
Abstract
Introduction:
Minimal invasive Achilles tendon repair is becoming more and more popular recently. We have evaluated our results in Achilles tendon repair using minimally invasive method by a suture-guiding device.
Methods:
This is a retrospective review of patients with acute Achilles tendon rupture, which was repaired using minimally invasive method namely the suture-guiding device, that was performed during 2003 to 2015 in our department. Outcome parameters were the incidence of re-rupture, other complications, and the functional outcome.
Results:
There were 36 men (90%) and 4 women (10%) in this study. Mechanisms of injury were basketball (28%), football (15%), squash (15%), and trauma (13%). The mean operating time was 59 min (range 30–90 min). The mean follow-up time was 8 months (range 3–35 months). The mean duration with casting was 7 weeks. The mean range of movement at 3 months was 8° dorsiflexion and 33° plantar flexion. There was no major complication necessitating surgical re-interventions such as re-ruptures and infections. No patient suffered from dysfunction of the sural nerve or delay wound healing.
Conclusion:
Minimally invasive Achilles tendon repair using suture-guiding device is a safe and quick procedure with a low rate of re-rupture and a satisfactory short-term and long-term recovery.
Introduction
Acute Achilles tendon rupture is often a sports injury that orthopedic surgeons encounter. It is most common in active adults, with a male predominance. Common mechanisms of injury are pushing off weight-bearing foot while knee is extended (e.g. when a sprinter starts a race), a sudden and unexpected dorsiflexion of the ankle (e.g. falling into a hole), and hyper dorsiflexion of ankle (e.g. landing a jump, falling from height). 1
The most common site for Achilles tendon rupture is around 3 to 4 cm proximal to the calcaneal insertion. It is known as the water-shed area, which is an avascular zone of the tendon. 2 The lack of blood supply predisposes the tendon from rupturing at this site.
Up till today, the best treatment for acute Achilles tendon rupture remains a controversy. Some surgeons prefer a nonoperative management, while some prefer a surgical repair. 3 For surgical repair, the traditional repair method for acute Achilles tendon rupture was an open method. 4 However, the open method is associated with high rate of wound complications. 5 Therefore, conventional open repair method had gradually been replaced with minimally invasive methods, for example, percutaneous, mini-open. 4 These methods had been proven to give good results; however, long-term results were generally lacking in the current literature. Caritas Medical Centre had been using the suture-guiding device for acute rupture of Achilles tendon since 2002. 6 In between 2002 and 2015, we had used mini-open method with suture-guiding devices to repair acute Achilles tendon rupture for 40 patients, and their short- and long-term results were evaluated.
Method
This study is a retrospective review. Inclusion criteria were all patients who attended the Orthopaedics Department of Caritas Medical Centre from 2002 and 2015, (1) who had (1) acute Achilles tendon rupture, and (2) who underwent Achilles tendon repair with suture-guiding device. Patients who suffered from chronic Achilles tendon rupture, rupture not at mid substance, open wound with cut tendon, or had other methods of repair (conservative, open, percutaneous) were excluded from this study.
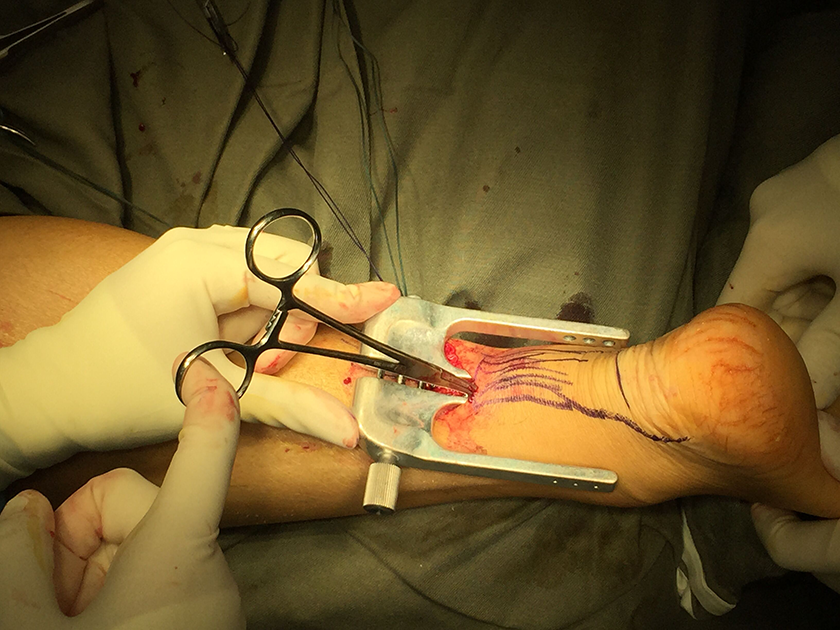
This technique involved a U-shaped device with four limbs for tendon approximation. This device was made by a local company using stainless steel in 2001, and we had been using it regularly since 2002. Its design was similar to the now commercially available device such as Achillon, however back in 2002, no similar product was available in Hong Kong. Our suture targeting device is autoclavable and reusable. Cardiac needle or angiocatheter can be used as needle driver to introduce the suture in. The inner two limbs are placed within the paratenon enclosing the ruptured tendon ends, while the outer limbs are placed outside the skin (Figures 1 –9).

