
Abstract
Lipoma is the most common benign soft tissue tumor; however, they are rarely seen in bony tissue. Osseous lipomas are classified as intraosseous (originating within the bone) or juxtacortical (on its surface). Surface lipomas may be further subdivided into parosteal lipoma and subparosteal lipoma, depending on its anatomical relationship to periosteum. Parosteal lipoma is a rare benign fatty neoplasm, accounting for less than 0.3% of all lipomas. They are almost always solitary occurring in the extremities sometimes with periosteal changes. Owing to its rarity, we report a case of parosteal lipoma of proximal radius in a 32-year-old female without periosteal changes and without nerve involvement. It was evaluated clinically and radiologically and a core needle biopsy was done which was suggestive of benign lipomatous lesion. Then en masse excisional biopsy was done and the diagnosis of parosteal lipoma was established after histopathological examination. Pertaining to its anatomical location, surgical dissection is very important to preserve superficial radial nerve, posterior interosseous nerve, and supinator muscle. At final follow-up, patient is doing well with full range of motion, preserved nerve function and elbow function.
Keywords
Introduction
Lipoma is the most common benign soft tissue tumor, containing mature adipose tissue and is generally asymptomatic. Osseous lipomas are extremely rare and are classified as intraosseous (originating within bone) or juxtacortical (on its surface). Surface/juxtacortical lipomas may be further subdivided into parosteal lipoma and subparosteal lipoma, depending on its anatomical relationship to periosteum. 1 Parosteal lipoma is an extremely rare benign fatty neoplasm, accounting for less than 0.3% of all lipomas. 2 They are almost always solitary occurring in the extremities in the middle-aged population and are mostly asymptomatic and thus go undetected. 3 They have been reported to occur most commonly in femur, tibia, humerus, and radius. 4,5 They are closely related to periosteum and sometimes present with periosteal changes. 6 We report a case of parosteal lipoma of proximal radius in a 32-year-old female without periosteal changes and without nerve involvement.
Case report
A 32-year-old female presented to the bone tumor clinic with a painless swelling over the anterolateral aspect of her right proximal forearm for last 1 year. This swelling had gradually increased in size over 1 year, to attain the present size. She had also complained of terminal restriction of pronation. On examination, there was a soft, well-defined (around 4 × 3 × 2 cm3), globular, non-pulsatile, and non-tender mass arising from proximal radius, without any associated skin changes. The mass moved with the radius on alternate pronation-supination. Overlying skin was free and mobile. Elbow movements were free, except terminal restriction of pronation. There was no distal neurovascular deficit. On primary radiological workup, conventional X-ray (Figure 1(a)) of proximal forearm with elbow was done, which revealed a radiolucent soft tissue shadow surrounding the pedunculated radiopaque osseous lesion which was arising from the anterolateral aspect of proximal radius near the bicipital tuberosity. Magnetic resonance imaging (MRI; Figure 1(b)) showed the evidence of 4 × 3 × 3.9 cm3 well-defined fat-containing lesion around the proximal radial shaft and neck attached to it by bony excrescence. Supinator muscle was superficial to the lesion with biceps tendon coursing anterior to it just before its radial attachment. MRI findings were consistent with benign soft tissue neoplasm most probably a parosteal lipoma. Considering the clinic-radiological presentation, a differential diagnosis of a pedunculated osteochondroma with a thick cartilaginous cap (with possible sarcomatous changes) was also kept. Then a core needle biopsy was performed which was suggestive of a benign lipomatous lesion. After the discussion in a multidisciplinary tumor board, an excisional biopsy (a wide local excision) was planned under general anesthesia.
