
Abstract
Study Design
Retrospective cohort study.
Objective
Spinal metastases are common in patients with breast cancer, and accurate estimation of postoperative survival is crucial for selecting appropriate candidates for metastasis surgery. This study investigated the association between breast cancer subtype, according to the St. Gallen classification, and survival after surgery for spinal metastases with the aim of improving prognostic assessment and supporting informed patient counselling.
Methods
This study included 110 patients with breast cancer who underwent surgery for spinal metastases identified from the Swedish Spine Register and the Swedish National Quality Register of Breast Cancer. Patients were categorized in terms of the breast cancer subtype according to the St. Gallen classification. Postoperative survival was analysed using Kaplan–Meier estimates and a Cox proportional hazards model.
Results
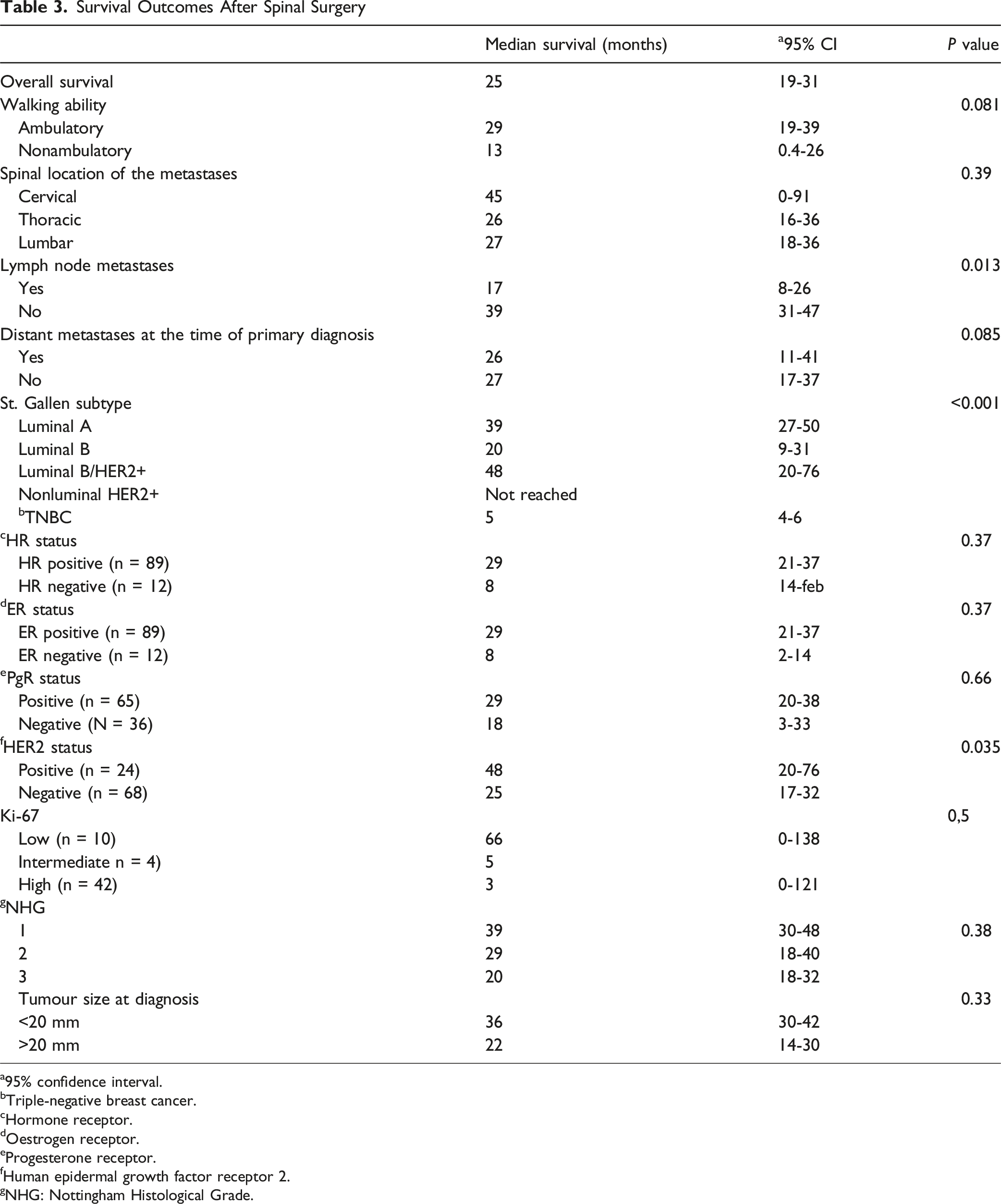
: The overall median survival following spinal surgery was 25 months (95% CI 19–31), while the median postoperative survival by subtype was 39 months (95% CI 28–50) for luminal A patients, 20 months (95% CI 9–31) for luminal B patients, and 48 months (95% CI 20–76) for luminal B/HER2+ patients. The median survival was not reached for the nonluminal HER2+ group, whereas patients with triple-negative breast cancer had a median survival of only 5 months (95% CI 4–6). The St. Gallen subtype was significantly associated with postoperative survival according to univariable (P<0.001) and multivariable analyses (P = 0.011).
