
Abstract
Study design
Retrospective study.
Objective
This study aims to evaluate and compare the accuracy and safety of 3D-printed navigation templates (3D-PNT), O-arm-based S8 navigation (O-S8), and freehand technology (FT)-assisted C2 pedicle screw (C2PS) placement in patients with high-riding vertebral arteries (HRVAs).
Methods
130 HRVA patients undergoing upper cervical spine surgery were included and classified based on the use of 3D-PNT, O-S8, or FT. The primary outcome was C2PS placement accuracy. Secondary outcomes included screw placement time, operative time, blood loss, radiation exposure, technical cost, hospital stay, and complications.
Results
The C2PS placement time, operative time, and fluoroscopy duration in the 3D-PNT group were significantly shorter than those in the other two groups, while the fluoroscopy time for O-S8 was significantly longer than the others. Postoperative VAS and JOA scores significantly improved compared to preoperative levels, with no significant intergroup differences. The accuracy rates (grades 0 + 1) were 92.59% (3D-PNT), 90.38% (O-S8), and 70.17% (FT), with 3D-PNT and O-S8 outperforming FT, though no significant difference in accuracy was found between 3D-PNT and O-S8.
Conclusions
Both 3D-PNT and O-S8 improve the accuracy and safety of C2PS in HRVA patients compared to FT. 3D-PNT demonstrated superior performance in reducing screw placement and fluoroscopy times compared to O-S8. However, the requirement for patient-specific customization and preoperative planning limits its immediate applicability in emergency surgeries.
Keywords
Introduction
C2 internal fixation technology is a pivotal advancement in spine surgery, significantly enhancing the development of upper cervical procedures. Specifically, C2 pedicle screw (C2PS) placement is frequently the preferred method of internal fixation for posterior upper cervical surgery. Biomechanical studies have demonstrated that C2PS placement provides superior control and pull-out strength, with the internal fixation system formed by C2PSs offering optimal fixation strength.1-3 However, C2’s complex anatomy, proximity to critical vessels and nerves, and high incidence of vertebral artery variations pose significant challenges.
Previous studies report a high incidence of high-riding vertebral artery (HRVA) in C2, ranging from 14.5% to 32%.4-6 Bloch et al defined HRVA as an isthmus internal height less than 2 mm, an isthmus height under 5 mm, or both. 7 The presence of HRVA increases the difficulty of C2PS placement and the risk of vascular injury, necessitating high precision in screw placement to minimize the risk of vascular damage. While C2PS placement using the freehand technique (FT) is commonly employed in upper cervical surgeries,8-10 it remains challenging for even experienced spine surgeons in patients with HRVAs.
Advances in medical imaging and digital orthopedic technologies have led to the adoption of intraoperative navigation and 3D-printed navigation template (3D-PNT) technology for improved screw placement accuracy. Previous studies have shown that navigation and navigation template technologies significantly enhance the precision of C2PS placement, thereby increasing the safety and efficacy of upper cervical surgery.11-13 However, a review of the literature reveals no studies directly comparing the advantages and disadvantages of 3D-PNT, O-arm-based S8 navigation (O-S8), and FT in assisting C2PS placement in patients with HRVAs. This study aims to compare and analyze the accuracy and safety of C2PS placement assisted by these three technologies in patients with HRVAs.
Materials and Methods
Inclusion and Exclusion Criteria
The inclusion criteria were as follows: (1) all patients had one HRVA or two HRVAs, where the standard for HRVA was as follows: the C2 isthmus height (the thickness of the isthmus as measured at the midpoint of atlantoaxial joint) was less than 5 mm, the C2 isthmus internal height (distance from the top of the vertebral foramen to the roof of the superior facet) was less than 2 mm, or both; (2) C2PS placement of the HRVA was assisted by 3D-PNT, O-S8 or the FT; and (3) the preoperative and postoperative data of the patients were complete. The exclusion criteria were as follows: (1) preoperative CTA showed that patients with severe HRVAs or HRVAs combined with pedicle stenosis could not undergo C2PS placement; (2) a tumor or infection of the upper cervical spine; (3) previous history of upper cervical spine surgery; and (4) patients with severe osteoporosis.
