
Abstract
Study Design
Retrospective Cohort Study.
Objectives
To evaluate clinical and patient reported outcomes between operative and non-operative management strategies for sacral U-type fractures.
Methods
This retrospective review included patients with sacral U-type fractures from a 12-year period at a Level 1 trauma center. Demographic, Modified 5-Item Frailty Index (mFI-5), complications, outcomes, and Patient-Reported Outcomes Measurement Information System (PROMIS) data were collected. Fractures were classified by the AO Spine Sacral Injury Classification System (AOSSIC) and analyzed by subtype and treatment modality (trans-sacral screw fixation (TSF) or lumbopelvic fixation (LPF) vs non-operative). Statistical significance was P < .05.
Results
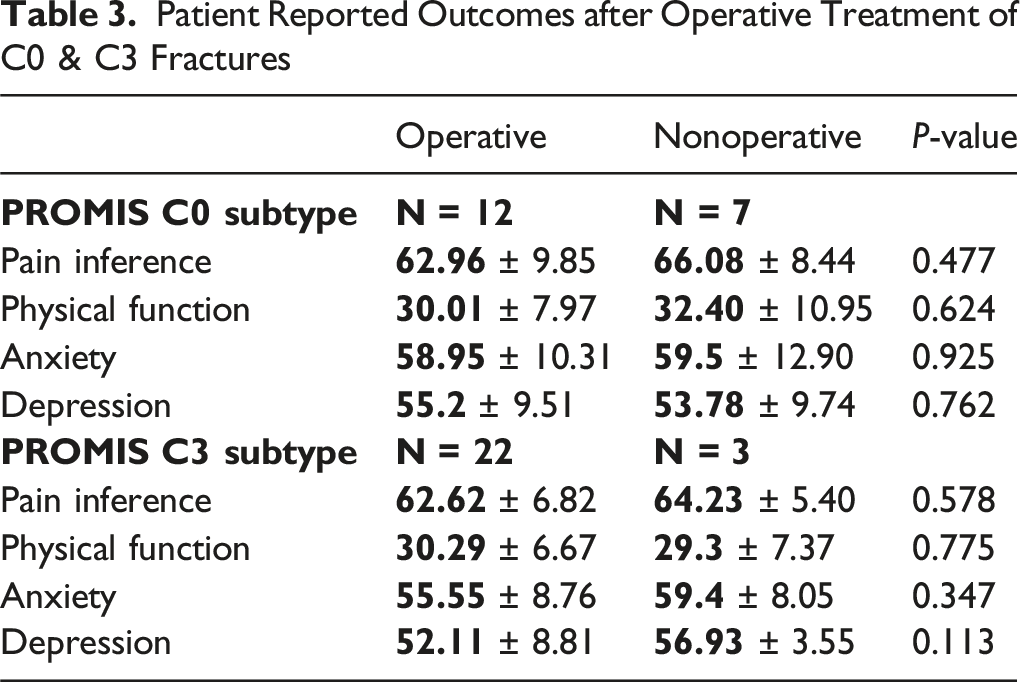
Sixty-five patients met inclusion criteria (mean age 59.7 ± 21.3 years, 49% male). Forty-seven (72%) were treated operatively (10 LPF, 37 TSF) and 18 non-operatively. Among C0 fractures, PROMIS Pain Interference (PI) and Physical Function (PF) scores were similar between operative and non-operative groups (62.96 vs 66.08, P = .48; 30.01 vs 32.40, P = .62). Similar findings were observed for C3 fractures (PI 62.62 vs 64.23, P = .58; PF 30.29 vs 29.3, P = .78). mFI-5 frailty scores were higher among non-operative C3 fracture patients compared to operative cases (2.25 vs 0.90, P < .001). Complication rates were low and comparable between groups. Symptomatic screw removal occurred in 8% of TSF cases.
Conclusions
Operative and non-operative management of AOSSIC Type C sacral fractures yield comparable PROMIS outcomes and complication rates when frailty scores are considered. TSF was associated with higher rates of symptomatic screw removal. Further investigation is needed to determine the optimal treatment and impact of frailty metrics for these injuries.
