
Abstract
Study Design
Bibliometric analysis.
Objectives
To identify and characterize the 100 most cited articles on lumbar disc arthroplasty (LDA) to better understand influential contributions to the field and highlight key trends in research focus and collaboration.
Methods
A Web of Science search for “lumbar disc arthroplasty” OR “lumbar disc replacement” was conducted on December 1, 2024. The top 100 articles by citation count were screened for inclusion. Extracted variables included number of citations, authorship, journal, publication year, institution, and keyword frequency. Citation trends and networks were analyzed using VOSviewer and the Bibliometrix package in RStudio.
Results
The 100 most cited articles were published between 2002 and 2018, with citation counts ranging from 27 to 377 (mean 66.6). The most cited study was a 2005 FDA investigational device trial on the CHARITÉ™ disc. Publication volume peaked in 2007. Spine was the leading journal (N = 38), followed by European Spine Journal (N = 20). Mayer HM, Siepe CJ, and McAfee PC were the most prolific authors. Network analysis identified 18 author clusters, demonstrating strong self-citation patterns and institutional concentration in North America and Europe. Keyword analysis showed recurring focus on “lumbar spine,” “degenerative disc disease,” and “prosthesis design”.
Conclusions
Influential LDA research has been shaped by a concentrated group of authors, institutions, and journals. While academic interest has been sustained, clinical adoption of LDA has lagged. Aligning future research efforts with clinical application may help support broader integration of motion-preserving technologies in spine surgery.
Keywords
Introduction
Lower back pain (LBP) is a common chronic disorder that is the leading cause of disability globally. 1 It affects an estimated 619 million people and is expected to impact 843 million people by the year 2050. 2 LBP can be attributed to several causes but is most often the result of structural and functional degeneration of the intervertebral disc, known as degenerative disc disease (DDD).3,4 Lumbar disc arthroplasty (LDA), also known as lumbar disc replacement (LDR), is a Food and Drug Administration (FDA) approved surgical intervention for DDD. It involves the removal of a damaged or degenerated intervertebral disc in the lower back and insertion of an artificial mechanical replacement to preserve mobility and function in the lower spine, ultimately helping to relieve LBP.
LDA is an alternative to posterior and posterolateral lumbar fusion (PLF) and lumbar interbody fusion (LIF) with distinct indications and a different perioperative risk profile. Rather than being equivalent to fusion, LDA prioritizes motion preservation and selected patient-reported outcomes, whereas fusion aims for segmental stabilization. These potential benefits must be weighed against anterior or retroperitoneal access risks and device-related complications. LIF places an implant or “cage” in the afflicted area to promote spinal stability while the vertebrae join together. Both PLF and LIF procedures limit the natural biomechanics of the spine and increase the amount of stress placed on nearby areas. Conversely, LDA replaces the degenerated disc with a prosthetic that is engineered to fit the spine’s natural height and alignment, functionally mimicking a healthy disc at the operated level. To perform this procedure, the surgeon creates a small abdominal incision. The degenerated disc is excised using an anterior approach and replaced with a synthetic implant, for which there are currently several FDA-approved models available. 5 Previous studies comparing LDA to lumbar fusion have shown that LDA is associated with lower postoperative Oswestry Disability Index (ODI) and Visual Analogue Scale (VAS) scores, indicating that it more effectively reduces disability among patients with DDD-related LBP. 6 LDA is also associated with lower risk of infection and reoperation at 90-day and 1-year follow-up. 7 However, vascular and neurological injury are still possible complications that should be monitored during and after surgery. 5
Spine health is a rapidly growing discipline that can be better understood through bibliometric analyses. Previous literature has examined conditions such as lumbar spinal stenosis and disc herniation, as well as procedures like transforaminal interbody fusion. 8 Such studies quantify patterns in top spine journals, provide valuable insight into collaboration patterns, and assess the overall landscape of global spine research. 9 In this study, we performed a bibliometric analysis of the top 100 cited articles on LDA. Our objective is to provide a thorough understanding of popular literature, authors, and concerns related to LDA that can enhance our overall understanding of lumbar spine health.
Methods
Study Design
This study utilized a bibliometric analysis to identify and evaluate the most cited literature on LDA within the fields of neurosurgery and orthopaedic surgery.
Search Strategy
The Web of Science database was used to search for documents using the search terms “lumbar disc arthroplasty” OR “lumbar disc replacement” on December 1st, 2024. Results were sorted in descending order by total citation count and independently screened for relevance.
Eligibility Criteria
Articles were included if they focused primarily on LDA or LDR in neurosurgery or orthopaedic surgery, were classified as primary research or review articles with full-text availability, published in peer-reviewed and indexed journals, and written in English. Articles were excluded if their primary focus was unrelated to LDA or LDR, if they were not peer-reviewed, or if they were not written in English.
Data Extraction
The following details were recorded from the 100 studies extracted: article title, author, journal, year of publication, total citation count, geographic origin, institution, study topic, and author keywords. Each included article was assigned to 1 primary study-design category — randomized controlled trial, prospective cohort, retrospective cohort, systematic review/meta-analysis, narrative review, basic/biomechanical/cadaveric/translational, technical/methods/reliability, case report/series, or health-economics/decision modeling — using predefined operational definitions. Two reviewers (PGM and LEM) classified articles independently, with disagreements resolved by a third-party (MKN).
Data Analysis
Descriptive statistics were used to summarize the data, while network analysis of author collaborations and keyword relationships were conducted using VOSviewer (version 1.6.20), RStudio (version 4.2.2), and the Bibliometrics Package to uncover and visualize trends within the field.
