
Abstract
Study Design
Umbrella systematic review.
Objective
To qualitatively synthesise systematic reviews evaluating the prevalence, correlates, and outcomes of mental illnesses in individuals with traumatic spinal cord injury (tSCI).
Methods
Systematic reviews reporting on depression, anxiety, post-traumatic stress disorder (PTSD), substance use disorders (SUD), cognitive impairment, and related psychological outcomes in tSCI populations were identified and synthesized as per PRISMA guidelines. Data on prevalence, risk factors, assessment tools, and interventions were extracted. Methodological quality was appraised using AMSTAR 2, and primary study overlap was assessed.
Results
Twenty systematic reviews published between 2005 and 2025 were included. Depression was the most frequently studied condition (n = 16), followed by anxiety (n = 10), PTSD (n = 6), and SUD (n = 4), with several reviews addressing multiple conditions. Primary study sample sizes ranged from 3152 to over 50 000 participants, with wide variation in injury characteristics, study design, and outcome measures. Pooled prevalence estimates indicated a substantial burden: depression affected up to 43% of community-dwelling individuals, anxiety symptoms around 27%, PTSD up to 62%, and hazardous alcohol use ≥50% in some cohorts. Common risk factors included pain, injury severity, incomplete injury, low social support, maladaptive coping, and co-occurring psychological symptoms. Evidence for effective interventions was limited, and few studies used standardised, validated tools across settings.
Conclusions
Mental health conditions are highly prevalent in the tSCI population, yet intervention research remains limited. Standardised assessment, longitudinal designs, and targeted, evidence-based interventions are urgently needed to address this critical but under-recognised aspect of tSCI care.
Introduction
Traumatic spinal cord injury (tSCI) is a severe neurological complication that results in serious morbidity, including physical dependence and mental stress. 1 The global burden of spinal injuries is mainly due to road traffic accidents, and is showing an increasing incidence, prevalence, and years lived with disability when projected in the current trend through 2046, with disproportionate impacts in low- and middle-income regions. 2 This growing epidemiological trend amplifies the need for holistic care models that address not only physical rehabilitation but also the psychological sequelae of tSCI. Although the mortality in acute and chronic SCI is still a major public health problem, the overall life expectancy has significantly improved over the recent decades.3,4 Such improved outcomes in tSCI have been broadly attributed to advancements in medical care and enhanced rehabilitative strategies. 5 The focus of management in these patients has thus gradually evolved from enhancing survival to meliorating functional independence and quality of life (QoL). 6
QoL is an ill-defined phenomenon, which has been correlated with diverse entities including physical functioning, subjective perception of health, psychological well-being, cognitive abilities, need satisfaction, socioeconomic milieu and severity of major mental or physical impairments. 7 Mental health is one of the crucial, yet undervalued, aspects of individual rehabilitation of an individual following traumatic major SCI. As mental health disorders such as depression, anxiety, and PTSD are increasingly recognised as critical determinants of recovery and quality of life, their integration into tSCI management is both timely and essential. Compared to other neurological and oncological conditions such as stroke, traumatic brain injury (TBI), and cancer, individuals with tSCI exhibit comparable or higher rates of psychiatric morbidity. 8 For instance, depression and anxiety are prevalent in up to 40% of stroke survivors and 30% of cancer patients, whereas PTSD and substance use disorders are more frequently reported in TBI cohorts.9-11 This underscores the need for focused mental health interventions in tSCI populations. Studies have reported that 30-40% and 20-25% of patients develop major depressive disorder (MDD) and anxiety disorder, respectively, following SCI.7,12 Additionally, psychological problems like substance use disorder (SUD), post-traumatic stress disorder (PTSD), suicidal tendencies and cognitive decline have also been increasingly described in SCI patients. 13 In this context, the importance of understanding clearly the psychosocial problems in tSCI cannot be understated.
Different systematic reviews have individually discussed the diverse psychiatric ailments afflicting patients with acute and chronic tSCI. The current overview of systematic reviews was thus planned to comprehensively analyse the different psychiatric conditions, their overall prevalence, as well as their relative influence on the outcome of patients with tSCI.
Methods
This study was designed as a systematic review in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 14 The review aimed to synthesise existing evidence on the prevalence, risk factors, and management strategies for different psychiatric conditions among individuals with tSCI, with a particular focus on the interplay between mental health outcomes and injury-related variables.