Conclusions
Breast cancer subtype according to the St. Gallen classification was significantly associated with survival after surgery for spinal metastases. These findings indicate that the St. Gallen classification may serve as a valuable prognostic tool in the metastatic spine setting. Incorporation of molecular subtype information may improve estimation of postoperative survival and support informed patient counselling, expectation management, and individualized surgical decision-making in patients with breast cancer spinal metastases.
Introduction
Breast cancer is the most common malignancy among women; in 2022, the WHO reported 2.3 million new cases of and 670 000 deaths from breast cancer worldwide 1 Survival outcomes depend on various factors, including age, comorbidities, cancer molecular subtype and disease stage at diagnosis2-4.The bone is the most common site for distant metastasis in patients with breast cancer, with the spine being the most commonly affected location. Spinal metastases pose risks of pathological fracture and metastatic spinal cord compression (MSCC) 4 ; approximately 5-10% of all cancer patients develop MSCC, with breast cancer accounting for approximately 20% of these cases.5-7 Surgery is generally recommended for patients with spinal metastases and a life expectancy of more than 3-6 months. 8
The St. Gallen classification is widely used to categorise patients according to breast cancer subtype and was initially developed to distinguish luminal A-like from luminal B-like breast cancer. The classification has been validated in clinical practice, as the subgroups exhibit different levels of aggressiveness, treatment responses, recurrence patterns and survival rates.2,3,9 Several studies have reported differing survival rates among breast cancer subtypes with bone or spinal metastasis,7,10-12 but few have specifically investigated survival outcomes after surgery for patients with spinal metastases on the basis of the St. Gallen classification.
This study aimed to evaluate survival after spinal surgery in breast cancer patients with spinal metastases. Particular focus was placed on the association between survival and breast cancer subtype according to the St. Gallen classification, and on the potential value of this classification for prognostic evaluation and informed patient counselling.
Methods and Materials
Study Design, Data Sources, and Setting
This observational register-based cohort study involved data obtained from the Swedish Spine Register (Swespine) and the Swedish National Quality Register for Breast Cancer (NKBC). The study included all patients registered in Swespine who had undergone surgery for spinal metastases due to breast cancer between 2011 and 2023, including those with unknown primary tumours at the time of spinal surgery for whom PAD confirmed a diagnosis of breast cancer. These records were then cross matched with those of the NKBC. For patients who underwent multiple surgeries, only the first spinal surgery was considered for the subsequent analyses.
Three patients who initially underwent surgery for an unknown primary tumour and were diagnosed with breast cancer years after spinal surgery were excluded, as their spinal surgery could not be definitively linked to breast cancer metastases. Additionally, 4 patients with an uncertain primary tumour diagnosis following spinal surgery were excluded (Figure 1). Flow chart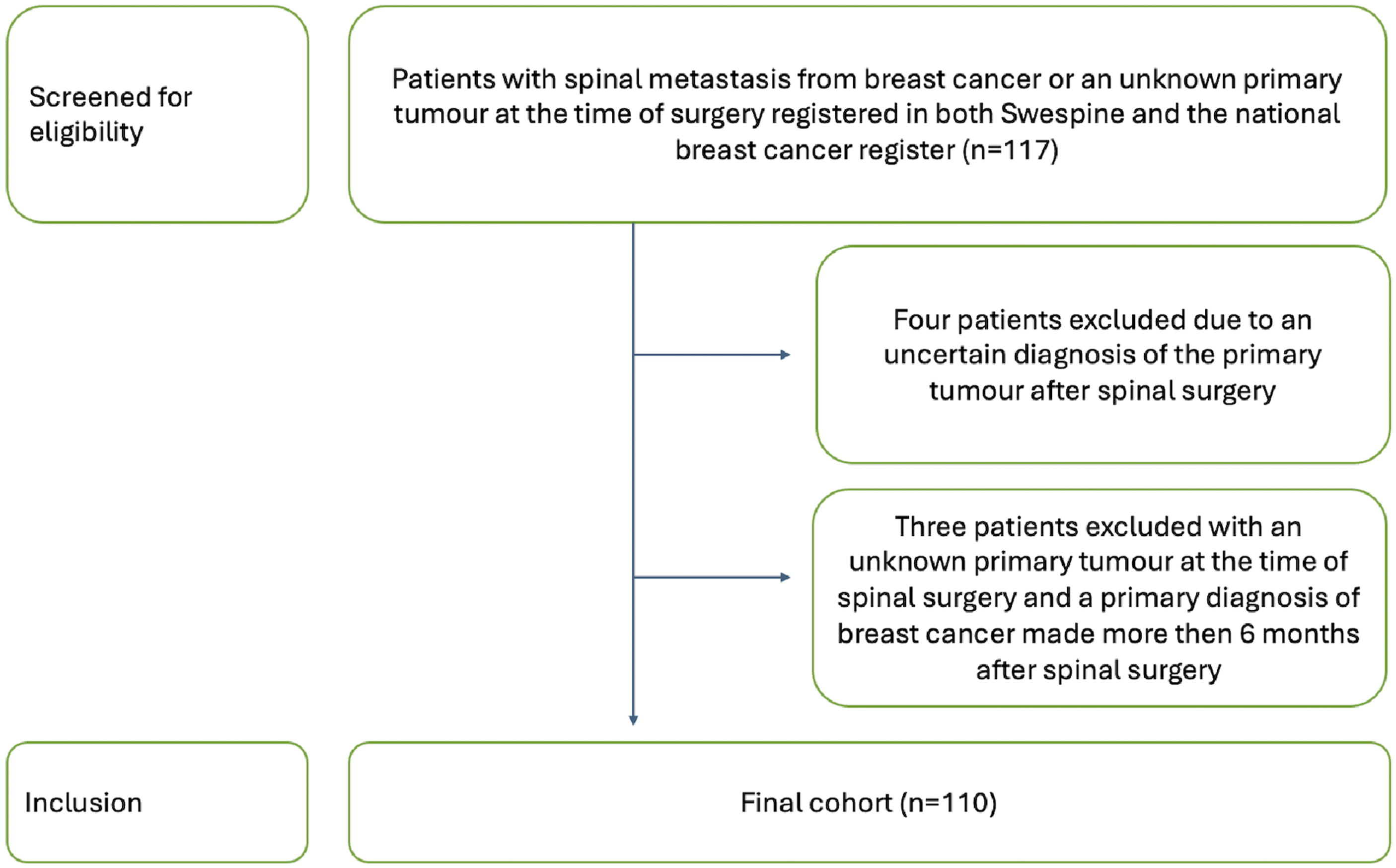
The NKBC, established in 2008, contains comprehensive data on the breast cancer diagnosis, tumour classification, TNM stage, preoperative oncological treatment, surgical interventions, postoperative oncological treatment, and survival of breast cancer patients. The register has a reported coverage of 99.9%. 13
