
Abstract
Study Design
Retrospective cohort study.
Objectives
Glucagon-like peptide-1 receptor agonists (GLP-1RAs) are prescribed for obesity and type 2 diabetes mellitus (T2DM) and exhibit anti-inflammatory and osteogenic effects which may influence fusion outcomes. This study evaluated the association between preoperative GLP-1RA use and perioperative complications, resource utilization, and revision rates after anterior cervical discectomy and fusion (ACDF) in patients with T2DM.
Methods
The TriNetX Global Network was queried for patients with T2DM undergoing single-level or multi-level ACDF. GLP-1RA users were defined by prescriptions within 6 months before and after surgery. Propensity score matching controlled for demographics, comorbidities, and socioeconomic factors. Outcomes included medical and surgical complications, revision rates, and healthcare utilization at 90 days, 6 months, and 1 year.
Results
608 single-level and 639 multi-level GLP-1RA users were compared with matched nonusers. GLP-1RA use was associated with lower revision rates after single-level ACDF at 90 days (OR:0.445, P = 0.032) and 6 months (OR:0.489, P = 0.034). Pseudarthrosis risk was reduced across all timepoints for both single-level and multi-level ACDF (OR:0.296-0.608, all P ≤ 0.008). GLP-1RA users also had lower dysphagia risk following single-level ACDF across all timepoints (OR:0.506-0.661, all P ≤ 0.030). Resource utilization was decreased, with fewer readmissions (single-level: OR:0.401-0.634; multi-level: OR:0.418-0.593, all P ≤ 0.003) and ED visits (single-level: OR:0.563-0.697, all P ≤ 0.007) across all timepoints. On multivariate Cox regression, GLP-1RA use independently predicted reduced pseudarthrosis at 1 year (HR:0.665, 95% CI:0.570-0.775, P = 0.005).
Conclusion
Perioperative GLP-1RA therapy was associated with reduced rates of pseudarthrosis, revision, dysphagia, and healthcare utilization following ACDF without increased adverse events.
Keywords
Introduction
As the global population ages, degenerative cervical spine disease has become increasingly prevalent. Anterior cervical discectomy and fusion (ACDF) is a common surgical treatment for degenerative cervical pathology that has failed conservative management. 1 Among patients undergoing spinal fusion, more than 70% are overweight or obese, and approximately 5%–12% have diabetes.2–5 Both of these comorbidities have been associated with increased complication rates and poorer clinical outcomes compared to nonobese and nondiabetic patients.4,6,7 As healthcare systems transition towards value-based payment models, identifying and optimizing these high-risk patients has become increasingly important.
Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) have emerged as attractive options for patients with obesity and type 2 diabetes mellitus (T2DM), especially given their ability to reduce postoperative risk in these patient populations. 8 Beyond their metabolic effects, preclinical studies have demonstrated their potential to increase bone mass, mechanical strength, and formation - all of which could be relevant to the biological mechanisms important for arthrodesis.9,10 These recent discoveries have prompted surgeons to study their effects on the outcomes of cervical fusion, although existing literature remains conflicting. In single-level ACDF, Chang et al reported an association between GLP-1 RA exposure and a lower risk of pseudarthrosis at 2 years, 11 which was echoed by Vatsia et al in their study on multi-level cervical fusion. 12 In contrast, Ng et al found that semaglutide use prior to posterior cervical fusion was associated with higher rates of pseudarthrosis and dysphagia at 2 years. 13 Similarly, Tao et al examined semaglutide use in patients undergoing cervical spine decompression and fusion and found no association with short-term adverse events at 6 months. 14 Given the heterogeneity in the literature regarding perioperative usage of GLP-1RA in spine surgery, and the limitation of existing studies which largely focus on fusion outcomes as well as semaglutide as a single agent rather than the GLP-1 RA as a drug class,13,14 it is clear that additional research regarding the impact of GLP-1RAs on the medical and surgical outcomes of cervical fusion is necessary.
The objective of the present study was therefore to evaluate the association between preoperative GLP-1 RA use and perioperative complications, resource utilization and revision rates after ACDF in patients with T2DM. We hypothesized that GLP-1 RA exposure would be associated with reduced pseudarthrosis and revision rates without a concomitant increase in adverse events.
Methods
Study Design
This study was conducted using the TriNetX Global Collaborative Network (TriNetX LLC, Cambridge, MA), which provides deidentified electronic health record data including demographic information, laboratory results, medications, medical diagnoses, and procedures from 156 participating institutions.
