
Abstract
Study Design
Retrospective propensity-score-matched cohort study.
Objectives
To evaluate whether postoperative glucagon-like peptide-1 receptor agonist (GLP-1 RA) use is associated with fewer complications, lower pseudarthrosis, and improved survival after lumbar fusion in adults aged 50 years and older.
Methods
The TriNetX Global Collaborative Network was queried to identify adults ≥50 years who underwent lumbar arthrodesis (2010-2025). GLP-1 RA exposure was defined as an active prescription within 1 to 90 days postoperatively. The comparison group consisted of patients without a GLP-1 RA prescription during this window. Propensity score matching adjusted for demographics, BMI, hemoglobin A1c, preoperative GLP-1 RA use, and comorbidities. Outcomes: 90-day and 1-year infectious, pulmonary, and thromboembolic complications, 1-year pseudarthrosis, and 1-year mortality rates. Survival was assessed with Kaplan Meier and Cox regression.
Results
Among 169 286 patients who underwent lumbar arthrodesis, 1844 had postoperative GLP-1 RA use and 167 442 did not. After matching, 1816 patients remained in each cohort. Postoperative GLP-1 RA use was associated with lower 90-day pneumonia (Risk Ratio [RR] 0.51), surgical site infection (RR 0.58), sepsis (RR 0.64), urinary tract infection (RR 0.56), wound dehiscence (RR 0.46), and venous thromboembolism (RR 0.54) (all P < 0.05), and 1-year lower hazard of death (HR 0.38; P = 0.018).
Conclusion
In this large propensity-score-matched cohort, postoperative GLP-1 RA use was associated with fewer early infectious, pulmonary, wound, and thromboembolic complications and improved 1-year survival after lumbar spinal fusion.
Keywords
Introduction
Obesity and Type 2 Diabetes Mellitus (T2DM) are prevalent diseases in the United States and are major drivers of escalating healthcare utilization.1–3 Approximately 34.9%, or 78.6 million, of US adults are obese 1 and 9.5% have T2DM. 3 By 2030, the prevalence of obesity is projected to be over 50%, 4 whereas 1 in 10 US adults are expected to have T2DM in 2040. 2 These metabolic conditions are common among spine surgery patients. Wiener et al noted that 70% of lumbar fusion patients are overweight or obese. 4 This is important because both these conditions are well understood to increase the risk of perioperative complications via impaired wound healing, altered immune function, and chronic systemic inflammation.1,2,5
Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) have transformed the current landscape in the management of obesity and T2DM. They can provide rapid weight loss, improved glucose control, and a mortality benefit in certain patients. 6 Roughly 12.5% of U.S. adults have been prescribed GLP-1 RA medication. 3 These medications are now understood to influence various surgically relevant pathways important to tissue healing and have become the subject of significant investigation across surgical disciplines.7,8
Prior large retrospective database studies evaluating spinal fusion cohorts have reported fewer complications and lower pseudarthrosis rates in patients taking GLP-1 RAs; however, nearly all of these studies defined GLP-1 RA exposure as a preoperative prescription. Many assumed continued postoperative use, despite little to no direct evidence that patients remained on therapy after surgery.3,4,9–17 This methodology cannot accurately separate these medication’s preoperative metabolic optimization effects from their direct anti-inflammatory influence during the postoperative healing period. Additionally, most of these studies analyze diabetic and obese patients separately, even though these conditions frequently overlap. Furthermore, an increasing proportion of GLP-1 RA prescriptions are now written for weight loss alone, which dilutes exposure groups and complicates interpretation. These issues are particularly relevant in older adults, who represent the largest group that is prescribed GLP-1 RAs, 18 and experience disproportionately higher postoperative complication rates compared to younger patients following spine surgery. 19
To address these gaps, we examined postoperative GLP-1 RA use, rather than preoperative exposure, in a spinal fusion cohort utilizing the TriNetX research database. We hypothesized that active GLP-1 RA therapy during the early postoperative period would be associated with fewer infectious and pulmonary complications, lower rates of pseudarthrosis, and decreased mortality after lumbar arthrodesis in adults aged 50 years and older.
Methods
Study Design & Source
We performed a retrospective, observational cohort study using the TriNetX research database, specifically the Global Collaborative Network. TriNetX is a federated electronic health records database that compiles real-time data from participating healthcare systems across the United States and other parts of the world. 20 The platform contains de-identified data from over 160 healthcare organizations worldwide and is compliant with HIPAA regulations, and thus this study was exempt from institutional review board approval.
Study Population
A query for adult patients ≥50 years who underwent a lumbar spine fusion between January 2010 and November 2025 was performed using CPT codes for lumbar arthrodesis. Eligible procedure codes included 22533, 22534, 22558, 22585, 22612, 22614, 22630, 22632, 22633, 22634 (Supplemental Table 1). Patients with any prior lumbar spine fusion code were excluded to ensure the study cohort was comprised of only index operations.