Swespine has documented spinal surgery data since 1993 and began including those of patients with spinal metastases in 2006. Currently, approximately 90% of all spinal surgery units in Sweden contribute data to Swespine, including all tumour surgery units. The estimated completeness of the data is 75%. 14 Swespine collects information on the primary tumour type, spinal surgery procedures and approaches, neurological function as assessed by the Frankel score, localization of metastases, complications, and date of death. A follow-up survey is conducted 6 weeks after the operation, including the patient-reported five-dimension (mobility, self-care, usual activities, pain/discomfort, and anxiety/depression) quality of life questionnaire EQ-5D. 15
Outcome Variables
From the Swespine register, data were collected on age at the time of spinal surgery, date of surgery, type of surgical approach and method, location of the spinal metastases, and preoperative neurological function as assessed using the Frankel scale. Patients were further categorized as nonambulatory (Frankel Grade A-C) or ambulatory (Frankel Grade D-E). Responses to the EQ-5D were retrieved at the time of surgery and at 6 weeks postoperatively.
Data including age and TNM stage at diagnosis, were obtained from the primary breast cancer patients included in the NKBC. In addition, we retrieved NKBC data on immunohistological characteristics, including the Nottingham histologic grade (NHG) and the expression of oestrogen receptor (ER), progesterone receptor (PgR), human epidermal growth factor receptor 2 (HER2) and Ki-67. Specifically, these variables were evaluated as positive/negative for ER and PgR and as low/intermediate/high for Ki-67. If a formal assessment was unavailable but a percentage was recorded, established cutoffs were applied; specifically, ER positivity (ER+) was defined as ≥ 10%, PgR + as ≥ 10%, and low, intermediate, and high Ki-67 as <14%, 14-19%, and ≥20%, respectively.9,16,17 Data on the pathological assessment of the entire tumour post breast surgery was prioritized; if these data were missing, the results from preoperative diagnostic needle biopsy were retrieved. On the basis of the abovementioned immunohistological markers, the breast cancer patients were classified into subgroups according to the St. Gallen subtype (Supplemental Table 1). 3
Statistical Analysis
Nominal variables are presented as frequencies and proportions, whereas continuous variables are reported as the means with standard deviations (SDs) and/or the medians with interquartile ranges (IQRs). Median postoperative survival was estimated using the Kaplan‒Meier method with the 95% confidence interval (CI), and survival outcomes were compared with the log-rank test. Normally distributed continuous variables were analysed using Student’s t test, and categorical variables were analysed using the chi-square test. Adjusted hazard ratios (HRs) with corresponding 95% CIs were calculated using a Cox regression model, with ambulation, age at surgery, St. Gallen subtype, spinal location and lymph node status at primary diagnosis as covariates. A P value <0.05 was considered to indicate statistical significance. Analyses were performed using IBM SPSS Statistics Version 29.
Results
Patient Characteristics at the Time of the Primary Diagnosis of Breast Cancer
The final cohort consisted of 110 patients (Figure 1) with a mean age of 57 (SD 13) years at the time of primary tumour diagnosis. At the time of the primary diagnosis, 47 patients had lymph node metastases, and 36 had distant metastases. On the basis of the St. Gallen classification, the breast cancer subtypes of the patients were identified as follows: luminal A, 18 patients; luminal B, 36 patients; luminal HER2-positive, 19 patients; nonluminal HER2-positive, 5 patients; and triple-negative breast cancer (TNBC), 5 patients. Twenty-seven patients did not have sufficient data for classification. Among the 5 patients classified as having TNBC, 2 had a HER2-, ER-, and PgR + status. A previous study suggested that patients with this “single PgR+” subtype have similarly poor outcomes to those who have a HER2-, ER- and PgR-status, which may be due to the ineffectiveness of hormonal and anti-HER2 therapies. 18 Therefore, these 2 patients were included in the TNBC subgroup. The histological grade according to the Nottingham grading system was available for 86 patients: NHG1, 10 patients; NHG2, 39 patients; and NHG3, 37 patients. These data were missing for 24 patients.