Introduction
Spinopelvic dissociation (SD) is a term used when the sacral fracture pattern creates discontinuity between the pelvis and the spine. These types of fractures represent a small proportion (approximately 2.9%) of all sacral fractures. 1 Treatment is critical as the sacrum allows for the transfer of axial loads from the upper body to the lower body while ambulating. Operative treatment, in the form of closed reduction and percutaneous trans-sacral screw fixation (TSF) and/or lumbopelvic fixation (LPF), produces generally good results for these injuries.2-5
Controversy exists regarding treatment options when these fractures are minimally displaced or occur in frail, elderly individuals. Historically, nondisplaced fractures were treated with prolonged bed rest, however, this strategy often led to high rates of pneumonia, thrombotic events, and urinary tract infections.6,7 Consequently, treatment has shifted to early mobility and physical therapy, however the risk of fracture displacement, neurologic dysfunction, and significant pain has become a concern. 8 Operative treatment in the form of closed reduction and percutaneous trans-sacral screw fixation is a minimally invasive procedure that has demonstrated good success with low reported complication rates but generally provides less stability when compared to lumbopelvic fixation. 9 Additionally, the ability to perform TSF relies on the presence of safe osseous fixation pathways across the posterior pelvic ring, which are often limited by fracture displacement and deformity. Meanwhile, LPF allows for the most biomechanically stable construct at the cost of higher morbidity and complication risks. 10
Prior studies have not consistently differentiated between displaced and non-displaced U-type fractures as separate entities, making identification of optimal treatment options more difficult. Thus, prior classification systems do not robustly guide management based on well-validated data, which has led to limited clinical applicability. 11 In contrast, the AO Spine Sacral Injury classification (AOSSIC) has excellent intraobserver (ƙ = 0.71) and interobserver reliability (ƙ = 0.75), considering both the biomechanical stability of the fracture and the patients’ neurologic status.12,13
The goal of this study was to add clarity to the treatment of sacral fractures, with a focus on AOSSIC fracture subtypes that represent historically controversial injury pattens. Our primary aim was to compare complication and hospital readmission rates between operative and nonoperative treatment for Type C U-shaped sacral fractures, which can be highly unstable since they are spinopelvic dissociation (SPD) injuries. Both non-displaced and displaced variants were analyzed. Secondarily, we aimed to understand how patient reported outcomes (PROMs) vary between operative and nonoperative management and to better understand which patients would benefit from early mobilization without operative intervention using the modified frailty index and the AOSSIC.
Materials and Methods
After obtaining IRB approval, we retrospectively queried patients who sustained a sacral fracture from August 2011 to August 2023. Patients with sacral fracture patterns resulting in spinopelvic dissociation, regardless of management, were considered for inclusion. Patients without spinopelvic dissociation and patients who were less than 18 years old at the time of injury were excluded. Demographic data including age, sex, concomitant injuries, complications, and Health-Related Quality of Life (HRQL) scores were extracted from the medical records.
Imaging
Upon arrival to the emergency department at our level 1 trauma center, standardized radiographic workup was obtained. Plain radiographs of the pelvis were taken to evaluate for a pelvic ring fracture and to evaluate for the presence of the paradoxical inlet of the upper sacrum on the anteroposterior view of the pelvis. When plain radiography identified a pelvic ring fracture, computed tomography (CT) of the pelvis was obtained and evaluated for the presence of vertical fractures of the bilateral sacral ala on axial imaging and/or transverse fracture of the sacral body on sagittal imaging. Fractures were later triaged by the orthopaedic trauma service based on instability for further treatment.
Treatment Approach
The patients in this study typically underwent surgical stabilization given the theoretical unstable nature of Type C fractures. However, some patients were trialed with non-operative management based on the on-call surgeon’s discretion. Trans-sacral screw fixation was the main form of fixation for all subtypes of C fractures in the absence of neurologic injury, severe comminution, or sacral dysmorphism of the S1 body. The aim was to place two trans-sacral screws if the S1 corridor allowed. In cases where the patient had a fracture pattern that was not amenable to safe placement of trans-sacral screws, concomitant neurologic injury or severe sacral comminution, lumbopelvic fixation was the construct of choice. Lumbopelvic fixation techniques for C0 patients included 1 open (L4-ilium) and 1 percutaneous (L5-ilium) approach, both with freehand screw placement, and the percutaneous case also underwent concomitant TSF placement. There were no cases with S2 alar-iliac (S2AI) screw placement. For C3 patients, the techniques were more varied with four L5-ilium, three L4-ilium, and one L3-ilium construct. Seven underwent open approaches with one minimally invasive approach, the minimally invasive case was also the only to utilize navigation assistance. Five cases utilized S2AI screws to augment the construct, and three cases (including one with S2AI screws) underwent concomitant TSF fixation. Those who underwent nonoperative management were treated with physical therapy and pain management for early mobilization and adequate pain control.