Results
The search for LDA and LDR yielded a total of 1423 articles. After filtering for peer-reviewed, full-text articles written in English, 1272 articles were included in the analysis (Figure 1). The top 100 most cited articles were selected and analyzed based on citation count. Citation totals for these articles ranged from 27 to 377, with an average of 66.6 citations per article. Identification Table for the Top 100 Articles Relevant to Lumbar Disc Arthroplasty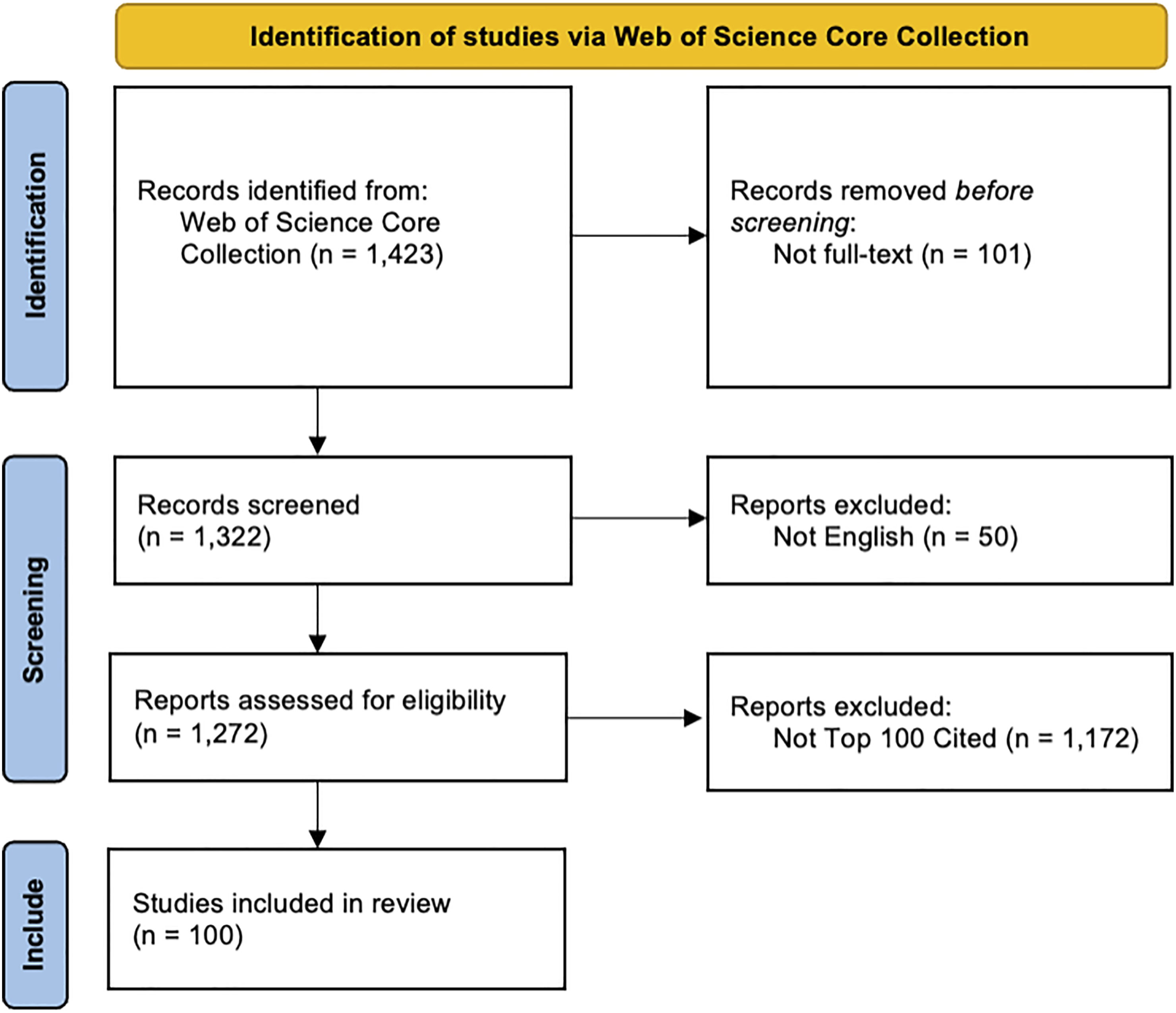
Breakdown of Article Types Among Top 100 Lumbar Disc Arthroplasty Studies
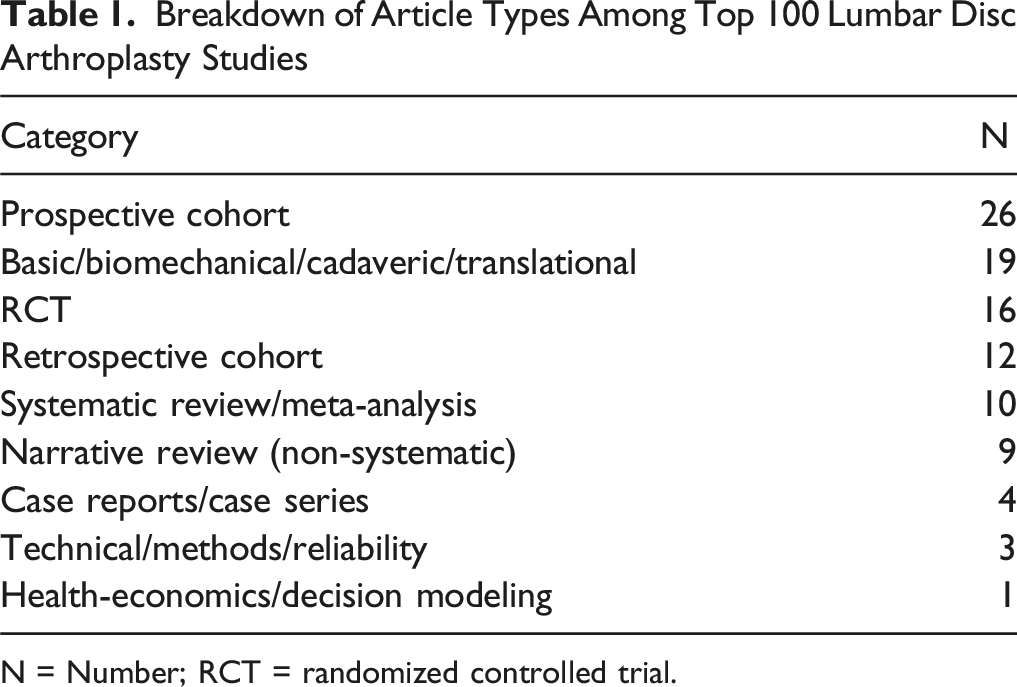
N = Number; RCT = randomized controlled trial.
Distribution of Articles by Publication Year
The top 100 articles spanned publication years from 2002 to 2018. The earliest article, “Indications for full prosthetic disc arthroplasty: a correlation of clinical outcome against a variety of indications” by Bertagnoli et al, was published in 2002 in European Spine Journal and ranked fourth in citation count. The most recent entry was a 2018 meta-analysis by Zigler et al, published in Global Spine Journal, which ranked 58th. Publication trends peaked in 2007, with 20 articles published that year. Citation averages per article increased over time: in 2002, the average was 3.92 citations per article, compared to 6.14 in 2018.