Clinical Characteristics at the Time of Primary Diagnosis of Breast Cancer
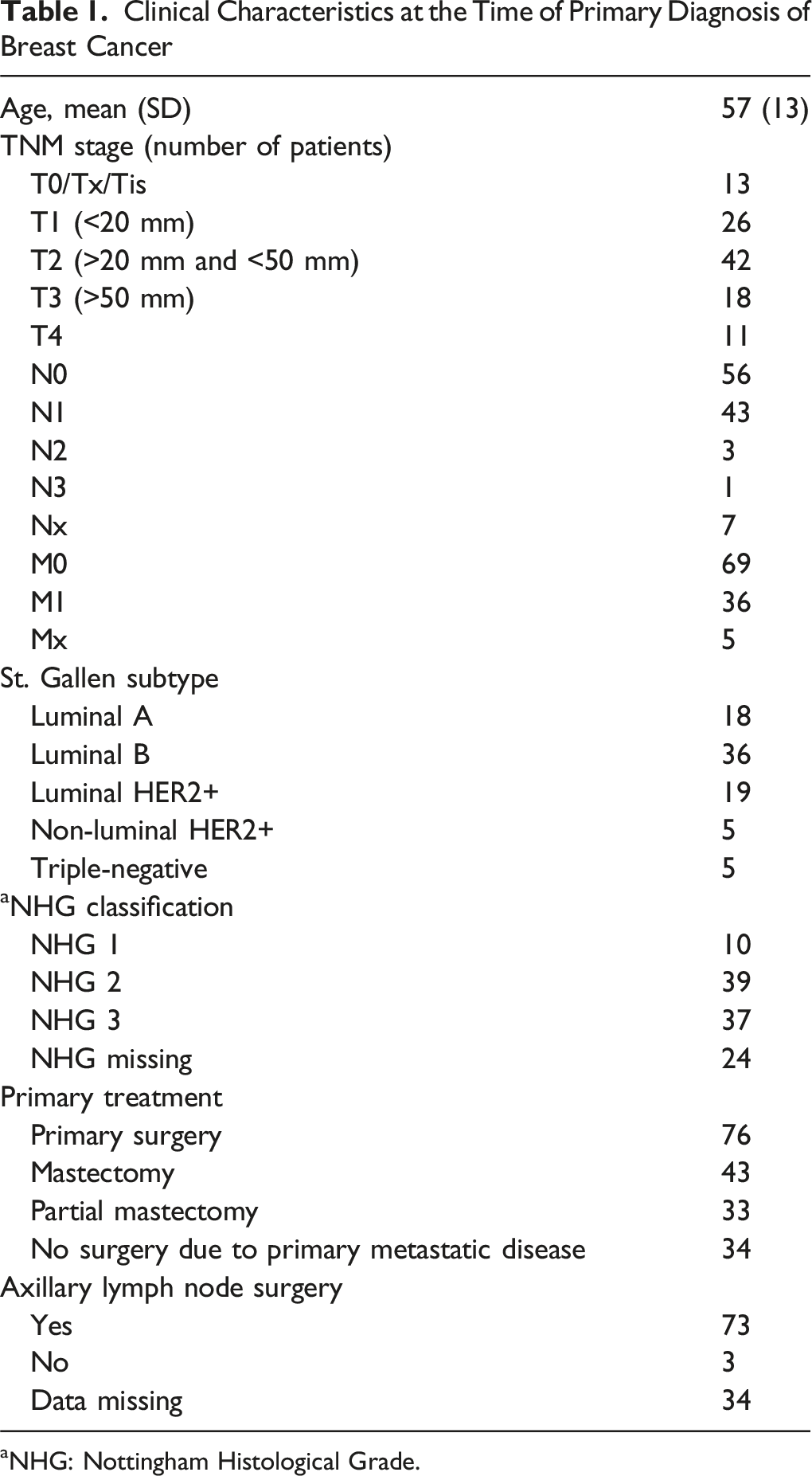
aNHG: Nottingham Histological Grade.