PROMIS Score
The Patient-Reported Outcomes Measurement Information System (PROMIS) scoring system is a standardized tool used to assess a patient’s physical, mental, and social health based on their self-reported experiences. 14 PROMIS uses item banks and short forms to evaluate domains such as pain, fatigue, physical function, depression, and social roles. Scores are reported as T-scores, where 50 represents the average score of the U.S. general population, and each 10-point deviation reflects one standard deviation above or below the mean. Higher T-scores indicate more of the measured domain, which may be positive or negative depending on the domain (e.g., higher scores in pain indicate worse symptoms, while higher scores in physical function suggest better health). The PROMIS score was obtained once within the 90-day global period after the pelvic fracture.
Modified Frailty Index – 5 (mFI-5)
The Modified Frailty Index-5 (mFI-5) is a clinical tool used to assess a patient’s frailty based on five specific health conditions. 15 To calculate the mFI-5, one point is assigned for the presence of each of the following: hypertension requiring medication, diabetes mellitus, congestive heart failure, chronic obstructive pulmonary disease (COPD) or a history of pneumonia, and non-independent functional status, meaning the patient is partially or totally dependent in activities of daily living. The total mFI-5 score ranges from 0 to 5, with higher scores indicating greater frailty and potentially increased risk for adverse outcomes. Patients’ frailty score was calculated from their history and physical examination at time of admission for their sacral injury.
Analysis
Descriptive statistics were used to analyze continuous and categorical variables. Continuous variables were presented as means with ranges and categorical data was presented as numbers and percentages. Continuous differences between groups regarding PROMIS scores (pain inference, physical function anxiety, depression) and mFI-5 were analyzed by using Student’s t-test. An alpha of P < .05 was considered significant. For categorical data, such as complications and readmissions, odds ratio was used to assess the association between the exposure and the outcome. Statistical analysis was performed with the aid of SPSS ver. 18 (Chicago, IL, 2009).
Results
Patient Demographics
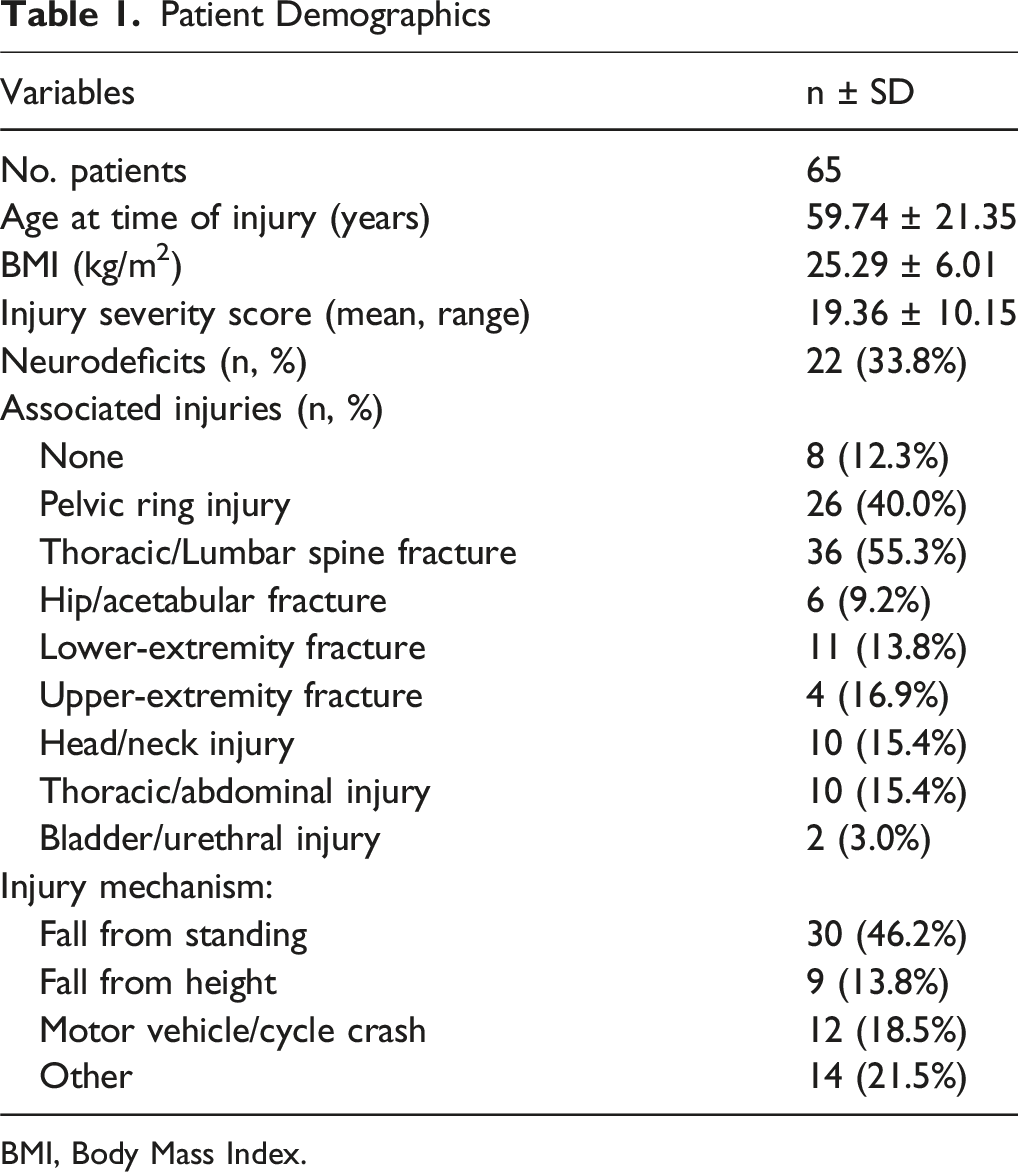
BMI, Body Mass Index.
