
Abstract
Purpose:
To date, the best treatment of acute Achilles tendon rupture (AATR) is still inconclusive. Achillon seems to be a promising approach with satisfactory function and low complication rate. We hypothesize a modified minimally invasive repair (MMIR), which provides direct visualization of proximal tendon stump without specialized equipment that could provide comparable results. This trial is aimed to evaluate the functional and surgical outcomes of MMIR comparing with Achillon.
Methods:
From February 2013 to February 2017, 114 patients with AATR were enrolled in this trial, underwent an alternative operation (Achillon or MMIR), and accelerated rehabilitation protocol. Forty-four patients took the Achillon and the other 70 patients took the MMIR at their subjective choice. One hundred eleven full follow-up data were obtained including Achilles tendon total rupture score (ATRS), time back to work, rerupture rate, overall complication rate, and operation time.
Results:
There was no significant difference between groups in demographic characters. There was no statistical difference between both groups regarding to time return to work and ATRS at 3rd, 6th, 12th, and 24th month, respectively. Five reruptures and two Achilles tendons tethering to skins were found in the Achillon group, and two reruptures and one sural nerve injury in the MMIR group. No wound infection and dehiscence occurred. Overall complication rate in the Achillon group is higher (16.3% vs. 4.4%, p = 0.044). The operation time of Achillon is less than MMIR (34.84 vs. 39.71, p < 0.001).
Conclusion:
Both techniques combining with accelerated rehabilitation showed to be reliable and effective. MMIR is safer and more economical, and Achillon is faster.
Introduction
Acute Achilles tendon ruptures (AATRs) usually occur in 30- to 50-year-old males who participate intermittently in sporting activities without the benefit of routine conditioning, the so-called “weekend warriors.”
Both operative and nonoperative treatments have been recommended. Operative treatment increases the risk of wound complications since the thin soft tissue envelope surrounding the repair has a poor blood circulation, increasing the risk of superficial wound dehiscence, infections, and skin necrosis. 1 Proponents of operative treatment emphasize lower rerupture rates, superior functional outcomes, shorter time to off work, and shorter time to return to sports. 2 A recent meta-analysis of eight randomized controlled trials involving 762 patients comparing operative versus nonoperative treatment found that the pooled results showed a significantly lower rerupture rate with surgical treatment (3.7% vs. 9.8%, p = 0.001). 3
Percutaneous surgery represents fewer wound complications, higher rate regarding sural nerve injury, and no significant difference in rerupture rate than open operative treatment. 4 It is more likely to cause sural nerve violation if the suturing process is blind, especially when suturing the proximal stump. 5 However, a meta-analysis shows that Achillon has advantages in reducing the risk of sural nerve injury. 6 But the Achillon device will also bring financial burden at the same time. We agree that the length of Achilles tendon can be properly restored under direct visualization, which leads to a more rapid recovery, more strength of calf muscles, and more strength of tendon reconstruction. 7 And modified minimally invasive repair (MMIR) can provide direct visualization. Currently, there is still a lack of consensus on which surgical method is more effective: minimally invasive or percutaneous. The Achilles tendon total rupture score (ATRS) is a patient-reported outcome measures for specific assessment of an Achilles tendon rupture with high validity, reliability, and sensitivity. 8 We hypothesize that MMIR is not inferior to Achillon. The aim of this study was to investigate MMIR conferred any benefits over Achillon on functional outcome, including ATRS and time return to work, and surgical outcome, including rerupture rate, overall complication rate, and operation time.
Patients and methods
This trial was approved by the research ethics committee of our hospital. The inclusion criteria are AATR, presentation within 1 week after injury, and between 18 and 70 years old. The exclusion criteria are open injury, with ruptures at the musculotendinous junction and bony Achilles tendon avulsions, neurological or vascular disease, and metabolic disorders. A total of 148 patients were diagnosed with Achilles tendon rupture by positive Thompson squeeze test and magnetic resonance imaging and received treatment in Orthopedic Hospital of Henan Province from February 2013 to February 2017 (Figure 1). All patients were informed of the current literature regarding the treatment of Achilles tendon injuries. Thirty-four patients were excluded from the study for the reasons given in Table 1. The remaining 114 patients in the trial received an alternative surgery (Achillon or MMIR). The choice between the two approaches was subjectively decided by patients themselves. Forty-four patients took the Achillon and the other 70 patients took the MMIR.