15
Data available on this platform is not insurance- or employment-based, but rather, a compilation of real-time deidentified charts from all patient encounters (inpatient, outpatient, emergency department, etc.) within a healthcare organization. Deidentification is performed using expert-attested processes like obfuscation and minimum thresholds, ensuring statistical blurring for any outcome with less than 10 patients. The database was queried on August 19, 2025, identifying all patients who had undergone single-level and multi-level ACDF using Current Procedural Terminology (CPT) and International Classification of Diseases, 10th Revision (ICD-10) codes (Supplemental Table 1). For periods prior to the adoption of ICD-10 codes, the platform automatically queries for the corresponding ICD-9 (Ninth Revision) codes. The single-level and multi-level ACDF patients were stratified into GLP-1RA use and nonuse based on whether they had documented GLP-1RA prescriptions in both the 6-month period before surgery as well as the 6-month period after surgery, resulting in 4 total cohorts: GLP-1RA users undergoing single-level ACDF (n = 613), non-GLP-1RA users undergoing single-level ACDF (n = 72 193), GLP-1RA users undergoing multi-level ACDF (n = 640), and non-GLP-1RA users undergoing multi-level ACDF (n = 52 469) (Figure 1). To ensure adequate follow-up, patients were required to have an additional healthcare visit or status of “deceased” between 3 months and 1 year after the index date of study inclusion.
16
Flow diagram of patient selection and cohort assembly
Matching Strategy
Baseline Demographics and Comorbidities of SL and ML ACDF Patients With and Without GLP-1RA Use, Before and After Propensity Score Matching

SL, single level; ML, multilevel; ACDF, anterior cervical discectomy and fusion; GLP-1RA, glucagon-like peptide-1 receptor agonist; CHF, congestive heart failure; COPD; chronic obstructive pulmonary disease; CKD, chronic kidney disease; HIV, human immunodeficiency virus; AIDS, Acquired Immunodeficiency Syndrome; BMI, body mass index; HbA1c, hemoglobin A1c; PSM, propensity-score matching; SD, standard deviation; SMD, standardized mean difference; *, indicates incidence occurring in less than 10 patients in both cohorts over the study period and exact number is not available to protect patient privacy. Bold values indicate statistical significance (P < 0.05).
Outcome Measures
Primary outcomes of interest included medical complications, surgical complications, readmission, ED visits, and revision. All outcomes were analyzed at a follow-up of 90 days, and surgical outcomes were also analyzed at a longer follow-up of 6 months and 1 year. Medical complications comprised deep vein thrombosis (DVT), pulmonary embolism (PE), anemia, acute kidney injury (AKI), aspiration, myocardial infarction (MI), and mortality. Surgical complications included deep infection, surgical site infection (SSI), pseudarthrosis, dysphagia, dysphonia, device failure, cerebrospinal fluid (CSF) leak, and hematoma/hemorrhage. All outcomes were first events in each time window identified using corresponding CPT and ICD-10 codes (Supplemental Table 2).
Data Analysis
Descriptive statistics were calculated for all continuous and categorical variables. Continuous variables were reported as mean ± standard deviation and compared using independent samples t-test. Categorical variables were reported as frequencies with percentages and compared using chi-squared tests. Differences in outcome variables were assessed using odds ratios (OR) and 95% confidence intervals. Cox proportional hazards regression was conducted to evaluate independent effect of GLP-1RA usage on pseudarthrosis. All statistical tests were performed using the TriNetX Analytis interface. Statistical significance was defined as a P-value of <0.05.
Cohort Assembly and Baseline Characteristics
A total of 133 892 ACDF cases were identified in the TriNetX Global Collaborative Network, of which 78 045 were single-level and 55 633 were multi-level. After applying the abovementioned inclusion and exclusion criteria, GLP-1RA users were identified and propensity score matched in a 1:1 ratio with non-users. This resulted in 608 patients in each group for single-level ACDF and 639 patients in each group for multi-level ACDF (Figure 1). Matching achieved excellent covariate balance, with no significant difference in demographics, BMI, comorbidities, smoking status, osteoporosis, or socioeconomic factors (P > 0.05 and SMD <0.10 for each; Table 1).