Fracture Classification, Treatment & Complications
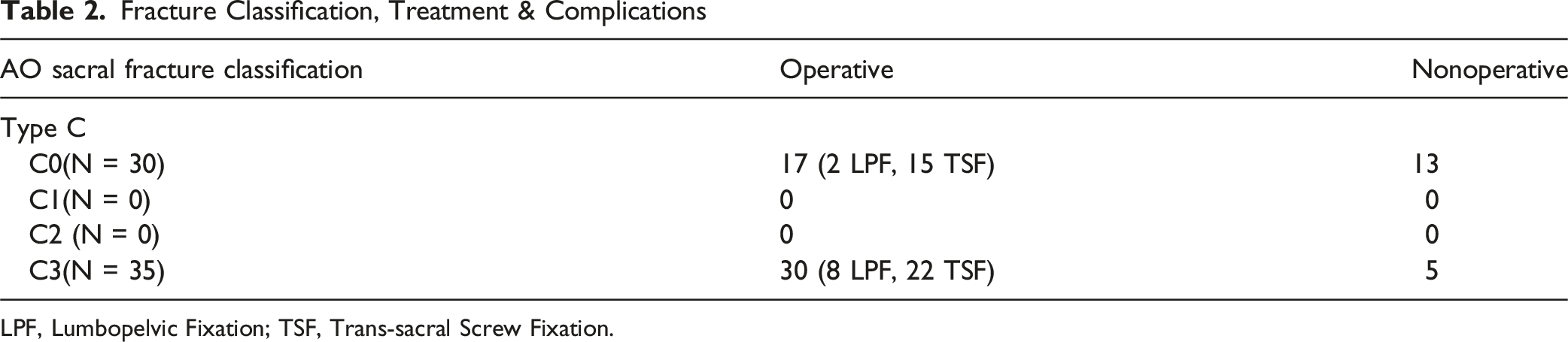
LPF, Lumbopelvic Fixation; TSF, Trans-sacral Screw Fixation.
Patient Reported Outcomes after Operative Treatment of C0 & C3 Fractures
Complications, Readmissions, Primary Treatment Failure
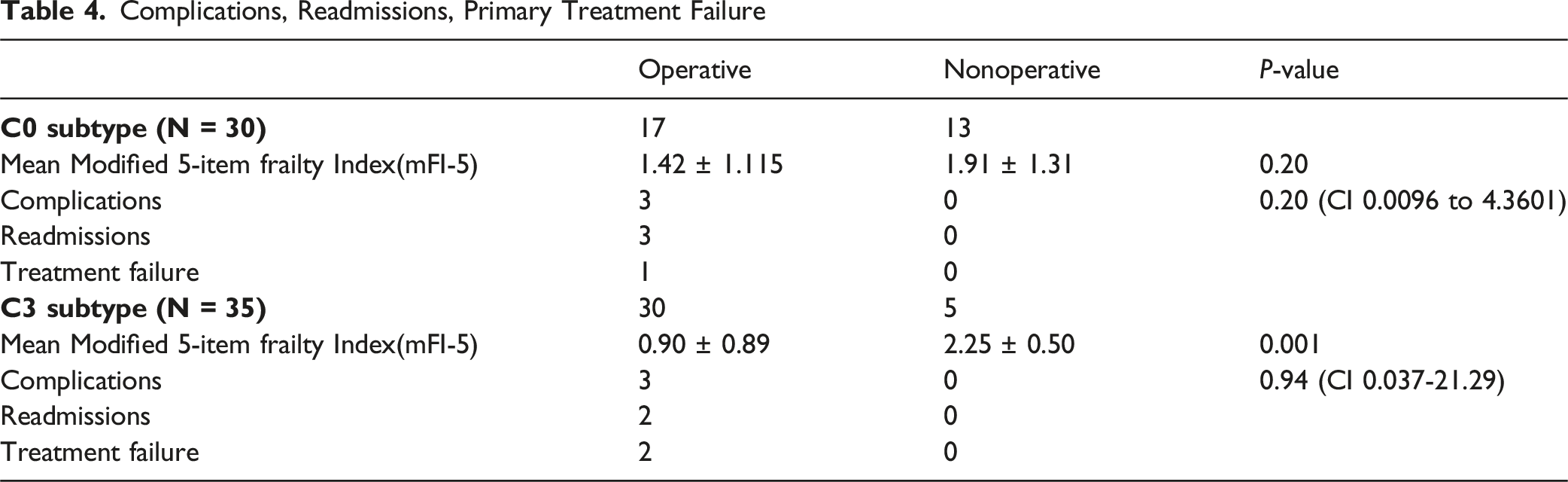
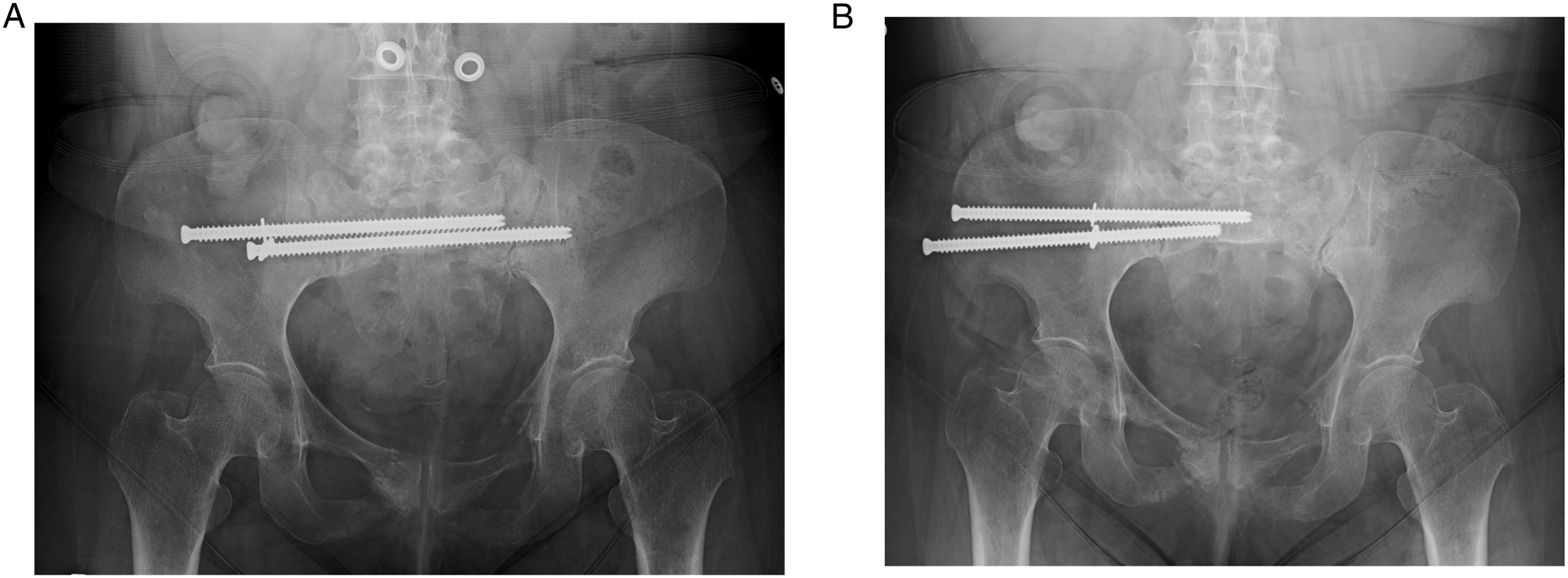
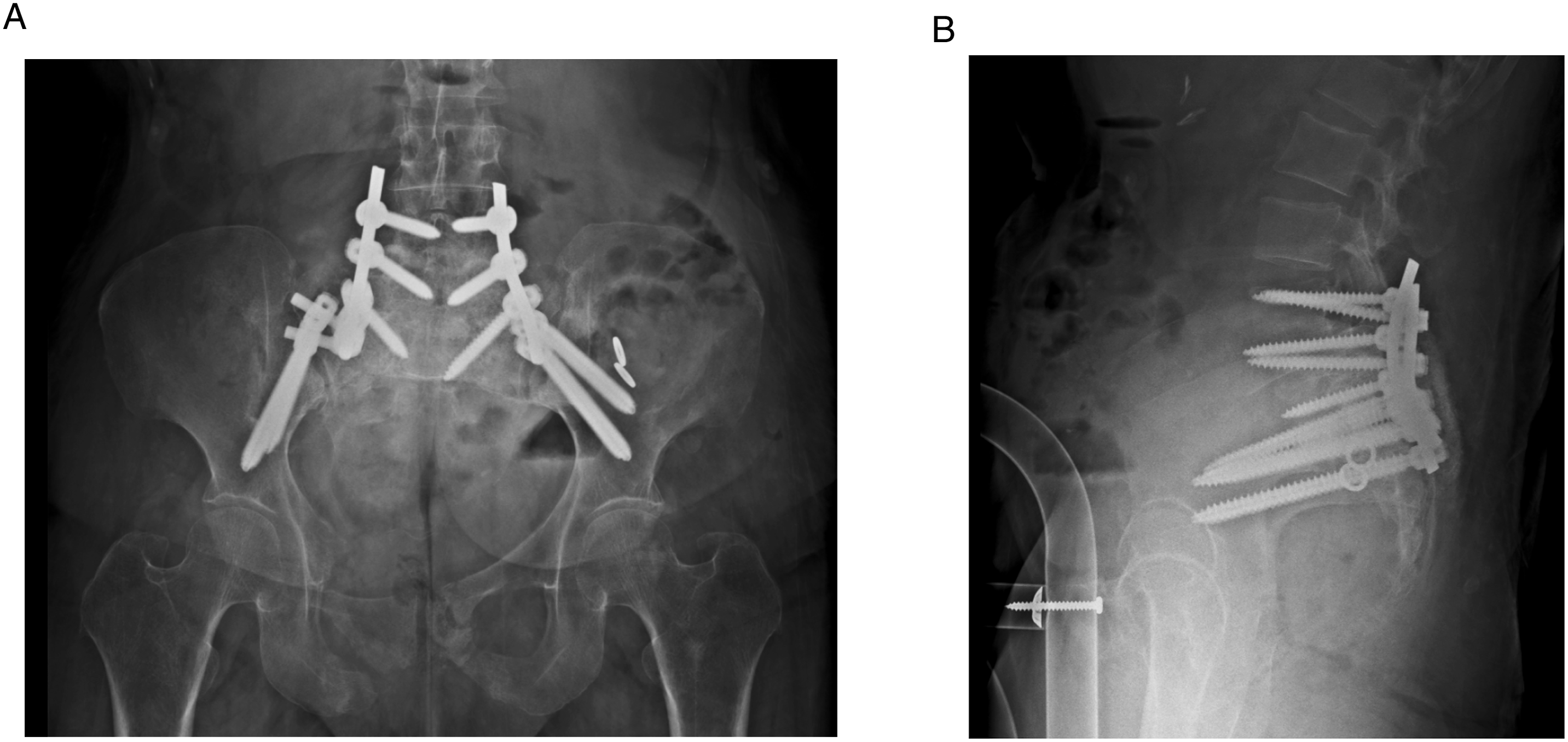
One case of treatment failure was seen in the operative management of the C0 subtype. Originally treated with 2 percutaneous trans-sacral screws, CT imaging revealed nerve impingement from one of the screws that necessitated screw removal and revision of the screw. Two cases of treatment failure were seen in the operative management of the C3 subtype. In the first case, the patient was initially treated with two S1 percutaneous trans-sacral screws and later developed radicular symptoms and weakness revealing a sacral non-union. This was managed with an L5-Ilium fixation with fusion at 7 months following the initial procedure. The second case was initially treated with