Patients and Baseline Data
Comparison of General Data Among the Three Groups
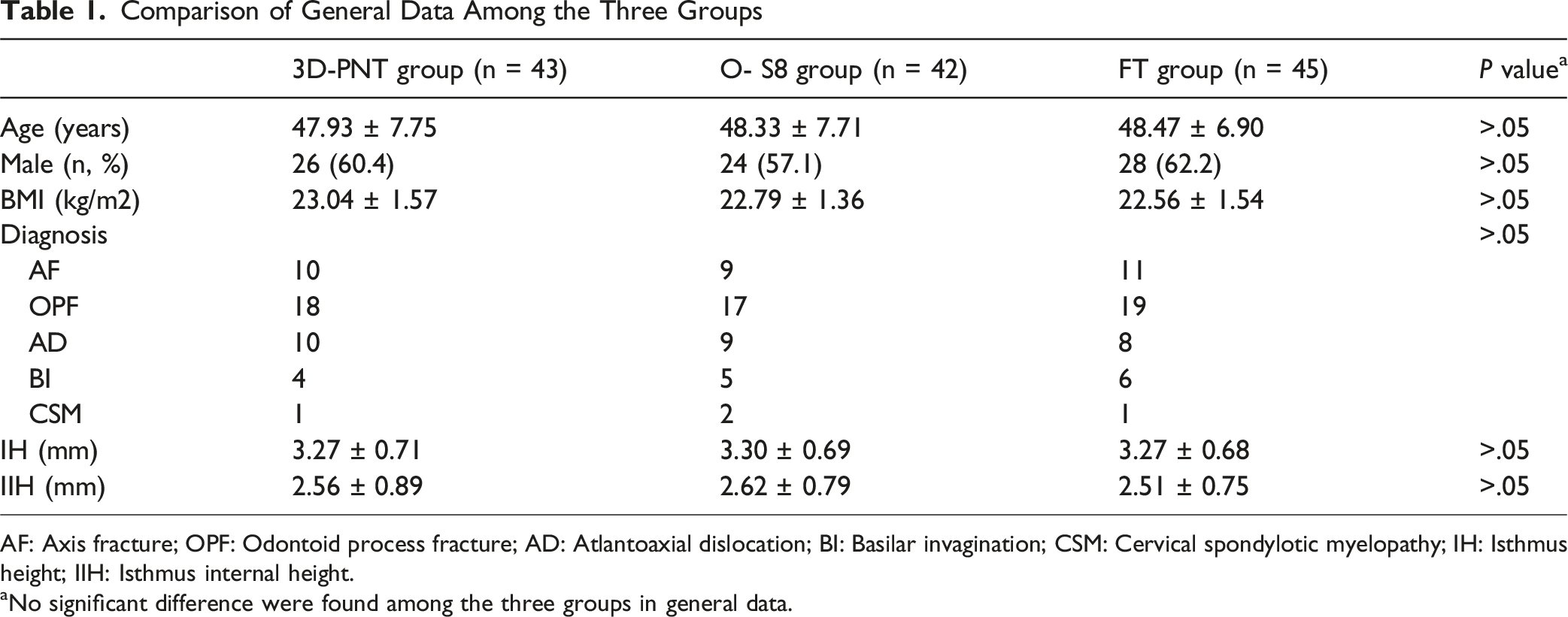
AF: Axis fracture; OPF: Odontoid process fracture; AD: Atlantoaxial dislocation; BI: Basilar invagination; CSM: Cervical spondylotic myelopathy; IH: Isthmus height; IIH: Isthmus internal height.
aNo significant difference were found among the three groups in general data.
Surgical Strategy
3D-PNT group: Production of 3D-PNT:All patients underwent plain CT scanning (0.5 mm slices) of the cervical spine at the operative segment before the operation. The obtained CT image data were stored in DICOM format and then imported into the 3D reconstruction software Mimics 17.0 (Materialise company, Belgium) for C2 3D model reconstruction. The reconstructed model was imported into 3-Matic (Materialise company, Belgium) software in STL format, and the screw position, direction and length were simulated to design the optimal screw path for the C2PS. The morphological anatomy of the C2 spinous process, lamina and lateral mass was extracted. The reverse template consistent with the above anatomical morphology was designed and fitted with the optimal screw path for the C2PS in the software to form a navigation template with two positioning guide holes. Finally, we saved the C2 3D model and template file as an STL file and input them into 3DS project 3600 photosensitive resin printing equipment (3DS company, the United States) to print out the C2 3D model and navigation template. The C2 3D model and 3D-PNT (Figure 1A and B) were sterilized with a plasma sterilizer before the operation, and we simulated C2PS placement in the 3D model. During the operation, the C2 spinous process, lamina and lateral mass were fully exposed, 3D-PNT was tightly attached to the posterior surface of C2, and the assistant assisted with the fixation (Figure 1C and D). We used a high-speed drill to drill the screw path along the direction of the guide hole and then used a probe to assess the safety of the four walls before placing the C2PSs with appropriate lengths. (A & B). 3D model and 3D-PNT of C2,it can be used to simulate screw placement before operation. (C & D). The 3D-PNT assisted C2PS placement in the operation
O-S8 group: After general anesthesia, the patient was placed in the prone position, and the paravertebral muscles were fully detached to complete the bone exposure. And the O-AN device was connected. We fixed the navigation reference frame on the C3 Spinous process and covered it completely with a sterile sheet. The CT images of the cervical spine were obtained by self-rotating scanning of the O-arm (Arcadis Orbic 3D, Siemens Healthcare GmbH Henkestr, Erlangen, Germany) and then automatically transferred to the navigation system (StealthStation S8,Medtronic) for registration and accuracy verification. The navigation probe was used to determine the optimal entry point and direction of the C2PS under the guidance of the CT image (Figure 2), and then the navigation drill was used to complete the preparation of the screw path along the predetermined trajectory. Then, we used a probe to assess the safety of the four walls before placing the C2PSs with appropriate lengths. Before each screw preparation, the navigation probe was used to contact the bone anatomical markers of the patient’s operative segments to confirm the accuracy of the navigation. (A). Simulating optimal screw placement under S8 navigational guidance. (B & C). Using navigational probe guidance on CT images to determine the optimal screw placement point and direction for C2PS insertion
FT group: After general anesthesia, the patient was placed in the prone position, and the paravertebral muscles were fully detached to complete the bone exposure. We determined the entry point and direction of the C2PS based on traditional anatomical signs and preoperative planning. Then, we used a high-speed drill to complete the preparation of the screw path and placed the C2PSs with appropriate lengths.
