
Abstract
Objectives
: Loeys-Dietz syndrome (LDS) is a rare autosomal dominant connective tissue disorder that may be associated with spinal abnormalities, but no comprehensive review exists on this subject. Therefore, this systematic review synthesized information specifically on spinal pathology in patients with LDS.
Methods
: A systematic review of spinal pathology in LDS was conducted via PRISMA guidelines using the online databases PubMed/MEDLINE, Embase, and Scopus. Studies were included if they detailed spinal pathology in LDS with extractable dada. Studies were excluded if they did not involve spinal pathology in LDS, did not have extractable data, involved spinal pathology not directly due to LDS, were review articles, or were nonhuman studies. Study quality and risk of bias were evaluated using the Newcastle-Ottawa scale.
Results
: A total of 21 studies encompassing 564 LDS patients were included. All articles were single-institution retrospective studies from between 2009-2024. The most common spinal pathologies were scoliosis (n = 154), cervical instability/deformity (n = 97), dural ectasia (n = 58), and spondylolisthesis (n = 32). Patients with cervical anomalies and spondylolisthesis required surgery at higher rates than for scoliosis. Spinal pathologies in LDS were often early-onset and progressive, with many patients failing conservative management. All studies were of limited quality and most had high risk of bias.
Conclusions
: The most common spinal pathologies in LDS were scoliosis, cervical instability/deformity, dural ectasia, and spondylolisthesis. Most scoliosis cases did not require surgery. Cervical pathology and spondylolisthesis required surgery at higher rates in these patients, particularly when progressive and early-onset. There is a need for prospective, larger-cohort studies for these patients.
Introduction
Loeys-Dietz syndrome (LDS) is a rare autosomal dominant connective tissue disorder first described in 2005. 1 LDS exhibits some phenotypic overlap with Marfan syndrome (MFS) and other connective tissue disorders such as vascular Ehlers-Danlos syndrome (EDS).2,3 However, it is now understood that there are distinct genetic underpinnings of LDS, which can be subdivided into 5 different genotypes. LDS types 1-5 are due to pathogenic and likely pathogenic variants (mutations) in TGFBR1, TGFBR2, SMAD3, TGFB2, and TGFB3, respectively.4,5 Most (∼75%) of these mutations arise de novo. These genetic alterations yield increased TGF-β signaling and downstream increases in connective tissue growth factors, collagen expression, and alterations to the connective tissue extracellular matrix. 2
Clinical manifestations of LDS may be broadly categorized as vascular, craniofacial, skeletal, and cutaneous. 2 The most distinguishing clinical features are typically bifid uvula, cleft palate, arterial tortuosity, and hypertelorism.2,3 To date, clinical investigations have largely focused on the vascular manifestations of LDS, which include aortic root dilation, aortic aneurysms, aortic dissections/ruptures, carotid/vertebral artery dissections and intracranial aneurysms.4,6,7 These vascular complications can present at very young ages and may prove life-threatening, which is no doubt why they have garnered the highest degree of scientific inquiry.
Nonetheless, skeletal manifestations of LDS - including pectus deformities, decreased bone quality, joint laxity, appendicular orthopedic deformities, or deformities/instability of the spine - are also common and may significantly affect patient quality of life. 8 Importantly, for practicing spine surgeons, particularly for those interested in spinal deformity, there is a nontrivial chance of encountering patients presenting with spinal sequelae of LDS such as scoliosis, spondylolisthesis, or cervical spine instability. Moreover, there is a paucity of comprehensive reviews specifically pertaining to spinal pathology in LDS. To address this gap, we conducted a systematic review of the available literature to synthesize information on spinal pathology in patients with LDS.