Eligibility Criteria
Systematic reviews were considered eligible if they met the following criteria: (1) involved human participants diagnosed with tSCI; (2) assessed mental illness such as depression, anxiety, PTSD, SUD, or cognitive impairment; (3) reported prevalence rates, associated risk factors, or intervention outcomes; (4) included observational (cross-sectional, cohort, or case-control) or interventional (randomized or non-randomized trials) studies in their study design; and (5) were published in peer-reviewed journals in English. Studies focusing on animal models or non-validated mental health assessments were excluded. No restrictions were placed on publication year to capture the full breadth of available literature.
Information Sources and Search Strategy
A comprehensive literature search was conducted across multiple electronic databases, including PubMed/MEDLINE, Embase, Scopus, Cochrane Database of Systematic reviews, CINAHL, and Web of Science, from their inception to the final search date on 31st August 2025. The search strategy was developed using controlled vocabulary terms (eg, MeSH, Emtree) and free-text keywords related to “spinal cord injury,” “depression,” “anxiety,” “post-traumatic stress disorder”, “substance abuse”, and “mental health” were combined using Boolean operators. The search strategy was adapted for each database to account for differences in indexing. Reference lists of included studies and relevant reviews were hand-searched to identify additional eligible publications. Grey literature sources, including clinical trial registries and dissertations, were screened to minimise publication bias.
Study Selection
All records retrieved from the database search were imported into a reference management system, and duplicates were removed before screening. Two reviewers independently screened titles and abstracts against the predefined eligibility criteria. No date restrictions were applied. Full texts of potentially eligible reviews were then assessed in detail, with disagreements resolved through discussion or consultation with a third reviewer. Reasons for exclusion at the full-text stage were documented, and the final set of included reviews was summarised in the PRISMA flow diagram.
Data Extraction
A standardised data extraction form was developed and pilot-tested on a subset of studies to ensure consistency. Extracted data included study characteristics (author, year, country, study design), participant demographics (sample size, age, sex distribution), tSCI-related variables (aetiology, level, and completeness of injury, time since injury), mental health assessment tools used, prevalence rates of identified illness, identified risk factors, and details of any interventions evaluated. For interventional studies, additional data on intervention type, duration, comparator, and outcome measures were recorded. Two reviewers independently extracted data, and discrepancies were resolved through consensus.
Quality Assessment
The methodological quality of each included systematic review was assessed using the AMSTAR 2 (A Measurement Tool to Assess Systematic Reviews) framework, which is specifically designed for appraising reviews of healthcare interventions. 15 Two reviewers independently rated each review across 16 domains, including protocol registration, comprehensiveness of the search strategy, duplicate study selection and data extraction, risk of bias assessment in included studies, and appropriateness of synthesis methods. Reviews were categorised as high, moderate, low, or critically low confidence based on the presence of critical flaws. Discrepancies in ratings were resolved through discussion or consultation with a third reviewer. The AMSTAR 2 ratings were used to contextualise the strength of evidence and guide interpretation of findings, particularly in cases of discordant conclusions across reviews.
Assessment of Overlap and Synthesis Approach
Given the nature of this study as a systematic overview, primary study overlap across included reviews was quantified using the corrected covered area (CCA) method. This metric allowed us to assess redundancy and potential bias introduced by repeated inclusion of the same studies. Overlap was categorised as slight, moderate, high, or very high, and findings were interpreted accordingly. No meta-analysis was conducted, as the overview aimed to synthesise findings qualitatively. Instead, a structured narrative synthesis was performed, grouping results by mental health condition (eg, depression, anxiety, PTSD, substance use disorders) and outcome type (eg, prevalence, severity, correlates, impact on quality of life). Where multiple reviews addressed the same condition, we prioritised those with higher methodological quality and more recent publication dates, while transparently reporting any discordance in findings. Certainty of evidence was judged qualitatively, considering AMSTAR 2 ratings, overlap magnitude, and consistency of findings across reviews.