All surgeries were performed by two senior spine surgeons with extensive experience in upper cervical spine surgery. Prior to this study, both surgeons routinely performed freehand C2PS placement and had received standardized training in navigation systems. Additionally, they had experience in designing, preoperatively simulating, and applying 3D-PNT during surgery.
Evaluation Methods
HRVA was evaluated based on the C2 isthmus height and isthmus internal height, measured through preoperative CT reconstructions or CTA (Figure 3). On the PACS system, the width of the C2 pedicle in HRVA cases was measured using PacsClient software. All C2PS placements in HRVAs were analyzed on the PACS system, and preoperative imaging confirmed the feasibility and safety of the screw insertion trajectory. Postoperatively, all patients underwent CT scans (0.5 mm thickness) of the fixed segments 4 to 7 days after surgery. Screw grading followed the criteria proposed by Kawaguchi et al
14
based on axial CT images. The grading system was as follows: grade 0—screw entirely within the pedicle; grade 1—screw perforates the pedicle wall by 2 mm or less; grade 2—screw breaches the pedicle wall by 2 mm or more; grade 3—vertebral artery or nerve injury. The maximal cortical breach or screw deviation, as seen on the axial CT slice, determined the grade. Multiplanar reconstructions (axial, sagittal, and coronal views) were reviewed for accuracy. Postoperative CT evaluations were conducted by two experienced spine surgeons, who were blinded to the screw insertion technique (3D-PNT, O-S8, or FT). Imaging data were anonymized to avoid bias. Inter observer agreement was good, and any discrepancies were resolved through discussion. Grade 0 screws were considered perfect, while grade 0 and grade 1 screws were deemed clinically acceptable. Grade 2 and grade 3 screws were classified as true malpositions. The accuracy of screw placement was assessed using grade 0 + 1 screws. This classification accounted for HRVA anatomical variations and aligned with clinical safety considerations. Even in cases with narrow pedicle widths, screws were deemed clinically acceptable as long as there was no significant cortical violation or vascular or neural injury. The following parameters were recorded and compared across the three groups: single C2PS placement time, total operation time, fluoroscopy time, intraoperative blood loss, operation cost, hospitalization time, and surgery-related complications. Fluoroscopy time was defined as the actual intraoperative imaging exposure time. For the 3D-PNT and FT groups, fluoroscopy time primarily reflected intermittent conventional C-arm fluoroscopy for intraoperative confirmation and postoperative verification. In contrast, the O-S8 group’s fluoroscopy time included the time for O-arm 3D scanning. Additionally, VAS scores and cervical JOA scores were compared among the groups preoperatively and at 3 days, 6 months, and the last follow-up postoperatively. (A). Using coronal CT images, the midline of the atlantoaxial joint (X) was determined based on the vertebral artery groove, and the corresponding sagittal CT images were obtained to identify HRVA. (B). First,we determined the top (yellow dot) of the VA groove (asterisk), isthmus internal height (A) is the distance from the yellow dot to the roof (red dot) of the superior facet,isthmus height (B) is defined as the minimum vertical distance between the superior and inferior cortices of the C2 pedicle isthmus. HRVA was defined as an isthmus height of less than 5 mm and/or isthmus internal height of less than 2 mm
Statistical Analysis
Statistical analysis was performed using SPSS 21.0 software. Continuous variables are expressed as the mean ± standard deviation (SD), while categorical variables are presented as frequencies and percentages. Prior to conducting one-way analysis of variance (ANOVA), the assumptions of normality and homogeneity of variances were checked. Normality was assessed using the Shapiro–Wilk test, and homogeneity of variances was evaluated using Levene’s test. One-way ANOVA was used to compare differences among the three groups. When a significant overall difference was identified, post-hoc pairwise comparisons were performed using Tukey’s honestly significant difference test or the Games–Howell test, as appropriate. Categorical variables were analyzed using the chi-square test or Fisher’s exact test, as needed. Paired t-tests were used for within-group comparisons. A P-value <.05 was considered statistically significant.