Methods
No institutional review board approval was required as this was a systematic review of previously published articles. This review was conducted according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses literature search extension (PRISMA-S) framework, 9 which is an extension of the traditional PRISMA guidelines, as well as the Peer Review of Electronic Search Strategies (PRESS) guidelines. 10
Search Strategy and Article Selection
The lead author performed the initial literature search using the online databases PubMed/MEDLINE, Embase, and Scopus. All searches occurred between August 8-10, 2025. The entire article selection process can be seen in Figure 1 and the full search strings for each database are shown in the Supplemental Material. No language or date limits were placed on these searches. Only full manuscripts (ie, not abstracts or conference papers) were included. Book chapters were not included. The initial search process yielded 338 results. After applying automatic de-duplication measures in EndNote,
11
the lead author manually screened all results to identify further duplicates. From this, 165 articles remained for closer review. Flowchart detailing the study selection process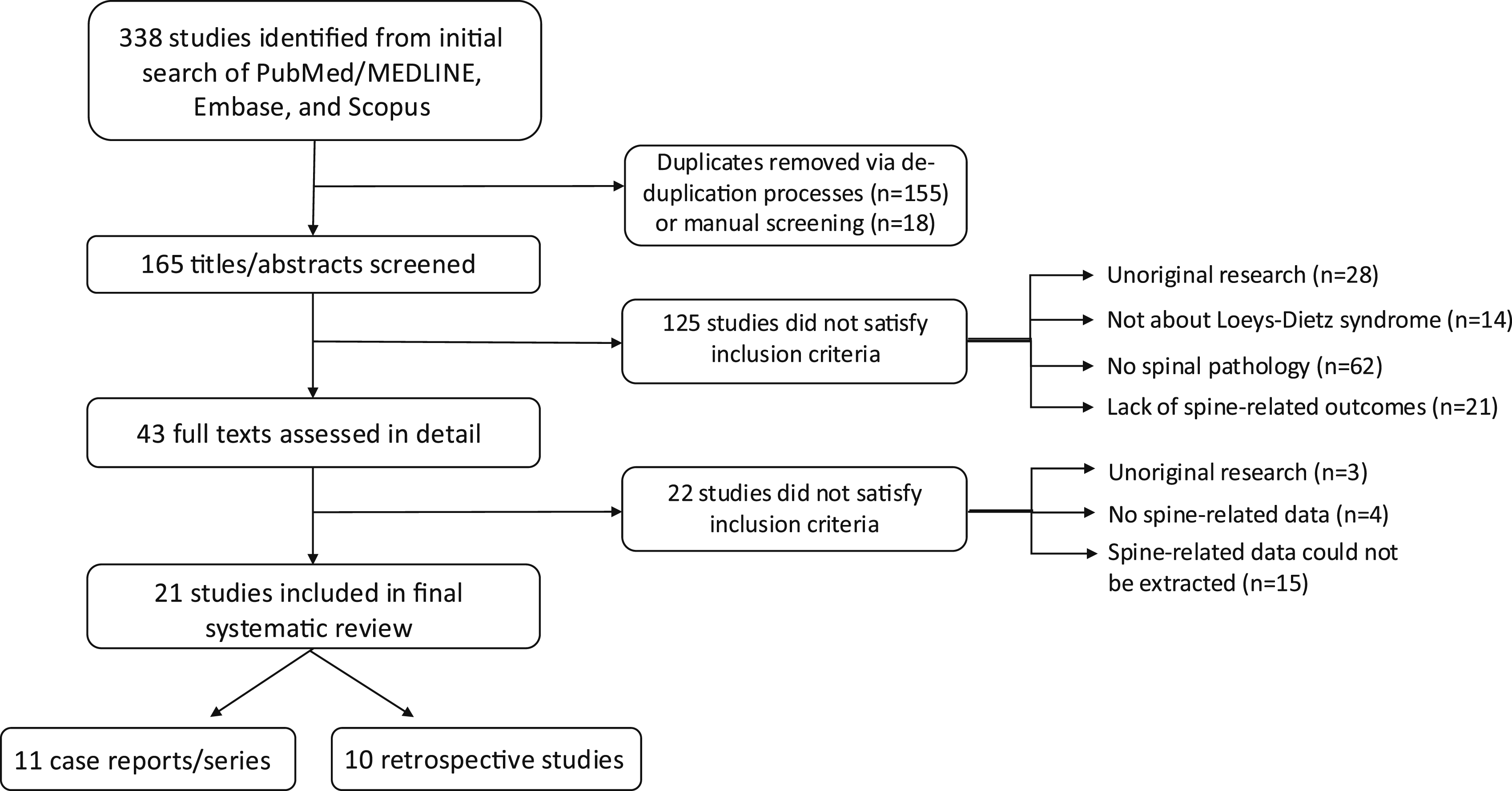
The lead author then assessed each article for inclusion into this study. Inclusion criteria were: (1) studies specifically evaluating spinal pathology in LDS; (2) studies evaluating various orthopedic or neurological pathologies in LDS from which information regarding spinal pathology could be extracted; (3) case reports or series detailing patients with LDS and spine pathology; and (4) studies evaluating radiographic findings for LDS patients from which information regarding spinal pathology could be extracted. Exclusion criteria were: (1) studies not involving patients with LDS; (2) studies evaluating outcomes, radiographic findings, or clinical presentations of LDS but not including spinal pathology; (3) studies evaluating non-spine pathologies in LDS (eg, vascular anomalies) that mentioned the prevalence of spinal pathology (eg, scoliosis) in their patient cohorts but did not provide additional detail regarding the spine; (4) studies evaluating orthopedic or neurological pathologies in LDS but from which specific data regarding the spine could not be extracted; (5) studies involving spinal trauma where it was unclear what role LDS may have played in spinal injury; (6) review articles; and (7) nonhuman studies.
There were no exclusion criteria for patients who had comorbid features of LDS in addition to their spinal pathology. Article titles and abstracts were assessed primarily by the lead author to determine appropriateness given the inclusion/exclusion criteria. Relevant full texts were subsequently read and evaluated. The references of these articles were also screened for additional potential studies. There were no limits for article review based on authors, journals, country of origin, or institutions. Email alerts were set for any potential new publications of interest. No authors were contacted for additional data. Any questions or uncertainties regarding the literature search, the article screening process, or article inclusion/exclusion were resolved through discussions and consensus decision-making among the three authors of this study. Though LDS has been potentially associated with Chiari-1 malformation, 4 we considered this to be brain, not spine, pathology and did not include it in our review.
