
Abstract
Study Design
Retrospective cohort comparative study.
Objective
To investigate whether specific upper instrumented vertebra (UIV) pedicle screw characteristics—particularly screw slope (UIV SS), tip-to-endplate distance (TED), and tip-to-anterior cortex distance (TAD)—are associated with the development of upper instrumented vertebra fracture (UIVF) following adult spinal deformity (ASD) surgery.
Methods
This retrospective study included 132 patients (mean age: 68.4 years) who underwent corrective surgery from 2013 to 2022, with a minimum follow-up of 2 years. The radiographic parameters and UIV screw characteristics were analyzed. Patients were categorized into UIVF and non-UIVF groups. Logistic regression and Receiver Operating Characteristic (ROC) curve analyses were used to identify the risk factors and cutoff values.
Results
UIVF occurred in 28.8% (38/132) of the patients. Post-thoracic kyphosis (Post-TK) and TED of the upper UIV screw (Post-TEDupper) were independently associated with UIVF. Cutoff values predictive of UIVF were post-TK > 36.5° and Post-TEDupper < 6.5 mm. Patients with a TEDupper < 6.5 mm had a significantly higher incidence of UIVF (HR = 2.417, P = 0.010). Kaplan–Meier analysis showed that UIVF commonly occurred within 3 months postoperatively. Progressive reduction in TED was observed over time, particularly in the UIVF group.
Conclusion
Post- TK > 36.5° and Post-TEDupper < 6.5 mm are significant predictors of UIVF. Based on the study findings, a postoperative TED of ≥ 6.5 mm may be associated with a reduced risk, and could be considered as a potential target in surgical planning, while acknowledging the limitations of the retrospective design and the model’s moderate predictive accuracy.
Keywords
Introduction
With an aging global population, adult spinal deformity (ASD) has become increasingly prevalent among older individuals. Schwab et al 1 reported that the incidence of ASD reaches 68% among healthy adult volunteers over the age of 60 years. While some ASD cases remain asymptomatic, the majority eventually require surgical correction as the deformity progresses and the clinical symptoms worsen.
However, a systematic review conducted by Lau et al 2 highlighted that the incidence of proximal junctional kyphosis (PJK) following ASD surgery remains high, ranging from 5% to 46%, with approximately 66% of PJK cases occurring within the first 3 months postoperatively and 80% within 18 months. Moreover, Micah et al 3 reported that 35% of proximal junctional failure (PJF) cases develop within 6 months after surgery, and between 13% and 55% of these patients eventually require revision surgery.
Proximal junctional failure (PJF) is characterized by structural compromise at the junctional level, including vertebral body fractures, ligamentous injuries, and disc disruption.4-6 Notably, fractures involving the upper instrumented vertebra (UIV) within the spectrum of PJF have been associated with serious neurological complications, such as spinal cord injury (SCI) and myelopathy.4,7,8
In recent years, there has been a growing interest in the field of adult spinal deformity surgery for the optimization of internal fixation materials and proximal instrumentation techniques to reduce the incidence of PJK and PJF.9,10 The pedicle screws used at the UIV represent a critical component of proximal fixation; however, limited research has addressed the influence of UIV pedicle screw characteristics on the development of PJF.
Given this gap in the literature, we hypothesized that specific UIV pedicle screw characteristics, such as screw slope (UIV SS), tip-to-upper endplate distance (TED), and tip-to-anterior cortex distance (TAD), may have a significant impact on the occurrence of upper instrumented vertebra fracture (UIVF).
Materials and Methods
Study Population
We retrospectively reviewed 233 consecutive patients who underwent surgery for ASD at our institution between May 2013 and December 2022. ASD was defined as the presence of at least one of the following radiographic criteria: adult degenerative or idiopathic scoliosis with a coronal curvature ≥ 20°, C7 sagittal vertical axis (C7SVA) ≥ 50 mm, pelvic tilt (PT) ≥ 25°, and/or thoracic kyphosis (TK) ≥ 60°. 11 All patients with ASD in this cohort had failed to respond to conservative treatment, which included at least 6 months of physical therapy, NSAIDs, or epidural steroid injections.