Results
Accuracy Evaluation
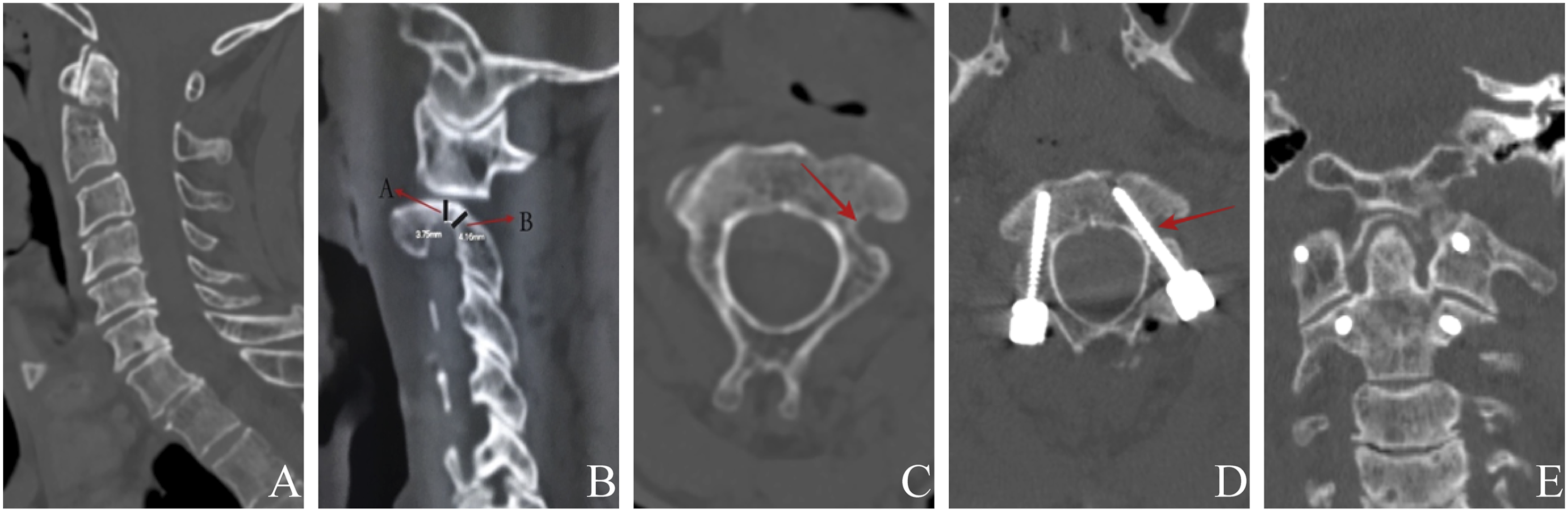
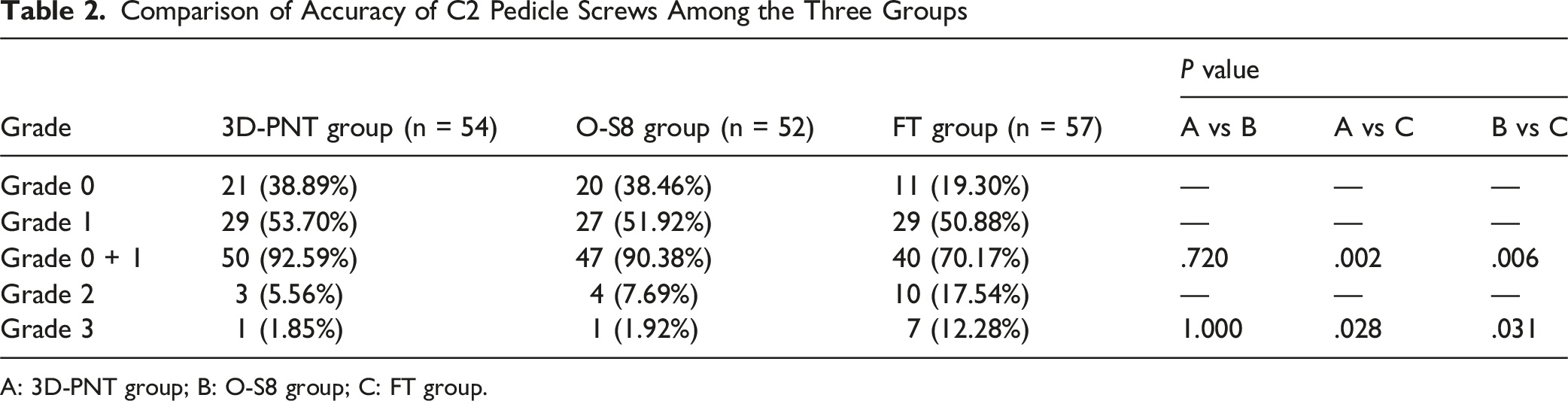
A total of 54 C2PSs were inserted in 3D-PNT group (Figure 4), and postoperative CT evaluation showed 21 grade 0 screws, 29 grade 1 screws, 3 grade 2 screws and 1 grade 3 screws. The accuracy of C2PS placement was 92.59% (50/54). A total of 52 C2PSs were inserted in O-S8 group (Figure 5): 20 grade 0 screws, 27 grade 1 screws, 4 grade 2 screws, and 1 grade 3 screw. The accuracy of C2PS placement was 90.38%% (47/52). A total of 57 C2PSs were inserted in FT group (Figure 6): 11 grade 0 screws, 29 grade 1 screws, 10 grade 2 screws and 7 grade 3 screws, and the accuracy was 70.17% (40/57). The accuracy of C2PS placement in 3D-PNT group and O-S8 group is significantly higher than that in FT group, but there was no significant difference between 3D-PNT group and O-S8 group. In addition, the proportion of grade 3 screw in 3D-PNT group and O-S8 group is significantly lower than that in FT group while there was no significant difference between this two groups (Table 2). A 48-year-old male patient was preoperatively diagnosed with odontoid process fracture. C2PS placement was assisted by 3D-PNT during operation. (A & B). Preoperative CT reconstruction showed odontoid process fracture. (C). Isthmus internal height (A) was 4.29 mm and isthmus height (B) was 