We restricted the cohort to adults aged ≥50 years to create a more homogeneous population in order to limit residual confounding, particularly confounding by indication. This older demographic is most commonly prescribed GLP-1 RAs, 18 are more likely to suffer from degenerative pathology, 9 and face higher rates of postoperative complications.5,21,22 Thus, the analysis focuses on patients who could potentially derive the most benefit from these medications.
Exposure cohorts were defined based on postoperative GLP-1 RA use. The GLP-1 RA cohort included patients with an active prescription for exenatide, liraglutide, dulaglutide, semaglutide, or tirzepatide between 1 to 90 days postoperatively. The comparison cohort consisted of patients without any recorded GLP-1 RA prescription during that same period.
Outcomes
The outcomes of interest were 90-day and 1-year postoperative complications: pneumonia, surgical site infection (SSI), sepsis, urinary tract infection (UTI), debridement and irrigation (D&I), wound dehiscence, venous thromboembolism (VTE), and pulmonary embolism (PE). Pseudarthrosis and mortality occurring within 1 year of the index procedure were also evaluated. Supplemental Table 1 lists the ICD-10 and CPT codes utilized to define each outcome.
Covariates and Matching
A 1:1 propensity score–matched (PSM) analysis was performed to limit confounding. Covariate selection followed recommendations from Brookhart et al, as we prioritized variables most likely associated with the outcomes of interest in order to reduce residual confounding. 23 These included age at index event, sex, diabetes mellitus, diseases of liver, nicotine dependence, diseases of arteries, arterioles, and capillaries, heart failure, chronic lower respiratory diseases, tobacco use, chronic kidney disease, inflammatory polyarthropathies, systemic connective tissue disorders, chronic ischemic heart disease, preoperative prescription for GLP-1 analogues, body mass index (further divided into: <20 kg/m2, 20 to <25 kg/m2, 25 to <30 kg/m2, 30 to <35 kg/m2, 35 to <40 kg/m2, 40 to <45 kg/m2, and ≥45 kg/m2.), and hemoglobin A1c (further divided into: <6.5, 6.5 to <7.5%, 7.5 to <8.5%, 8.5 to <9.5%, 9.5 to <10.5%, 10.5 to <11.5%, 11.5 to <12.5%, 12.5 to <13.5%, ≥13.5%). The covariate time window was any instance of documentation of these variables in the patient’s medical record from 3 months to 1 day before surgery.
Statistical Analysis
Analyses were conducted within TriNetX. Propensity score matching (1:1 nearest neighbor; caliper 0.1) was applied to balance covariates between exposure groups, with standardized mean differences (SMD) less than 0.10 considered acceptable balance. Continuous variables were compared