Spinal Surgery
Clinical Characteristics at the Time of Surgery for Spinal Metastases
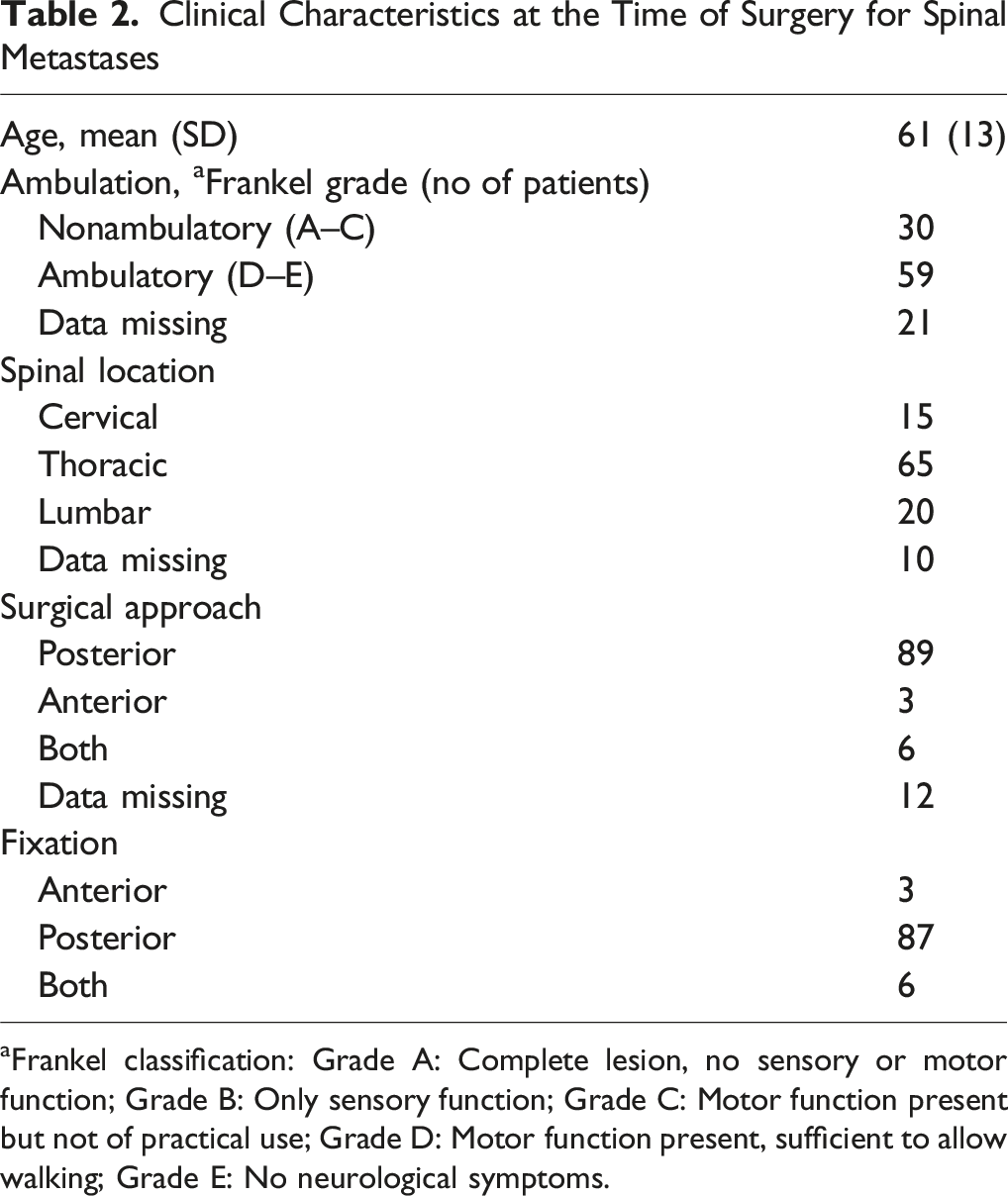
aFrankel classification: Grade A: Complete lesion, no sensory or motor function; Grade B: Only sensory function; Grade C: Motor function present but not of practical use; Grade D: Motor function present, sufficient to allow walking; Grade E: No neurological symptoms.
Posterior decompression and fusion were performed for 87 patients, anterior decompression and fusion were performed for 3 patients, and a combination of anterior and posterior stabilization was performed for 6 patients. Decompression alone was performed for 10 patients, and data on the type of surgery was missing for 4 patients.
Survival After Surgery
Survival Outcomes After Spinal Surgery
a95% confidence interval.
bTriple-negative breast cancer.
cHormone receptor.
dOestrogen receptor.
eProgesterone receptor.
fHuman epidermal growth factor receptor 2.
gNHG: Nottingham Histological Grade.