4.76 mm (<5 mm). (D). Preoperative CT showed right-sided HRVA, and the vertebral artery obviously deviated inward and upward (arrow). (E). Postoperative CT scan showed that screw perforated the wall of the pedicle less 2 mm and achieved a grade 1 rating A 54-year-old male patient was preoperatively diagnosed with odontoid process fracture. C2PS placement was assisted by O-S8 during operation. (A). Preoperative CT reconstruction showed odontoid process fracture. (B & C). Isthmus height (B) was 4.16 mm (<5 mm), the patient had a left-sided HRVA, and the vertebral artery obviously deviated inward and upward (arrow). (D & E). Postoperative CT scan showed that screw perforated the wall of the pedicle less 2 mm and achieved a grade 1 rating A 56-year-old female patient was preoperatively diagnosed with free odontoid fragment combined with atlantoaxial dislocation. C2PS placement via FT during operation. (A). Preoperative CT reconstruction showed free odontoid fragment combined with atlantoaxial dislocation. (B & C). Isthmus height was 4.05 mm (<5 mm) Comparison of Accuracy of C2 Pedicle Screws Among the Three Groups A: 3D-PNT group; B: O-S8 group; C: FT group.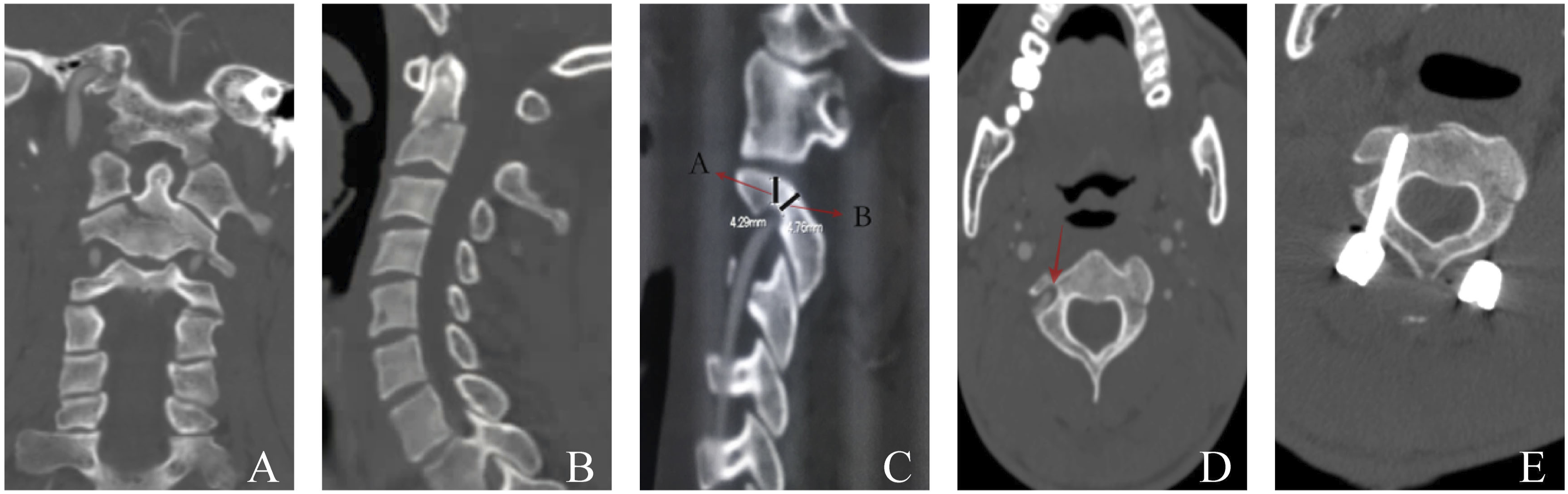

Clinical Outcomes
Comparison of Perioperative Data Among the Three Groups
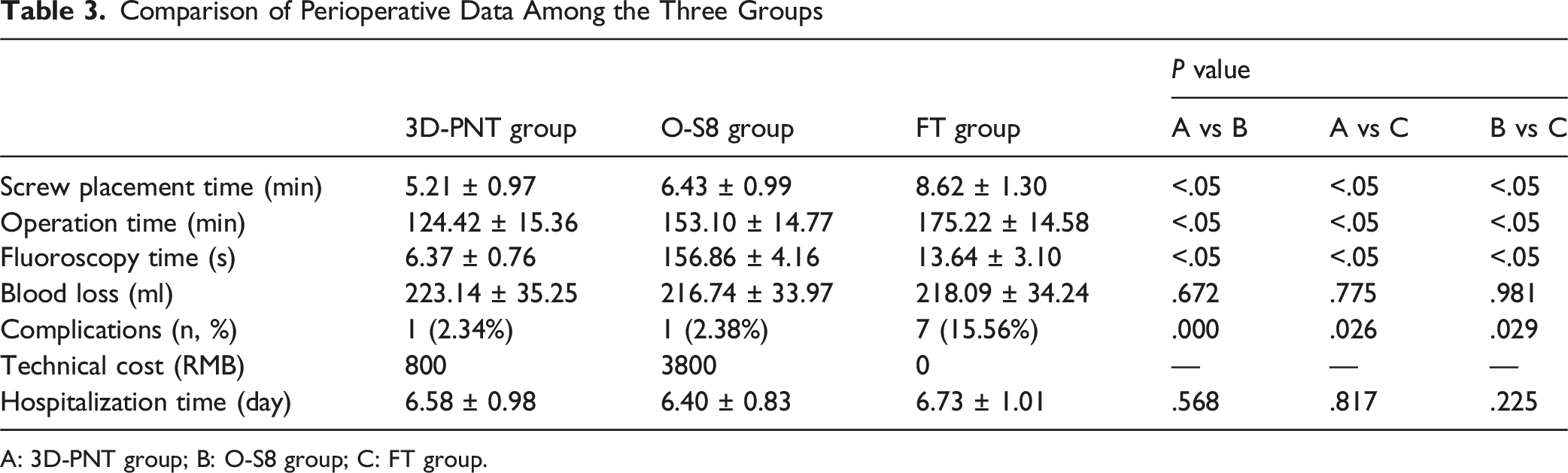
A: 3D-PNT group; B: O-S8 group; C: FT group.