Surgical Procedure
All patients underwent spinal corrective fusion surgery. Two surgical approaches were employed based on the curve characteristics: For harmonic and relatively flexible curves, first, in the lateral decubitus position, multilevel lateral lumbar interbody fusion (LLIF) was performed via an anterior approach from L1/2 to L5/S1. This was followed by repositioning the patient to the prone position for multilevel posterior column osteotomies (PCO) and posterior instrumented corrective fusion (PSF). For sharp and relatively rigid curves, a 3-column osteotomy was performed at the sagittal apex, followed by PSF.
The inclusion criteria were as follows: (1) age ≥ 40 years, (2) a minimum follow-up period of 2 years, (3) a pedicle screw diameter of 5.5 mm, and a length of more than 35 mm at the upper instrumented vertebra (UIV), and (4) instrumented fusion extending from T9/T10 to the pelvis, with pelvic fixation achieved using S2-alar-iliac (S2AI) screws.
The exclusion criteria were as follows: (1) use of prophylactic techniques (eg, transverse process hooks, vertebroplasty, or tapers) at the UIV or UIV+1 levels; (2) incomplete radiographic data within 2 years; (3) spinal deformity secondary to neuromuscular disease or spinal infection; and (4) malpositioned screws, defined as screw cutout to outside at the UIV level, which was subsequently confirmed by postoperative imaging.
Upper Instrumented Vertebral Fracture (UIVF) Definition
The primary outcome was UIVF, defined as a morphological change > grade 2 at UIV or UIV+1 (Genant classification) 12 or requiring revision for SCI or myelopathy. Patients were divided into UIVF and N-UIVF (no upper instrumented vertebra fracture) groups, with time to UIVF and reoperation recorded over a 2-year follow-up period.
Data Collection
The following patient characteristics were assessed: sex, age, height, weight, body mass index (BMI), preoperative use of teriparatide and bone mineral density (BMD). Osteoporosis was defined as a T-score < −2.5. Surgical parameters included the use of posterior column osteotomy (PCO), three-column osteotomy (grades 3, 4, 5), 13 operative time (OPT), and estimated blood loss (EBL). BMD was measured using dual-energy X-ray absorptiometry (DEXA) of the total proximal femur and reported as a T-score.
Radiographic Measurements
Whole-spine radiographs were obtained using 36-inch cassettes in the standing position. Three experienced spinal surgeons, blinded to the study design, independently measured radiographic parameters using the PACS system (Centricity RIS/PACS, GE Healthcare), and the average of their measurements was used for the analysis. Spinopelvic parameters were assessed at 3 time points: preoperatively (Pre-), postoperatively (Post-), and at the final follow-up (F, ≥2 years after surgery). Parameters included C7SVA, thoracic kyphosis (TK), lumbar lordosis (LL), pelvic incidence (PI), pelvic tilt (PT), sacral slope (SS), T1 pelvic angle (T1PA), and T1 slope (T1S).