two S1 percutaneous trans-sacral screws that showed signs of loosening 6 weeks after the initial procedure. This also revealed a sacral non-union and was managed with L4-S1 posterior spinal fusion with bilateral pelvic fixation at 4 months after the initial procedure. Imaging related to this case can be seen in Figures 1-3. No cases of treatment failure were noted in the non-operative management cohort of both subtypes. C3 subtype treatment failure index procedure Preoperative/postoperative imaging. Preop Fracture CT 1 (a). Preoperative coronal computed tomography of the pelvis demonstrating AOSSIC type C fracture pattern. Preop Fracture CT 2 (b). Preoperative coronal computed tomography of the pelvis demonstrating AOSSIC type C fracture pattern. Index Procedure Post-Op CT (c). Immediate index-procedure postoperative coronal computed tomography of the pelvis demonstrating appropriate trans-sacral screw placement C3 subtype treatment progressive failure imaging. 6wk Index Post-Op XR (a). Anterior-posterior plain radiograph of the pelvis at 6 weeks after the index procedure demonstrating evidence of screw loosening. 14wk Index Post-Op XR (b). Anterior-posterior plain radiograph of the pelvis at 14 weeks after the index procedure demonstrating progressive advancement of screw loosening C3 subtype treatment failure revision postoperative imaging. Revision Post-Op XR 1 (a). Immediate revision post-operative anterior-posterior plain radiograph of the pelvis the demonstrating revision procedureRevision Post-Op XR 2 (b). Immediate revision postoperative lateral plain radiograph of the pelvis demonstrating revision procedure
Discussion
This study shows that both operative and non-operative treatment can be appropriate management options for low-energy, nondisplaced U-type sacral fractures with similar outcomes when frailty scores are considered, particularly in the C3 subtype cohort. This finding is further supported by similar PROMIS scores between the two treatments, suggesting that both operative and non-operative approaches are reasonable if the patient and their family are adequately informed of the risks and benefits of surgery.