Flow diagram for the study.
Reasons for exclusion in 34 patients.

Surgical technique
All surgeries were performed by the same one experienced specialized foot and ankle surgeon. After the induction of general anesthesia, the patient is placed in a prone position on the operating table.
In the Achillon group, a standard Achillon technique is performed. 9 A 2-cm transverse incision is made at the interval gap between the distal end and the proximal end and extended to the paratenon of Achilles. The Achillon device (General care, Shanghai, China) is inserted within the paratenon along the proximal end. Three sutures are introduced percutaneously through the proximal section. Once sutures are passed, the device is pulled out. This pulls the sutures out of the incision alongside Achilles tendon. The same procedure is performed to the distal stump. All sutures are tightened at the correct length, and subcutaneous tissues and skins are sutured layer-by-layer.
In the MMIR group, the same incision is made. The paratenon sheath is transversely incised and the proximal stump of the tendon is identified and clamped with an Allis-type clamp. The knee joint is flexed and the tendon is exposed for 3–5 cm outside of the wound using traction. Direct visualization of the proximal tendon is achieved, minimizing potential injury to the sural nerve. A No. 2 Ethibond (Ethicon Inc., Cincinnati, Ohio, USA) suture is placed transversely through the most proximal end of the proximal stump. Both ends of this suture are then passed through the proximal stump in a figure-of-eight or crisscross manner (Figures 2 and 3). If the proximal end is severely retracted and cannot be identified in the initial incision, a second incision can be made 4–5 cm more proximally (Figure 4). A clamp is placed on the distal stump, and traction applied as a lumbar puncture needle is passed transversely through the most distal aspect of the tendon. Suture is passed through the needle, which can be performed with the aid of suction applied to the opposite side of the needle (Figure 5). The needle is withdrawn and reinserted diagonally so that it exits at the prior skin entry point. The suture is passed using the same technique. After the distal stump is secured, the two ends of the tendon are pulled into apposition. Direct visualization of the apposition is achieved through the incision to ensure that there is a contact of two ends and no residual gap. The sutures are tied with the foot in plantar flexion. The knots are buried beneath the paratenon, and the paratenon and subcutaneous tissue are closed in layers.
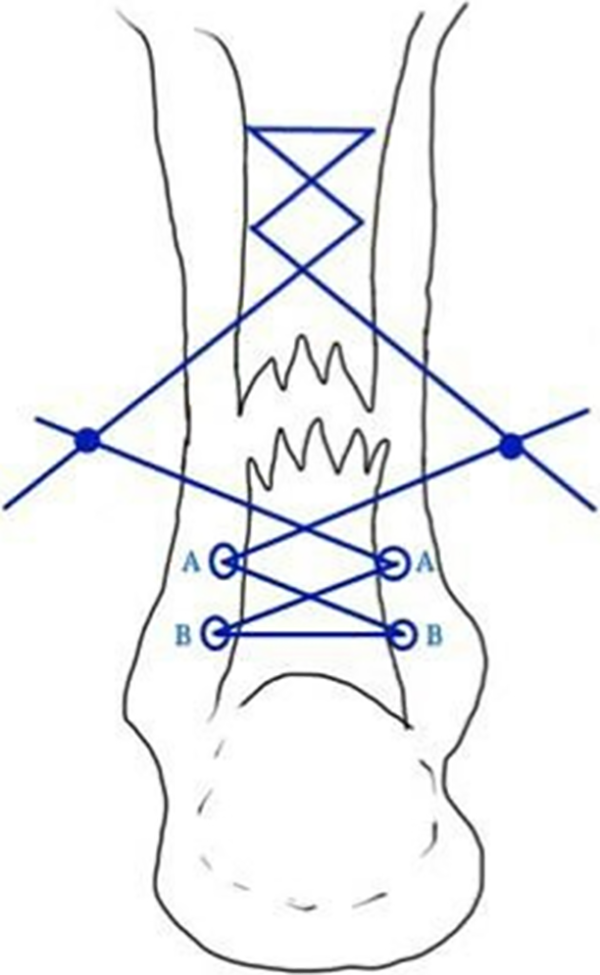
The ruptured tendon was sutured in Bunnell fashion. Symmetrical A and B points are skin stabs that threads pass through.