Citation Trends Over Time
Yearly citations for the top 100 LDA articles rose from near zero in 2002 to a clear peak in 2012 with 546 citations, with a secondary high in 2015 of 525 citations, followed by a gradual taper to 153 in 2023 and 191 in 2024. Publication of the top 100 articles clustered in the mid-2000s and became uncommon after 2016, consistent with the older cohort driving most citation accrual while recent entries remain sparse (Figure 2). Publication and Citation Counts Over Time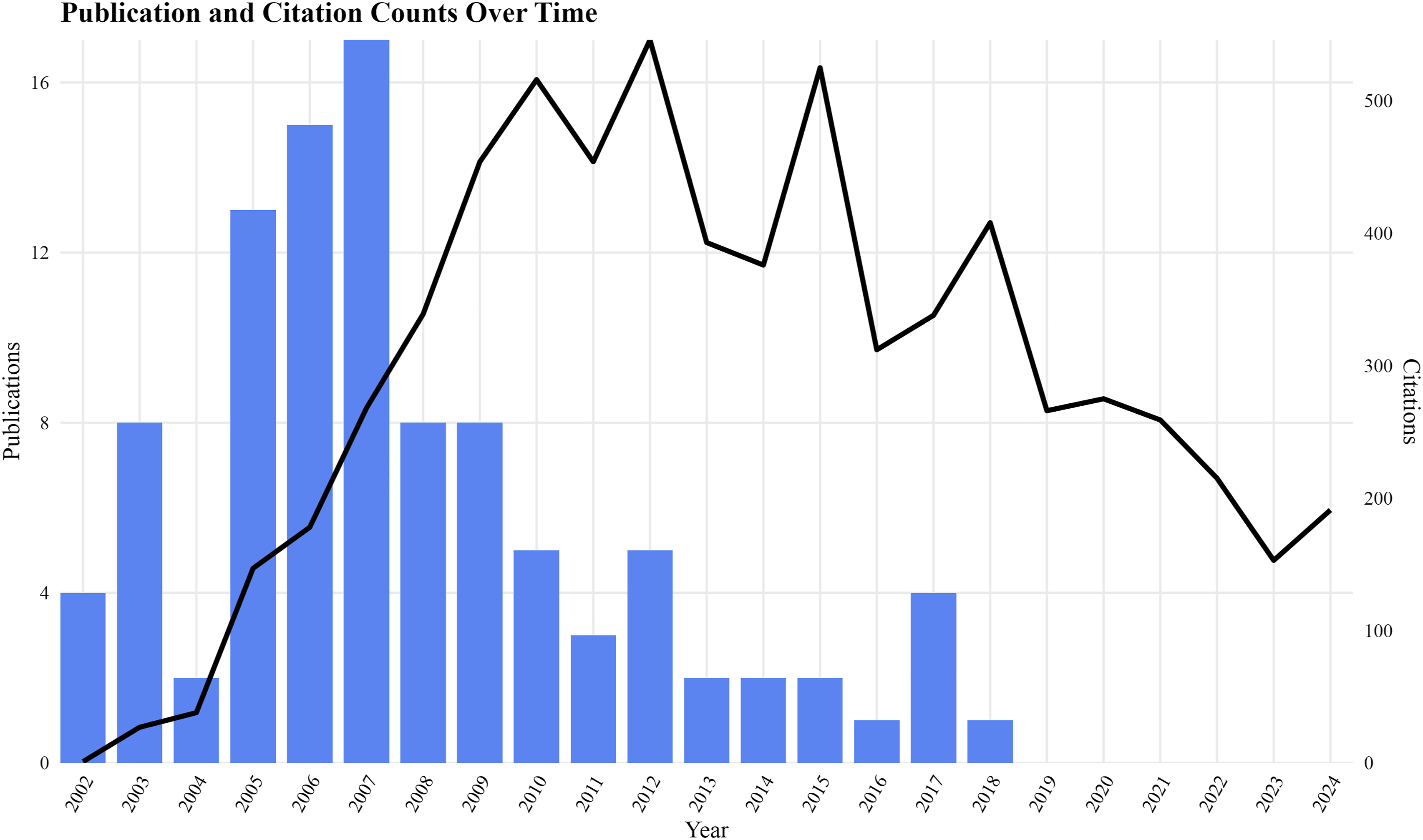
Most Cited Articles
The top-cited article was “A prospective, randomized, multicenter Food and Drug Administration Investigational Device Exemptions study of lumbar total disc replacement with the CHARITÉ™ artificial disc vs lumbar fusion” by Blumenthal et al., published in Spine in 2005, which received 377 citations. Other highly cited works included those by Zigler et al. (N = 300), Lemaire et al. (N = 181), and Bertagnoli et al. (N = 150), followed by articles by Van den Eerenbeemt (N = 148), Putzier (N = 140), David (N = 138), Schmidt (N = 117), Shim (N = 111), and Tropiano (N = 109). None of the top 10 articles had authors with multiple entries in the list (Figure 3). Top 10 Most Cited Articles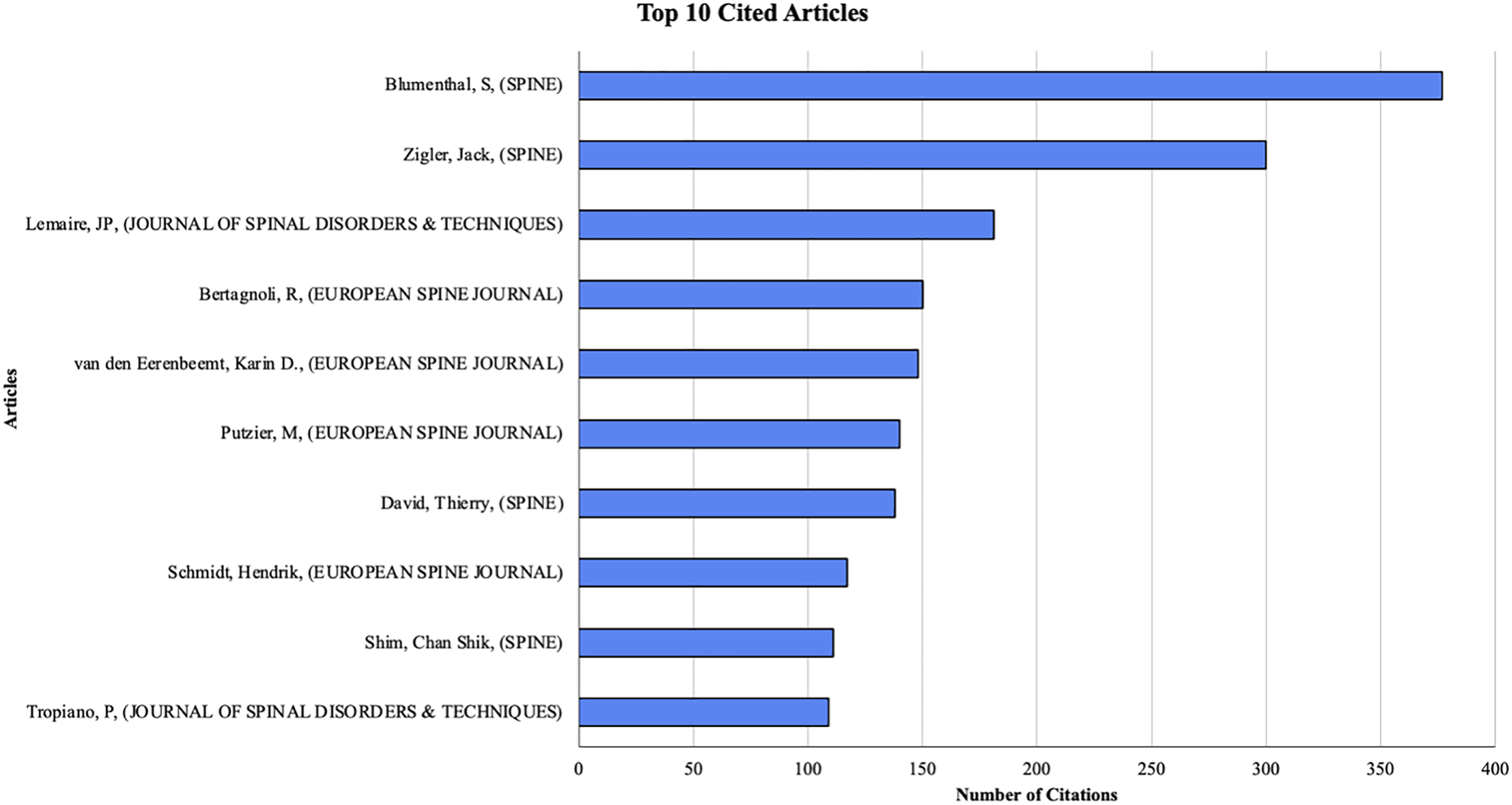
Author Productivity