Data Extraction and Quality Assessment
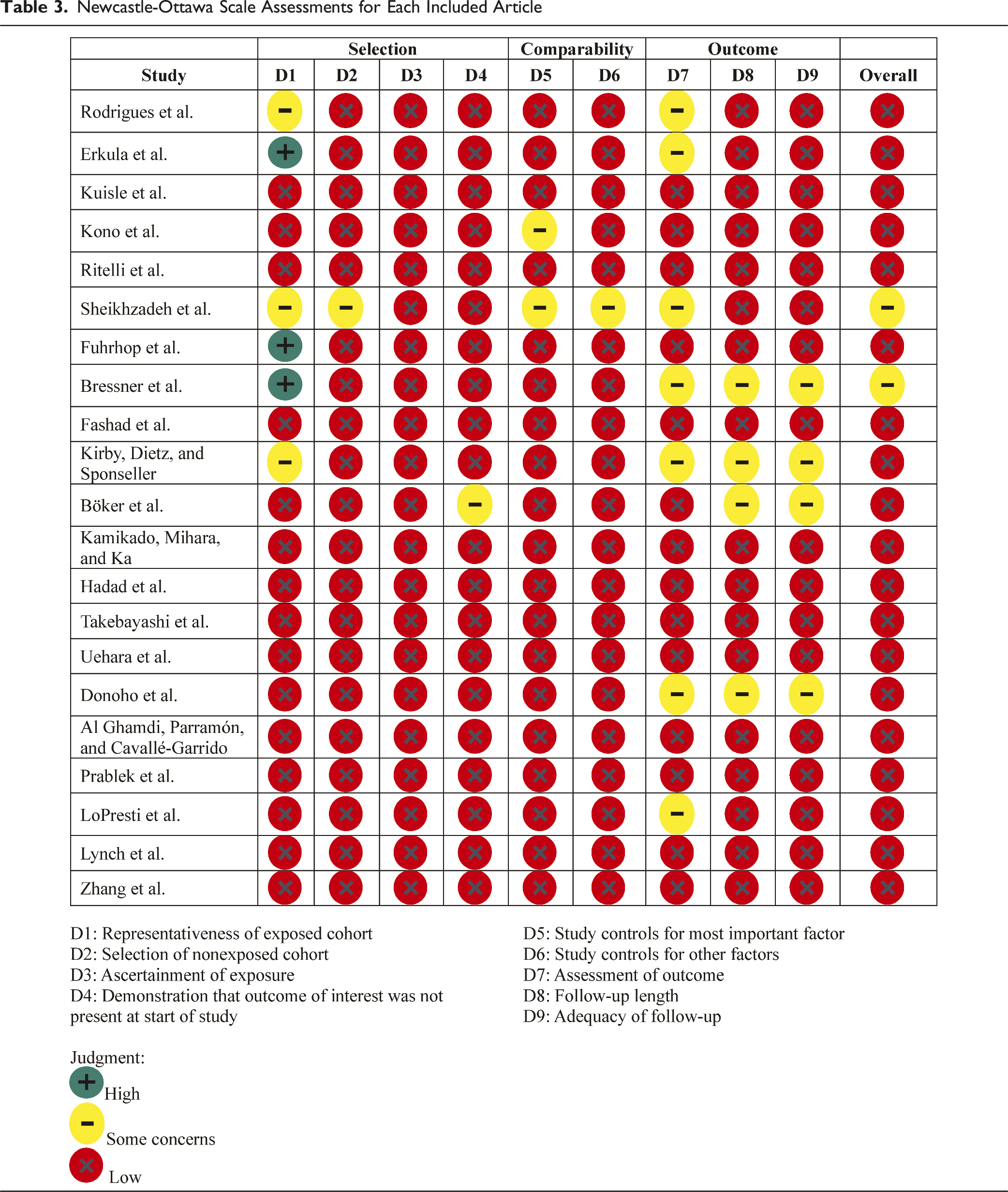
Data, if available from a particular study, regarding total patients, sex, age, type of spinal pathology, management strategies (eg, surgical vs conservative), other comorbid LDS features, types of radiographic findings, and clinical outcomes were extracted from each article into an Excel worksheet. While there was not full duplicate independent data extraction, data was extracted according to inputs from all authors, with any questions data-related questions resolved through discussions. The quality of evidence and risk of bias for each study was evaluated using the Newcastle-Ottawa scale, which is a framework for evaluating evidence quality and identifying biases for observational studies included in systematic reviews and meta-analyses. 12 This scale assesses literature based on three main domains: selection, comparability, and outcomes, with multiple potential components per domain.
Data Analysis
Counts and clinical descriptions for each of the variables of interest were include as able for each study. Data was maintained using Microsoft Excel.
Results
Search Results
After eliminating duplicates, the initial literature search produced 165 studies (Figure 1). After screening titles and abstracts, 125 studies were excluded for not meeting inclusion criteria. Most studies were excluded at this juncture for focusing on non-spine aspects of LDS, being review articles, or not providing extractable information about spinal pathologies. Forty-three were read in full, of which 22 were excluded. Ultimately, 21 articles were included in the review.