A transverse incision is made on skin between the proximal end and the distal end. The proximal end is pulling out.

If the retraction prohibits exposure of the proximal end, another incision is made 4–5 cm proximal to the first incision. The proximal end is pulling out through the second incision.

A lumbar puncture needle is transversely passed through the distal end of the very beginning. The thread is suctioned through the hollow needle by the aspirator.

The appearance of the scar.
Postoperative rehabilitation
The ankle is immobilized in a plantar flexed short leg cast with partial weight-bearing for 2 weeks. From postoperative third week, an adjustable orthosis is used and 10–30° plantar flexion is allowed. Full weight-bearing with clutch and 1-h daily stretching exercises are recommended. Walking without orthosis protection and a full range of motion exercise was permitted from sixth week postoperatively. Running and sports training were encouraged at 16 weeks.
Measures
The functional outcome was evaluated using ATRS at 3rd, 6th, 12th, and 24th month postoperatively and time return to work. The surgical outcomes include rerupture rate, overall complication rate, and operation time. The presence of any complications related to the treatment, such as sural nerve damage, wound infection, and rerupture, would be recorded. The operation time is defined as the time from the incision of skin to the completion of wound.
Statistical analysis
This was conducted using SPSS statistics v.19.0. Normality of the variable was tested using Shapiro–Wilk test. Normally distributed data were using independent-sample Student’s t-test for assessing differences between groups at one time point. In the independent sample t-test, the independent variable was the treatment group and the dependent variable was the continuous outcome. The results are presented as the mean ± SD. Nonparametric data were using Mann–Whitney test for assessment. The complication rate was compared using Pearson’s χ 2 test or Fisher’s exact test. The level of significance was set at p <0.05.
Results
There is no significant difference between both groups in demographic characteristics (Table 2). The average interval between injury and operation was 4.52 days (range 3–7 days) in the Achillon group and 4.64 days (range 3–7 days) in the MMIR group. Three patients were lost to follow-up after sixth month, and the data of the three patients were excluded from the analysis. Full follow-up was obtained for 43 cases in the Achillon group and 68 cases in the MMIR group.
Demographic characteristics.