Results
Search Outcome and Review Selection
The initial database search yielded a total of 1842 records. After removal of duplicates (n = 1112), 730 titles and abstracts were screened. Of these, 127 full-text articles were assessed for eligibility, resulting in 20 systematic reviews8,12-30 that met the inclusion criteria as shown in Figure 1. Reasons for exclusion at the full-text stage included lack of focus on tSCI populations, absence of mental health outcomes, or failure to meet minimum methodological standards for systematic reviews. PRISMA flow diagram of inclusion of studies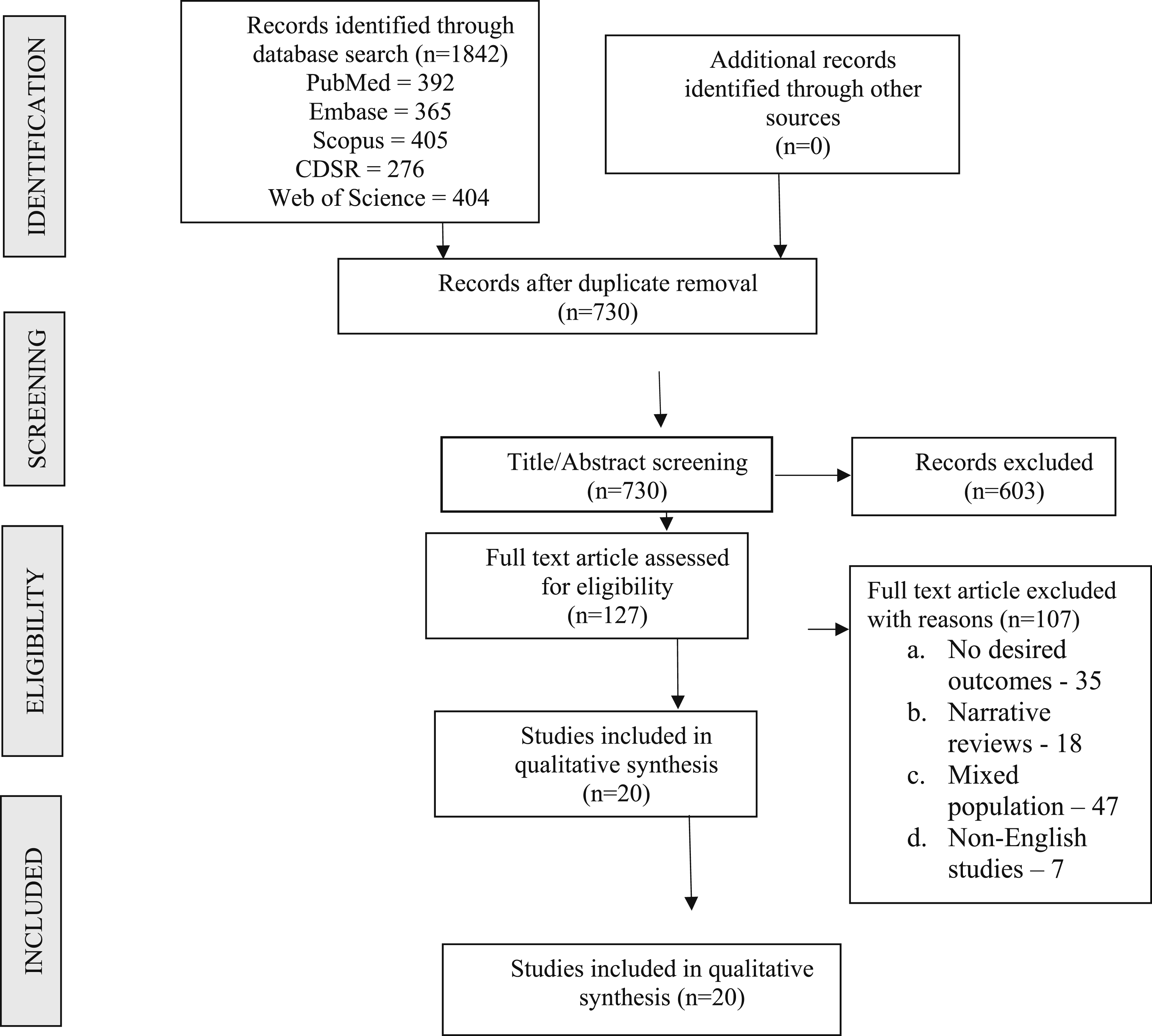
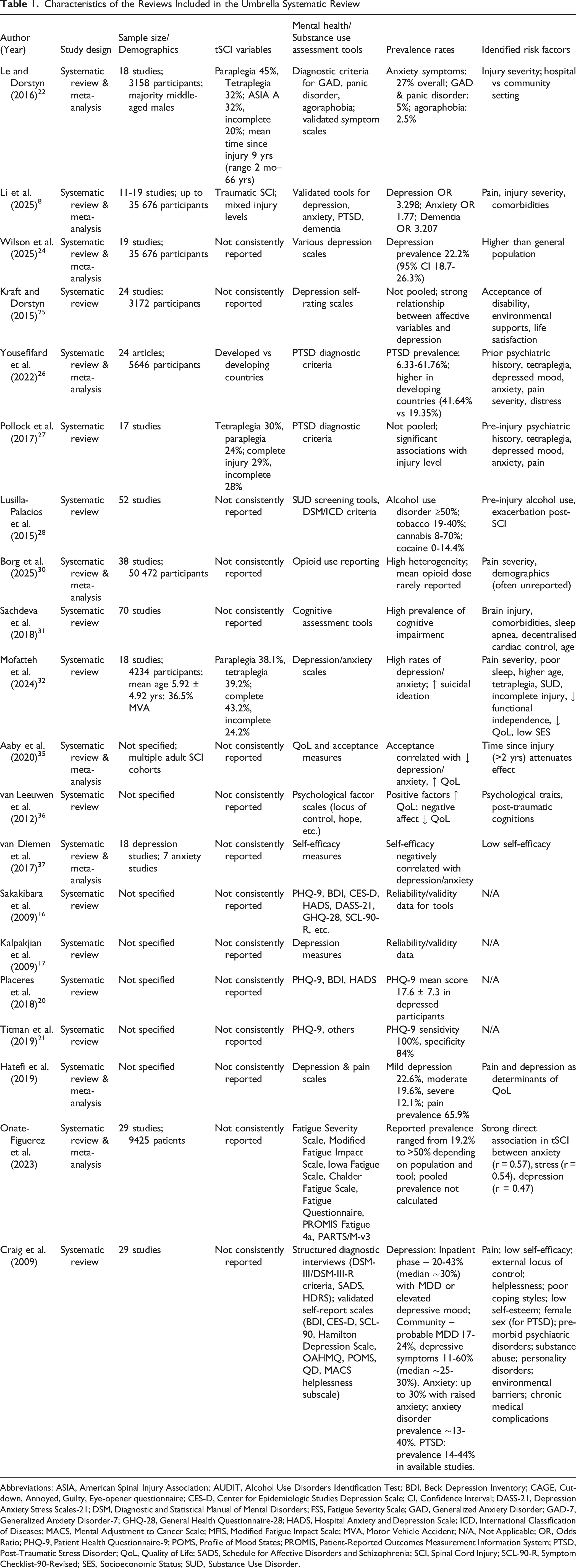
Characteristics of Included Reviews
Characteristics of the Reviews Included in the Umbrella Systematic Review
Abbreviations: ASIA, American Spinal Injury Association; AUDIT, Alcohol Use Disorders Identification Test; BDI, Beck Depression Inventory; CAGE, Cut-down, Annoyed, Guilty, Eye-opener questionnaire; CES-D, Center for Epidemiologic Studies Depression Scale; CI, Confidence Interval; DASS-21, Depression Anxiety Stress Scales-21; DSM, Diagnostic and Statistical Manual of Mental Disorders; FSS, Fatigue Severity Scale; GAD, Generalized Anxiety Disorder; GAD-7, Generalized Anxiety Disorder-7; GHQ-28, General Health Questionnaire-28; HADS, Hospital Anxiety and Depression