Comparison of the VAS and JOA Scores Among the Three Groups
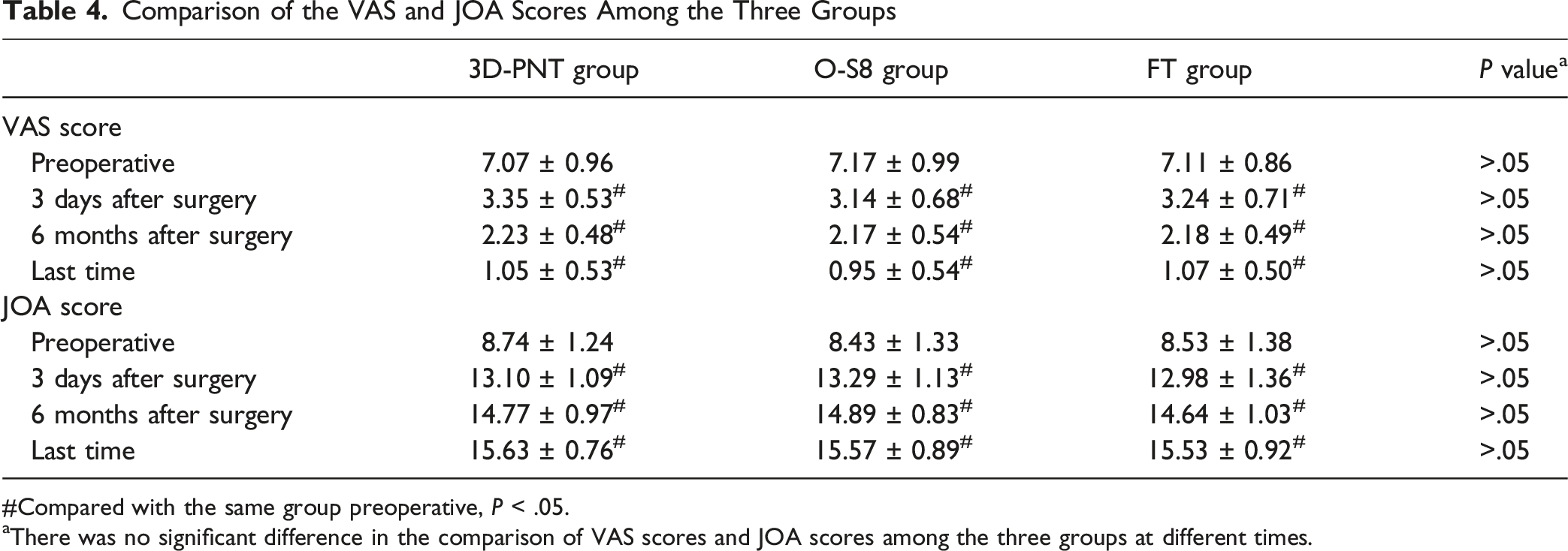
#Compared with the same group preoperative, P < .05.
aThere was no significant difference in the comparison of VAS scores and JOA scores among the three groups at different times.
Discussion
In 1994, Goel and Laheri first introduced the C2PS technique for treating atlantoaxial dislocation. 15 With advancements in spine surgery, C2PS placement has become widely utilized in upper cervical procedures due to its favorable biomechanical properties and satisfactory clinical outcomes. The conventional entry point for C2PS placement is located at the midpoint between the superior and inferior articular processes of C2, with a head inclination of 20°-25° and an inward inclination of 15°-30°. 15 However, in patients with HRVAs, the entry point and angle for C2PS placement are altered due to variations in the vertebral artery. Lee et al 16 classified the intra-axial vertebral artery (IAVA) into nine types, with HRVA encompassing C-2 and certain B-2 types. They proposed that in HRVA, the entry point for C2PS placement should be more laterally on the C2 lateral mass, with increased internal and head inclinations. Our findings indicate that, compared to conventional screw placement, C2PS insertion using the FT presents increased difficulty and risk in patients with HRVAs. Consequently, a more reliable method is needed to enhance the accuracy of C2PS placement. Recent developments in digital orthopedic technologies, such as 3D-PNT and navigation systems, have shown significant promise in improving the precision of complex upper cervical surgeries. However, it remains unclear whether these technologies offer superior accuracy and safety compared to the FT for C2PS placement in HRVA patients.