MMIR: modified minimally invasive repair; M/F: male/female; L/R: left/right.
Functional outcome
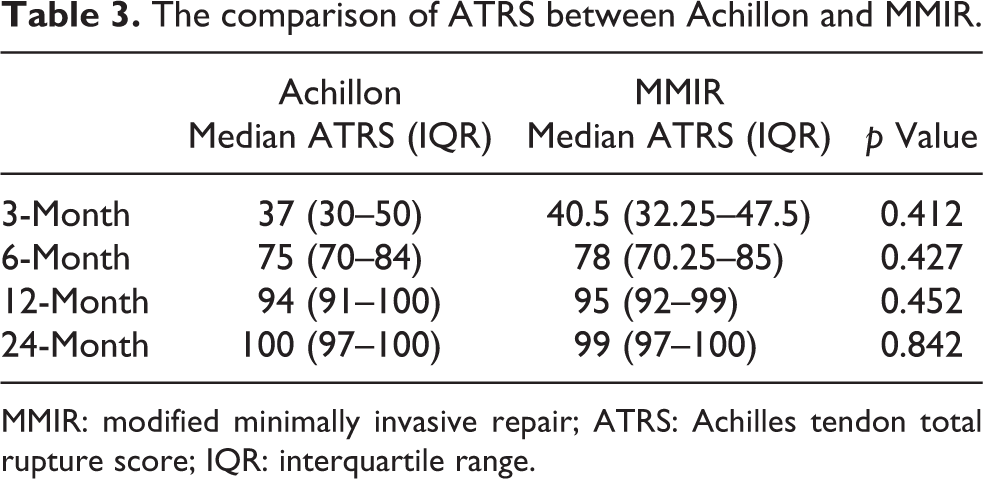
The outcomes were presented as median ATRS (interquartile range (IQR)) due to the abnormal distribution of the data. The median ATRS in the Achillon group was 37 (IQR 30–50) at 3-month evaluation, 75 (IQR 70–84) at 6-month evaluation, 94 (IQR 91–100) at 12-month evaluation, and 100 (IQR 97–100) at 24-month evaluation. The median ATRS in the MMIR group was 40.5 (IQR 32.25–47.5) at 3-month evaluation, 78 (IQR 70.25–85) at 6-month evaluation, 95 (IQR 92–99) at 12-month evaluation, and 99 (IQR 97–100) at 24-month evaluation. There is no significant difference between both groups at four points, respectively (Mann–Whitney U-test, p = 0.412, 0.427, 0.452, 0.842; Table 3). The time return to work in the Achillon group is earlier, however, the difference between both groups is not significant.
The comparison of ATRS between Achillon and MMIR.
MMIR: modified minimally invasive repair; ATRS: Achilles tendon total rupture score; IQR: interquartile range.
Surgical outcome
Reruptures occurred in five patients in the Achillon group and two patients in the MMIR group after the third month. Six patients experienced reruptures for the first time to take running exercise. Three patients who suffered a rerupture were treated nonoperatively at their own request and the others received revision surgery. All of them recovered without any other complications. Achillon group’s rerupture rate is higher, but the difference is not significant (Fisher’s exact test, 11.6% vs. 2.9%, p = 0.106). Sural nerve injury occurred in one patient treated with MMIR. Fortunately, the symptoms caused by sural nerve damage resolved within 1 year. There were two Achilles tendons tethering to skins found in the Achillon group. No wound infection, dehiscence, and Deep Vein Thrombosis (DVT) were found in both groups. Overall complication rate with MMIR is lower than the rate with Achillon (Fisher’s exact test, 16.3% vs. 4.4%, p = 0.044). The time cost of operations with Achillon is significantly less than that with MMIR (Student’s t-test, 34.84 vs. 39.71 min, p < 0.001; Table 4).
The comparison of outcomes between Achillon and MMIR.