Mayer HM had the most publications (N = 9), followed by McAfee PC and Siepe CJ (N = 7 each). However, none of these authors contributed to the top 10 most cited articles. Among primary authors, Siepe CJ led with 7 total entries (Figure 4). Top 10 Most Productive Primary Authors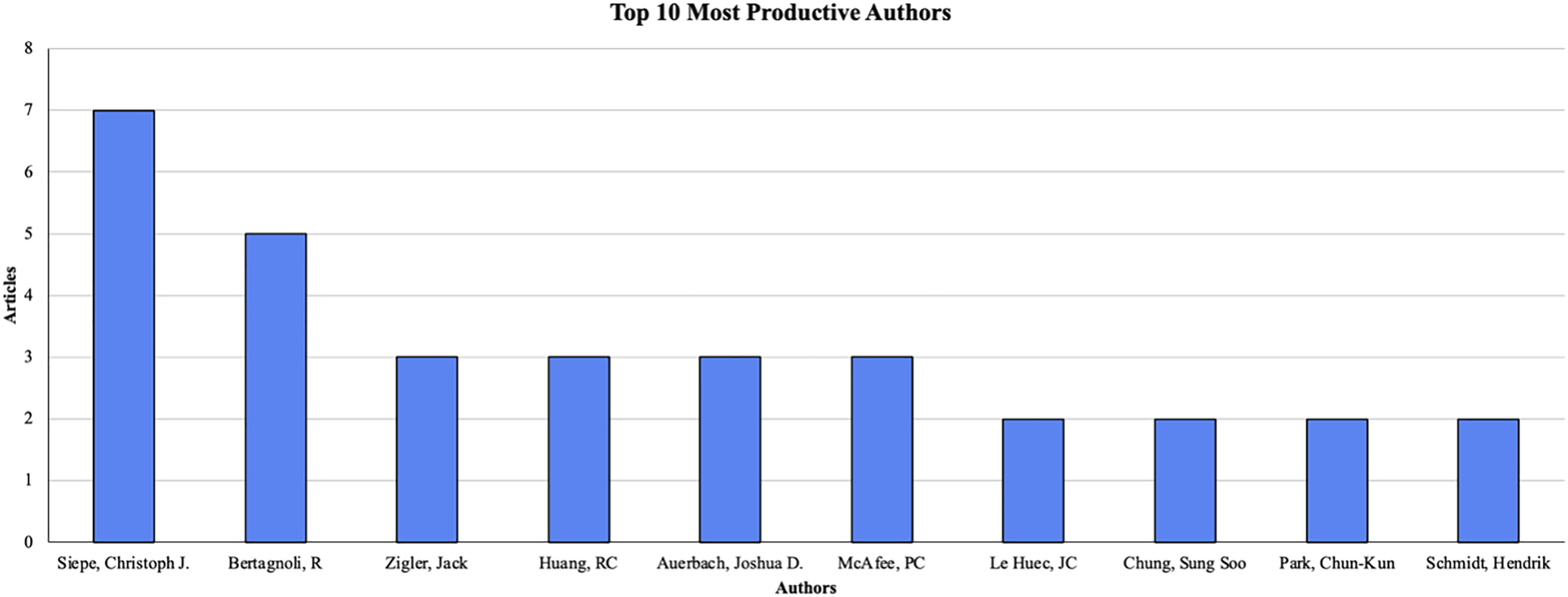
Journals and Institutional Affiliation
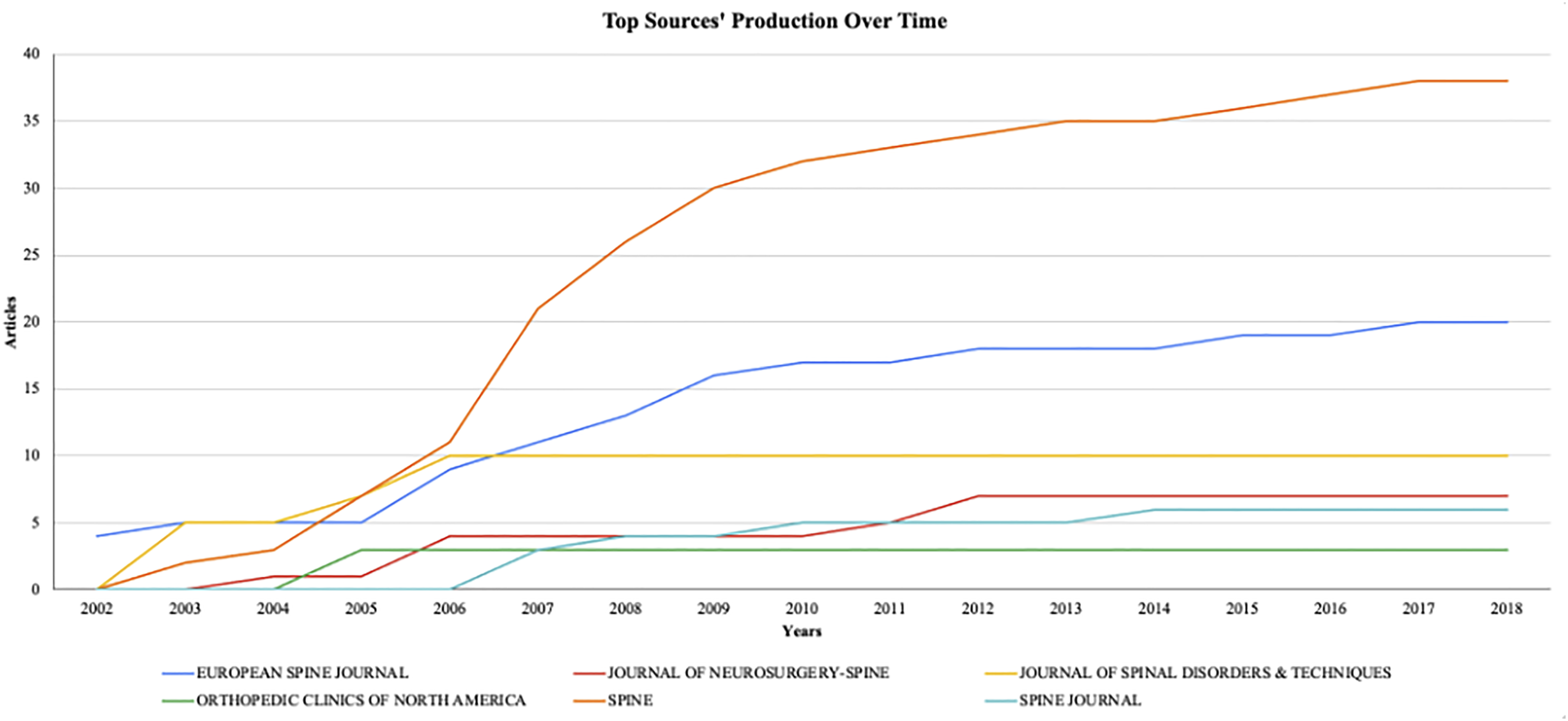
The top 100 articles appeared across 18 journals. The top 3 journals accounted for 68% of these articles: Spine (N = 38), European Spine Journal (N = 20), and Journal of Spinal Disorders & Techniques (N = 10; Figure 5). Notably, since 2005, Spine has been the leading journal publishing top-cited LDA and LDR articles. The Journal of Spinal Disorders & Techniques published its last top-cited articles between 2002 and 2006 (Figure 6). Top 10 Most Relevant Sources Top Sources’ Production Over Time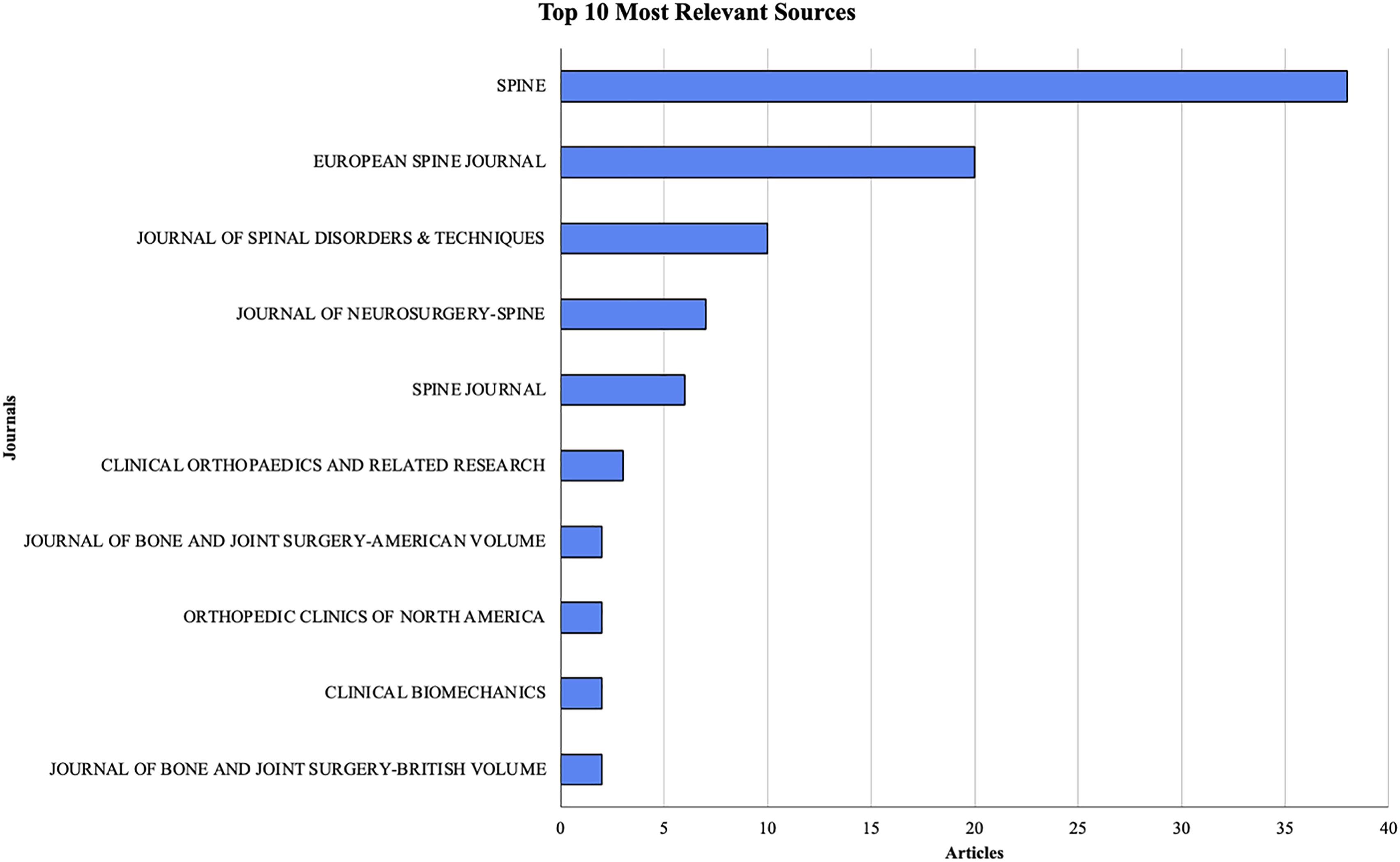
The most frequent institutional affiliations were Texas Back Institute (N = 16), Yale University (N = 16), Hospital for Special Surgery (N = 14), and Penn Hospital (N = 7; Figure 7). Top 10 Most Productive Affiliations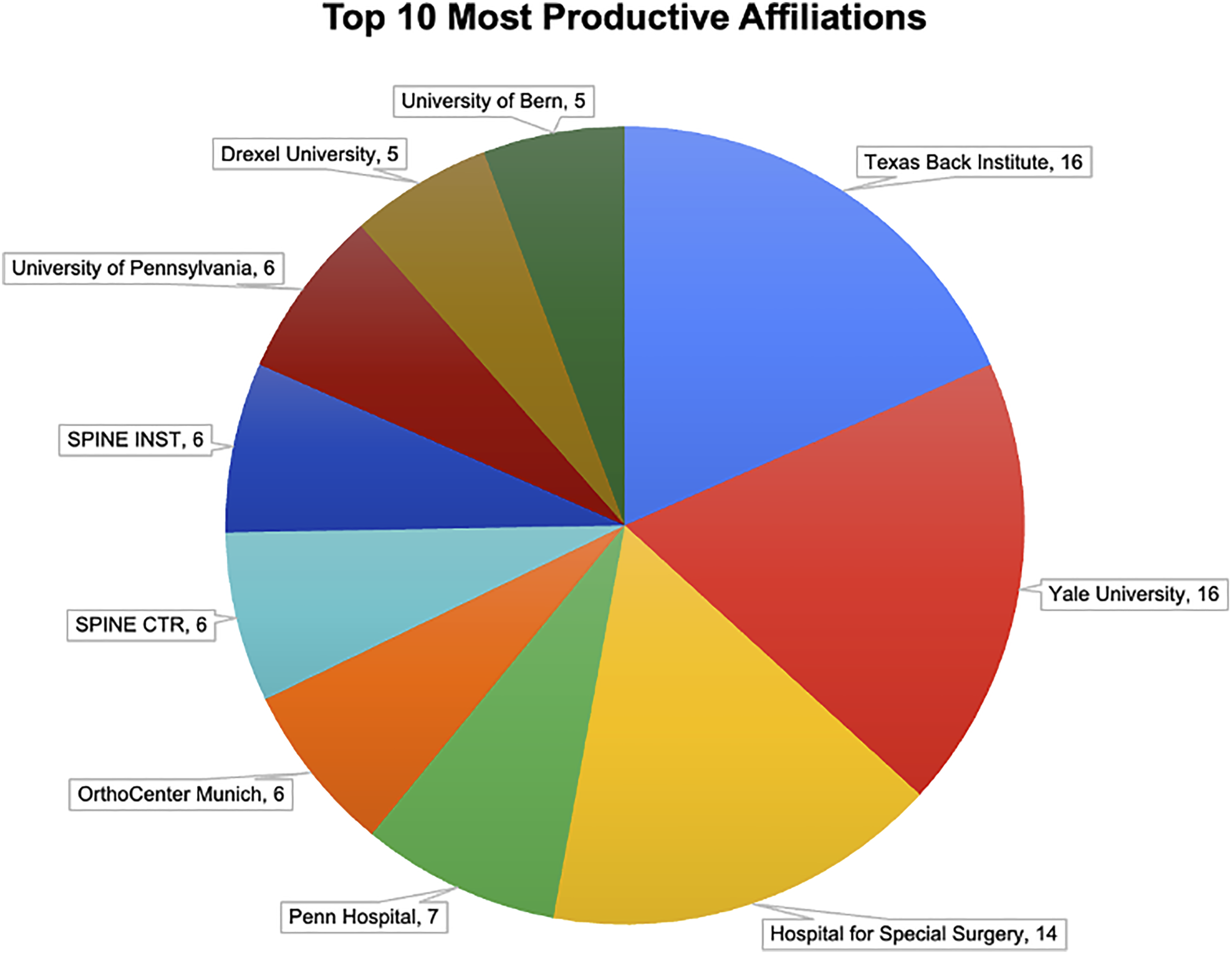
Citation Network Analysis