Operative vs Non-Operative Management
Significant controversy exists regarding the treatment of fracture patterns where the connection between the pelvic ring and the spinal column is lost, (i.e. AOSSIC Type C Fractures). For minimally displaced unstable fracture patterns, good results have been reported with surgical and non-surgical intervention. However, each carry their own set of inherent risks. Those treated nonoperatively typically undergo early mobilization to mitigate the risks associated with prolonged immobilization. In our cohort, those with high frailty scores were considered candidates for non-operative management. Patients with increased frailty might be considered to have a limited ability to perform early mobilization leading to poor outcomes. However, this was not the case in this study as PROMIS scores and complication rates were not different between operative and non-operative groups.
For displaced fractures in patients amenable to surgical management, lumbopelvic fixation provides the most biomechanically rigid construct at the expense of increased morbidity. 16 The success rates of LPF in unstable sacral fractures has been widely reported in the literature with good neurological function recovery and fusion rates approaching 100%. 4 However, this success comes at the cost of increased surgical exposure, healthcare expenditure, and generally higher complication risk.17,18 While still regarded as the treatment of choice for unstable, displaced sacral fractures, infection and wound healing complications associated with larger, open surgery should be taken into consideration when deciding treatment options.
Although less morbid, TSF is a less stable construct that nevertheless has been shown to display comparable outcomes to LPF in previous studies.19,20 The benefit of less biomechanical stability is seen in decreased soft tissue disruption, making TSF an attractive option when similar reported outcomes are considered. 18 However, as seen in this study, TSF is associated with increased rates of symptomatic screw loosening. Additionally, a TSF may be supplemented with an LPF if the trans-sacral screw placement stability or purchase is insufficient. Furthermore, screw loosening in TSF procedures, particularly in patients with osteoporosis or poor bone quality, could be augmented with cement, however this has not been performed at our institution since evidence remains limited in the literature. 21 Thus, both TSF and LPF have a place in management of U-type sacral fractures, and their use should be carefully evaluated for each case.
All patients treated at our institution who sustained a Type C sacral fracture pattern underwent surgical intervention unless they were considered non-surgical candidates due to increased frailty or other comorbidity prohibiting surgical intervention. The first surgical option considered was TSF due to this option’s minimally invasive technique and associated lower morbidity. Although there is minimal soft tissue disruption, TSF constructs were associated with a higher rate of late screw removal. LPF was used as a definitive fixation method for patients deemed not amenable to TSF based on the consulting surgeon’s review of advanced imaging studies and determination of the ability to safely place two trans-sacral screws across the S1 corridor. Both techniques had very high success rates with minimal complications and similar PROMIS outcomes in this cohort.
The decision to pursue operative or non-operative management at our institution was largely driven by frailty scores and the patient’s ability to tolerate and benefit from surgery. The results of this study suggest that when indicated based on frailty scores, particularly in the C3 subtype, there is no difference in PROMIS scores. Prior studies investigating PROMs do not include the newer PROMIS score tool. However Andresen et al in 2022 demonstrated that those with sacral fragility fractures, a less severe injury than spinopelvic dissociation and using a different method of determining operative candidacy, did tend to benefit more from conservative management if the presenting symptoms were less severe. 22 While we are not able to suggest a standardized management decision pathway based on this data, these findings suggest that frail patients with less severe symptoms at presentation could have similar outcomes when managed conservatively, especially in the C3 subtype cohort. Patients with C0 subtype fractures had similar PROMIS and clinical outcomes even though frailty scores were not different.