Included Studies and Patient Details
Characteristics of 21 Studies Meeting Inclusion Criteria. The Total Number of Patients With LDS in Each Study May Include Patients Without Spinal Pathology
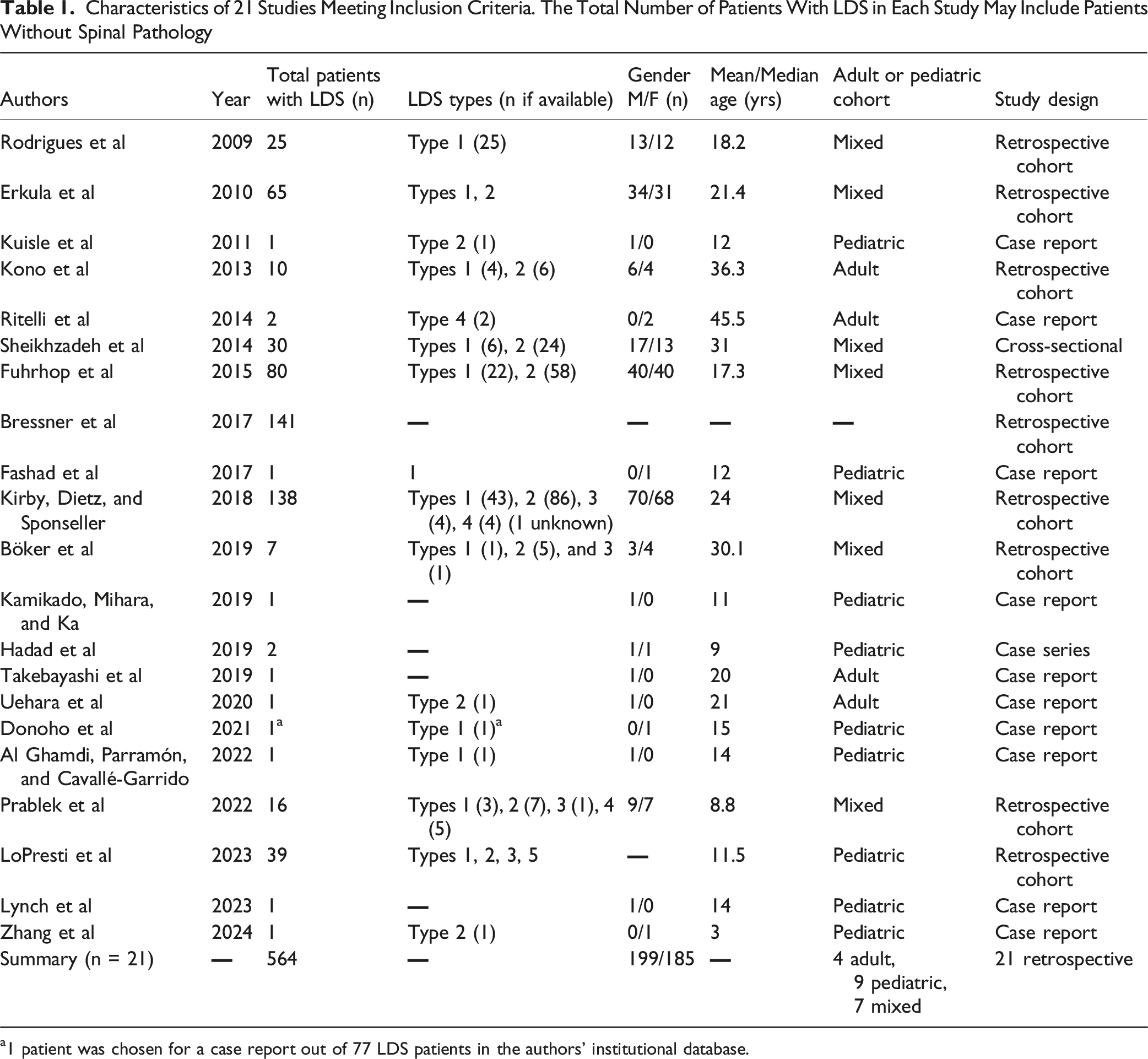
a1 patient was chosen for a case report out of 77 LDS patients in the authors’ institutional database.