A citation network was constructed based on authors with 4 or more publications, resulting in 18 distinct clusters (Figure 8). Mayer HM (TLS = 596) emerged as the most central figure, frequently citing his own work (N = 48), a pattern common among senior researchers. Other prominent authors included Siepe CJ (TLS = 443) and McAfee PC (TLS = 356). Strong citation ties were observed between Mayer HM and McAfee PC (N = 39) and between Siepe CJ and McAfee PC (N = 36). Bidirectional citations between Mayer HM and Siepe CJ suggest thematic overlap or collaboration. Mayer also demonstrated inter-cluster connectivity, notably citing Girardi FP (N = 35) and Cammisa FP (N = 35). Authors With 3 or More Publications and Citation Networks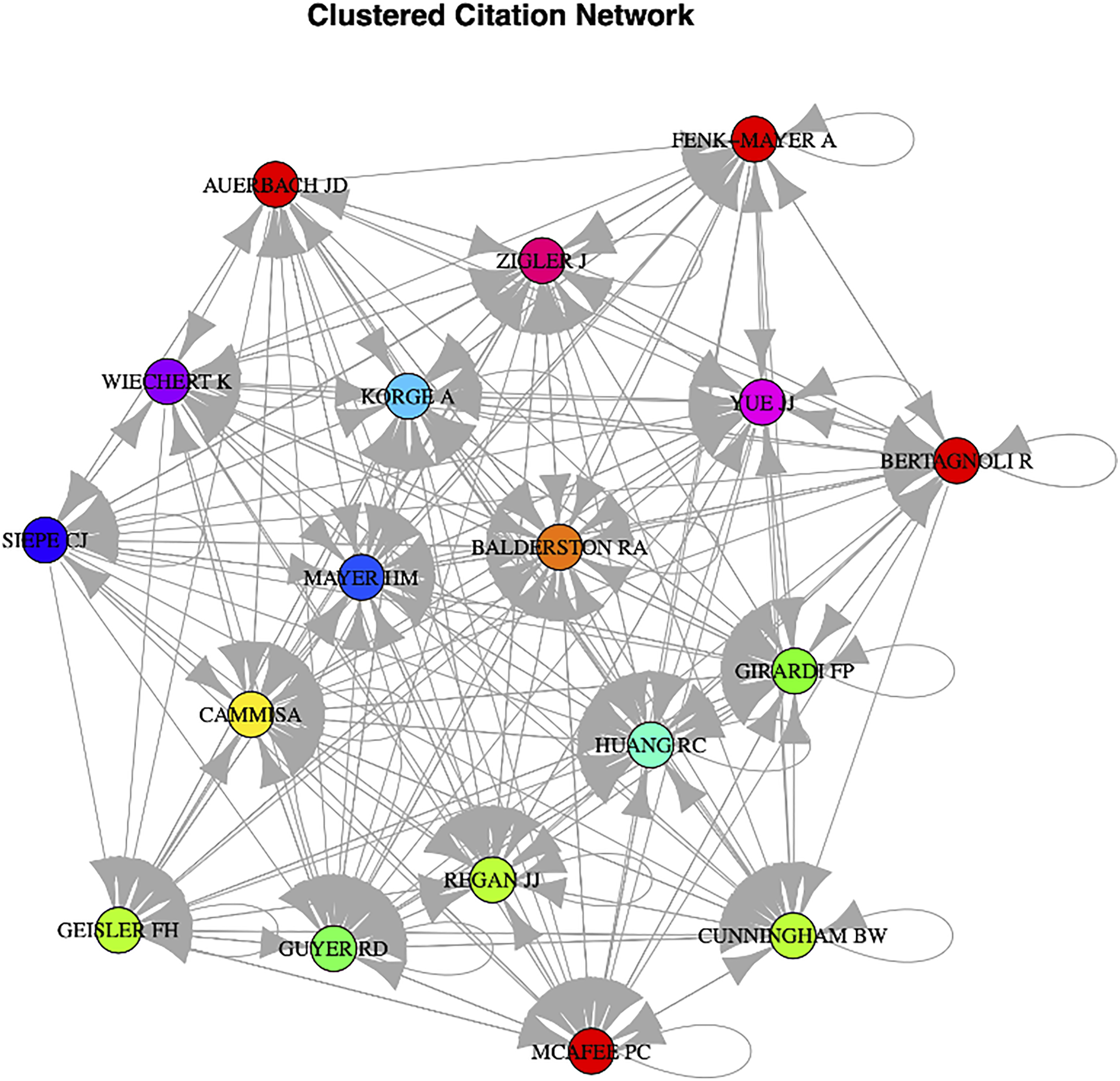
Keyword and Historical Analysis
The top 10 trending keywords were extracted to assess thematic trends in LDA and LDR research. A historical citation analysis mapped relationships among citation roots, leading authors, and research themes (Figure 9). Ten key authors were linked to seminal works and core descriptors such as “lumbar spine” and “artificial disc.” These connections illustrate how foundational studies have influenced emerging themes and show the evolution of LDA and LDR scholarship through author collaborations and conceptual continuity. Keyword Evolution and Author Citation Roots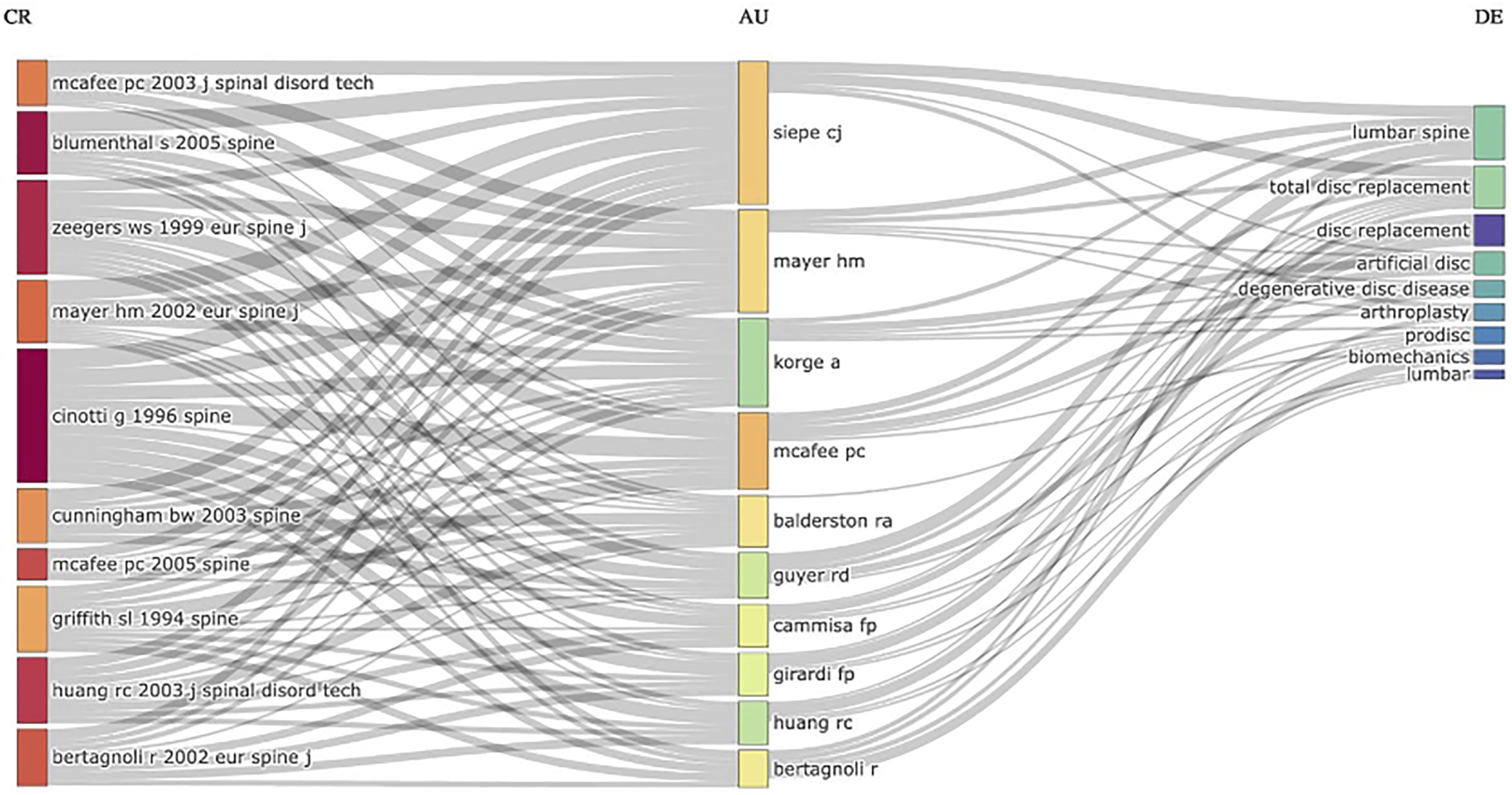
Discussion