This study evaluated the accuracy and safety of 3D-PNT, O-S8, and FT-assisted C2PS placement in patients with HRVAs. Our results indicated that the accuracy of screw placement in the FT group was 70.2%. However, two previous studies9,17 reported C2PS placement accuracies of 82.7% and 85% via the FT in patients with normal anatomy, which were notably higher than our findings. This discrepancy likely reflects the increased anatomical complexity in HRVA cases, where conventional landmarks are altered, and the safe margin for screw placement is significantly reduced. As a result, even experienced spinal surgeons face a considerable increase in difficulty due to the variations in vascular anatomy. The accuracy of screw placement in the 3D-PNT and O-S8 groups was significantly higher than that in the FT group. One advantage of O-S8 is its ability to provide real-time navigation during surgery, while 3D imaging helps guide the selection of the optimal screw entry point and trajectory, effectively avoiding the vertebral artery. Previous studies18,19 reported navigation-assisted C2PS placement accuracies of 95.24% and 100%, respectively, highlighting the reliability and precision of navigation systems in the anatomically complex upper cervical region. In this study, the accuracy in the navigation-assisted groups was 90.38%, which is slightly lower than that in previous studies. This difference may be attributed to variations in the study population and clinical settings, as most prior studies included patients with normal or mixed cervical anatomy, whereas our cohort exclusively consisted of HRVA patients with C2PS placement. Nonetheless, the screw placement accuracy in the O-S8 navigation group remained high at 90.38%, which, although somewhat lower than previous reports, was still significantly superior to the FT technique. These results suggest that navigation-assisted techniques maintain a consistently high level of screw placement accuracy even in the challenging anatomical conditions of HRVA. Interestingly, Hur et al 20 noted that factors such as changes in the C2 relative position, reference frame shifts, and navigation matching errors could reduce navigation accuracy. Given the greater mobility of the atlantoaxial region, our approach focuses on ensuring the stability of both the atlantoaxial segment and the reference frame during surgery to enhance navigation accuracy.
The 3D-PNT technique, based on a reverse design of the C2 anatomy, provides two guide holes that facilitate the selection of the optimal screw entry point and direction. Notably, 3D-PNT is not constrained by vascular variations, allowing for precise screw placement under the guidance of these guide holes. Al-Saadawi et al 21 reported accuracy rates ranging from 95.7% to 100% for upper cervical pedicle screw placement assisted by patient-specific 3D-printed drill guides. Their findings highlighted the significant improvement in screw placement accuracy these guides offer, demonstrating reliability even in cases of severe C2 vertebral deformity. A systematic review and meta-analysis by Azimi et al 22 analyzed 13 studies involving 1323 pedicle screws and found an overall accuracy rate of 97.3% for cervical pedicle screw placement assisted by 3D-PNT. The authors emphasized that the main advantage of guide templates lies in their ability to ensure highly accurate screw placement without increasing operative time or procedural complexity, making them particularly beneficial for patients with severe cervical spinal deformities. The accuracy observed in our study was 92.59%, slightly lower than that reported in previous studies. This difference can be attributed to factors similar to those affecting navigation-assisted techniques, such as patient selection and anatomical complexity. Additionally, the C2PS placements in our study were technically more challenging than screws placed at other cervical levels in earlier reports. Despite these challenges, the 92.59% accuracy achieved with 3D-PNT remains high and is consistent with the lower range of values reported in the literature. These findings suggest that 3D-printed templates can reliably maintain screw placement accuracy even in high-risk anatomical conditions. More importantly, 3D-PNT corresponds to a single vertebral body, allowing for precise matching with the posterior structure of C2. The templates are closely attached to the bone, preventing inaccuracies due to changes in the patient’s position or atlantoaxial alignment. 23 To ensure precise adhesion during surgery and to prevent screw trajectory deviation, our approach involves simulating screw placement using the 3D-PNT and a 3D model of C2 before the operation. The surgical plan includes determining the exposure range, ensuring that the soft tissue covering the bone surface is thoroughly removed during surgery for optimal fit. Additionally, the 3D-PNT is stabilized by an assistant during screw placement. Notably, the 3D-PNT only controls the “entry point” and “direction,” and the drilling process within the bone is “blind,” meaning there is no monitoring of cortical breach. Therefore, a probe must be used for exploration before screw insertion to avoid damaging the cortex.
In this study, 7 cases in the FT group (7 of 45, 15.6%), 1 case in the 3D-PNT group (1 of 43, 2.3%), and 1 case in the O-S8 group (1 of 42, 2.4%) experienced vertebral artery injury. All 9 cases of vertebral artery injury were attributed to inaccurate screw trajectories. Traditional screw placement primarily relies on normal anatomical landmarks and the clinical experience of the surgeon. However, in patients with HRVAs, the variation in blood vessel anatomy leads to significant inward and upward deviation of the vertebral artery as it passes through the C2 transverse foramen. This deviation occupies part of the isthmus bone, reducing the thickness or internal height of the isthmus. As a result, the anatomical variation in C2 alters the conventional screw entry point and angle, and in some HRVA patients, there may be only one optimal screw path. Any intraoperative adjustment to the screw path increases the difficulty of screw placement and significantly raises the risk of cortical breach. For HRVA patients, C2PS placement via FT not only demands higher skill from the surgeon but also considerably increases the risk of vertebral artery injury due to these anatomical variations.4,24 In contrast, 3D-PNT and O-S8 can mitigate the shortcomings of FT-assisted placement. By planning the optimal screw entry point and angle before the procedure, both techniques substantially improve the accuracy and safety of C2PS placement. The advantages of O-S8 and 3D-PNT are particularly evident in HRVA patients with combined pedicle stenosis. Even in cases where the pedicle width is smaller than the screw diameter, C2PS placement can still be safely achieved with minimal cortical breach, thanks to precise preoperative assessment and assistance from O-S8 or 3D-PNT. Thus, the primary focus of this study was to compare the effectiveness of different assisted techniques in reducing the incidence of true screw malposition.