Type of Spinal Pathology Stratified by Study. Individual Patients May Have Exhibited Multiple Spinal Pathologies
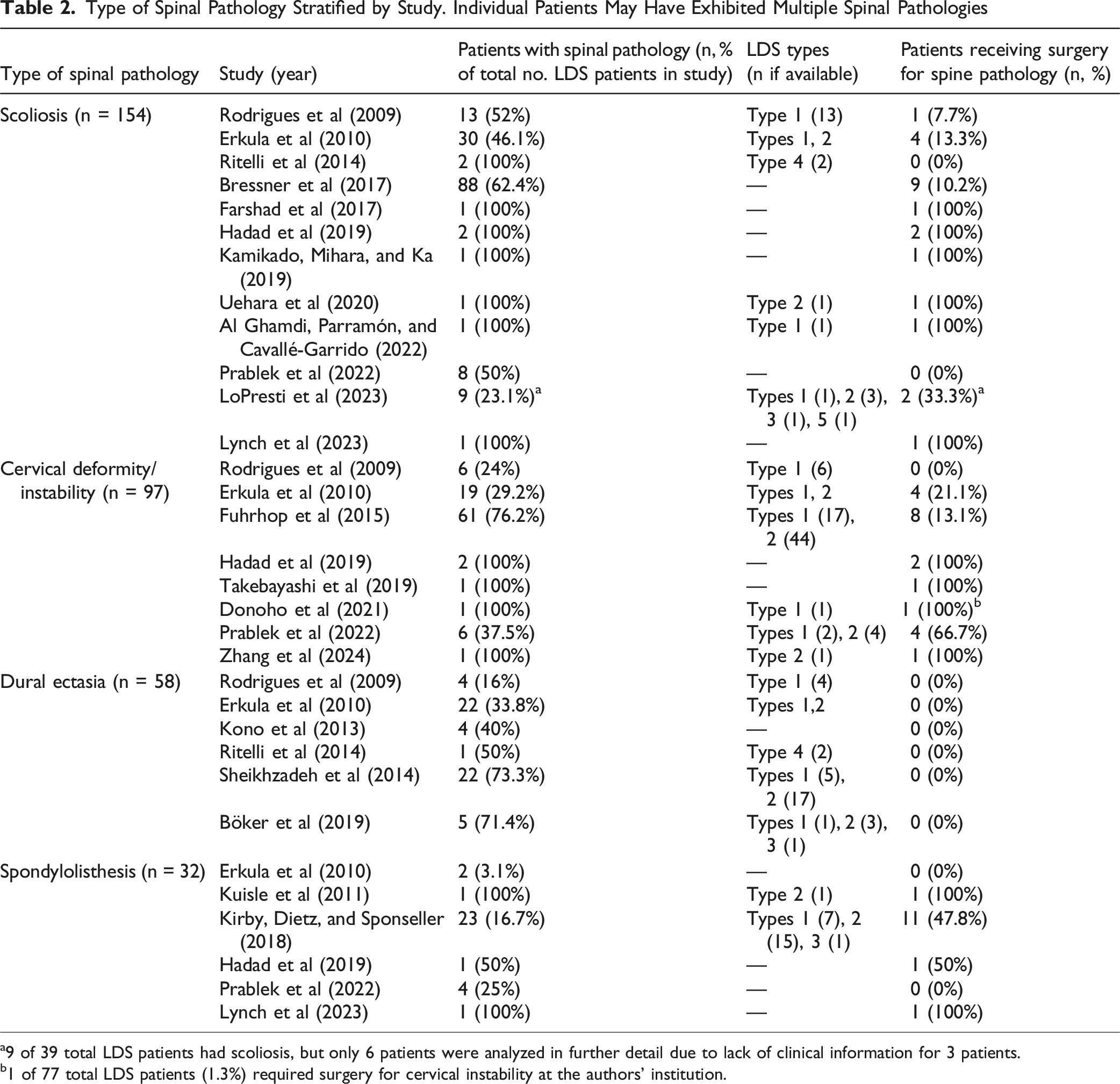
a9 of 39 total LDS patients had scoliosis, but only 6 patients were analyzed in further detail due to lack of clinical information for 3 patients.
b1 of 77 total LDS patients (1.3%) required surgery for cervical instability at the authors’ institution.
In aggregate, 564 patients with LDS were included across all studies (Table 1). The minimum number of patients contributed by a single study was one (10 total studies) and the most was 141. Data on patient sex were found in 19 studies for 384 patients, of whom 199 (51.8%) were male. LDS types 1-5 were represented, though six studies did not stratify patients by type of LDS.15-17,22,23,28 Two studies involved patients multiple types of LDS but did not provide complete counts for each type.25,32 Among studies providing numbers for each type, the most common type of LDS was type 2 [TGFBR2] (n = 209), followed by type 1 [TGFBR1] (n = 107), type 4 [TGFB2] (n = 11), type 3 [SMAD3] (n = 7), and type 5 [TGFB3] (n = 1). A paucity of studies compared LDS cohorts to cohorts with either other connective tissue disorders (eg, MFS) or control groups.
Types of Spinal Pathologies
Across all studies, four main kinds of spinal pathology were discussed. In descending order of frequency, these were: scoliosis (n = 154), cervical instability/deformity (n = 97), dural ectasia (n = 58), and spondylolisthesis (n = 32). The stratification of each type of pathology by article is detailed in Table 2. As noted previously, each article did not necessarily investigate only cohorts with LDS and spinal pathology. For those articles, patients with spinal pathology comprised between 16.7% and 76.2% of the total number of LDS patients. Not all studies stratified spinal pathology by number of patients with each type of LDS. Within those bounds, the most common type of LDS with spinal pathology was type 2 (n = 71), followed by type 1 (n = 57), type 4 (n = 4), type 3 (n = 3), and type 5 (n = 1). Many case studies involved patients who received surgery specifically for spinal pathology. For retrospective cohort studies with larger patient samples, a minority of those patients received surgery. One study detailed a case study of one patient who received surgery for cervical deformity in type 1 LDS, but the authors noted that this was the only patient who underwent surgery for this condition in their institutional database of 77 LDS patients. 19 They thus did not focus on the other 76 patients.