Scale; ICD, International Classification of Diseases; MACS, Mental Adjustment to Cancer Scale; MFIS, Modified Fatigue Impact Scale; MVA, Motor Vehicle Accident; N/A, Not Applicable; OR, Odds Ratio; PHQ-9, Patient Health Questionnaire-9; POMS, Profile of Mood States; PROMIS, Patient-Reported Outcomes Measurement Information System; PTSD, Post-Traumatic Stress Disorder; QoL, Quality of Life; SADS, Schedule for Affective Disorders and Schizophrenia; SCI, Spinal Cord Injury; SCL-90-R, Symptom Checklist-90-Revised; SES, Socioeconomic Status; SUD, Substance Use Disorder.
Methodological Quality and Overlap
Using the AMSTAR 2 tool, 6 reviews were rated as high confidence, 8 as moderate, 5 as low, and 3 as critically low. Common methodological limitations included a lack of protocol registration, inadequate assessment of risk of bias in primary studies, and the absence of funding source disclosure in the primary studies. The CCA analysis revealed moderate overlap across reviews (CCA = 8.2%), with higher redundancy observed in studies addressing depression and anxiety. This overlap was accounted for in the synthesis and interpretation of findings.
Diagnostic Criteria Employed
In a systematic review by Sakakibara et al, 16 Psychometric measures of different anxiety and depression instruments in patients with SCI were individually evaluated.