UIV screw characteristics were evaluated at the same intervals and included: (1) screw slope (UIV SS), the angle between the screw axis and the upper endplate; (2) tip-to-endplate distance (TED), the perpendicular distance from the screw tip to the upper endplate; and (3) tip-to-anterior cortex distance (TAD), and the horizontal distance from the screw tip to the anterior vertebral margin. The most cranial and caudal screws on the sagittal radiographs were labeled as “upper” and “lower,” respectively. The measurements are shown in Figure 1. Measurements of UIV Screw-Related Parameters. (UIV: Upper Instrumented Vertebra; (a) UIV SS: UIV Screw Slope; (b) TED: Tip-to-Endplate Distance; (c) TAD: Tip-to-Anterior Cortex Distance)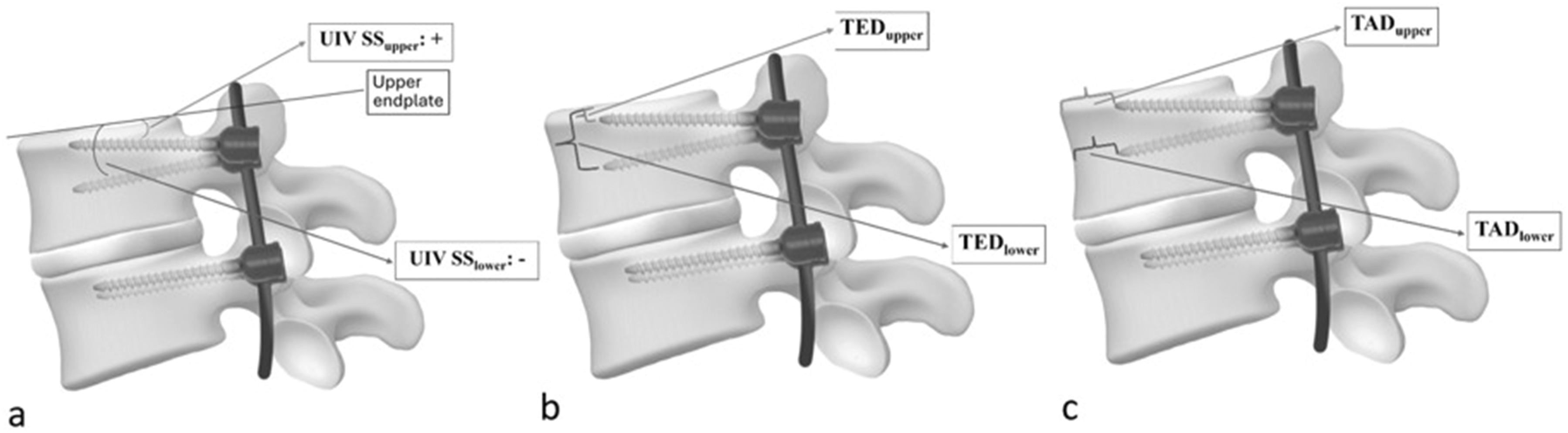
Statistical Analyses
Categorical variables were compared using the chi-square test, whereas continuous variables were analyzed using t-tests or rank-sum tests based on distribution. The inter-rater reliability of UIV screw measurements was excellent (ICC = 0.950). Binary logistic regression