Scoliosis
Scoliosis was the most frequently observed spinal pathology (n = 154) across 12 studies.14-16,18,22-25,28,31,32,34 Despite this, only three studies presented >10 patients.24,25,28 The other nine were case studies or retrospective cohort studies with small sample sizes. Among the larger patient cohorts, the vast majority of scoliotic curves were managed nonoperatively (ranging from 7.7-13.3%). Bressner et al, 28 in the largest study, found that 88/141 patients (62%) with LDS had some degree of scoliosis. 28 The types of LDS were not recorded for this study. The most common types of curves were main thoracic (40%), followed by thoracolumbar/lumbar (31%). Mean curve angles were mild: 16 ± 12° for proximal thoracic, 20 ± 21° for main thoracic, and 12 ± 15° for thoracolumbar/lumbar curves. Nine of these patients (10.2%) underwent surgical deformity correction. Sixteen underwent a trial of bracing (all braced patients were Risser stage 0), of which all but four were considered failures at a mean time of 2.3 years of post-bracing follow-up due to curve progression (10 patients had progressed to a curve >50 degrees). Seven of the patients who failed bracing ultimately received surgery. For surgical patients, the estimated blood loss was high, and nearly half of cases had blood loss >20% of estimated total blood volume. 28 Similar high blood loss and/or intraoperative hemodynamic instability of unclear etiology was noted in multiple case reports of patients undergoing scoliotic correction.15,34 One case report noted a large syrinx in patient undergoing surgery (without accompanying Chiari malformation), 18 though syringomyelia was not noted in other studies examining scoliosis.
Rodrigues et al, in a radiographic analysis of 25 LDS patients, found that 13 patients (52%) had thoracolumbar scoliosis (nearly all curves <15°) but only one patient necessitated surgery for a curve >30°. The highest proportions of patients undergoing surgery were in studies by LoPresti et al 32 (2/6, 33.3%) and Erkula et al 25 (4/30, 13.3%), though the LoPresti et al study excluded three scoliotic patients from their final analysis due to lack of clinical information. Thirty of 55 LDS patients in the Erkukla et al study (54.5%) had scoliosis, with an average Cobb angle of 29.6 ± 17.9°. Most patients (20/30, 66.7%) had thoracic curves. More detailed information regarding patient outcomes for bracing vs surgery was not included in that study.
Cervical Instability/Deformity
Cervical instability or deformity was noted for 97 patients across eight studies.16,17,19,21,24,25,27,31 Only two studies provided >10 patients.25,27 Multiple case reports/series detailed surgical stabilization and/or deformity correction for atlantoaxial instability and unstable subluxations causing severe kyphotic deformities.16,17,19,21 For studies that were not purely dedicated to surgical cases, the rate of surgery ranged from 0-66.7%.24,25,27,31 Fuhrhop et al found that 61/80 patients (76.2%) with LDS (17 type 1, 44 type (2) had vertebral malformations somewhere from C1-C3. 27 Of these, 28 patients (45.9%) had C1 malformations (primarily anterior arch malformations, though nearly half of these had both anterior and posterior arch malformations). Fifty-three patients (86.9%) had C2 malformations, with a majority having dens elongation. Ten patients (16.4%) had hypoplastic subaxial cervical vertebrae. Atlantoaxial instability occurred in eight patients (13.1%), subaxial instability in nine (14.7%), and focal kyphosis in eight (13.1%). Eight patients were treated surgically (13.1%); one was treated in a halo. Of note, 7/8 surgically treated patients (87.5%) required reoperation for postoperative complications related to pseudoarthrosis/instrumentation failure or adjacent level instability. Seventeen of 61 patients (27.9%) in this study had type 1 LDS while 44 (72.1%) had type 2. There were no statistically significant differences in the rates of various cervical spine anomalies by LDS type. 27 Those authors did not make note of vertebral artery abnormalities alongside these cervical pathologies.
Erkula et al 25 found that 19/65 patients (29.2%) with LDS types 1 or 2 had cervical abnormalities (authors did not stratify by LDS type). 25 These also largely involved C1 and C2, with many patients presenting with atlantoaxial instability, rotary subluxation of C1 on C2, or malpositioning of the dens within the C1 ring. This study had the highest proportion of patients receiving surgery for instability (21.1%). Rodrigues et al 24 noted radiographic evidence of cervical malalignment in 24% of patients, but none of these underwent surgery. 24 Prablek et al 31 found cervical deformity or instability in 6/16 patients (37.5%) who received screening cervical radiographs for LDS. 31 Of these, four (66.7%) ultimately necessitated surgery, often after failing a trial of observation secondary to progressive instability or deformity.