using t-tests and categorical variables using χ2 tests. Risk ratios (RR) and absolute risk differences were calculated with 95% confidence intervals (CI) to estimate associations between GLP-1 RA use and 90-day postoperative complications. One-year all-cause mortality was evaluated using Kaplan–Meier survival analysis. Survival was compared using the log-rank test. A Cox proportional hazards model was then used to estimate the hazard ratio and 95% CI for mortality associated with postoperative GLP-1 RA use. Statistical significance was defined as P < 0.05.
Results
Patient Characteristics Before Propensity Score Matching
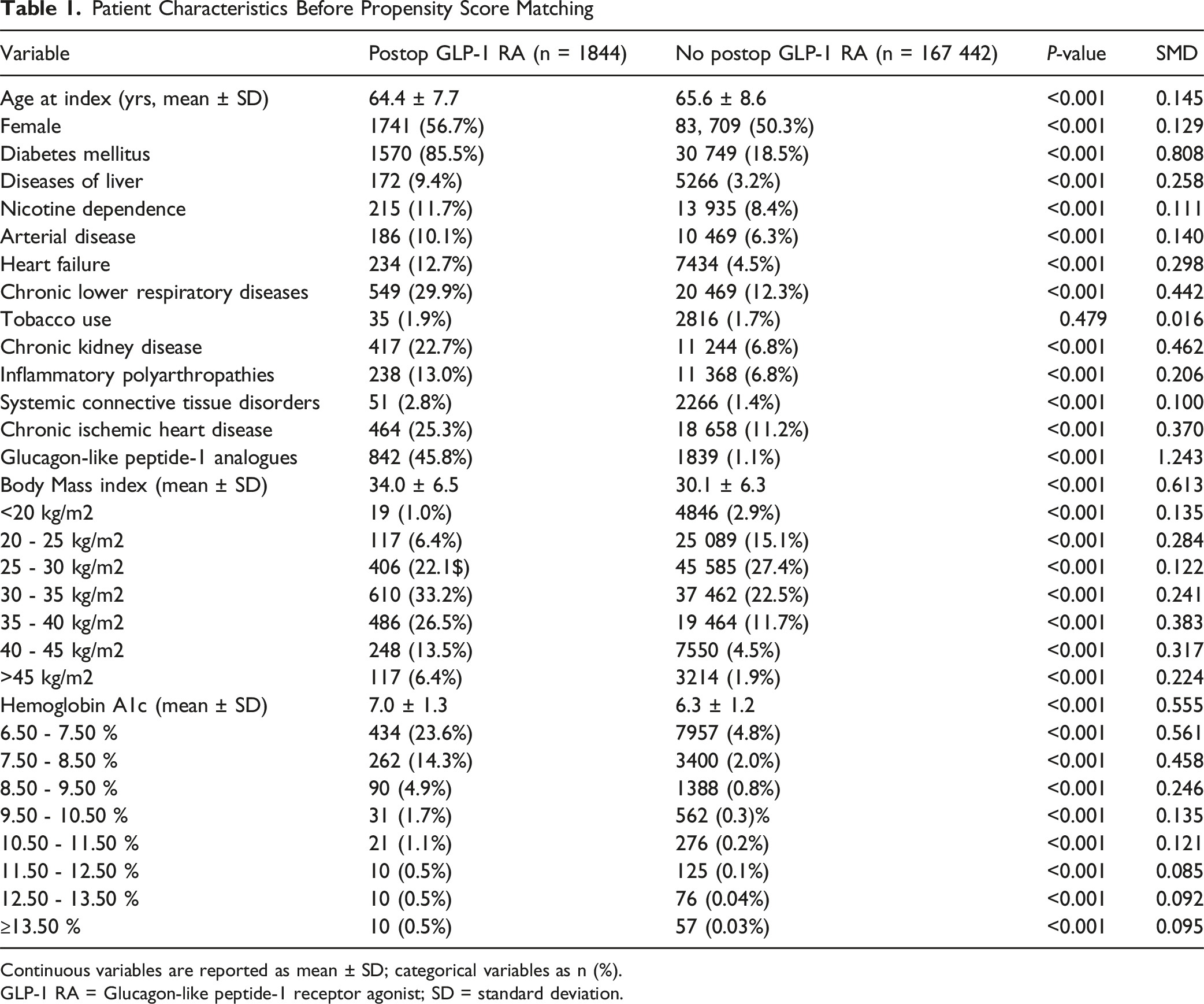
Continuous variables are reported as mean ± SD; categorical variables as n (%).
GLP-1 RA = Glucagon-like peptide-1 receptor agonist; SD = standard deviation.
Patient Characteristics After Propensity Score Matching
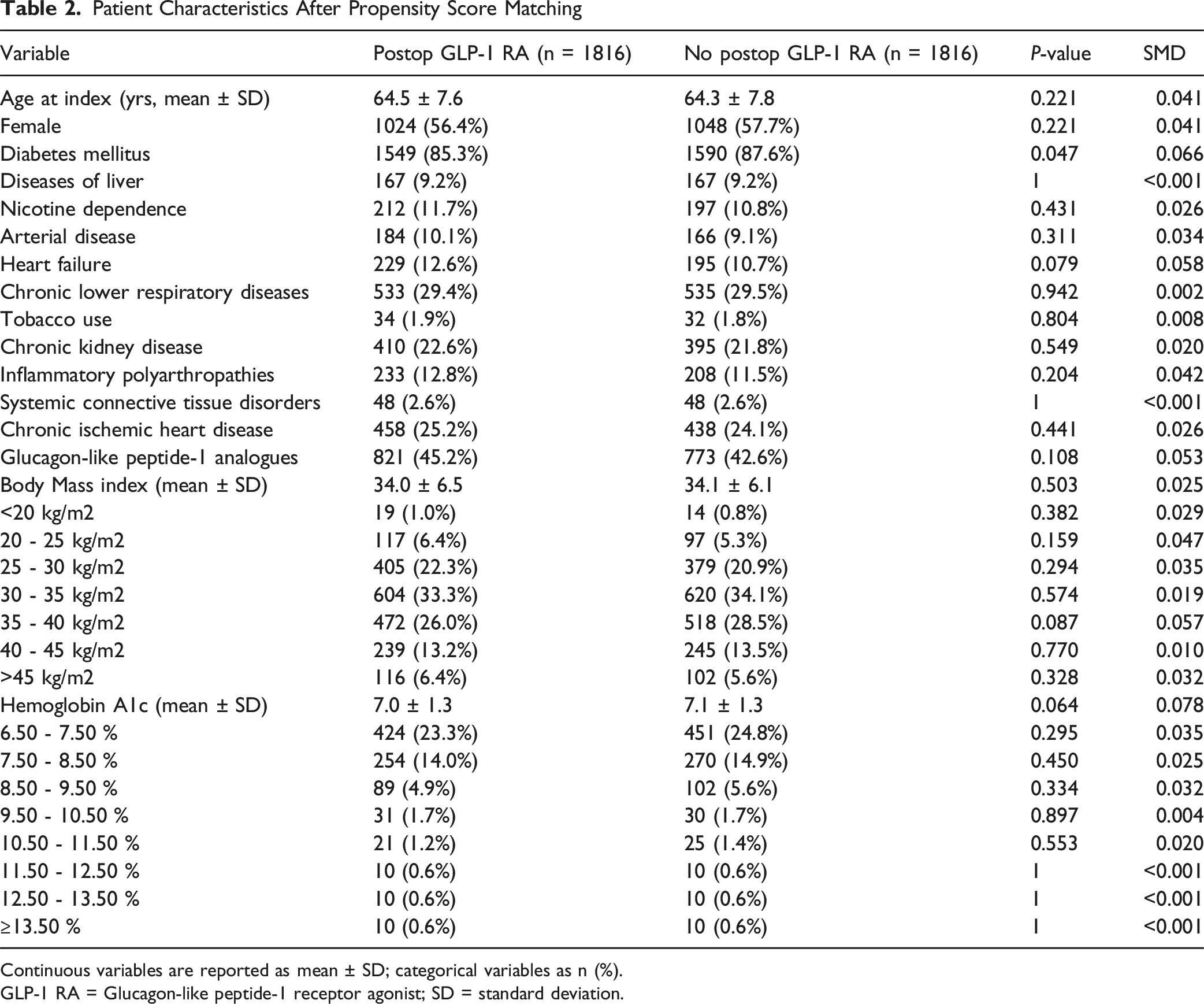
Continuous variables are reported as mean ± SD; categorical variables as n (%).
GLP-1 RA = Glucagon-like peptide-1 receptor agonist; SD = standard deviation.
Post-match Analysis of Outcomes after Lumbar Fusion Surgery
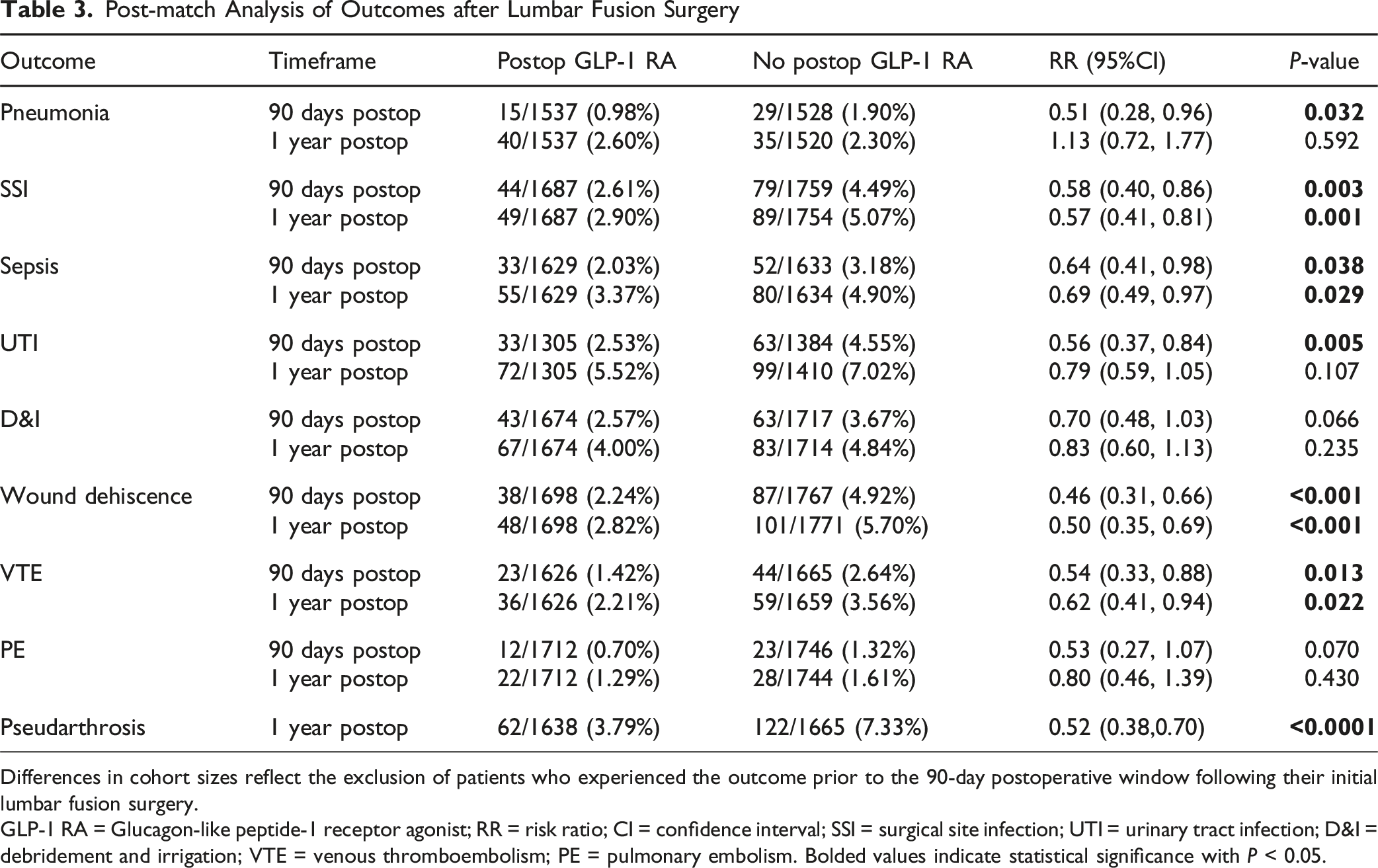
Differences in cohort sizes reflect the exclusion of patients who experienced the outcome prior to the 90-day postoperative window following their initial lumbar fusion surgery.