Results
Ninety-Day Outcomes
Ninety-Day Postoperative Outcomes Following ACDF in GLP-1RA Users Versus Nonusers
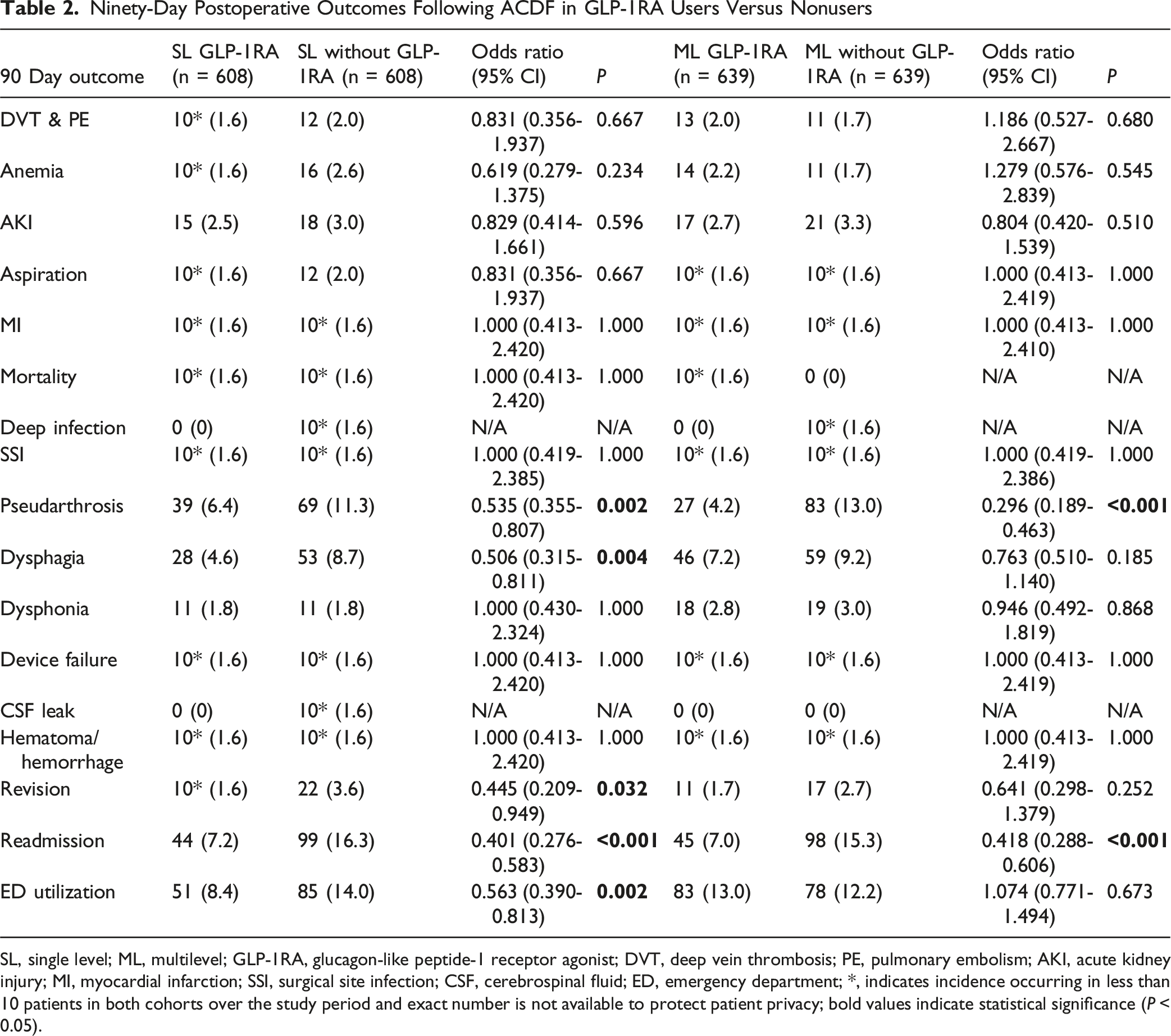
SL, single level; ML, multilevel; GLP-1RA, glucagon-like peptide-1 receptor agonist; DVT, deep vein thrombosis; PE, pulmonary embolism; AKI, acute kidney injury; MI, myocardial infarction; SSI, surgical site infection; CSF, cerebrospinal fluid; ED, emergency department; *, indicates incidence occurring in less than 10 patients in both cohorts over the study period and exact number is not available to protect patient privacy; bold values indicate statistical significance (P < 0.05).