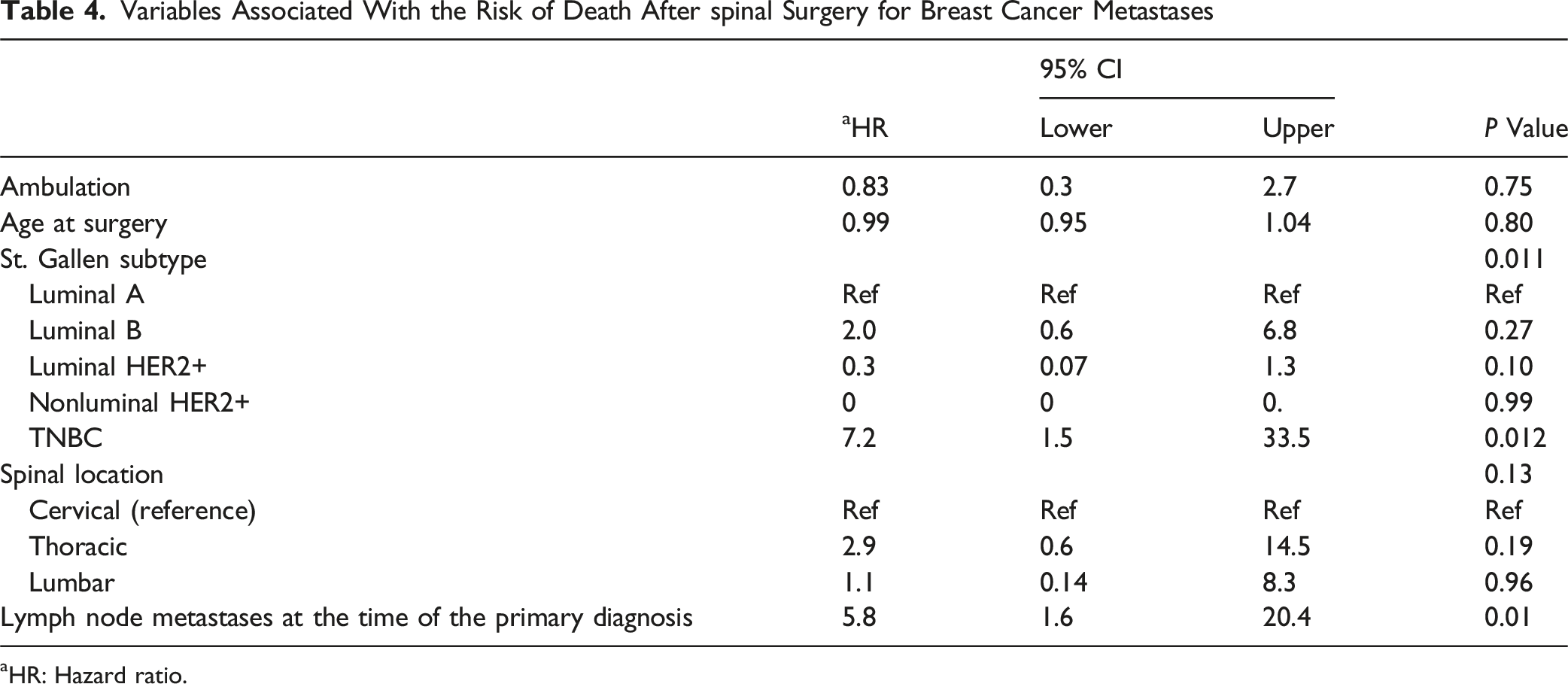
Survival outcomes differed by the St. Gallen subtype: patients with the luminal HER2 + subtype had the longest median survival, 48 months (95% CI: 20-76), whereas those with TNBC had the shortest median survival, 5 months (95% CI: 4-6). Luminal A patients had a median survival of 39 months (95% CI: 28-50), and luminal B patients had a median survival of 20 months (95% CI: 9-31). However, the median survival was not reached for the nonluminal HER2 + subtype, as fewer than 50% of patients in this group died (Figure 2). The St. Gallen subtype was significantly associated with postoperative survival in the univariable analysis (P < 0.001) (Table 3). In the subsequent multivariable analysis, both the presence of lymph node metastases at the primary diagnosis (P = 0.01) and the St. Gallen classification (P = 0.011) were significantly associated with post-spinal surgery survival (Table 4). Survival after spinal for patients with different subtypes of breast cancer according to the St. Gallen classification Variables Associated With the Risk of Death After spinal Surgery for Breast Cancer Metastases aHR: Hazard ratio.
Quality of Life
Estimates of Quality of Life at the Time of Spinal Surgery and 6 Weeks Postoperatively as Measured With the Patient-Reported EQ-5D
Discussion
We found that survival after surgery for patients with spinal metastases from breast cancer was significantly associated with the cancer subtype according to the St. Gallen classification.
Determining the optimal treatment strategy for breast cancer patients with spinal metastasis is a complex process that requires a multidisciplinary approach, and surgical decisions need to be individualized on the basis of the patient’s specific risk and potential benefits from surgery. A crucial part of this decision-making process is the prediction of life expectancy, which, according to our findings, should involve the consideration of the molecular subtype of breast cancer. This consideration has been previously suggested by Tan et al (2018), but validation in larger cohorts has been lacking. 19 The molecular subtype significantly impacts disease progression, including survival outcomes after spinal surgery. This finding supports prior criticisms of existing treatment strategies by Tan et al and Zhou et al, who highlighted the limitations of the most widely used Tomita and Tokuhashi scoring systems for predicting postoperative survival, which lack these nuances and do not incorporate molecular distinctions.12,19,20
The main findings of this study indicate that survival after spinal surgery differs among the St. Gallen subtypes, with patients with the HER2 + subtype showing the best outcomes and those with TNBC showing the poorest outcomes. Previous studies have reported that patients with any of the luminal subtypes generally exhibit longer survival than those with the TNBC subtype, likely because of the better responsiveness to adjuvant endocrine therapy, higher radio- and chemosensitivity, and less aggressive nature of the tumours.2,10 Furthermore, consistent with our results, an association between TNBC and poor outcomes has previously been reported.2,10,19
Few studies have specifically analysed the association between breast cancer subtype and postoperative survival after spinal surgery. A retrospective study by Zhao et al, 12 which categorized 58 surgically treated patients with breast cancer spinal metastases according to the St. Gallen subtype, revealed that patients with the luminal A subtype had the longest overall survival from primary tumour diagnosis, but the association between survival after spinal surgery and the St. Gallen classification was not presented. Similar, breast cancer subtypes were associated with overall survival for patients with spinal metastases in a national cohort by Amelot et al. 21 Wang et al. 22 reported significant survival differences among breast cancer subtypes after spinal metastasis surgery in a retrospective cohort of 151 patients, with ER-negative, hormone receptor-negative and TNBC patients exhibiting the shortest survival times. Molecular subtypes were significantly associated with postoperative survival for spinal metastases in a retrospective study of 98 patients by Duvall et al. 23 In a review, Qiao et al assessed prognostic factors for survival in breast cancer patients with spinal metastases and concluded that the ER status and HR status (ER and PgR status combined) were key prognostic factors for survival in both surgically treated patients and those who received radiotherapy alone. 24 This finding is consistent with our results, as the TNBC subtype was associated with the shortest survival. However, the luminal subtypes exhibited varying survival outcomes, ranging from 20 to 48 months in our study.