Instruments Specific to the Diagnosis of Depression 17
Among the instruments specific to the diagnosis of depression, PHQ-9 (Patient Health Questionnaire-9) and PHQ-9-Short (employed to screen and evaluate the symptom severity for MDD) were shown to have excellent reliability (alpha = 0.87) and validity ranging between adequate and excellent. 18 The BDI (Beck Depression Inventory), CESD-20 (Centre for Epidemiological Studies Depression Scale), CESD-10 and SRS (employed to evaluate the severity of depression) demonstrated excellent reliability (alpha = 0.89, 0.91, 0.86 and 0.81, respectively). 19 MEDS was also evaluated as a measure to evaluate the severity of symptoms, and was reported to have excellent internal consistency (alpha = 0.92) and excellent validity. In the study by Placeres et al, the mean total PHQ-9 score of patients meeting the criteria for depression was 17.6 ± 7.3%. On the other hand, BDI and HADS (Hospital Anxiety and Depression Scale) scores were 51.6 ± 15.1% and 37.5 ± 31%, respectively, in those presenting with some degree of depression. 20 Based on the review by Titman et al, 21 the PHQ-9 has been reported to carry one of the highest sensitivity (100%) and specificity (84%) rates.
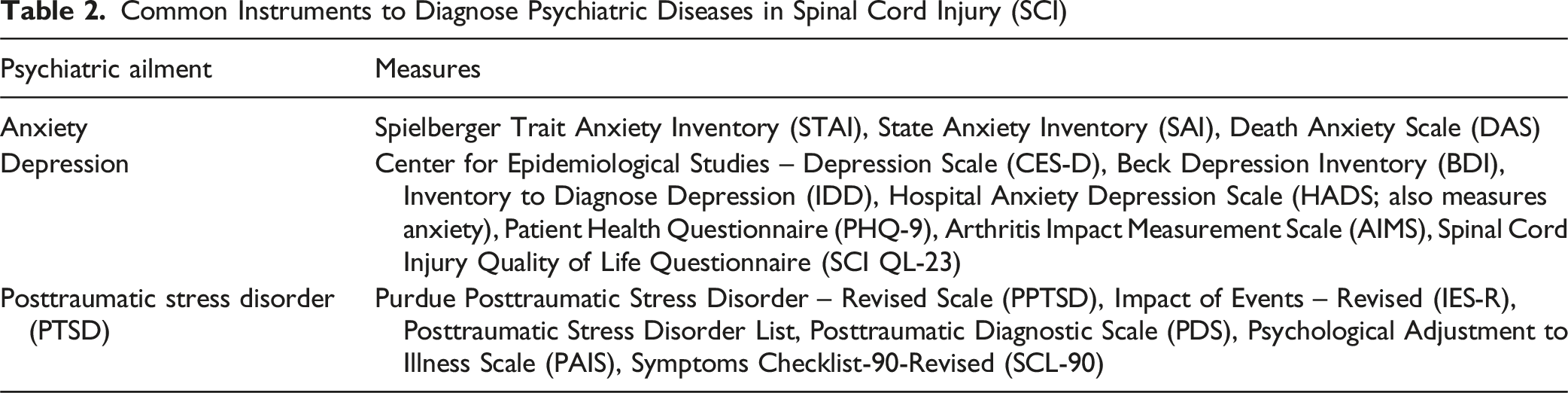
Instruments Specific to the Diagnosis of Depression and Anxiety
Common Instruments to Diagnose Psychiatric Diseases in Spinal Cord Injury (SCI)
Anxiety in SCI
In the systematic review by Le et al. 22 (2016) involving 18 independent studies (3158 patients), a majority of patients were middle-aged males. The injury patterns were inconsistently described in the individual studies. Overall, 45% and 32% of patients had paraplegia and tetraplegia, respectively. Among the patients with neurological deficits, while 32% presented with ASIA A neurology, 20% had incomplete weakness (AIS B, C and D). The mean time since the onset of tSCI was 9 years (ranging between 2 months and 66 years). Overall, 27% of individuals (ranging between 15 and 32%) reported clinically significant anxiety-related symptoms. Overall, anxiety symptoms were reported in 27% and 29% of tSCI patients in hospital- and community-based samples, respectively. Based on diagnostic criteria (reported in 2 studies), 5% had the diagnosis of general anxiety disorder (GAD) and panic disorder, while 2.5% were diagnosed with agoraphobia. In another recent meta-analysis, Li et al 8 showed that patients with tSCI had a significantly increased risk of anxiety (in comparison with non-tSCI patients; OR: 1.77, 95% CI: 1.512-2.072; P < .001).