Six-Month Outcomes
Six-Month Postoperative Outcomes Following ACDF in GLP-1RA Users Versus Nonusers
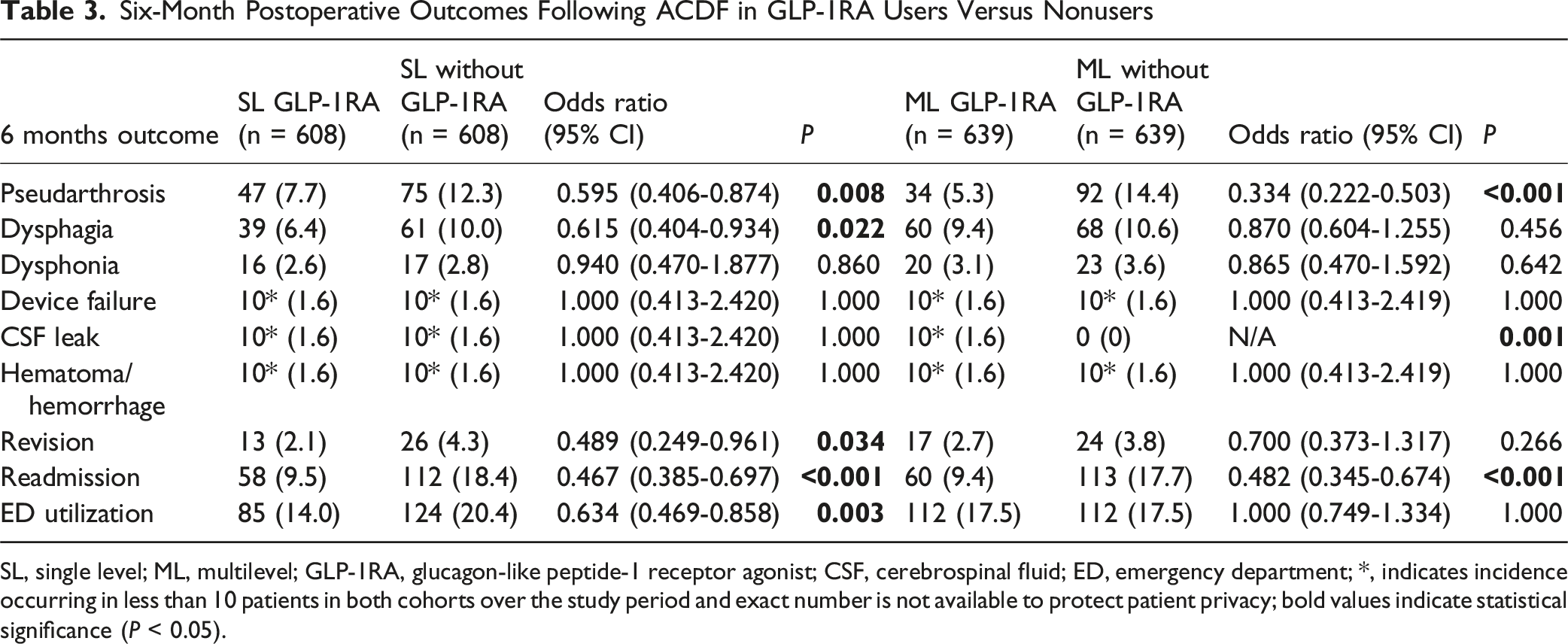
SL, single level; ML, multilevel; GLP-1RA, glucagon-like peptide-1 receptor agonist; CSF, cerebrospinal fluid; ED, emergency department; *, indicates incidence occurring in less than 10 patients in both cohorts over the study period and exact number is not available to protect patient privacy; bold values indicate statistical significance (P < 0.05).