Previous studies have not distinguished between the different ER + subtypes, despite relevant modifications of the St. Gallen classification over the years to further differentiate these subtypes. These updates include the addition of the NGH classification for histological grading and inclusion of the Ki-67 proliferation marker, 8 which reflect differences in treatment response and aggressiveness.2,21 Compared with the luminal B subtype, the luminal A subtype is generally considered less aggressive and is characterized by a lower histological grade and proliferation rate; thus, distinct treatment approaches are needed between the two luminal subtypes.2,9,25,26,27 Our findings support this assumption, demonstrating that patients with the luminal B subtype had shorter survival than those with either the luminal A or the luminal HER2 + subtypes, despite HER2 being an oncogene. However, this may be explained by access to effective HER2-targeted therapies.3,26
Previous studies have suggested that the location of the spinal metastasis may influence survival after surgery,10,28 whereas other studies have not reported such an association.29,30 In the present study, we found no significant relationship between spinal location and postoperative survival. Similarly, an association between preoperative ambulation status and postoperative survival, previously reported in earlier studies6,22,24 was not supported by our study.
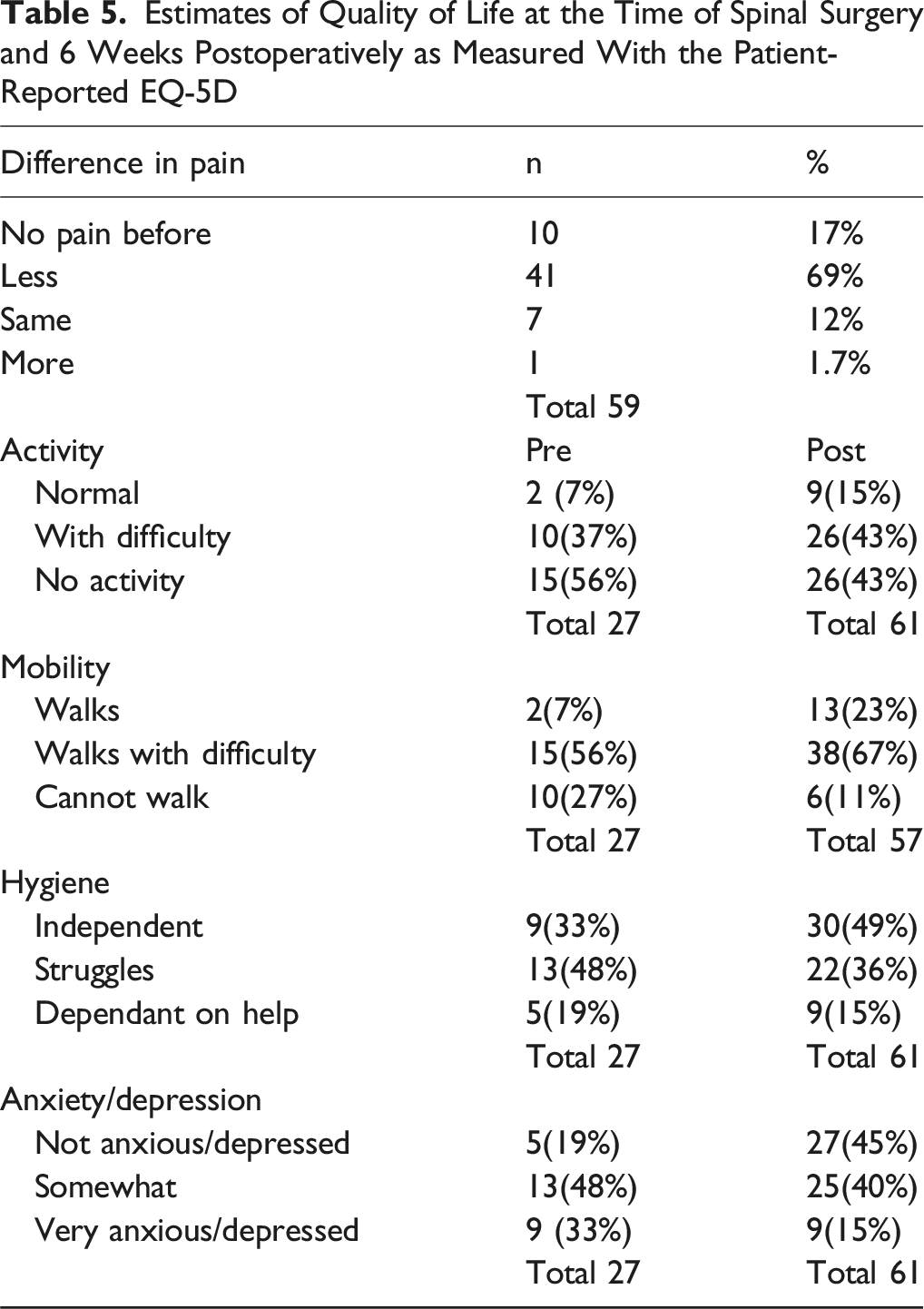
Quality of life was assessed using the EQ-5D at baseline and 6 weeks after spinal surgery. However, data were missing for nearly half of the patients; since surgery for spinal metastases is typically palliative and often performed under urgent conditions in severely ill patients, follow-up is challenging. These factors likely contributed to the low response rates, which were 22% preoperatively and 55% postoperatively.