Depression in SCI
Based on the analysis of 5 studies, Li et al 8 concluded that tSCI patients had a significantly enhanced risk of depression [Odds Ratio (OR): 3.298, 95% CI: 2.622-4.150; P < .001]. In another systematic review, 23 the prevalence of mild, moderate and severe depression in tSCI patients was 22.6%, 19.6% and 12.1%, respectively. In this series, the overall prevalence of pain following SCI was 65.9% (95% CI: 53.9%-76.1%), and the authors concluded that both pain and depression were significant determinants of health status and QoL.
In a meta-analysis by Wilson et al. 24 Involving 19 studies (35 676 patients), the mean prevalence of depression after SCI was 22.2% (ranging between 18.7% and 26.3%). Based on this review, they observed that the rates of depression were significantly greater than the prevalence in the general population (16% overall prevalence and 6.7% annual prevalence rates in the United States). Based on a review of 24 studies (3172 patients), Kraft et al 25 demonstrated that individual personal variables like affective feelings, beliefs and thoughts (which are specific to tSCI) bore the strongest relationship with depression self-rating; while acceptance of disability, environmental supports, and life satisfaction carried medium-to-strong relationships with the development of depression. They observed from longitudinal studies that symptoms of depression continuously influenced the psychosocial outcome in patients even until 10 years following injury. They also recommended that adopting a unified approach for measuring depression could enable a targeted approach to its treatment.
PTSD in SCI
A recent systematic review by Yousefifard et al 26 involving 24 articles (5646 patients) demonstrated that PTSD symptoms were prevalent in 6.33% (95% CI 2.73-13.97%) to 61.76% (95% CI 52.07-70.61%). The pooled analysis revealed that the overall prevalence of PTSD was substantially higher in the developing world, in comparison with developed countries [41.64% (95% CI 31.11-52.55%) vs 19.35% (95% CI 14.66-24.51%); OR: 1.24; P = .003].
In another systematic review by Pollock et al 27 involving 17 studies, 30% and 24% had tetraplegia and paraplegia, respectively. While 29% of patients had complete (ASIA A) neurological injury, 28% had incomplete (ASIA B, C, D) injury. Pre-injury and injury-related parameters such as prior psychiatric history (P = .01) and tetraplegia (P < .01) significantly correlated with the development of PTSD. Among the post-injury parameters, depressed mood, anxiety, pain severity, distress and negative appraisal were significantly associated with PTSD. Based on limited data involving the veteran population, the levels of injury significantly correlated with PTSD (P < .001).
Substance Use Disorder (SUD) in SCI
There is limited data regarding diverse substance use disorders in patients with tSCI. 28 In a systematic review by Lusilla-Palacios et al, 28 involving 52 studies, it was shown that while 86.5% of reviewed articles discussed alcohol use disorder, 28.8% reported on the use of tobacco. On the other hand, the evidence regarding the other drugs is still substantially limited (11.5% of articles report on cannabis and illicit drugs). Based on their review, it was observed that SUD was significantly more common in the SCI patients, in comparison with the general population. At least 50% of tSCI patients had significantly higher alcohol consumption (ranging between moderate and heavy drinking, based on screening procedures, DSM or CIE criteria). They also observed relatively higher pre-injury prevalence of SUD (particularly, alcohol), which showed an exacerbation following the tSCI. 29 They reported prevalence rates of tobacco use, cannabis and cocaine (or other psychostimulants) ranging between 19 and 40%, 8 and 70%, and 0 and 14.4%, respectively.
In a systematic review by Borg et al. 30 (2025) involving 38 studies (50 472 patients; 5% studies with high risk of bias), a high heterogeneity was observed (prediction interval twice as high as 95% CI). The mean opioid dose was not reported in 95% of studies, and other factors (like pain severity or demographic characteristics of the population) associated with opioid use in tSCI patients were not reported in the majority of studies. They thus highlighted the inconsistency in the reporting of opioid use and its severity in tSCI patients, and emphasised the need for additional studies to investigate the magnitude of this problem in this high-risk cohort.
Cognitive Issues in SCI
In a study by Sachdeva et al, 31 70 studies reporting on cognitive function in patients with tSCI were reviewed. They reported that there was substantially enhanced prevalence of cognitive impairment following tSCI, with potential risk factors such as associated brain injury, mental or somatic comorbidities, sleep apnea, decentralised cardiac control, and age. They could not observe any clear association between incidence of cognitive impairment and the level of injury.