Motion preservation has garnered significant attention in spine surgery, particularly in the cervical spine. Notably, LDA was approved 3 years prior to cervical disc arthroplasty (CDA), yet remains far less widely adopted. 10 This limited uptake persists despite high-quality studies suggesting favorable long-term outcomes.11,12 Understanding the disconnect between research attention and clinical adoption warrants a closer examination of the scientific landscape surrounding LDA. This study identified the 100 most cited articles on LDA and LDR, providing a comprehensive bibliometric profile of the field. Articles ranged from 2002 to 2018, with a publication peak in 2007 and Spine emerging as the dominant journal. Network analysis highlighted Siepe, Mayer, and McAfee as prolific contributors, while the most cited article was the FDA investigational device exemptions (IDE) trial on the CHARITÉ™ disc by Blumenthal et al. These findings reflect the foundational research and key contributors that have shaped LDA discourse over the past 2 decades.
Interestingly, although the search queried literature through December 2024, no article published after 2018 reached the top 100 by citation count. This citation lag is a well-known limitation of bibliometric research, as more recent studies have had limited time to accumulate citations. Nevertheless, this may indicate that the most influential LDA research occurred during an earlier period of clinical enthusiasm, particularly surrounding FDA approvals and initial device adoption. This interpretation is consistent, as the most cited article was a 2005 FDA IDE study by Blumenthal et al. regarding the CHARITÉ™ artificial disc device, 1 of 3 FDA-approved LDA devices — though it was later discontinued in 2012.5,13 To note, 4 main landmark trials leading to the approval of these devices — CHARITÉ™ (DePuy Synthes, Inc), ProDisc L (Centinel Spine, Inc) and activL (Aesculap USA, Inc) — were all included in our bibliometric analysis.14-16 In contrast, the most recent article to make the top 100 list — a 2018 meta-analysis by Zigler et al. 17 — signals a potential shift in the narrative. The study applied rigorous randomized controlled trial methodology to evaluate the long-term efficacy and safety of LDA, ultimately supporting its viability as a treatment option. Its relatively high citation volume despite recent publication suggests that newer studies continue to reference it favorably, potentially reinforcing its conclusions and contributing to a more optimistic outlook on LDA. The continued citation of recent high-quality studies may help reshape clinical perspectives, as growing emphasis on the long-term benefits of LDA in the literature could influence both surgical decision-making and patient care.
