
Abstract
The Thompson’s approach is used as the standard posterior approach by many surgeons. Although posterior interosseous nerve palsy following the Thompson’s approach has been reported by several authors, isolated paralysis of the extensor digitorum communis (EDC) is a rare occurrence. We report to you a case of isolated paralysis of EDC following the Thompson’s approach in a 14-year-old boy who recovered completely on the 5th postoperative day. Each of the approaches to the proximal radius poses a risk of damage to the posterior interosseous nerve and its branches because of traction. Damage may occur during exposure or implant insertion. Any surgery around the supinator and the radial tunnel region is dangerous because of complex anatomy, lack of intermuscular planes and varying distribution of the radial nerve. Avoiding excessive posterior or ulnar retraction of the EDC and improper dissection can avoid the “sign of horns” deformity following the Thompson’s approach.
Introduction
The proximal radius can be approached by various approaches, including the modified Henry’s anterior approach, the Thompson’s posterior approach and the modified Gordon-Boyd’s approach. 1
The Thompson’s approach is used as the standard posterior approach by many surgeons. The plane of dissection is an internervous plane between the extensor carpi radialis brevis (ECRB) and the extensor digitorum communis (EDC). 2 Thompson suggested the posterior approach on account of the high muscle bulk and more depth in the anterior forearm. 2 However, complications such as posterior interosseous nerve (PIN) palsy 3 and anterior interosseous nerve lesions 4 have been reported with this approach.