In the meta-analysis by Li et al, 8 it was demonstrated that tSCI patients had a significantly increased risk of dementia (OR: 3.207, 95% CI: 2.485-4.137; P = .001). Based on their meta-analysis, they did not observe any significant correlation between SCI and Alzheimer’s disease; however, other types of dementia were significantly increased in this patient cohort.
Mental Health in Pediatric SCI
A recent systematic review by Mofatteh et al 32 involving 18 studies (4234 patients with the youngest mean age at of time of injury was 5.92 ± 4.92 years, and 36.5% underwent motor vehicle accidents) evaluated the diverse risk factors associated with increased levels of depression and anxiety in pediatric patients presenting with major tSCI. Overall, while 1613 (38.1%) and 1658 (39.2%) patients had paraplegia and tetraplegia, respectively, 1831 (43.2%) and 1024 (24.2%) had complete and incomplete tSCI, respectively. They demonstrated that factors including pain severity (P < .01), reduced quality of sleep (P < .001), higher age (P < .001), tetraplegia (P = .011), substance use disorder, incomplete cord injury (P = .013), decreased functional independence, shorter duration since injury (P = .043), decreased QoL (P < .001), and lower socioeconomic status (unemployment, lower annual income, and prolonged hospitalization) substantially increased the risk of developing anxiety and depressive symptoms. They reported that patients with pediatric-onset tSCI had significantly enhanced suicidal ideation 33 [with factors like male sex (P = .035), reduced motor function (P = .043) and elevated depression levels (P < .001) contributing significantly to the occurrence of suicidal tendencies].
Discussion
Some of the common mental health disorders in patients with traumatic SCI include depression, anxiety-related disorders, PTSD, cognitive disabilities and SUD. The current overview comprehensively discusses the psychological morbidity in patients with traumatic SCI, the role of acceptance on mental health, association with quality of life (QoL), and the overall clinical impact on the patients and their caregivers.
Psychological Morbidity and Traumatic SCI
In the meta-analysis by Li et al 8 (including 11 studies), patients with tSCI were at significantly enhanced risk for developing anxiety, depression, dementia, insomnia, adjustment disorders, mood disorders, psychosis, neuropathic pain, personality disorders, and substance use disorders (including alcohol-related disorders) (P = .05). There was no statistically significant association between tSCI and PTSD. Based on their meta-analysis of 4 studies, they concluded that patients with SCI had substantially enhanced risk for psychological morbidity (OR: 2.736, 95% CI: 2.166-3.456; P < .001). These findings underscore the broad spectrum of psychological morbidity associated with tSCI, extending beyond depression and anxiety to include cognitive, behavioral, and affective disorders. The lack of a significant association with PTSD contrasts with other reviews, suggesting potential variability in diagnostic criteria, population characteristics, or underrecognition of trauma-related symptoms in tSCI cohorts.
Acceptance and Mental Health
Acceptance is described as “perception of the injury as an integral part of life; re-evaluating values of life; and developing a coping strategy which is relevant in unalterable conditions.34,35 In a recent meta-analysis, Aaby et al 35 showed that greater acceptance significantly correlated with higher global and psychological QoL, mental health, sense of well-being, life satisfaction, and decreased levels of anxiety and depression (although the correlation with PTSD was inconsistent). However, beyond the initial 2 years following the injury, such a correlation between acceptance and any of these outcome parameters (such as QoL or mental health) was no longer observed.
QoL and Mental Health
There is substantial evidence regarding the influence of psychological parameters on the patients’ QoL following tSCI. Studies have demonstrated considerable evidence about the impact of psychological parameters on the QoL of patients with tSCI. In a recent meta-analysis by van Leeuwen et al, 36 while locus of control, sense of coherence, self-worth, positive affect, purpose in life, and hope were substantially associated with higher QoL; negative affect and negative posttraumatic cognitions consistently correlated with lower QoL.
Self-efficacy is defined as an individual’s belief in their capacity to execute behaviours and successfully achieve their specific goals. High self-efficacy leads to improved resilience and performance, while poor self-esteem results in avoidance behaviour. In the systematic review by van Diemen et al 37 (involving 18 and 7 studies on depressive and anxiety disorders, respectively), self-efficacy is negatively correlated with anxiety and depressive symptoms in tSCI patients.