One-Year Outcomes
One-year Postoperative Outcomes Following ACDF in GLP-1RA Users Versus Nonusers
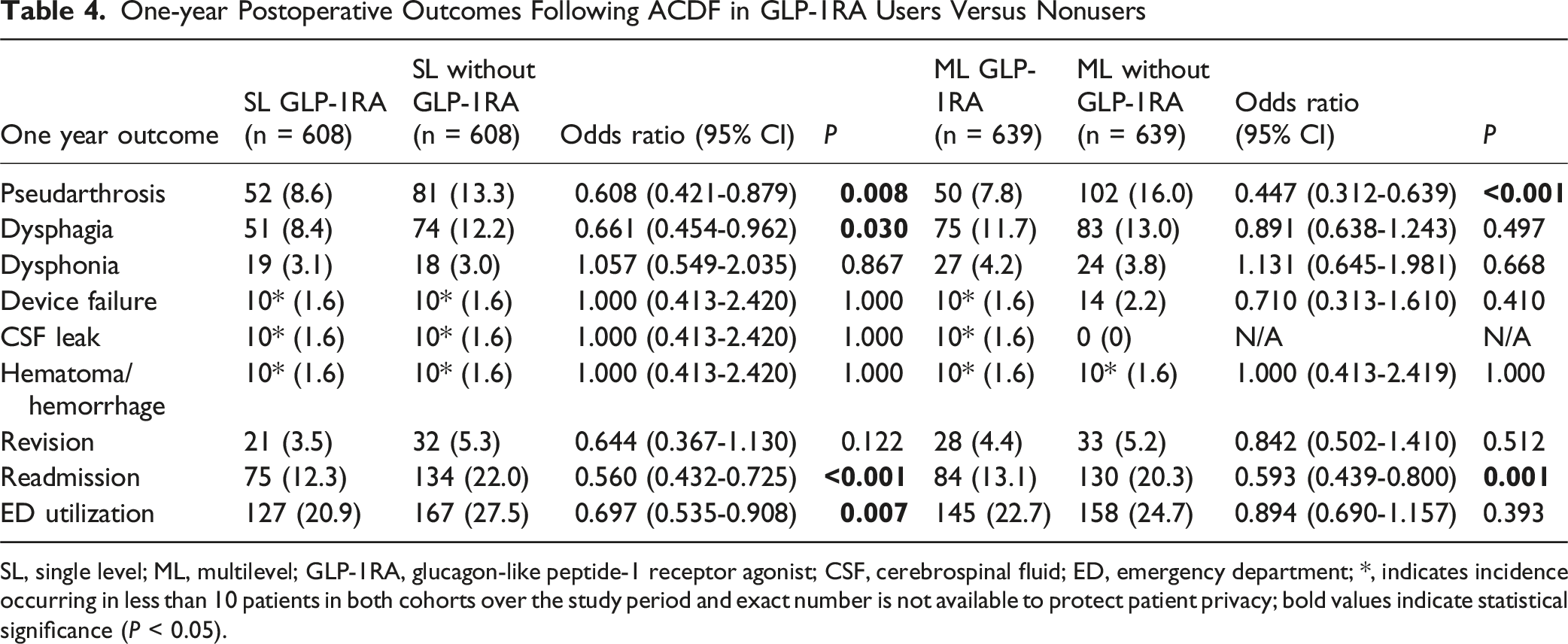
SL, single level; ML, multilevel; GLP-1RA, glucagon-like peptide-1 receptor agonist; CSF, cerebrospinal fluid; ED, emergency department; *, indicates incidence occurring in less than 10 patients in both cohorts over the study period and exact number is not available to protect patient privacy; bold values indicate statistical significance (P < 0.05).
Using Cox proportional hazards regression to control for demographic, comorbidity, and socioeconomic variables, GLP-1RA use remained independently associated with a lower rate of pseudarthrosis at 1 year (HR 0.665, 95% CI 0.570-0.775, P = 0.005).
Discussion
This propensity score-matched cohort of 2494 patients represents the largest study to date evaluating the association between preoperative GLP-1 RA use and clinical outcomes following ACDF, and the first to incorporate both single-level and multi-level procedures. GLP-1 RA exposure was associated with a consistent reduction in pseudarthrosis across multiple timepoints following single-level and multi-level ACDF, as well as a corresponding decrease in revision rates after single-level ACDF. In addition, GLP-1 RA use was associated with a lower risk of dysphagia after single-level ACDF, and overall resource utilization was lower following single-level and multi-level ACDF. When taken together, these findings suggest that GLP-1 RAs may offer both medical and surgical benefits in diabetic patients undergoing ACDF, extending beyond metabolic control to potentially improve fusion biology and perioperative outcomes.