Complications
Symptomatic instrumentation was the most common postoperative complication in patients undergoing TSF. Thus, the potential for symptomatic instrumentation and future reoperation for its removal should be discussed with patients. This is consistent with previous literature describing TSF instrumentation irritation as a potential drawback to percutaneous fixation. 23 Our institution also encourages immediate weight bearing as tolerated after TSF. No intraoperative complications occurred in either group, and readmission rates were low for both groups. These results suggest that operative fixation is a generally safe option, albeit not without morbidity. Although safe for most patients, the risks may outweigh the benefits in frail patients who may achieve similar outcomes nonoperatively, especially for type C0 fracture patterns. Additionally, medically frail patients may benefit from non-operative management and early mobilization if they accept the risk of fracture displacement and delayed surgery.
Future Directions
Including frailty index scores as a metric for operative or non-operative management of unstable sacral fractures provides a unique avenue for continued research. Traditionally, fracture morphology and symptom severity have driven treatment decisions. However, the results of this investigation reveal that other patient characteristics, such as the mFI-5 frailty index score, could provide an additional decision mechanism. Additionally, multidisciplinary collaboration between sub-specialty surgeons on management pathways for these patients, particularly complex cases where management preferences may differ, would likely improve patient outcomes. Further investigation into this metric, as well as other patient characteristics, could provide improved decision-making tools for surgeons to use when creating management plans. While not calculated in this study, a prospective study investigating an mFI-5 score cutoff for operative vs non-operative management would add a valuable metric for management decisions.
Limitations
This study has several limitations inherent of retrospective study design and selection bias. Surgical and non-surgical treatment was guided by the orthopaedic trauma surgeon who was on call when the patient arrived to the emergency department. We do not follow structured algorithms for deciding who is an operative or non-operative candidate or which type of fixation strategy is appropriate. Additionally, most trauma patients are not established in our system, and we do not have data regarding their osteoporosis status. Furthermore, U-type sacral fractures are an uncommon and heterogeneous injury, thus limiting generalizability due to the small sample size. Although our sample size was small, we did collect all patients who presented to our level I trauma service over a ten-year period making larger studies with greater samples inherently difficult to achieve.
Patients who underwent conservative treatment had shorter follow up time, and most patients overall had a follow-up time of less than one year, limiting our ability to understand long term outcomes between treatment groups. This includes PROMIS score data, where collection was not standardized at this institution for the full ten-year collection period and was only able to be collected for 68% of patients, likely implanting bias into the results. Finally, there was no standardized physical therapy protocol for patients, however it typically included weight bearing as tolerated with a walker as a mobility aid.
Conclusion
This study compared nonoperative and operative treatment of sacral fractures with associated spinopelvic dissociation. Our results indicated that both approaches yield similar outcomes and complication rates when modified 5-Item frailty index scores are considered. While TSF was associated with a higher rate of symptomatic screw removal it is the least invasive surgical treatment option. Thus, more research is needed to determine the optimal treatment choice based on patient-specific factors instead of relying solely on fracture characteristics.
Supplemental Material
Supplemental Material - Sacral U-Type Fractures: A Comparative Study of Treatment Approaches
Supplemental Material for Sacral U-Type Fractures: A Comparative Study of Treatment Approaches by Arnaldo Martinez Rivera, Garrison P. Bentz, Dillon H. Stone, Daniel E. Pereira, Jeffrey T. Galla, Jonathan A. Ledesma, Jonathan Dalton, Blake K. Montgomery, John C. Clohisy, Jenna-Leigh Wilson, Brian J. Neuman, Jacob Buchowski, Keith Bridwell, Mitchel R. Obey, Anna N. Miller, Mark J. Lambrechts in Global Spine Journal
Footnotes
Ethical Considerations
Approved by the Washington University IRB (approval number: 202409159), no further ethical approvals were necessary.
Author Contributions
Conception and design: Rivera, Perez, Lambrechts, Data Collection: Rivera, Perez, Galla, Stone, Analysis and Interpretation: Rivera, Perez, Pereira, Stone, Lambrechts
Manuscript Writing: Rivera, Perez, Pereira, Stone
Manuscript Revision: Ledesma, Dalton, Obey, Bridwell, Wilson, Clohisy, Neuman, Montgomery, Buchowski, Miller, Lambrechts
Final Approval: All authors
Senior Author: Lambrechts
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is available upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.