Patient is put in prone position, then palpate along the Achilles tendon and feel for the gap which corresponds to the rupture site. The site is marked with marking pen.

A small vertical incision is made medial to the tendon, around 1.5 to 2 cm in length over the rupture site. Retract the skin and make a 2 cm vertical incision over the paratenon.

Then place a stay suture on the edge of each side of the paratenon and carefully dissect proximally and distally to clearly visualize the “tunnel shape” of the paratenon. The tendon can be mobilized with small sponge forceps or dental swabs in case there is some retraction. Carefully introduce the suture-guiding device under the paratenon proximally. Make sure the tendon falls between the two central branches of the instrument. This ensures a good grasp of the tendon for suturing.
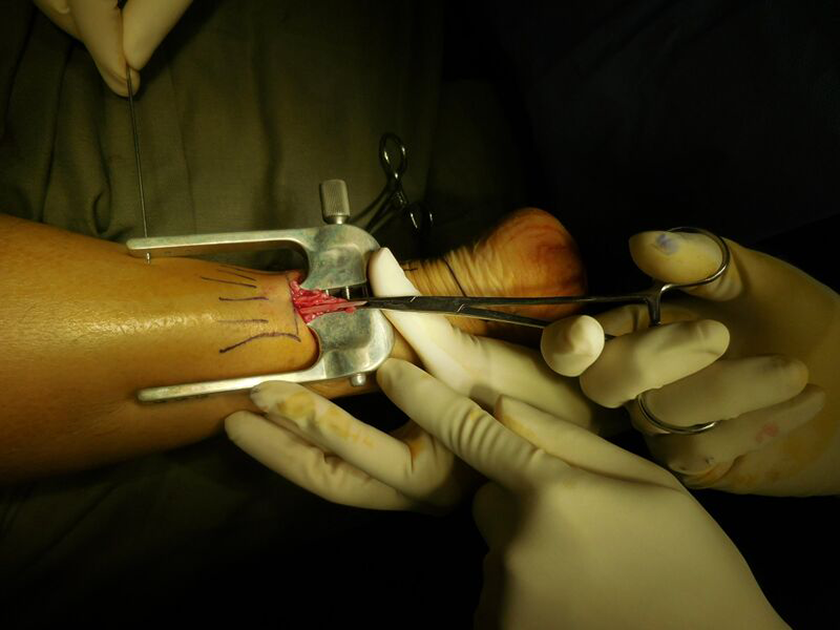
Then, using a needle driver, introduce three needles with Ethibond 5 sutures through the holes of the four limbs of the suture-guiding device. Make sure the tendon is still secure between the inner limbs.

Retrieve the sutures to the central limb of the device.

Gently remove the suture-guiding device and place a clamp on each suture on their respective side.
Correctly organize and pair the sutures and tie them to the corresponding pair (i.e. most proximal pair of sutures in the proximal stump tie with the most distal pair of sutures of the distal stump; the middle pair of each stump tie together; the most distal pair of sutures of the proximal stump tie with the most proximal pair of sutures of the distal stump).

Closure of paratenon and skin.