was performed to identify the risk factors for UIVF using variables with a significance level of ≤ 0.05 in the univariate analyses to include all potential confounders. The receiver operating characteristic (ROC) curve is plotted with sensitivity on the y-axis and 1-specificity on the x-axis. The Youden Index is defined as sensitivity + specificity – 1. The optimal cutoff value, which minimizes both false positives and false negatives, is determined based on the maximum Youden Index. The optimal cutoff value was used to generate Kaplan–Meier curves and hazard ratios. Statistical significance was set at P-value ≤ 0.05. All analyses were conducted using SPSS v23, and figures were created using GraphPad Prism 10.
Results
Demographic Data
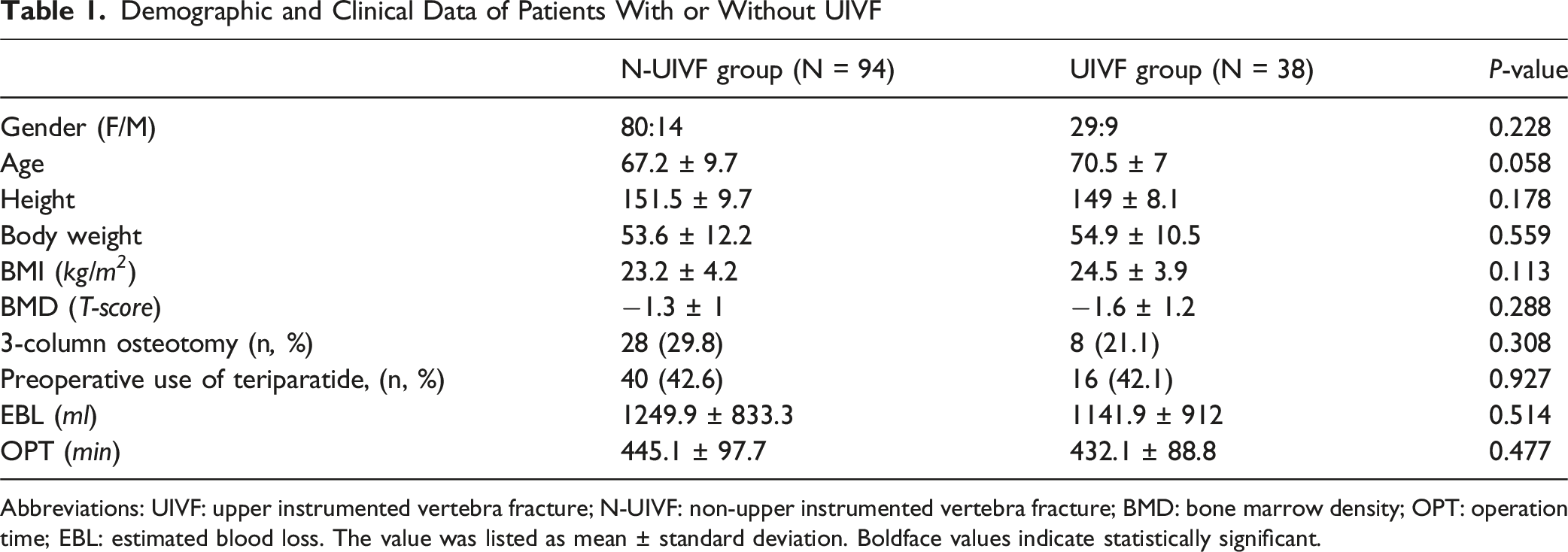
As illustrated in Figure 2, 101 patients were excluded for the following reasons: use of prophylactic techniques (20 patients), incomplete radiographic data (43 patients), neuromuscular disease (30 patients), spinal infection (5 patients), and malpositioned screws at the UIV