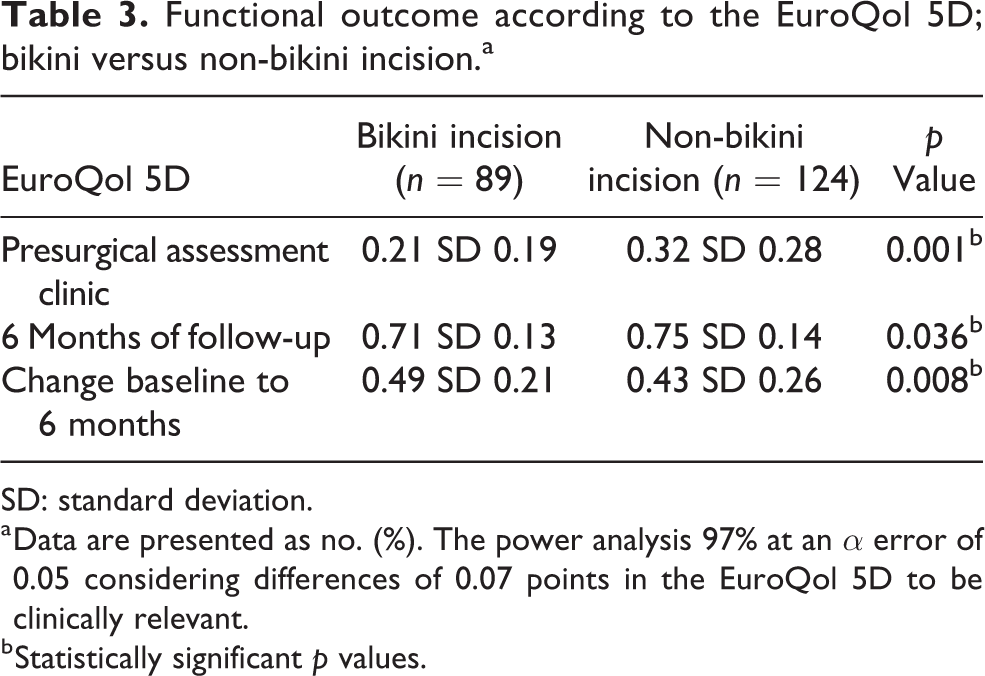
SD: standard deviation.
a Data are presented as no. (%). The power analysis 97% at an α error of 0.05 considering differences of 0.07 points in the EuroQol 5D to be clinically relevant.
b Statistically significant p values.
Complications
Reported complications included one superficial wound infection in each group, which equated to 1.1% in the bikini-incision group versus 0.8% in the non-bikini group. There were no other reported complications.
Discussion
The purpose of this study was to compare the functional and general health outcomes between a ‘bikini’ and a longitudinal incision in DAA THAs. We observed that both groups showed significant improvement in functional score at 6 months. Beard et al. have reported that for the Oxford hip score, there is a minimally important difference of five points 14 and so values under this are considered clinically inconsequential. We found that the two groups had no clinically significant difference in functional outcome in terms of ‘6-month’ or ‘change from baseline to 6-month’ scores. This finding is consistent with initial findings of Leunig et al. that short-term outcomes are comparable between bikini- and longitudinal-incision DAA. 6
Both groups also showed a clinically significant improvement in ‘health-related quality of life’ at 6 months. The ‘bikini’ group had a statistically significant larger increase in EuroQol score than the longitudinal group. Nevertheless, these differences are less than 0.074 and so should be considered clinically inconsequential. 15 Our findings suggest that general health outcomes are comparable at 6 months post-operatively between the two groups. This is the first time that general health outcomes of the ‘bikini-incision’ have been compared with a longitudinal incision and so there is no literature to validate our findings against.
Previous articles have shown that patients have higher satisfaction with the appearance of a bikini-incision scar than the longitudinal-incision scar. 6 Since ‘bikini’-incision outcomes are comparable to longitudinal-incision DAA, we suggest that this variation of the DAA may have a role in patients concerned about scar appearance.
Strengths and weaknesses
Our study has numerous strengths. Firstly, our study groups are the largest reported in the literature comparing bikini-incision with longitudinal-incision DAA outcomes. In addition, our sample size was sufficient to detect significant differences between different approaches with a statistical power >85% and an α error of 0.05. Secondly, the patients included were operated on consecutively and had the same preoperative and post-operative protocols. Thirdly, all the operations were performed by the same surgeon, excluding operative bias. The learning curve for adopting the DAA has been established at between 40 and100 patients, 16 but there is currently no data on the learning curve to adapt from the longitudinal- to the bikini-incision DAA. Since the learning curve was unclear, we opted to include all his initial cases in the analysis. This, however, introduced two problems. Firstly, while initially learning the procedure, the surgeon chose patients with perceived easier anatomy, which introduced a patient selection bias. Secondly, a proportion of the ‘bikini-incision’ group was performed while the surgeon was still perfecting his technique, while all those in the longitudinal-incision group underwent an operation the surgeon was experienced with (>1000 cases). This may consequently have resulted in bikini outcomes reported under their potential value.
Conclusion
The bikini-approach DAA has comparable 6-month functional and general-health outcomes to the longitudinal-approach DAA. Given the advantage in cosmesis, we feel that the bikini-approach DAA has a role in THAs for patients who are conscious of scar appearance.
Footnotes
Authors’ Note
Iskandar Tamimi Marino is now affiliated with Hospital Regional Universitario de Málaga - Departamento de Cirugía Ortopédica y Traumatología, Málaga, Spain.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.