GLP-1 RA use was associated with a lower incidence of pseudarthrosis at 90 days, 6 months, and 1 year after both single-level and multi-level ACDF. Pseudarthrosis after cervical fusion compromises the success of surgery and negatively influences patient outcomes. 12 Reported pseudarthrosis rates typically range from 0% to 20%, but can exceed 60% in certain high-risk populations. 19 Although definitive diagnosis of pseudarthrosis is most commonly established at 2-year follow-up, prior literature has shown that early radiographic and clinical indicators of nonunion frequently manifest within the first postoperative year and are therefore strongly associated with later fusion status, 20 supporting the use of 1-year pseudarthrosis as a meaningful early surrogate for long-term fusion outcomes. Nonunion is linked to persistent pain, segmental instability, radiculopathy, and myelopathy, often necessitating additional surgery. 12 Three recent investigations have examined GLP-1 RAs in cervical fusion with mixed findings.11-13 Chang et al used propensity score matching within the TriNetX database to compare 1245 GLP-1 RA users with nonusers undergoing single-level ACDF, observing a lower 2-year pseudarthrosis rate among GLP-1 RA users. 11 Similarly, Vatsia et al evaluated 5164 patients undergoing multi-level cervical fusion and found a lower 2-year pseudarthrosis rate with GLP-1 RA exposure. 12 In contrast, Ng et al analyzed 1880 posterior cervical fusions and reported higher 2-year pseudarthrosis in patients receiving semaglutide. 13 While the mechanisms underlying this protective effect against pseudarthrosis may be speculative, GLP-1 receptors have been identified on osteoblastic precursor cells, and in-vitro studies have shown that GLP-1RAs may enhance the viability of these cells. 21 Because osteointegration is central to successful arthrodesis, improved osteoblastic function could translate to higher fusion rates among GLP-1 RA users. It is therefore plausible that GLP1-RAs could be used to complement established intraoperative strategies for promoting fusion, including recombinant human bone morphogenetic protein-2, 22 synthetic bone graft substitutes, 23 iliac crest autograft, local autograft, and allograft, 24 although future prospective studies are needed to validate these findings.
In the same vein, GLP-1 RA use was associated with a lower early revision rate at 90 days and 6 months after single-level ACDF. This finding was consistent with that of Wiener et al, who evaluated 2263 patients undergoing any spinal arthrodesis and found lower rates of infection, revision, and readmission among GLP-1 RA users. 8 In contrast, Tao et al analyzed a propensity-matched cohort of 596 patients undergoing single-level or multi-level cervical fusion and found no significant difference in 6-month reoperation rates. 14 Common indications for revision after ACDF include pseudarthrosis, adjacent segment disease, implant failure, infection, postoperative hematoma, and inadequate decompression25–28; for early revisions in particular, hematoma and infection predominate.25,26 In addition to the decreased pseudoarthrosis rate, GLP-1 RA exposure has been associated with reduced postoperative hematoma in certain surgical populations. 29 Mechanistically, GLP-1 receptor activation may limit endothelial injury by decreasing oxidative stress, promoting neoangiogenesis and indirectly inhibiting platelet activation, thereby reducing microvascular thrombosis.30-32 Additional metabolic effects such as improved insulin sensitivity, tighter glucose control, and lower pro-inflammatory cytokine release from visceral adipose tissue could also lead to improved wound healing and reduced infection risk. 33 Collectively, these mechanisms may explain the decreased need for early revision surgery in GLP-1RA users. However, although baseline BMI was included as a criterion for propensity score matching to ensure comparable preoperative body habitus between groups, the TriNetX platform does not reliably capture postoperative BMI changes or weight-loss trajectories. Given that GLP-1RAs can induce substantial weight reduction, it is possible that a reduction in BMI and resultant lower mechanical load during the period of bony fusion contributed to the lower rates of pseudarthrosis or revision observed in the GLP-1RA cohort.