GLP-1 RA = Glucagon-like peptide-1 receptor agonist; RR = risk ratio; CI = confidence interval; SSI = surgical site infection; UTI = urinary tract infection; D&I = debridement and irrigation; VTE = venous thromboembolism; PE = pulmonary embolism. Bolded values indicate statistical significance with P < 0.05.
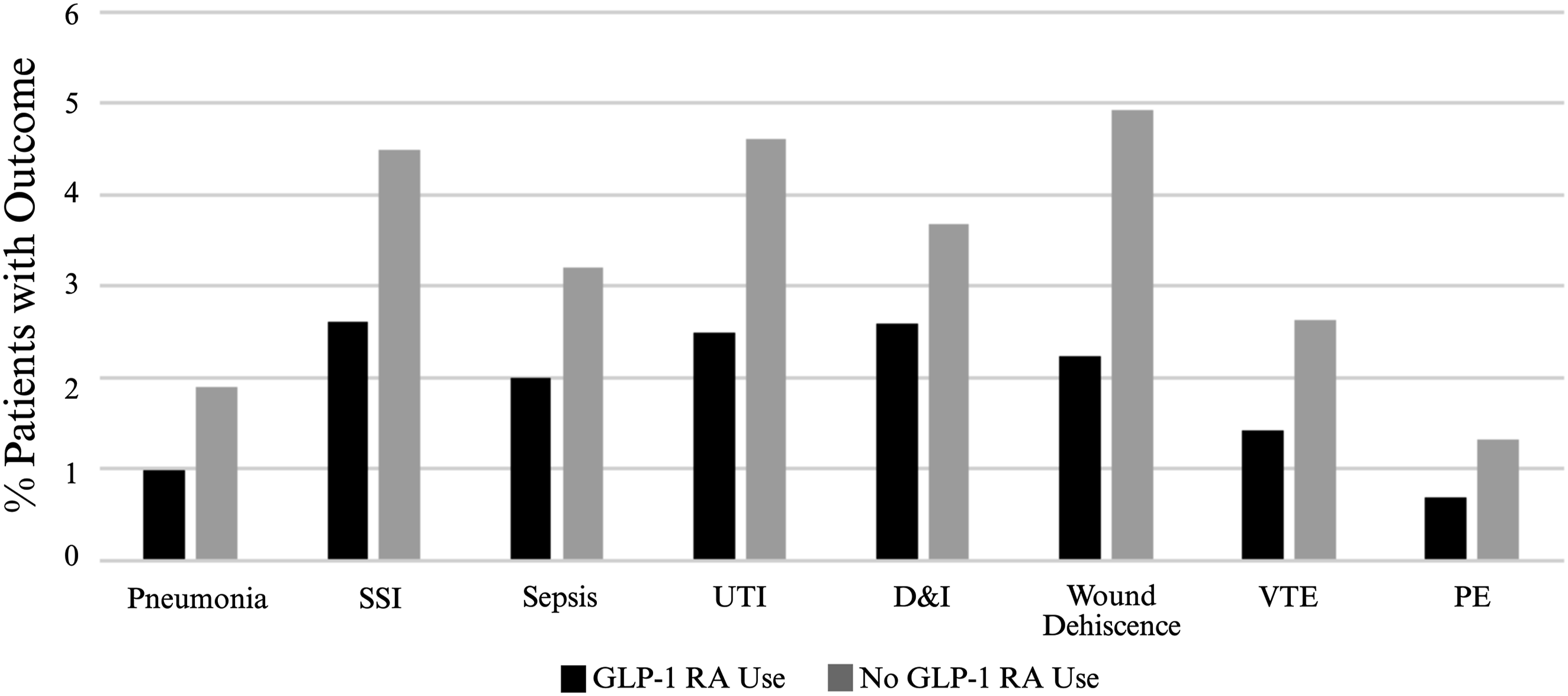
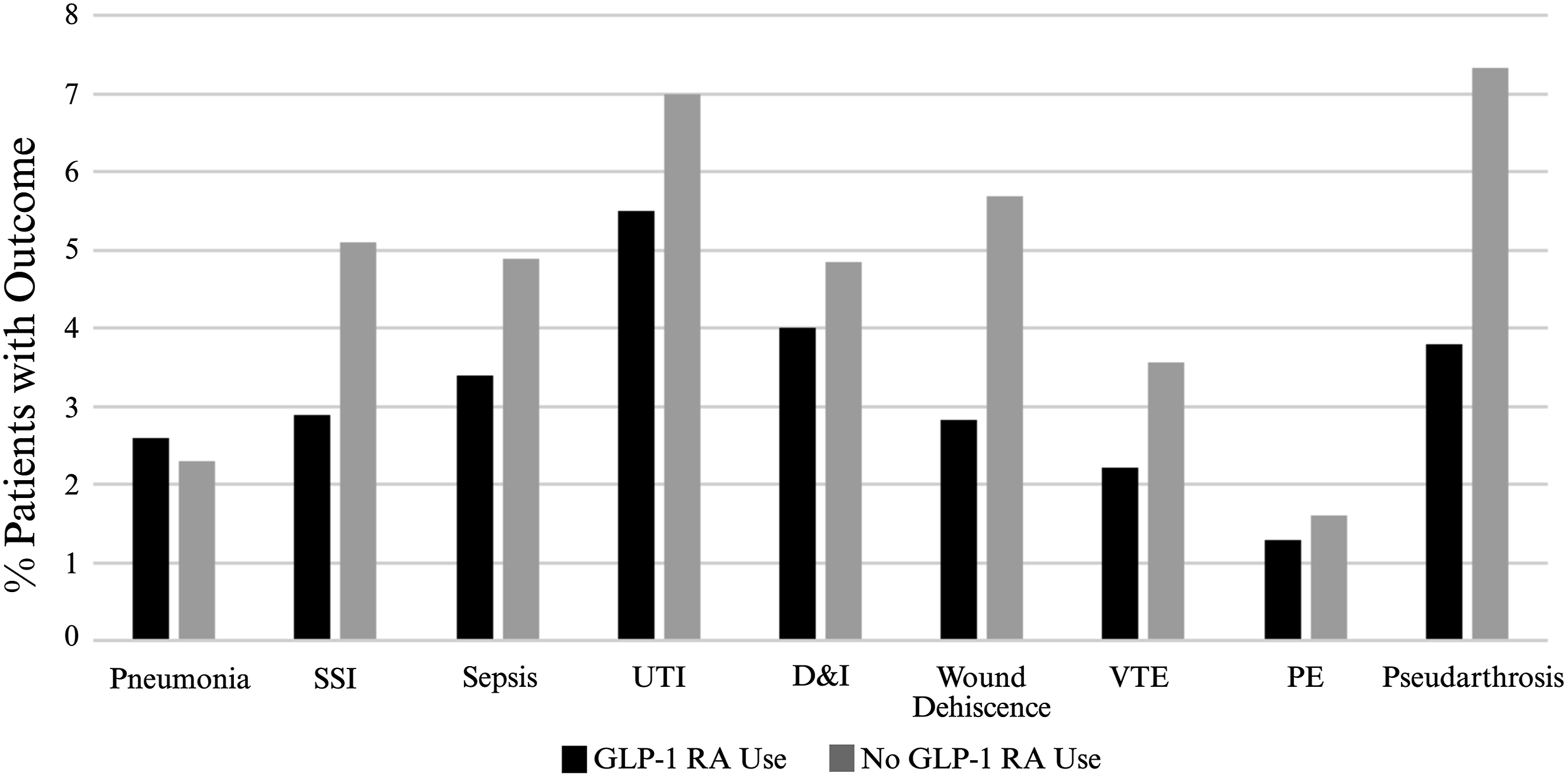
Ninety-day postoperative complication rates by postoperative GLP-1 receptor agonist use. Bars show the percentage of patients with each complication within 90 days of index surgery. Abbreviations: GLP-1 RA = Glucagon-like peptide-1 receptor agonist; SSI = surgical site infection; UTI = urinary tract infection; D & I = debridement and irrigation; VTE = venous thromboembolism; PE = pulmonary embolism. Black Bars = GLP-1 RA use, Gray Bars = No GLP-1 RA use
One-year postoperative complication rates by postoperative GLP-1 receptor agonist use. Bars show the percentage of patients with each complication within 1 year of index surgery. Abbreviations: GLP-1 RA = Glucagon-like peptide-1 receptor agonist; SSI = surgical site infection; UTI = urinary tract infection; D & I = debridement and irrigation; VTE = venous thromboembolism; PE = pulmonary embolism. Black Bars = GLP-1 RA use, Gray Bars = No GLP-1 RA use
At 90 days postoperatively, GLP-1 RA users were 49% less likely to develop pneumonia (RR 0.51, 95% CI 0.28-0.96; P = 0.032), 42% less likely to develop an SSI (RR 0.58, 95% CI 0.40-0.86; P = 0.003), 36% less likely to develop sepsis (RR 0.64, 95% CI 0.41-0.98; P = 0.038), and 44% less likely to develop a UTI (RR 0.56, 95% CI 0.37-0.84; P = 0.005). Postoperative GLP-1 RA use was also associated with a 54% reduction in wound dehiscence (RR 0.46, 95% CI 0.31-0.66; P < 0.001) and a 46% reduction in VTE (RR 0.54, 95% CI 0.33-0.88; P = 0.013).