Current Findings and Their Clinical Impact
The management of patients with tSCI can be substantially improved by carefully monitoring their psychological status and enhancing the idea that he/she is a valuable individual in excellent control of their own meaningful life. 36 The patients sustaining major SCI have an enhanced risk of developing diverse mental health and cognitive dysfunctions, which substantially impair their mood/affect, personality and learning abilities. Caregiving spouses and nursing staff are exposed to substantially enhanced levels of psychological morbidity, including severe burnout, fatigue, resentment and emotional stress.24,38 It is of utmost importance for rehabilitative physicians or other individuals involved in the long-term care of patients with tSCI to recognise their psychological limitations and develop realistic views of expectation. Such an approach would help in ameliorating the overall outcome as well as mitigating the stress levels of the family members and members of the rehabilitative team.
Only 6 of the 20 included reviews reported treatment rates. Among these, less than 30% of patients with diagnosed mental health conditions were receiving active psychological or pharmacological interventions, highlighting a significant care gap. The elevated prevalence of psychiatric conditions in tSCI patients is not merely a statistical observation—it reflects a systemic gap in post-injury care. Despite high rates of depression, anxiety, and PTSD, treatment uptake remains low, and validated screening tools are inconsistently applied. The psychological burden extends beyond patients to caregivers, who often experience burnout, emotional exhaustion, and secondary trauma. Early psychosocial intervention, caregiver support programs, and routine mental health screening should be integrated into rehabilitation protocols. Future research should explore the timing and modality of interventions whether early psychological support during acute care improves long-term outcomes, and how digital tools or peer-led programs might enhance accessibility in resource-limited settings.
Limitations
This overview has several limitations that should be considered when interpreting its findings. The included systematic reviews exhibited substantial heterogeneity in study design, participant characteristics, injury chronicity, diagnostic criteria, and outcome measures, which limited direct comparability and precluded quantitative synthesis. Although some reviews achieved high or moderate confidence ratings on AMSTAR 2, others were of low or critically low quality, often due to absent protocol registration, incomplete risk-of-bias assessment, or inadequate reporting of funding sources. Primary study overlap was moderate, particularly for depression and anxiety, raising the possibility of inflated effect estimates in these domains. Mental health outcomes were assessed using a wide range of screening tools and diagnostic criteria, many of which lacked validation in tSCI populations, potentially affecting prevalence estimates. Furthermore, most primary studies originated from high-income countries, with limited representation from low- and middle-income settings, where prevalence patterns and risk factors may differ. Despite efforts to search grey literature, the reliance on peer-reviewed sources may have excluded relevant unpublished data, especially for less-studied conditions such as substance use disorders and cognitive impairment. Finally, the included reviews span nearly two decades, during which diagnostic practices, rehabilitation strategies, and societal attitudes toward mental health have evolved, potentially influencing reported prevalence and associated factors.
Conclusion
This umbrella systematic review demonstrates that mental health disorders—particularly depression, anxiety, PTSD, SUD, and cognitive impairment—are highly prevalent among individuals with tSCI, with the most consistent evidence supporting depression and anxiety as the leading conditions. These disorders exert a profound negative impact on quality of life, functional recovery, and caregiver well-being. The findings highlight the urgent need for routine mental health screening using validated, SCI-specific tools across all stages of care, alongside integrated, multidisciplinary interventions that address both physical and psychological rehabilitation. Standardisation of outcome measures is essential to improve comparability across studies and strengthen future evidence synthesis. Moreover, targeted research is needed in underrepresented populations and on less-studied conditions to ensure a more comprehensive understanding of mental health in tSCI. By recognising and addressing the psychological dimensions of spinal cord injury, clinicians, researchers, and policymakers can work toward more holistic, patient-centred models of care that improve long-term outcomes for this vulnerable population. By integrating mental health into the continuum of tSCI care, from acute management to long-term rehabilitation, clinicians can foster more holistic recovery. This review underscores the need for standardised assessment, targeted interventions, and inclusive research that reflects global diversity in tSCI populations.
Footnotes
Author Contributions
Dr SMuthu and Dr VKV contributed to the conceptualization and design of the research goals and aims. Dr SMuthu developed the methodology and statistical framework. Dr BP carried out the data collection. Data validation and ensuring the accuracy of results were undertaken by Dr SMuthu and Dr VKV. Dr SMuthu secured the necessary resources for the study, and Dr BP curated and organized the study data. Writing the original draft of the manuscript was managed by Dr SMuthu, with Dr VKV providing critical revisions and editing. Visualization and creation of figures were executed by Dr SMuthu. Supervision and coordination of the project were led by Dr SMuthu. Dr KS and Dr SKRC helped in the revision of the manuscript. All the authors approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data generated in the study will be made available upon reasonable request to the authors.