The VAS and JOA scores in all three groups significantly improved compared to preoperative values, with no significant differences observed between the groups, indicating satisfactory postoperative clinical outcomes. In the O-S8 group, intraoperative O-arm scanning, image transmission, and system registration were required. During screw placement, continuous adjustments to the navigation probe were necessary to achieve the optimal screw entry point and direction. If there was any relative movement of the reference frame or patient position, re-registration was needed, resulting in longer screw placement, operation, and fluoroscopy times. The longer operative time in the FT group was primarily due to repeated probing and intraoperative verification, including multiple fluoroscopic checks, to ensure screw placement accuracy and safety. In contrast, 3D-PNT typically requires only two fluoroscopic exposures—preoperative and postoperative—with the guide hole assisting in screw placement, making the procedure more straightforward. As a result, the 3D-PNT group demonstrated significantly shorter screw placement time, operation time, and fluoroscopy time compared to both the O-S8 and FT groups. Previous studies have also confirmed that 3D-PNT-assisted screw placement can substantially reduce both operation time and radiation exposure for patients and operators.11,13,25 Notably, the fluoroscopy time reported in this study reflects the actual intraoperative imaging workflow associated with each guidance technique. The observed differences in fluoroscopy time primarily result from variations in imaging workflows and technical characteristics and should be interpreted accordingly. The cost of the C2 3D-PNT device used in this study was approximately 800 RMB per piece, while the cost of using the navigation system was around 3800 RMB per case. The cost analysis focused on the direct additional technical and material fees incurred by each patient during surgery. Specifically, the navigation cost includes expenses for intraoperative use of the O-arm–based S8 navigation system, such as equipment utilization, disposable components, and technical support. The cost of 3D-PNT primarily covers the design of patient-specific templates, 3D printing, and sterilization. The 0 RMB cost in the FT group reflects the absence of additional technical fees. Capital investments, equipment depreciation, maintenance, and other indirect hospital costs were not considered. Therefore, in terms of technology cost, the O-S8 group incurred the highest expenses, while the FT group had the lowest.
Furthermore, during the use of O-S8, it was observed that this technology required complex equipment, a long learning curve, and intricate operation. In contrast, 3D-PNT was easy to use, with minimal requirements for both the surgeon and equipment. It was particularly beneficial in cases with anatomical variations, as it provided excellent assistance in screw placement. However, it is crucial to ensure that the soft tissue covering the bone surface is completely exposed when using the guide plate, allowing the 3D-PNT to securely attach to the C2 and ensuring optimal screw placement accuracy.26,27 A limitation of 3D-PNT is the need for preoperative preparation, as the navigation template must be designed in advance, which may present challenges in emergency situations where surgical planning is not feasible.
Limitations of This Study
This study has several limitations. First, as a retrospective study, patients were not randomly assigned, and treatment decisions were based on clinical practice. Although the baseline characteristics of the enrolled patients were statistically balanced, potential selection bias cannot be completely ruled out. Second, the relatively small sample size prevented further subgroup and regression analyses, as well as the calculation of effect sizes, which may limit the robustness of our findings. Third, all procedures were performed by a single team of two senior spinal surgeons with extensive expertise in upper cervical surgery, who were proficient in all three techniques. However, during the early adoption phase of the new techniques, the potential impact of the learning curve on surgical accuracy and efficiency cannot be entirely excluded. Therefore, large-scale, multi-center, prospective cohort studies are necessary to further validate and confirm our results.
Conclusions
Both 3D-PNT and O-S8 can enhance the accuracy and safety of C2PS placement in patients with HRVAs compared to the FT. These two techniques can thus be widely applied in HRVA cases. However, compared to O-S8, 3D-PNT demonstrated advantages in reducing screw placement and fluoroscopy times. The need for patient-specific customization and preoperative planning with 3D-PNT, however, may limit its immediate applicability in emergency surgeries.
Footnotes
Acknowledgments
We wish to thank all of those who generously agreed to be interviewed for this research. We thank Bullet Edits Limited for the linguistic editing and proofreading of the manuscript.
Ethical Considerations
This study was approved by the institutional internal review board of the leading participating institution (Honghui Hospital, Xi’an Jiaotong University, No.2025-KY-109-01). All procedures performed in studies involving human participants were in accordance with the ethical standards of institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Written informed consent was obtained from all patients included in this study.
Consent to Publication
Written informed consent was obtained from the participants for the publication for the publication of any potentially identifiable images or data included in this article.
Author contributions
YT and SXW conceived and designed this study; YT wrote the manuscript; YT, ST, JBG and SXW collected the data; TJL and LY performed operations. SXW and YT performed the data analysis; YCD and SXW reviewed and revised this manuscript. All authors reviewed the final manuscript. All authors agree to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the NSFC Seed Funding Project of Xi’an Honghui Hospital (Grant No. 2025zz-qn07) and Research Project of Xi’an Municipal Health Commission (Grant No. 2026qn08).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.