The “Sign of Horns” in the hand implies extension of the index and middle fingers with simultaneous flexion of the middle and ring fingers. 5 It results from an isolated loss of function of the EDC with normal function of the extensor indicis proprius and the extensor digiti quinti.
Although PIN palsy following the Thompson’s approach have been reported by several authors, isolated paralysis of the EDC is a rare occurrence.
We report to you a case of isolated paralysis of the EDC following the Thompson’s approach in a 14-year-old boy.
Case Report
A 14-year-old right-hand dominant boy presented to us with pain and swelling of the right forearm after a road traffic accident. It was a closed injury with no distal neurovascular deficit. Radiographs showed a displaced fracture of the proximal one-third of the right radius (Figure 1). He was operated the following day with open reduction and internal fixation of a 7-hole dynamic compression plate (DCP) and six screws (Figure 2). One 2-mm Kirschner wire was inserted to stabilise the distal radioulnar joint. We used the Thompson’s posterior approach to reach the fracture site. The supinator was subperiosteally elevated from its ulnar aspect without dissecting the PIN (Figure 3). The wound was closed over a drain.

Pre-operative radiograph.
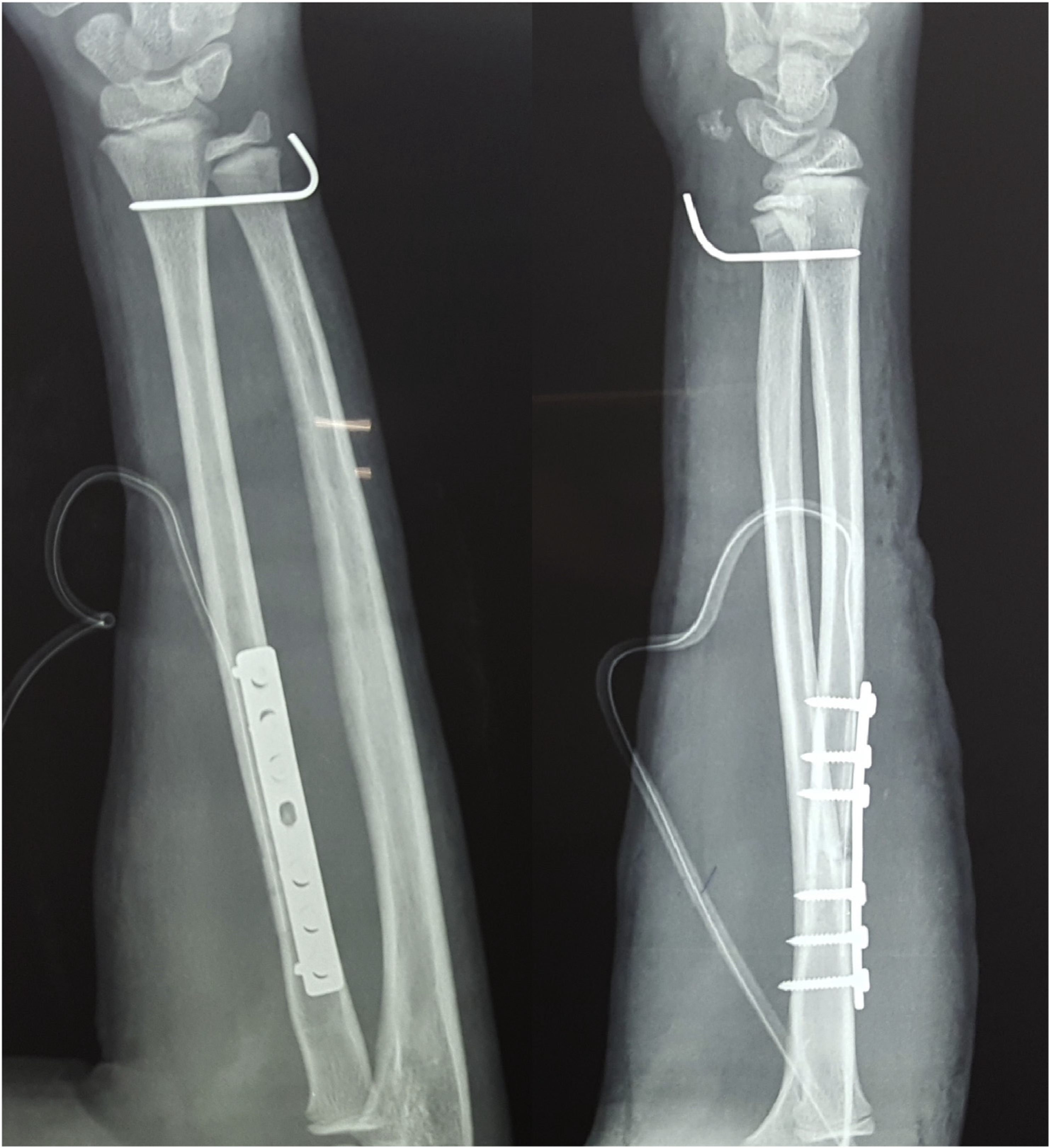
Post-operative radiograph.
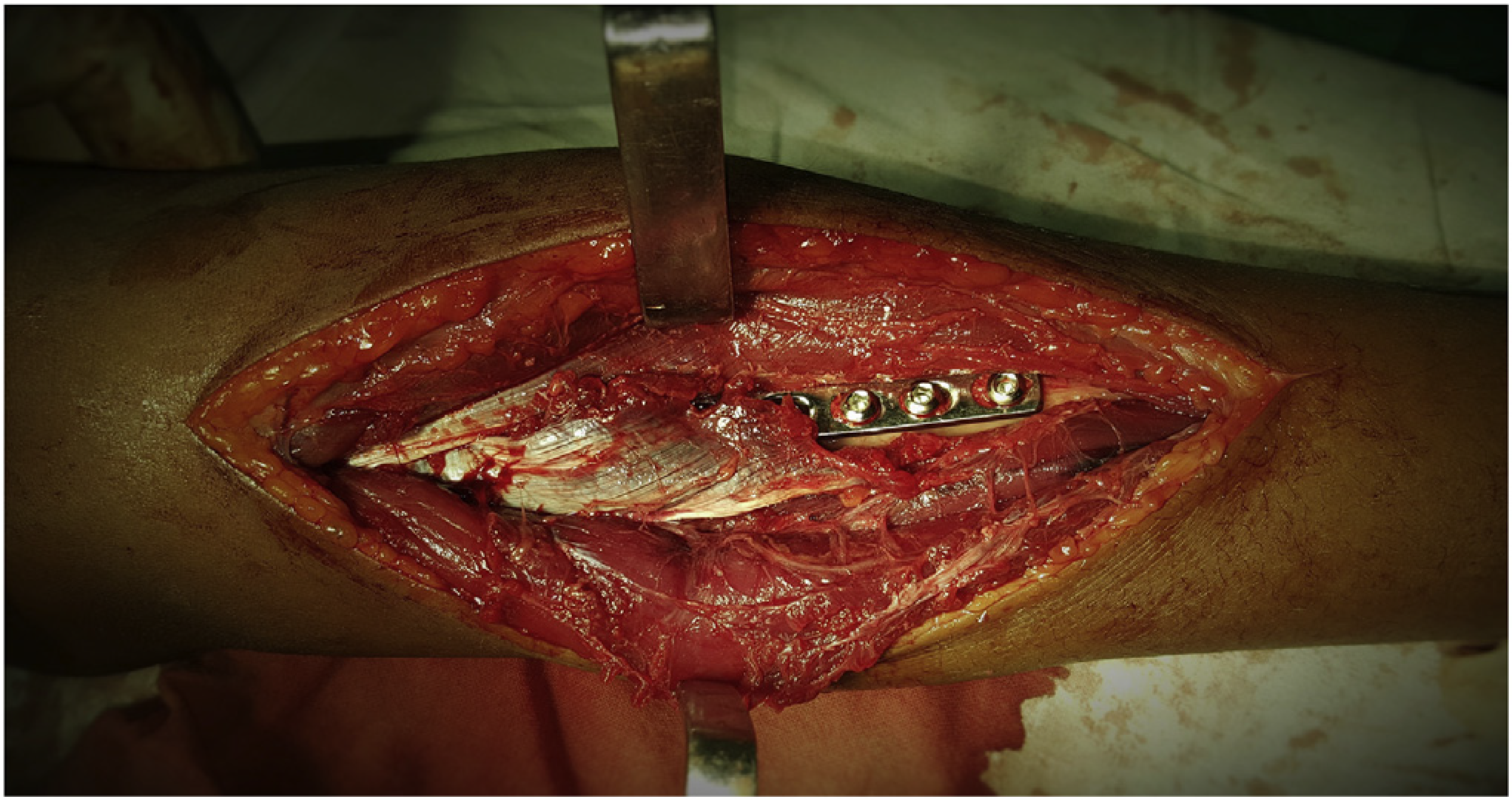
Intra-operative picture of the approach.