Dural Ectasia
Dural ectasia was noted in 58 patients across six studies.14,24-26,33 Rates of ectasia spanned from 16-73.3%. Some studies identified ectasia on imaging obtained for other reasons, while others specifically evaluated ectasia. Multiple studies found similar frequency and severity of dural ectasia for LDS vs MFS, while both diseases significantly differed from asyndromic controls.26,30,33 The largest studies, by Erkula et al 25 and Sheikhzadeh et al 33 (each involving 22 patients), found the prevalence of dural ectasia to be 33.8% and 73.3%, respectively. No interventions or specific changes in management were undertaken for dural ectasia in any study.
Spondylolisthesis
Spondylolisthesis was present for 32 patients across six studies.13,16,22,25,29,31 Only one study provided a reasonably large patient cohort. 29 Kirby, Dietz, and Sponseller reported that of 138 patients with LDS, 24 (17.4%) had lumbar spondylolysis and 23 (16.7%) had lumbar spondylolisthesis (19 L5 on S1 and 4 L4 on L5). 29 By LDS type, 15/23 spondylolisthesis patents (65.2%) had type 2, 7/23 (30.4%) had type 1, and 1/23 (4.4%) had type 3. Fourteen of 23 (60.9%) instances of spondylolisthesis were high-grade (grades 3-5). The median age was 11 years overall, though the median age for high-grade spondylolisthesis was 9 years. Eleven patients (47.8%) received surgery, primarily for high-grade spondylolisthesis, in the setting of progressive back pain, lower extremity symptoms, or worsening slips. Four of these cases required revision for instrumentation failures. Another case report by Lynch et al 22 detailed the occurrence of spondyloptosis in a 14-year-old male who subsequently underwent decompression, partial reduction, and fusion. 22
Spinal Fractures/Poor Bone Quality
There was insufficient numbers of these pathologies to include as a formal part of this review, though a few different studies were found that detailed nontraumatic spinal compression fractures or poor spinal bone quality in the setting of LDS.35-37 No real inferences could be drawn from the low numbers of patients. One case series detailing cervical implant failures in 166 pediatric fusion patients highlighted an instance of anterior screw/plate loosening in a 5-year-old female with LDS, though it is uncertain if her bone quality/LDS actually contributed to this complication. 38
Study Quality
Newcastle-Ottawa Scale Assessments for Each Included Article

Discussion
The connection between LDS and various disorders of the spine is well-known. However, much less research has been published regarding spinal pathology in LDS than, for instance, vascular pathology. This intuitively makes some sense as vascular presentations such as aortic dilation or dissections, carotid/vertebral artery disease, or intracranial aneurysms can pose a significant risk to patients’ lives. These conditions are rapidly progressive and may arise early in childhood, making accurate identification, close surveillance, and optimally timed interventions of the utmost importance. By comparison, spinal pathology in LDS is of relatively lower acuity. This does not mean, though, that proper management of this condition and an understanding of the relevant risks are not of interest to patients or practicing spine surgeons. While LDS is relatively uncommon, many spine surgeons will care for patients with LDS. This systematic review is the largest effort to date to synthesize the available information on the most frequent spinal pathologies found in LDS.
Scoliosis was the most common spinal pathology that was identified in our review. This is consistent with a prior review from 2021 by Conor et al 8 that broadly examined orthopedic deformities among patients with LDS, including certain spinal conditions. No significant large studies on either scoliosis or any other spinal pathology have been published since that time, underscoring the need for continued research in this area. LDS, similar to other connective tissue disorders, can cause joint hypermobility, osseous malformations, and other abnormalities of bone/tissue interfaces, which contribute to increased rates of scoliosis. 39 Prior research has shown that the degree of joint laxity in LDS may depend on the underlying genetic mutation. 40 Among patients with LDS, types 1 (20-25%) and 2 (55-60%) are the most common, which was reflected across the studies in our review. Studies examining presentations across all types of LDS have shown that perhaps scoliosis is a more common presentation in type 2 LDS than type 1. 4 Regardless, though scoliosis presents more frequently in patients with LDS, the minority of patients in our review ultimately received surgical correction of their curves. Many studies included mild curves that were treated with observation or a trial of bracing. Patients who were successfully braced experienced minimal curve progression or achieved skeletal maturity with curves <50 degrees. Those who failed bracing experienced curve progression and typically developed curves that exceeded 50°degrees. It should be noted that multiple studies identified patients who were offered surgery for their scoliosis but were not surgical candidates due to need for aortic surgery or other vascular sequelae of LDS. Additional studies should be conducted to further differentiate nuances in scoliotic progression and presentations among LDS, other connective tissue disorders, and idiopathic cases.
LDS type 3, caused by mutations in SMAD3, was first described in 2011 and is characterized by osseous anomalies - including early-onset joint degeneration, osteoarthritis, and osteochondritis dissecans - that are not seen to the same degree in other forms of LDS. 41 Indeed, this subtype was initially called aneurysms-osteoarthritis syndrome before it was incorporated into the spectrum of LDS types. Interestingly, for studies that recorded types of LDS, LDS type 3 was only found in seven patients, of which three displayed some form of spine pathology (one scoliosis, one dural ectasia, one spondylolisthesis). Thus, it appears that the distinctive osseous manifestations found in LDS type 3, though they affect bone and joint quality, may not contribute to spinal pathology to the same degree as LDS types 1 or 2, hinting at the relative importance of different types of connective tissue involvement in these conditions.