Among the available data, there was a trend toward improved quality of life following surgery, with the majority of patients reporting reduced pain. Although surgical intervention is frequently palliative, few studies have specifically addressed quality of life outcomes and pain reduction in breast cancer patients undergoing spinal metastasis surgery. Consistent with our findings, Shehadi et al reported that pain levels decreased from a median visual analogue scale (VAS) score of 6 preoperatively to 2 postoperatively. 31 Relatedly, Dea et al recently suggested that, in light of the observed improvements in quality of life, surgery may be justified even for patients with a limited life expectancy. 32
The main strengths of this cohort study are its nationwide representation and the relatively large number of patients. To our knowledge, this is the only study examining the impact of the widely accepted St. Gallen classification system on postoperative survival in breast cancer patients with spinal metastases.
The limitations of this study include potential selection bias, since all included patients had undergone surgery. Additionally, the distribution of patients across the St. Gallen subtypes was uneven, with TNBC being the least represented (five patients). This may indicate either that TNBC does not metastasize to the spine to the same degree as other subtypes of breast cancer do, as reported in previous studies, 31 or that TNBC patients present with more advanced disease at the time of spinal involvement, which is likely given the highly aggressive nature of this subtype. Quality-of-life data were based on patient surveys conducted 6 weeks postoperatively and were incomplete, limiting iterpretability. The retrospective registry-based design limited the availability of disease-specific outcome measures; while EQ-5D was available, validated instruments for metastatic spine disease such as Spine Oncology Study Group Outcomes Questionnaire 2.0 (SOSGOQ2.0) were not.33,34 In addition, data required to calculate established spinal metastasis prognostic scores (eg, Tokuhashi or Tomita) were not consistently recorded, precluding comparison with these classification systems. Collectively, these limitations highlight the need for prospective studies integrating molecular breast cancer subtypes with spinal-specific prognostic tools and disease-specific patient-reported outcomes.
Conclusion
The St. Gallen breast cancer subtypes were associated with survival after surgery for spinal metastases and may enhance prognostic accuracy and support informed counselling and individualized surgical decision-making.
Supplemental Material
Supplemental material - The St. Gallen Classification of Breast Cancer Subtype and Its Association with Survival After Surgery for Spinal Metastases
Supplemental material for The St. Gallen Classification of Breast Cancer Subtype and Its Association with Survival After Surgery for Spinal Metastases by Sara Edman, Jessica Lindberg, Pedram Tabatabaei, Catharina Parai, Olof Westin, Oskar Hemmingsson, Sead Crnalic and Johan Wänman in Global Spine Journal
Footnotes
Acknowledgments
We thank all the physicians who made time to enter information into the Swespine register and the Swedish National Quality Register for Breast Cancer. Methodological support, statistical analysis, and assistance with the conduct of the study were provided by Johan Svensson, Diagnostic and intervention, Umeå University Hospital and the Department of Statistics, Umea School of Business, Economics and Statistics, Umea University Sweden.
Ethical Considerations
This study was approved by the Swedish Ethical Review Authority. Dnr 2023-070809-01.
Authors Contributions
JW and SC developed the initial study concepts. The study was designed by JW, OH, and SC. Data were acquired by JW and JL, while data and algorithm quality control were conducted by JW, SE, and JL. SE and JW were responsible for data analysis and interpretation. Statistical analyses were performed by SE, JW, and JL. The manuscript was prepared by SE, JW, PT, CP, and OW. All authors contributed to editing and reviewing the manuscript and approved the final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors have no relevant financial or non-financial interests to disclose, or conflict of interest. All authors have seen and approved the final version of the manuscript.
Data Availability Statement
These data cannot be shared publicly because the individual-level data contain potentially identifying and sensitive patient information and cannot be published owing to legislation and ethical review restrictions (https://etikprovningsmyndigheten.se). The use of data from national health data registers is further restricted by the Swedish Board of Health and Welfare (https://www.socialstyrelsen.se/en/) and Statistics Sweden (![]() ), which are government agencies providing access to linked healthcare registers.
), which are government agencies providing access to linked healthcare registers.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.