level (3 patients). Finally, 132 patients met the inclusion criteria and were included in the final analysis. Among these, 38 patients (28.8%) were classified into the UIVF group, and the remaining 94 patients (71.2%) were classified into the N-UIVF group. The mean age was 70.5 ± 7.0 years in UIVF group and 67.2 ± 9.7 years in N-UIVF group (P = 0.058). There were 29 female patients (76.3%) in the UIVF group and 80 female patients (85.1%) in the N-UIVF group (P = 0.228). In the N-UIVF group, 28 patients (29.8%) underwent 3-column osteotomy, whereas in the UIVF group, 8 patients (21.1%) received the same procedure. The proportion of patients receiving preoperative teriparatide was 40 cases (42.6%) in the N-UIVF group and 16 cases (42.1%) in the UIVF group. There were no significant differences in demographics among these groups preoperatively (Pre-), including sex, age, BMI, BMD, presence of 3-column osteotomy, preoperative use of teriparatide, EBL, and OPT. The detailed data are listed in Table 1. Flow Diagram Illustrating Patient Recruitment and Grouping in the Study Demographic and Clinical Data of Patients With or Without UIVF Abbreviations: UIVF: upper instrumented vertebra fracture; N-UIVF: non-upper instrumented vertebra fracture; BMD: bone marrow density; OPT: operation time; EBL: estimated blood loss. The value was listed as mean ± standard deviation. Boldface values indicate statistically significant.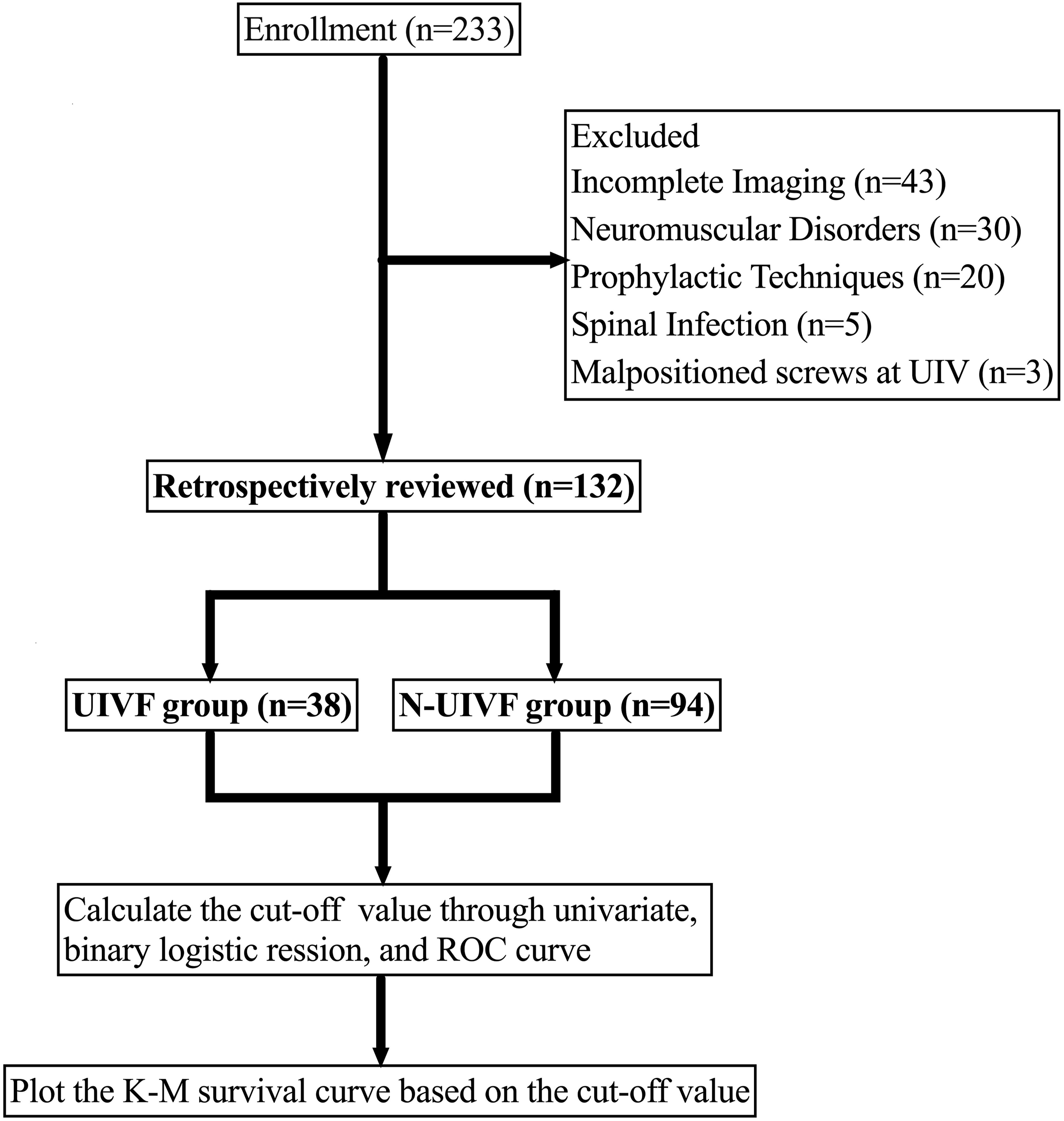
Analysis of Risk Factors for UIVF
Comparison of Radiographic Parameters Between UIVF and N-UIVF Groups Before and After Surgery
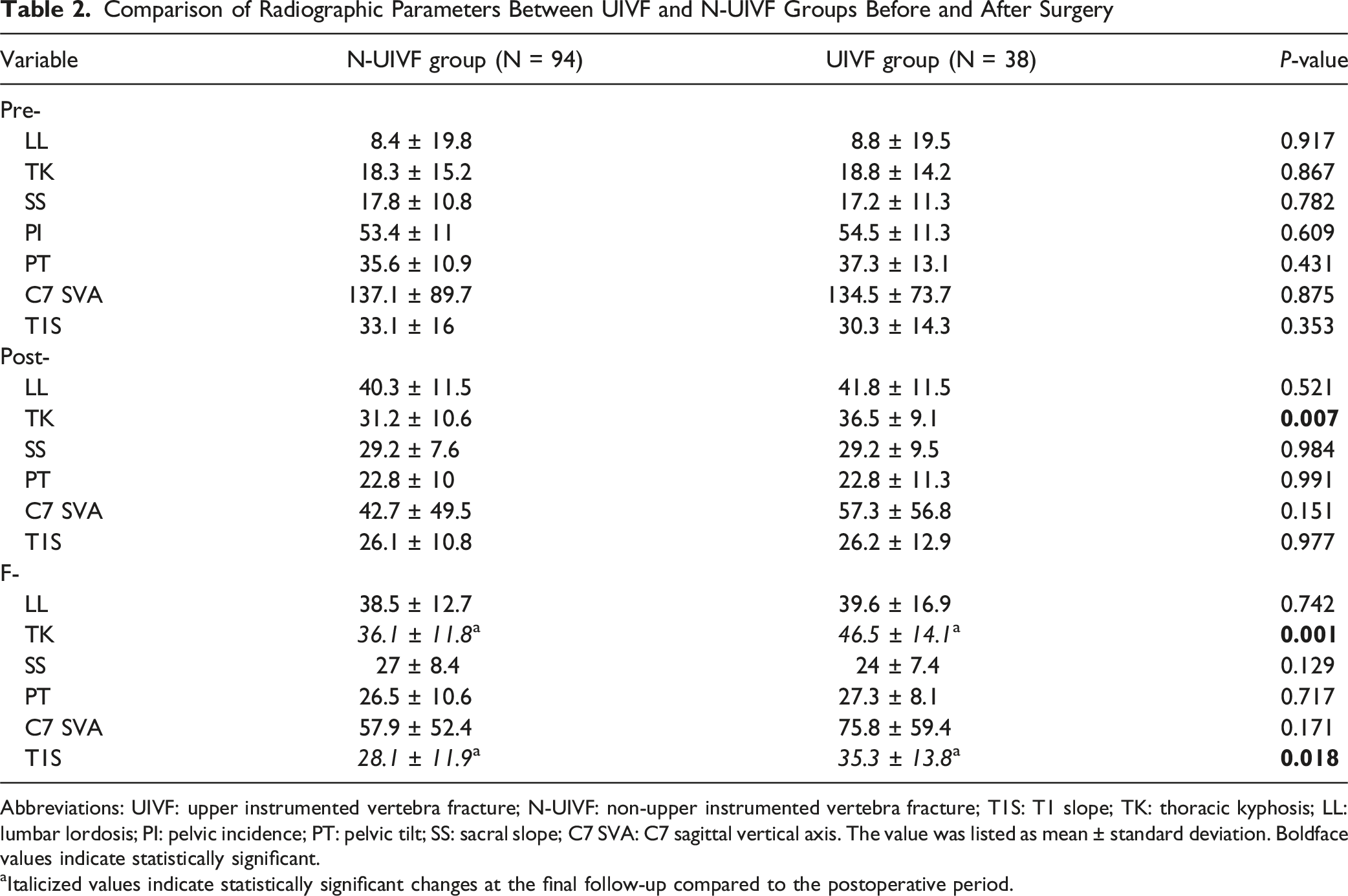
Abbreviations: UIVF: upper instrumented vertebra fracture; N-UIVF: non-upper instrumented vertebra fracture; T1S: T1 slope; TK: thoracic kyphosis; LL: lumbar lordosis; PI: pelvic incidence; PT: pelvic tilt; SS: sacral slope; C7 SVA: C7 sagittal vertical axis. The value was listed as mean ± standard deviation. Boldface values indicate statistically significant.
aItalicized values indicate statistically significant changes at the final follow-up compared to the postoperative period.