Post operative photo.
Surgical procedure is as follows: Patient is put in prone position, then palpate along the Achilles tendon and feel for the gap which corresponds to the rupture site. The site is marked with marking pen. A small vertical incision is made medial to the tendon, around 1.5 to 2 cm in length over the rupture site. Retract the skin and make a 2 cm vertical incision over the paratenon. Then place a stay suture on the edge of each side of the paratenon and carefully dissect proximally and distally to clearly visualize the “tunnel shape” of the paratenon. The tendon can be mobilized with small sponge forceps or dental swabs in case there is some retraction. Carefully introduce the suture-guiding device under the paratenon proximally. Make sure the tendon falls between the two central branches of the instrument. This ensures a good grasp of the tendon for suturing. Then, using a needle driver, introduce three needles with Ethibond 5 sutures through the holes of the four limbs of the suture-guiding device. Make sure the tendon is still secure between the inner limbs. Gently remove the suture-guiding device and place a clamp on each suture on their respective side. Repeat the same sequence to the distal stump. There is a choice of using six sutures with six knots or three sutures with three knots. Details will be further discussed in “Author’s suggestions with this device” section. Correctly organize and pair the sutures and tie them to the corresponding pair (i.e. most proximal pair of sutures in the proximal stump tie with the most distal pair of sutures of the distal stump; the middle pair of each stump tie together; the most distal pair of sutures of the proximal stump tie with the most proximal pair of sutures of the distal stump). Closure of paratenon and skin.
All of the patients were put under the same rehab protocol. Short leg plaster cast was kept in the 30° equinus position for 3 weeks. At week 3, the cast was changed to a hinged ankle brace and gradually allowed an increase in ankle dorsiflexion up to neutral at 6 weeks after operation. Weight-bearing was avoided for the initial 6 weeks after operation, and partial weight-bearing commenced at week 6 for 3 weeks. At 9 weeks, active strengthening and stretching could be started under physiotherapists’ supervision. Gentle sports could be resumed at 3 months and contact sports at 6 months after operation. This regime had been in use since 2004 and is now changing. Our new rehab regime will be shown in the discussion part.
We had retrospectively reviewed hospital records, gathered the basic epidemiology of the patients, including gender and age, as well as injury-oriented details (e.g. mechanism of injury). The outcome parameters included major complications (re-rupture, major wound infection, dysfunction of sural nerve, delay wound healing), as well as the range of movement at 3 months after the index operation.
Furthermore, a telephone interview was contacted in late 2015 to assess the long-term outcome of patients, which included any re-rupture, and their functional outcome including whether the patient could resume previous job, resume previous sports, any residual pain, and any residual stiffness.
Results
A total of 40 patients were recruited. Thirty-six were men (90%) and 4 were women (10%). The mean age of injury was 42.56 years, and the median age of injury was 40 years (range 26–65, SD 11). All 40 patients had acute injuries, which was defined as injury within 4 weeks. Regarding the mechanisms of injury, most were sports-related injury, with basketball being the most dominant cause, making up to 27% of the injuries. Other sports included football (15%), squash (15%), badminton (7%), volleyball (3%), tennis (2%), and other sports (5%). There were also 13% of non-sports related trauma injuries.
All 40 patients underwent Achilles tendon repair using suture-guiding devices. The mean surgery time was 59 min (range 30–90 min, SD 14), while the mean post-operative length of stay was 1.5 days (range 1–10, SD 2).
The mean follow-up time was 8 months (range 3–35 months, SD 6). The mean range of movement at 3 months was 8° dorsiflexion (range 5–20, SD 7) and 33° plantar flexion (range 25–60, SD 12). The mean range of movement at 6 months was 20° dorsiflexion (range 15–30, SD 6) and 40° plantar flexion (range 30–60, SD 5).
There were no major complications necessitating surgical reinterventions such as re-ruptures and infections. There were no patients that suffered from dysfunction of the sural nerve. There were no patients that suffered from delay wound healing.
Telephone interviews were performed in late 2015 to assess patient’s functional outcome. We tried to contact all 40 patients to perform a telephone interview. We were able to perform the interview for 30 of the patients. We asked whether the patient could resume previous job, resume previous sports, any residual pain, and any residual stiffness. Only one person could not resume previous job (2.5%), he was a construction site worker, and mainly complained of mild residual pain over the surgical wound, and opted for a more sedentary job after the injury. Twenty-three (58%) could resume back to previous level sports, while 5 (12.5%) reported to have changed to an easier sport. Only two (0.05%) reported to be unable to resume any kind of sports. None of the patients reported a re-rupture of Achilles tendon.
Discussion
The gold standard for managing acute Achilles tendon rupture is still a controversy. There are two main believes: operative and nonoperative methods. For nonoperative treatment, it is vital to immobilize the ankle joint to facilitate the healing of tendon. Patient will be put into a cast with a period of non-weight-bearing. There is different rehabilitation protocol with nonoperative treatment of Achilles tendon, some advocate for a longer period of immobilization, while some prefer early mobilization. So far no gold standard is established yet. 7
The re-rupture rate between operative and nonoperative treatment is actually comparable. Soroceanu et al. had performed a study and determined that there was no significant difference in the re-rupture rate between operative and nonoperative treatment. 8 However, nonoperative treatment still reported a lower functional outcome when compared with operative treatment. The extended period of immobilization caused wasting of calf muscles, and hence was associated with significant loss of strength, especially with plantar flexion of the ankle. 9 Only 37% with nonoperative treatment could return to same level of sports, 7,10,11 while 58% of patients in our study could return to same level of sports. This could also be explained by better approximation of tendon end in operative treatment, which allowed better healing of tendon.