Cervical pathology, which is more associated with LDS than other connective tissue diseases, has also been primarily associated with LDS types 1 and 2.4,40 Flexion/extension radiographs of the cervical spine are recommended upon diagnosis of LDS. 42 In the studies we reviewed, cervical deformity or instability required surgery at a higher rate than scoliosis. This is likely because of the tendency for cervical pathology in LDS to involve the upper cervical spine, particularly C1 and C2. Atlantoaxial instability, even if not overtly symptomatic, requires treatment given the danger of devastating spinal cord injury. Trials with bracing or observation is not as viable an option as for scoliosis. Importantly, for reasons that have not been entirely elucidated, LDS patients who receive instrumentation and fusion in our review very often required revision surgery due to instrumentation failure or pseudoarthrosis. This could conceivable be due to the difficulty in fusing cervical vertebrae that frequently have accompanying osseous malformations or due to generally diminished bone health or connective tissue laxity that is also found in these patients. For this reason, patients should be closely monitored after surgery, even if asymptomatic.
Spondylolisthesis, while the least common of the four spinal pathologies examined in this review, nonetheless occurred in LDS patients at a higher rate than in the general population. Of note, the included studies emphasize that LDS patients may have progressive and high-grade spondylolisthesis at an especially young age. As with cervical pathology, patients undergoing fusion for spondylolisthesis also experienced a relatively high rate of revision surgery due to instrumentation failure or pseudoarthrosis. Further research is warranted in this area to inform surgical decision-making, perioperative management of these patients, and the roles that poor bone quality or excessive motion caused by LDS may play in developing spondylolisthesis.
Dural ectasia is not unique to LDS and represents a common overlap among various connective tissue diseases. In our review, we found that up to 73% of LDS patients were found to have dural ectasia. Such pathology has also been reported as occurring in high frequency among patients with EDS, MFS, neurofibromatosis type 1 (NF1), or Hadju-Cheney syndrome. 39 The exact pathogenesis of dural ectasia is still not entirely known, but likely a loss of dural integrity from abnormal connective tissue results in ectasia, meningoceles, or related pathology due to pulsatile pressure from cerebrospinal fluid (CSF). For patients with NF1, it has been hypothesized that the dura is weakened by abnormal tissue infiltration. 43 Dural ectasia is often seen in proximity to vertebral osseous malformations or scoliosis, which hints at a link between these pathologies, but ectasia may also be seen in isolation around normal-appearing anatomy. Large ectasias may cause neurological symptoms and require repair or CSF diversion, 43 but this was not observed in any case in our review.
Study Strengths and Limitations
Strengths of our study include an extensive literature search regarding spinal pathology in LDS, encompassing >500 patients among 21 studies, making this the largest systematic review dedicated to these presentations of LDS. We were able to stratify spinal pathology somewhat by type of LDS and included cohorts of both pediatric and adult patients. This review highlights the need for further research in this area utilizing large databases to compare outcomes in LDS to both other connective tissue disorders as well as normal control patients. Multicenter efforts should likely be undertaken to achieve sufficient patient cohorts.
That said, there are limitations to this study. Since LDS is a rare disease, the number of patients available for any single study was generally low. As exhibited by our Newcastle-Ottawa assessments, the literature overall is of concerning quality. The fact that the majority of the literature search, screening process, and article inclusion process was performed by a one author introduces the risk of bias, though discussions were had among all authors to resolve questions/concerns. Moreover, LDS is a fairly new disease, and our understanding of its genetics has increased rapidly over the past 20 years. Multiple studies did not stratify patients by subtype of LDS, which impedes full understanding of the nuances underlying the pathologies described in those studies. Many of the studies provided relatively cursory analyses, at times neglecting longer-term follow-up, demographic data, or specific details regarding patient presentations. Finally, limited quantitative analyses were performed on the data extracted from studies given the heterogeneity of the data, small sample sizes, and inconsistent reporting of results. Nonetheless, this systematic review fills a vacant niche in the literature by synthesizing and describing the existing literature on this important topic.
Conclusions
Scoliosis was the most common spinal pathology in LDS, though most of these patients did not necessitate surgery. Cervical instability/deformity required surgery at higher rates than other pathologies. Symptomatic high-grade spondylolisthesis may occur at young ages in these patients. Dural ectasia is common in LDS as with other connective tissue diseases. Spinal pathology, especially if early-onset, is likely progressive and increases the likelihood of requiring intervention. There is a need for prospective, larger-cohort, higher-quality studies with improved genetic information, control cohorts, follow-up, and outcomes reporting.
Supplemental Material
Supplemental Material - Spinal Pathologies Associated With Loeys-Dietz Syndrome: A Systematic Review
Supplemental Material for Spinal Pathologies Associated With Loeys-Dietz Syndrome: A Systematic Review by Alexander T. Yahanda, Alan C. Braverman and Camilo A. Molina in Global Spine Journal
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
None of the authors have any conflicts of interest to declare.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.