At 1 year following lumbar fusion, GLP-1 RA use remained associated with significantly lower rates of SSI (RR 0.57, 95% CI 0.41-0.81; P = 0.001), wound dehiscence (RR 0.50, 95% CI 0.35-0.69; P < 0.001), VTE (RR 0.62, 95% CI 0.41-0.94; P = 0.022), and pseudarthrosis (RR 0.52, 95% CI 0.38-0.70; P < 0.001).
One-Year Survival and Mortality after Spine Surgery by GLP-1 RA Use

KM = Kaplan-Meier; GLP-1 RA = Glucagon-like peptide-1 receptor agonist. Bolded values indicate statistical significance with P < 0.05. *Log-rank χ2 = 20.754 (df = 1).
Discussion
In this large, multicenter PSM cohort study within the TriNetX research database, postoperative exposure to GLP-1 RAs within the first 3 months following lumbar fusion was associated with a significantly lower incidence of early postoperative medical complications. This study is novel due to the fact that GLP-1RA exposure was defined as use in the postoperative period, whereas prior large database studies have only assessed preoperative or a combined pre and postoperative exposure to these medications.3,4,9–11,13,14,24–26 By isolating active use during the recovery period, our findings directly address a clinically relevant question for spine surgeons regarding the safety and even the potential benefit of initiating or resuming GLP-1 RA therapy immediately after lumbar fusion. Importantly, propensity score matching achieved excellent balance across BMI and hemoglobin A1c, allowing for comparison of patients with similar metabolic phenotypes who did or did not receive a GLP-1 RA. The persistence of these significant outcome associations despite matching suggests that the observed benefit of these medications is not solely due to differences in weight or glycemic control, but instead may relate to GLP-1 RA effects beyond metabolic regulation, including anti-inflammatory pathways that could mitigate postoperative complications.
The analysis demonstrated that postoperative GLP-1 RA use was associated with lower 90-day rates of several significant medical complications such as pneumonia, SSI, sepsis, UTI, wound dehiscence, and VTE (Table 3). These associations were most pronounced in the 90-day postoperative window, which aligns with the period when systemic inflammation, immune dysregulation, and endothelial dysfunction most strongly contribute to morbidity after lumbar spine fusion.7,27,28
At 1 year postoperatively, pneumonia and UTI rates were similar between the 2 groups. In contrast, the lower rates of SSI, sepsis, wound dehiscence, and VTE for GLP-1 RA users persisted at 1 year (Table 3). These later findings should be interpreted cautiously, as GLP-1 RA exposure was defined only within the first 90 postoperative days, and events at 1 year are more likely influenced by baseline comorbidities and other exposures unrelated to the index surgery. However, the sustained differences in many complication rates at 1 year postoperatively may reflect the broad systemic effects of GLP-1 RAs on these outcomes, independent of surgical exposure. Preclinical and clinical evidence has shown that GLP-1 RAs directly influence critical inflammatory and immunomodulatory pathways. 7 Thus, although GLP-1 RAs limit chronic hyperglycemia, a known risk factor for postoperative infection and pulmonary complications,22,29 the observed reductions in these complications may also reflect anti-inflammatory effects beyond glycemic control alone. Our methods also support this interpretation, as we included non-diabetic patients in the analysis and most recent HbA1c in the matching process, suggesting that the observed associations are not explained by improved glycemic control alone.
Importantly, postoperative GLP-1 RA use was associated with roughly a 50% lower 1-year risk of pseudarthrosis (RR 0.52; P < 0.0001; Table 3). Multiple studies have demonstrated reduced pseudarthrosis rates among patients prescribed GLP-1 RAs prior to spine surgery,3,9,10,13 and recent systematic reviews and meta-analyses have supported these findings.25,26 However, these studies largely defined exposure as preoperative prescription only, or included a range of 6 months pre- and postoperatively.9,10 Therefore, these data cannot support the conclusion that continued GLP-1 RA therapy during the postoperative period influenced fusion success.
As previously mentioned, the present study’s exposure definition suggests that continued or new GLP-1 RA therapy during the postoperative period may play a direct role in promoting successful fusion, rather than attributing the effects on fusion to preoperative metabolic and glycemic optimization. This is critical for spine surgeons who may face decisions of whether patients should resume or are safe to start a new GLP-1 RA in the postoperative period. Our findings support their safety and even favorable complication profile after lumbar spine surgery.