MMIR: modified minimally invasive repair; ATRS: Achilles tendon total rupture score; SD: standard deviation.
Discussion
The best treatment for AATRs remains a topic of debate, with the options of nonoperative, open surgical, minimally invasive, and percutaneous approaches. Numerous randomized studies have been performed comparing operative versus nonoperative treatment, Achillon technique to open repair, and various percutaneous techniques to open repair. 2,10 –13 A number of meta-analyses have been performed based on these prospective studies. 2,3,6,14 –16 Traditional open surgical approach allows direct visualization of the tendon and ensures accurate apposition without any intervening gap, which likely contributes to the lower rerupture rate. However, the disadvantage of traditional open surgical approaches is an increased risk of wound infection. The traditional incision of open repair is a posterior midline incision that can be associated with high skin tension leading to skin necrosis, skin ischemia, wound healing delay, and wound dehiscence. The Achillon technique seems to be a promising method to treat AATRs with low wound infection, rerupture rate, and satisfactory functional outcome. But a cadaveric study presents a high risk (14.8%) of sural nerve damage through suturing with Achillon device in a neutral position. 5 The sural nerve injury risk is related to the device passers and the proximal passer needle has a higher risk. This trial is aimed to evaluate the functional and surgical outcomes of MMIR comparing with Achillon.
In our study, there was no patient undergoing sural nerve injury with Achillon technique, which consists with other reported trials and does not support the results of this cadaveric study. 6,17 Only one sural nerve violation occurred in a patient treated with MMIR, which resolved within 1 year. It may be contributed by excessive traction. The potential disadvantage of many percutaneous techniques is the risk of sural nerve injury that occurs with each blind pass of the needle through the skin. 18 Therefore, the risk of sural nerve injury about Achillon technique is inconclusive yet. MMIR can also decrease the risk for sural nerve injury seen in purely percutaneous approaches since the technique provides direct visualization of the proximal tendon stump, which is the area, where the sural nerve is at greatest risk. The sural nerve typically travels along the lateral border of the Achilles tendon and tracks more anteriorly as it approaches the distal aspect of the tendon, allowing the distal stump sutures to be safely placed percutaneously. The sural nerve is approximately 2 cm from the lateral border of the Achilles tendon at the level of its calcaneal insertion. 19
Two Achilles tendon tethered with skin, which may be caused by paratenon damage during the insertion of Achillon device. Limited open repair can preserve the integrity of paratenon contributing to vascularization and providing a gliding surface. 20
The median ATRS in the Achillon group was comparable with the score in the MMIR group at 3, 6, 12, and 24 months, respectively. The results are better than that in other reports. 10 According to us, the limited open and accelerated rehabilitation contributes to a better result (Table 5).
The comparison of outcomes in the literature.

MMIR: modified minimally invasive repair; ATRS: Achilles tendon total rupture score.
We found that the Achillon technique and MMIR described in this article were effective in decreasing rerupture following Achilles tendon repair. Direct visualization of the tendon apposition ensured that there is no gap present in the repair, a problem that can potentially occur in a purely percutaneous approach. The risk of rerupture is likely higher when a residual gap is present since the defect becomes filled with weaker fibrous tissue. In addition, preservation of the paratenon may permit improved vascularization and contribute to improved tendon healing. The rerupture rate was 11.6% in the Achillon group and 2.9% in the MMIR group. We consider this result as acceptable.
To decrease the wound infection risks, various percutaneous techniques have been developed. The advantages of percutaneous repair include decreased operative time, reduced use of analgesics, fewer deep infections, improved American Orthopedic Foot and Ankle Society scores, and lower healthcare costs. 4,24 No wound infections or dehiscence were found in this study. The skin incision used in both groups is parallel to the normal skin creases and is relaxed with slight foot plantar flexion, that is effective in avoiding wound healing complications and infections (Figure 6). In addition, we tried to preserve the paratenon, which is helpful in promoting tendon healing and smooth gliding and may also prevent superficial wound infections from spreading into deeper layers. 18
Percutaneous techniques using specialized equipment have been developed to minimize the risk of sural nerve injury. 25,26 The use of these devices allows the surgeon to accurately see the tendon ends to ensure direct apposition while minimizing nerve and wound-healing complications. The use of these devices also avoids the need for excessive surgical dissection, minimizing disruption of local vascularity. Achillon device is an excellent representative in them, but the use of this specialized equipment increases the overall operative cost.
The modified minimally invasive technique described in this article provides the benefits of direct tendon visualization with the decreased sural nerve injury risks seen in percutaneous approaches. The technique does not require specialized equipment and its associated cost. There were no wound dehiscence and infection in this series of patients treated with this MMIR. And the result is comparable with that in the Achillon group. We consider this MMIR as a safe and reliable method without increasing financial cost.
Our study has several limitations. The number of patients studied was small and their follow-up was limited to 2 years. Randomization is not carried out in this study. It is unable to avoid subjective bias. Since less patients would accept extra financial burden without more exact benefits from the approach. Further research should be based on the larger sample size and randomized controlled trial.
Conclusion
This study showed Achillon technique and modified MMIR to be similar in effectiveness. MMIR technique is safer and more economical, while the Achillon technique is significantly faster. Therefore, for AATR, we recommend MMIR.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.