While early randomized and cohort studies reported favorable outcomes in carefully selected patients, LDA carries a distinct risk profile — including vascular or retroperitoneal access complications, implant wear and mechanical failure, heterotopic ossification with loss of motion, and challenging revision pathways — that likely tempered broad clinical uptake.14-16 Beyond clinical concerns, several factors help explain the paucity of recent high-impact publications, including the inherent citation lag that disadvantages newer studies in a top 100 framework, device-market changes such as discontinuations and consolidation that curtailed large sponsored trials, limited training exposure with a steeper learning curve, reimbursement and coding uncertainties, and unresolved revision strategies. Together, these headwinds reduced trial momentum and day-to-day adoption, narrowing the pipeline of contemporary studies that would otherwise accumulate citations despite early enthusiasm.
Our author network analysis revealed concentrated contributions from several key figures and institutions, most notably Mayer HM, Siepe CJ, and McAfee PC. Mayer’s central role within citation clusters — characterized by strong internal links and frequent self-citation — reflects his longstanding influence on the evolution of LDA research. Similarly, Siepe, Bertagnoli, and Zigler emerged as the 3 most productive authors based on publication count, with their work consistently contributing to the field’s most cited literature. These citation and collaboration patterns highlight how a relatively small group of researchers has shaped both the discourse and direction of the LDA literature. Mapping these networks can help identify opportunities for greater knowledge transfer, foster collaboration among research hubs, and offer insight into how academic momentum aligns with or diverges from clinical adoption trends.
Spine accounted for 38% of the most cited articles in our analysis, making it the most frequently represented journal among high-impact LDA publications. This observation is consistent with a prior bibliometric study by Yang et al., 18 which identified Spine as the leading journal for the 100 most cited articles on intervertebral discs more broadly. Although their analysis encompassed a wider range of topics beyond LDA, the finding reinforces Spine’s prominent role in disseminating influential spine research. The frequent appearance of LDA-related articles in a small group of specialized journals may reflect longstanding editorial focus, established readerships, and disciplinary alignment within the spine surgery community. This distribution lends support to Bradford’s Law, which posits that a small number of core journals in a given field account for the majority of influential publications — an observation clearly reflected in the concentration of top-cited LDA articles within Spine and a few other specialty journals. 19 Similarly, institutions such as the Texas Back Institute and Yale University were among the most frequent sources of top-cited work, underscoring the role of select academic centers in advancing LDA research. In the context of LDA’s relatively hesitant clinical adoption, this institutional concentration may shape not only the direction of academic discourse but also broader perceptions of the procedure’s legitimacy and utility in surgical practice.
Although our findings suggest sustained academic interest in LDA, these trends have not been mirrored in widespread clinical adoption. As noted in previous national database studies, LDA procedure volumes have remained stagnant or declined relative to lumbar fusion. Possible reasons include limited training exposure, reimbursement disparities, and unresolved questions regarding long-term efficacy. This disconnect raises important questions about how research attention translates — or fails to translate — into surgical practice. While our results suggest increasing interest in LDA, a large nationwide database study by Ng et al. 20 found that the absolute number of LDAs has remained constant over the last decade and the relative number, when compared to lumbar fusion (LF), has decreased. A number of potential reasons may exist for these findings, such as lower reimbursement rates for LDAs, surgeon unfamiliarity with LDA devices, and a lack of consensus regarding revision strategy. 21 There is currently no consensus regarding the long-term efficacy of LDA. Some literature suggests there is no significant clinical difference between LDA and LF, while other studies demonstrate that LDA is associated with lower costs and readmission and improved patient-reported outcome measures.22-25 Bridging this gap between academic interest and clinical practice will require not only further high-quality evidence, but also strategic efforts to address systemic barriers to adoption. As interest in motion-preserving lumbar procedures grows, aligning research priorities with practical implementation strategies will be essential to realizing the full potential of LDA in improving patient outcomes. Looking forward, device-specific registries and truly long-term follow-up, in the range of 10-20 years, are essential to confirm durability, clarify failure modes, and benchmark revision strategies — standards that transformed evidence in total joint arthroplasty.
This study is not without limitations. It relied exclusively on the Web of Science database, which, while widely used in bibliometric research, may have excluded relevant high-quality studies indexed in other databases such as Scopus or PubMed. Because citation rankings privilege older publications, our top 100 approach reflects historical influence rather than a complete account of contemporary clinical performance, and newer long-term cohorts or negative studies may be underrepresented. Additionally, citation volume does not necessarily correlate with methodological quality or clinical relevance, as it may be influenced by journal visibility, author prominence, field-specific citation behaviors, and self-citation. These factors underscore the need to interpret bibliometric findings in context, supplementing quantitative metrics with qualitative assessment of the underlying literature.
Conclusions
This bibliometric analysis provides a comprehensive overview of the most influential research in LDA over the past 2 decades. Our findings highlight a core group of authors, journals, and institutions that have shaped the academic landscape, as well as temporal trends reflecting both early enthusiasm and sustained scholarly interest. Despite this robust body of literature, clinical adoption of LDA remains limited. Understanding where research influence concentrates — and how it diverges from real-world practice — can help guide future investigations, policy considerations, and educational efforts. As interest in motion-preserving lumbar procedures continues to grow, aligning academic output with practical implementation will be critical to advancing the role of LDA in spine surgery.
Footnotes
Author Disclosures
Mitchell K. Ng has the following disclosures: VB Spine LLC (paid consultant), Stryker. Inc (paid consultant), Johnson & Johnson Ethicon Inc (paid consultant), CurvaFix Inc (paid consultant), Pacira BioSciences Inc (paid consultant), Sage Products Inc (paid consultant), Alafair Biosciences Inc (paid consultant), Next Science LLC (paid consultant), Bonutti Technologies Inc (paid consultant), Hippocrates Opportunities Fund LLC (paid consultant), and Ferghana Partners Inc (paid consultant). Afshin E. Razi has the following disclosures: 4D Motion (IP royalties), Clinical Orthopaedic Society (fiduciary officer; president; board of directors/committee member), and New York State Society of Orthopaedic Surgeons (fiduciary officer; secretary; board of directors/committee member). All other authors have no other relevant financial disclosures. The author(s) declare that there is no conflict of interest and received no financial support for the research, authorship, and/or publication of this article. No IRB approval was required for performance of this review.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.