GLP-1 RA use was also associated with a lower risk of dysphagia at 90 days, 6 months, and 1 year after single-level ACDF. Although dysphagia is the most frequently reported ACDF complication in large administrative databases, its incidence spans a wide range in the literature – approximately 1-79% and 0.2-87.5% in recent systematic reviews34–36 – and this complication typically defined as a subjective increase in the time or effort needed to move a bolus from mouth to stomach. 37 The present findings differs from that of Ng et al, who observed higher odds of dysphagia at 2 years after posterior cervical fusion among patients receiving semaglutide, 13 a finding that they contextualized with reports that GLP-1RAs can delay gastric emptying and heightened aspiration risk.38,39 Notwithstanding, the aforementioned gastrointestinal effects are likely less pertinent to ACDF, in which swallowing difficulty is more closely related to prevertebral soft-tissue edema, hematoma, transient neuropraxia from nerve compression or retraction, inflammatory irritation from anterior hardware, and esophageal retraction.36,40,41 Mechanistically, GLP-1RAs demonstrate anti-inflammatory effects, lowering IL-6 and TNF-α and increasing IL-10, 42 and they promote endothelial health by improving vascular function and reducing oxidative stress.43,44 By dampening inflammatory signaling, enhancing microvascular function, and stabilizing endothelial barrier integrity, GLP-1 RAs could theoretically reduce anterior neck edema and expedite recovery, providing a biologically plausible explanation for the lower dysphagia rates observed after ACDF. However, as radiographic measures of soft-tissue thickness were not available, this proposed mechanism remains speculative.
This study is not without limitations. As with all large database studies, our findings rely on accurate diagnosis and complete coding of individual procedures, medications, and complications for each patient. The retrospective nature and lack of control over data collection could also introduce selection bias, which we attempted to minimize by extensive propensity score matching. However, there are remaining residual confounding factors such as concomitant antidiabetic drugs, smoking cessation, and the duration of T2DM that are inherently difficult to capture in a large database study. These unmeasured variables raise the possibility that GLP-1RA use may function as a marker of better overall T2DM management, greater access to healthcare, healthier behaviors, or more intensive follow-up, rather than a direct causal factor influencing surgical outcomes. Although socioeconomic variables were incorporated into our propensity score matching to ameliorate this issue, such matching cannot fully account for confounding by indication or differences in underlying disease control. Furthermore, we could not assess GLP-1 RA dose, adherence, initiation date, or duration, limiting inferences about optimal regimen or preoperative timing. It is important to acknowledge that individual GLP-1RA agents may not exert identical biological effects, particularly with respect to bone metabolism and resulting fusion biology. 45 However, we were unable to determine whether specific agents conferred differential outcomes following ACDF because the code utilized to classify GLP-1RAs use grouped all agents together. Although a few semaglutide-specific studies exist, limited data for other GLP-1RA agents underscore the need for future prospective, agent-specific studies. In addition, the dataset lacked sufficient granularity to specify the exact vertebral levels decompressed or fused, limiting procedure-level interpretation. Likewise, the number of fused levels within the multi-level ACDF cohort could not be determined from the ICD-10 and CPT codes utilized in the TriNetX database. As a result, we were unable to assess whether the distribution of 2-, 3-, 4-level constructs was balanced between the GLP-1RA users and nonusers, which could potentially counfound the observed outcomes in the multi-level cohort. We also did not have consistent postoperative hemoglobin A1C data for the respective groups, which might have shown varying degrees of glucose control. If the GLP-1 RA groups had better glucose control, that alone might explain the different outcomes. But even if that were the case, it would not negate the results of our study, which demonstrated superior medical and surgical outcomes in diabetic patients treated with GLP-1 RA for their diabetes. Despite these constraints, the large cohort size and long follow-up strengthen the findings and provide evidence to inform counseling of ACDF candidates using GLP-1 RAs. Our results suggest that treating diabetic patients with GLP-1RA in the perioperative setting may have advantages for post-operative morbidities and surgical outcomes, but further studies need to be performed to definitively answer this important question.
Conclusion
GLP-1RA use was associated with lower rates of revision, pseudarthrosis, and dysphagia, without a corresponding increase in adverse events. Resource utilization was also lower. These findings suggest that perioperative GLP-1RA therapy could play an important role in optimizing outcomes for high-risk spine surgery candidates, particularly those with obesity or diabetes.
Supplemental Material
Supplemental Material - Perioperative GLP-1 Receptor Agonist Use is Associated With Reduced Revisions and Complications Following ACDF: A Propensity-Matched Analysis
Supplemental Material for Perioperative GLP-1 Receptor Agonist Use is Associated With Reduced Revisions and Complications Following ACDF: A Propensity-Matched Analysis by Matthew T. Kim, Seungjun Lee, Graham S. Goh, K. Daniel Riew in Global Spine Journal
Footnotes
Consent to Participate
This research utilized deidentified, aggregated data from a database. No individual patient identifiers were accessed, and therefore informed consent was not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
IRB Approval
This study did not require ethics approval from an institutional review board.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.