Most notably, postoperative GLP-1 RA exposure was associated with lower 1-year mortality and higher Kaplan-Meier survival in this analysis (Table 4). Kaplan-Meier estimates found significantly higher survival at 1 year (log-rank P < 0.001) and Cox proportional hazards modeling found a 62% lower hazard of death (HR 0.38, 95% CI 0.24-0.58, P = 0.018). This is consistent with prior literature that reports clinically significant cardiovascular and mortality benefits of GLP-1 RAs in non-surgical populations.6,13 Our findings suggest an even larger protective mortality signal in this lumbar fusion cohort, but this should be interpreted cautiously given the retrospective design of the present study compared with the high-quality randomized controlled trials included in Rivera et al. 6 Regardless, spine surgeons should recognize that these medications provide substantial benefits that extend far beyond postoperative complication reduction.
In addition to appetite suppression and glycemic control, GLP-1 RA’s exert direct biologic effects via various anti-inflammatory pathways. Basic science and clinical evidence demonstrate that GLP-1 RAs suppress nuclear factor–κB signaling, reduce pro-inflammatory cytokine production, and enhance anti-inflammatory pathways. 7 These agents can drastically improve endothelial function and microvascular perfusion, aiding immune system function, tissue oxygenation, and wound healing. Direct reductions in cytokines such as tumor necrosis factor-alpha (TNF-α) and interleukin-6 (IL-6) have been found in patients using these medications, independent of weight loss. 7 Collectively, these mechanisms provide biologic plausibility for the reductions in infection, wound complications, VTE, and mortality observed in our study.
This study has several strengths. It represents one of the largest multicenter analyses evaluating GLP-1 RA use in spine surgery and is the first to define exposure specifically and only during the postoperative period, which is most relevant to complications that occur in the postoperative setting. Rigorous propensity score matching was used to minimize baseline differences, and outcomes were assessed at two clinically meaningful timepoints. Finally, inclusion of both diabetic and non-diabetic patients allowed evaluation of GLP-1 RA effects beyond glycemic control alone and thus improves the generalizability of our findings.
Importantly, a recent meta-analysis of GLP-1 RA use in spine surgery noted that prior studies did not ensure metabolic comparability between exposure groups, particularly with respect to BMI thresholds, glycemic control, concurrent metabolic therapies, and complications of obesity and diabetes. 24 The present study addressed several of these concerns by incorporating detailed BMI and hemoglobin A1c stratification into matching, adjusting for diabetes status and preoperative GLP-1 analogue use, and matching on multiple comorbid conditions commonly associated with metabolic disease. This approach improves comparability between these groups and strengthens confidence that the observed associations are not simply attributable to baseline metabolic differences.
This study also has limitations. Given its retrospective nature, causality cannot be inferred, and residual confounding persists despite matching. TriNetX lacks granular procedural detail, limiting adjustment for surgical complexity, fusion technique, and surgeon-specific or institution-specific factors. Medication adherence, dosage, and duration cannot be verified in TriNetX. Nonetheless, the consistency of increased complications across multiple categories, different timepoints, and the analytic approach utilized in this study strengthens confidence in the validity of observed findings.
Conclusion
In this propensity-matched cohort study, postoperative GLP-1 RA use demonstrated a protective association with early complications after lumbar spine fusion. Postoperative GLP-1 RA use was associated with lower rates of 90 day infectious and pulmonary complications and venous thromboembolism, as well as reduced 1-year pseudarthrosis and lower 1-year mortality. These findings support continuation of GLP-1 RAs in the immediate postoperative period and suggest that postoperative GLP-1 RA use may be a potential strategy to reduce morbidity in an increasingly metabolically complex spine surgery population. Future prospective studies could evaluate these medications in postoperative spine surgery patients to determine whether they causally reduce early infectious, pulmonary, and thromboembolic complications.
Supplemental Material
Supplemental material - Reduced Complications and Improved Survival With Postoperative GLP-1 Receptor Agonist Use Following Lumbar Arthrodesis
Supplemental material for Reduced Complications and Improved Survival With Postoperative GLP-1 Receptor Agonist Use Following Lumbar Arthrodesis by Emma Proffitt, BA, Samuel W. Rice, MD, Ryan Schiedo, MD and Michael Stauff, MD in Global Spine Journal
Footnotes
Ethical Considerations
This study used a HIPAA-compliant, de-identified database and was therefore exempt from institutional review board approval.
Author Contributions
Emma Proffitt: Conceptualization, Background Research, Data Analysis, Figure Creation, Manuscript Writing & Editing. Samuel Rice: Conceptualization, Background Research, Data Analysis, Manuscript Writing & Editing. Ryan Schiedo: Conceptualization, Methodology, Manuscript Writing & Editing, Supervision. Michael Stauff: Conceptualization, Methodology, Manuscript Writing & Editing, Supervision.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data are available through TriNetX Global Collaborative network and are not publicly available.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.