For operative treatment, traditionally it was performed with an open repair. A longitudinal incision was made to the medial aspect of tendon to avoid injury to sural nerve. Different suturing methods can be used, including modified Bunnell, Kessler, Krackow, and triple-bundle technique. Jaakkola et al. did a biomechanical study comparing triple-bundle technique and Krakow technique in repair of Achilles tendon. They concluded that triple-bundle technique provides the strongest suture repair. 12 However open repair was associated with high wound complication rate. Lim et al. quoted that open repair was associated with 21% chance of wound infections and 6% of re-rupture. 13 Therefore, less-invasive surgical techniques had been developed, namely mini-open and percutaneous techniques.
Percutaneous repair is defined as a repair method without directly exposing the rupture site. Studies had proved that there was no difference in re-rupture rate and no difference in functional outcome when compared with open technique. 14 However, such technique requires medial and lateral stab incisions posteriorly, which could potentially damage the sural nerve. Hence, there was a higher chance of sural nerve injury using percutaneous technique. 15 Mini-open repair using suture-guiding device is another popular alternative minimally invasive surgery in repair of acute Achilles tendon rupture. It can allow direct visualization to confirm the approximation of tendon. It is also associated with lower sural nerve complication as no stab wound is needed over the lateral side of tendon, and all the instruments and sutures were placed inside the paratenon, away from sural nerve. As seen in our study, it gave a good outcome with minimal complications. There were no cases of re-rupture and no cases of wound complication. There were no cases of sural nerve injury.
There were also numerous studies that showed a low wound complication rate using suture-guiding device. 16 It allowed a faster wound healing, therefore allowed a more aggressive rehabilitation program, which could potentially enhance the range of movement of ankle and decrease the chance of calf muscle wasting. Mini-open repair using suture-guiding device can also provide a stronger repair. Huffard et al. performed an anatomic in vitro biomechanical study comparing Achillon system versus Krackow suture. It showed that the mean load to failure in Krackow suture group being 276 N and Achillon suture being 342 N. 17 Also, it was speculated that a smaller wound incision have less disruption of blood supply to the tendon, hence enhancing the speed of tendon healing. 18
The most common site for acute Achilles tendon rupture is around 3 to 4 cm proximal to the calcaneal insertion, as it is the watershed area. This area could easily be tackled by suture-guiding device, as the stump proximal to calcaneal insertion is long enough to be held by the device.
Furthermore, from the results of our study, not only does repair using suture-guiding device yields good short-term results, the long-term results were also good. Fifty-eight percent can return to sports at the same level, and only 0.05% cannot resume any level of sports. The two patients who could not return to sports were 60 and 65 years old, respectively, who were two of the oldest patients in our patient group. Hence, their demands to return to sport maybe lower than the younger patients.
Authors’ suggestion with this device
We had used this suture-guiding device for 13 years. Based on the good surgical results, we had modified our techniques to further strengthen the repair and reduce the complications. We used Ethibond 5 suture instead of an absorbable suture to increase the short-term and long-term strength of the repair. Yuhan Ji et al. had performed a study comparing Ethibond and PDS II for repairing acute closed Achilles tendon rupture. They concluded that minimal differences were observed in the incision infection, re-rupture rate, and Achilles tendon adhesion. However, based on the AOFAS score and pain score, the Ethibond suture performed better. 19
For six-strand repair, we used total three sutures with three knots (i.e. the most proximal suture will pass through both the most proximal and the most distal hole as well to create only one knot in a pair) instead of six sutures with six knots (i.e. each suture will pass through one hole only, and two knots is needed to connect the pair), and the knots were carefully buried inside the repair site. No evidence was published regarding this method, but as a personal opinion, we found that it can minimize the tension at wound area.
For rehabilitation, the regime included in our study was undergoing modification currently. The regime we used required immobilization for 6 weeks, and some patients developed calf wasting. Current literature supports a more aggressive rehab regime to speed up rehabilitation progress. 20 We have sped up the rehab regime from July 2015 onward, which was excluded in our study period. Some of the young fit patients are currently under a fast track rehabilitation, that is, early functional bracing at 2 weeks post-op with ankle in slight plantar flexion and start partial weight-bearing. They will continue a brace in neutral position with full weight-bearing walking at 4 weeks. The early results were promising. Future studies will target for this early rehabilitation regime.
Limitations
We had only included patients using suture-guiding device. A larger scale study is required to compare the difference between nonoperative, open repair and percutaneous repair.
Conclusion
As we can see from the study, the complication rate of minimally invasive Achilles tendon repair using suture-guiding device is very low. The wound complication rate is lower than that of open, and the rate of sural nerve damage is lower than that of percutaneous repair. There is a low rate of re-rupture with a satisfactory recovery. The long-term results are also excellent. Thus, it is reasonable to say this is a safe procedure. We would like to advocate the use of suture-guiding device in future acute Achilles tendon rupture patients.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.