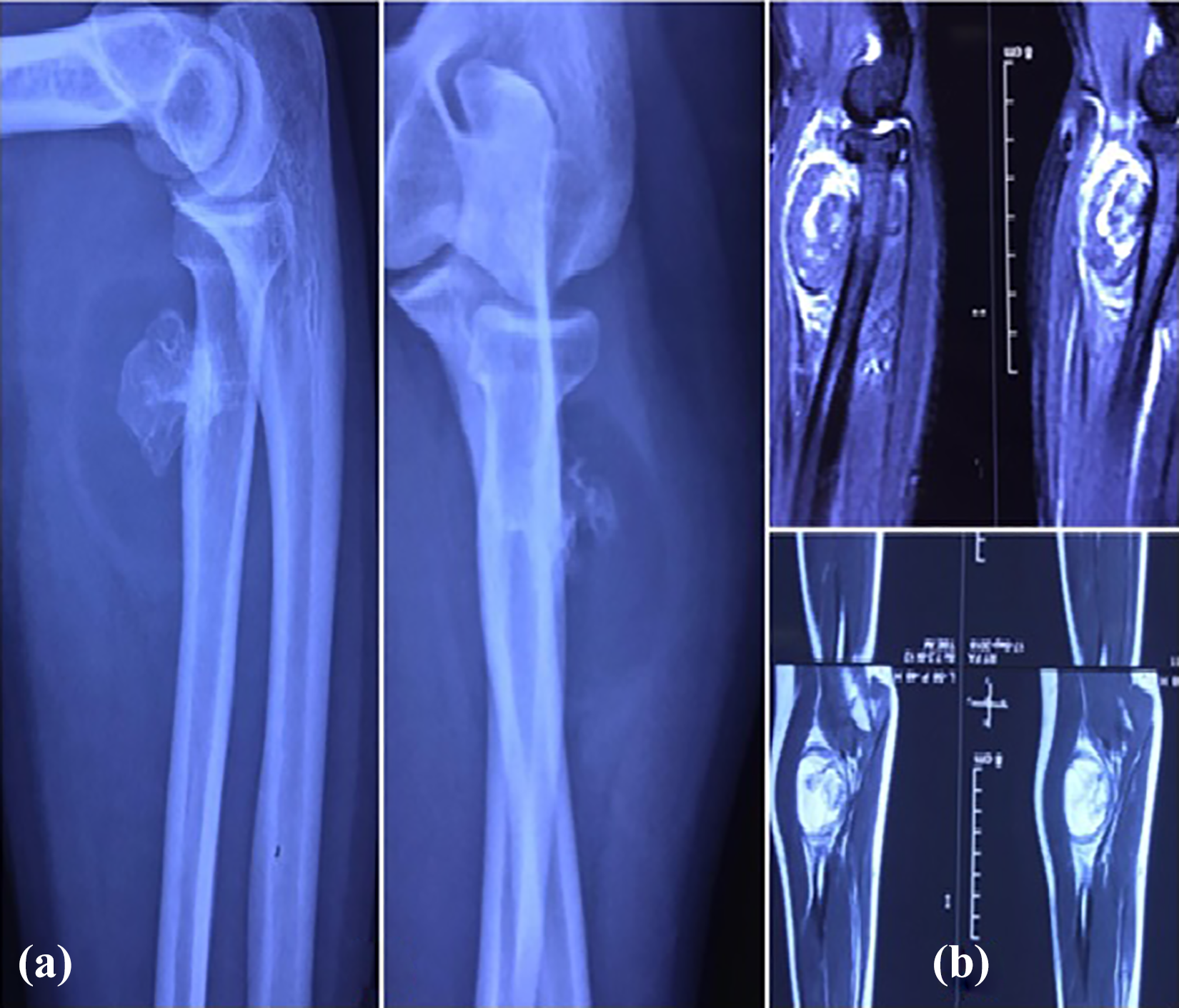
(a) X-ray of elbow showing radiolucent soft tissue mass with radiopaque bony density arising from the anterolateral aspect of proximal radius near the bicipital tuberosity. (b) MRI images showing fat-containing lesion around the proximal radial shaft and neck attached to it by bony excrescence. MRI: magnetic resonance imaging.
Lesion was approached via standard Henry’s approach to proximal forearm. Superficial radial nerve was isolated (Figure 2(a)) and brachioradialis was retracted laterally. The flexor carpi radialis (FCR) and pronator teres were retracted medially. Retraction exposed the supinator muscle covering the globular swelling (Figure 2(b)). Supinator was detached from its attachment at ulna and reflected laterally off the swelling keeping forearm in fully supinated position to preserve the posterior interosseous nerve (PIN). It exposed the globular mass which was found to be attached to the proximal radius near the bicipital tuberosity with bony excrescence and there were no periosteal/cortical changes (Figure 2(c)). Biceps tendon was seen just medial to the lesion inserting on to bicipital tuberosity. En-bloc excision of the lesion with a portion of superficial radial cortex was done (Figure 3(a)) with an osteotome and material was sent for histopathological examination.