The patient was examined after the effect of anaesthesia wore off. He was unable to actively extend the middle and ring fingers (Figure 4). However, he was able to actively extend the index and little fingers along with the thumb demonstrating grade 5 power. Motor function of the finger flexors, wrist flexors and extensors was normal. The hand and the forearm had normal sensibility. On the 3rd postoperative day, he showed partial recovery with grade 3 power on extension of the middle and ring fingers. The patient achieved full clinical recovery on the 5th postoperative day with no residual motor deficit.

Isolated paralysis of the EDC (“Sign of Horns”deformity).
Discussion
Each of the approaches to the proximal radius poses a risk of damage to the PIN and its branches because of traction. Damage may occur during exposure or implant insertion. 6 Anatomy of this region may be altered due to fractures, tumours or inflammation. 1 Any surgery around the supinator and the radial tunnel region is dangerous because of the complex anatomy, lack of intermuscular planes and varying distribution of the radial nerve. 7
The radial nerve divides into the PIN and superficial radial nerve 8.0 ± 9 cm distal to the lateral intermuscular septum and 3.6 ±0.7cm proximal to the leading edge of the supinator. 7 After the division, the PIN travels beneath the origin of the ECRB and into the supinator muscle. 7 It now innervates the various muscles of the dorsal compartment. 7
Abrams et al stated that the order of innervation of the various muscles supplied by the PIN is variable. 8 The innervation of ECRL, supinator and ECRB in this order is the only constant order observed by them. They also observed that the EDC was innervated always before the extensor indicis proprius and EPL and almost always before the extensor digiti quinti.
Spinner et al 9 observed that despite the aforementioned variability in innervation, the individual muscular components are innervated in a reproducible and useful pattern. They noted that the middle and ring fingers were supplied by the recurrent branches which innervated the proximal EDC. The proximal EDC is an area mostly consisting of muscle fibres of the middle and ring fingers.
With context to the number of branches, the EDC is supplied by the maximum number of branches from the PIN. 8 Abrams et al suggested that the higher branch number was due to the multiple independently functioning tendon units in the EDC and the fact that it crosses two joints to exercise its function.
The “Sign of Horns” presentation was first described by Furnas and Spinner in 1978. 5 Spinner et al reported seven patients suffering an isolated paralysis of the EDC following the Thompson’s approach to the proximal radius. 9 All their patients developed the “Sign of Horns” deformity immediately after surgery with no sensory involvement. One of them showed full clinical recovery by 4 weeks after surgery, but the rest had a permanent deficit. They reported denervation atrophy of the midportion of the EDC in three patients who underwent tendon transfers. They performed electrophysiologic studies in healthy patients and successfully demonstrated that the middle and ring fingers could be activated together without activation of the index or the little fingers.
Thus, the isolated paralysis of the EDC can be explained by injury to the specific recurrent branches of the PIN distal to the supinator. 9 Any injury proximal to or at the level of the supinator would produce a more complex or a complete PIN lesion. 9
Mekhail et al 1 suggested two techniques to avoid PIN injury in the Thompson’s approach. One can supinate the forearm fully and incise the supinator insertion from below upwards gradually retracting it subperiosteally. Alternatively, one may identify the PIN distally and follow it upwards by incising the superficial layer of the supinator muscle. But, in both the aforementioned methods, the recurrent branches to the PIN may still be vulnerable because of excessive retraction of the EDC itself.
In our case, the motor recovery began early on the 3rd postoperative day. Damage to the EDC nerve supply would have taken a longer time to recover. Rather, a direct trauma to the EDC due to excessive retraction and handling, leading to atonia, seems to be the most probable cause of the deformity. Nerve conduction studies were not performed as the patient had shown early signs of recovery.
Thus, in the Thompson’s approach, it is important to pay attention not only to the dissection of the supinator but also to the retraction of the EDC which may produce a partial lesion of the EDC. In addition, in traumatic cases, the altered anatomy would further complicate the approach around the supinator and EDC, making it difficult to visualise the PIN or its distal common leash and branches. Avoiding excessive posterior or ulnar retraction of the EDC and improper dissection can avoid the “Sign of Horns” deformity following the Thompson’s approach. 9
Footnotes
Conflicts of interest
The authors have no conflicts of interest relevant to this article.
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors, and no material support of any kind was received.