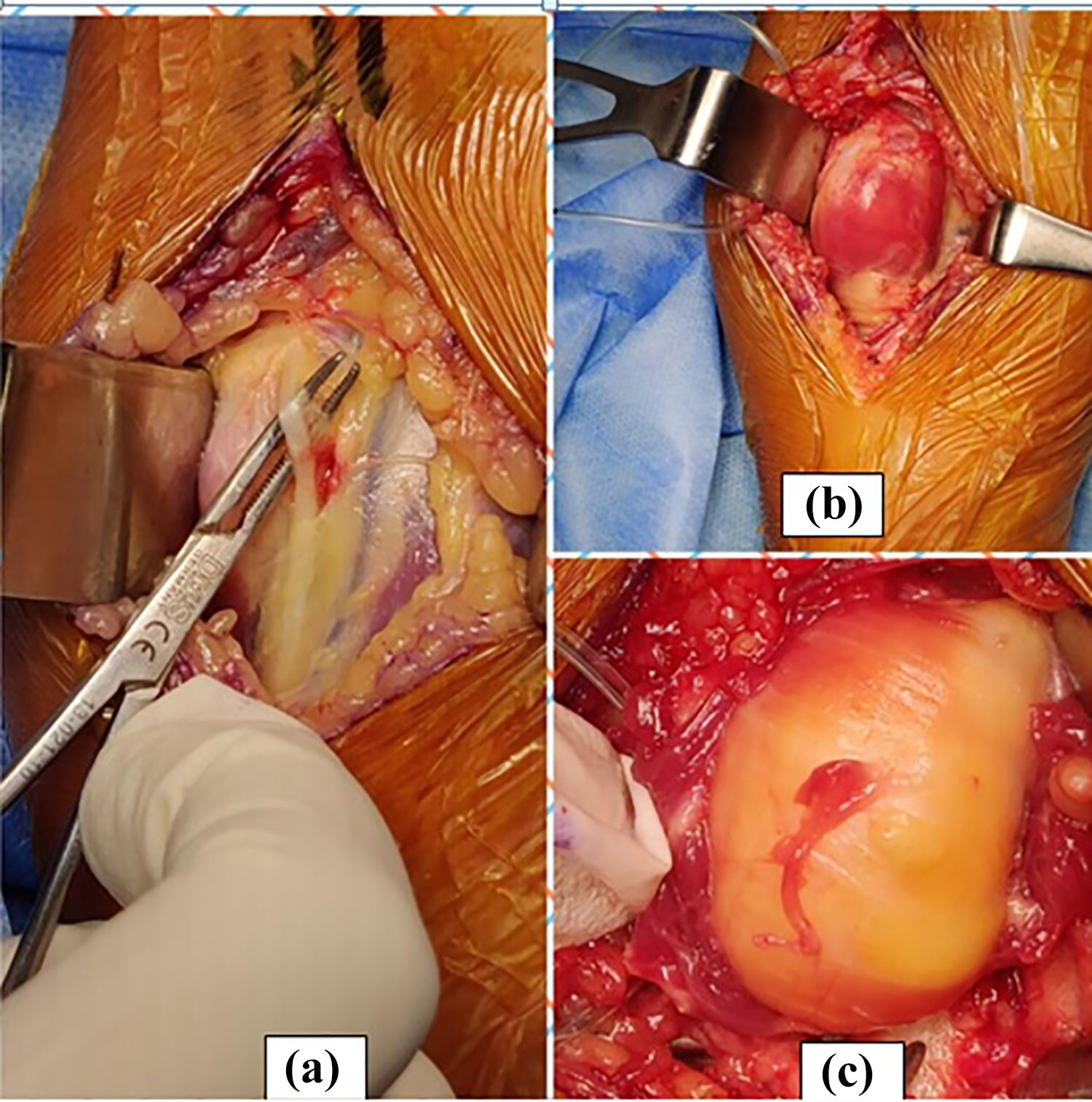
(a) Superficial radial nerve isolated, (b) supinator muscle covering the lipoma, and (c) supinator reflected laterally from its attachment at ulna.
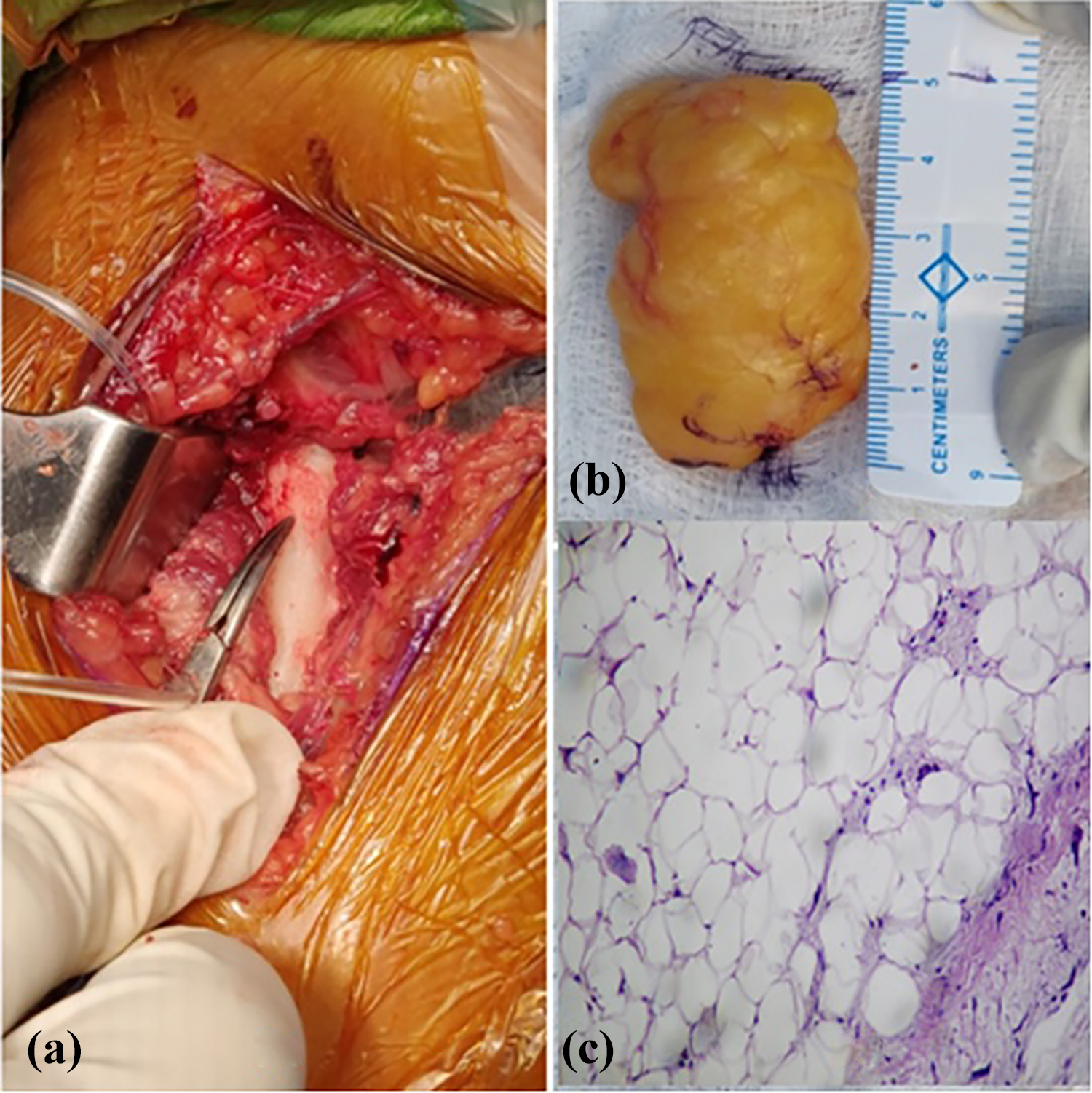
(a) Image showing proximal radius after excising the lesion, (b) excised lipoma with bony base, longitudinally measuring around 4.8 cm, and (c) histopathological slide showing mature adipocytes with fibrous septa.
Grossly the mass measured around 4.8 × 3 × 2 cm3 and it had a bony excrescence at its base (Figure 3(b)). Histologically, the lesion showed benign adipose tissue surrounded by thin fibrous septa consistent with parosteal lipoma (Figure 3(c)). At 1 year postoperatively, the patient is doing well with no evidence of recurrence, full elbow range of motion and strength, and no nerve palsy.
Discussion
Parosteal lipomas are rare, 0.3% of all lipomas 2 and even rarer (0.1%) among all the primary bone tumors. 6 They are benign soft tissue tumor but at times may mimic malignancy like liposarcoma because of its permeation in skeletal muscle 3 and periosteal changes. 7 They might also be seen in other sites like clavicle, ribs, skull, metacarpals, and metatarsals. 3 Unlike other lipomas, parosteal lipomas present late and are relatively difficult to diagnose because of its deep-seated nature. They are usually small lesions and one of the largest parosteal lipoma reported is by Aoki et al. 8 in femur in 2014. These lesions are usually asymptomatic unless complicated by compression over nearby neurovascular structure leading to neuropraxia or vessel engorgement, or restricted motion of adjacent joint. Some reported cases of parosteal lipoma of proximal radius have presented as neuropraxia of PIN and restriction of elbow movement. 1,2
MRI is an investigation choice and is also an important adjunct to plain X-ray, for the diagnostic and preoperative workup of parosteal lipoma, as it can delineate the lesion in multiple planes along with important neurovascular structures around the tumor. 9 Hence, it is very useful in the planning of surgery.
In our case there was no neuropraxia and no periosteal changes. Considering the anatomical location, dissection has to be very careful to avoid injury of superficial radial nerve, PIN, biceps tendon, proximal radius fracture, and supinator muscle integrity. In our case at 1 year follow-up, there was no neuropraxia or nerve injury, no muscle weakness. The patient had fully functional supinator muscle and full elbow range of movements.
Conclusion
These are rare cases and may be misdiagnosed or overdiagnosed at times, so they should be reported to increase awareness among orthopedic surgeons. Parosteal lipoma is a benign lesion with no malignant potential and good prognosis. Also the take-home message will be to always follow the systematic approach in management of such lesions and the involvement of multidisciplinary team is very important.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.