Comparison of Postoperative (Post-) and Two-Year Follow-Up(F-) UIV Screw Parameters Between UIVF and N-UIVF Groups
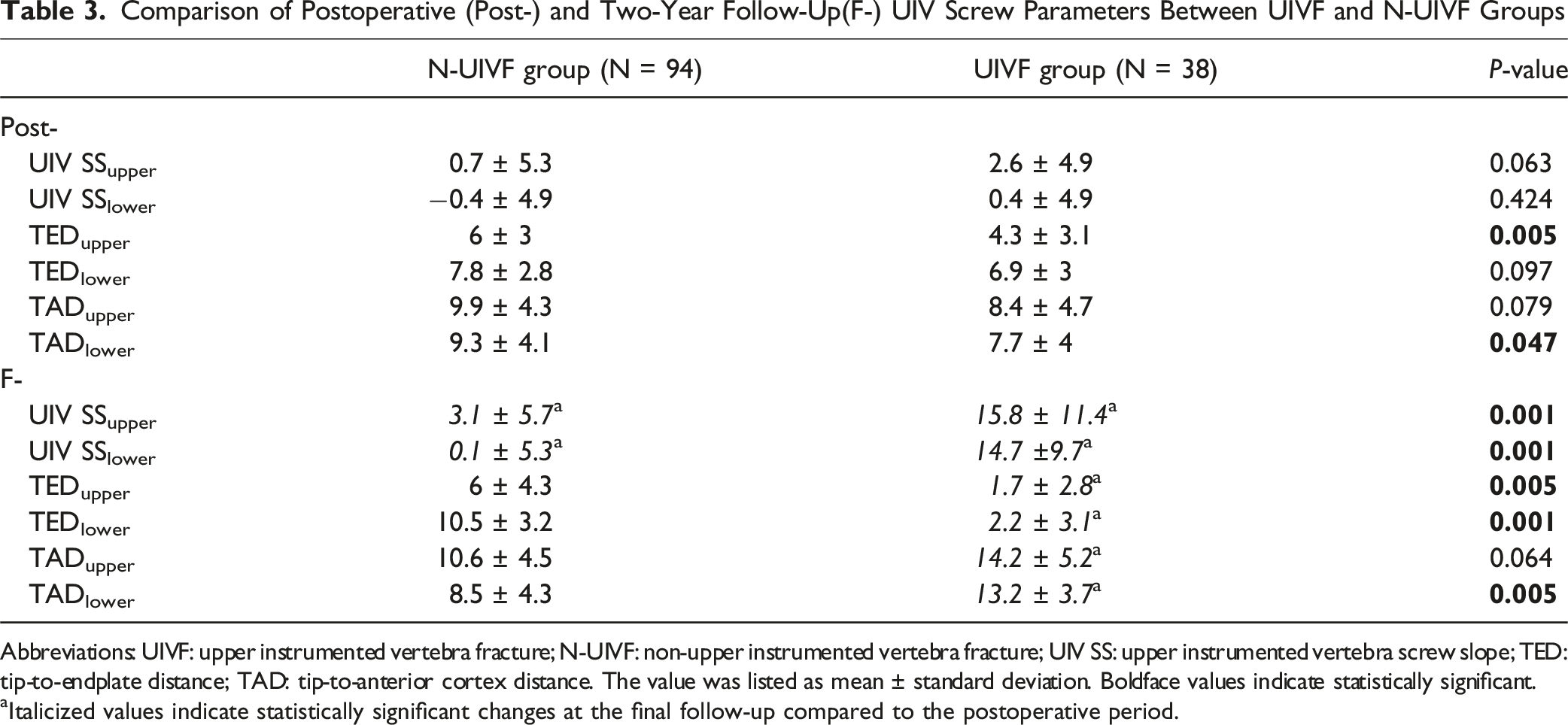
Abbreviations: UIVF: upper instrumented vertebra fracture; N-UIVF: non-upper instrumented vertebra fracture; UIV SS: upper instrumented vertebra screw slope; TED: tip-to-endplate distance; TAD: tip-to-anterior cortex distance. The value was listed as mean ± standard deviation. Boldface values indicate statistically significant.
aItalicized values indicate statistically significant changes at the final follow-up compared to the postoperative period.
Cutoff Values for UIVF
Risk Factors of Postoperative UIVF Based on Logistic Regression and Receiver Operating Characteristic Curve
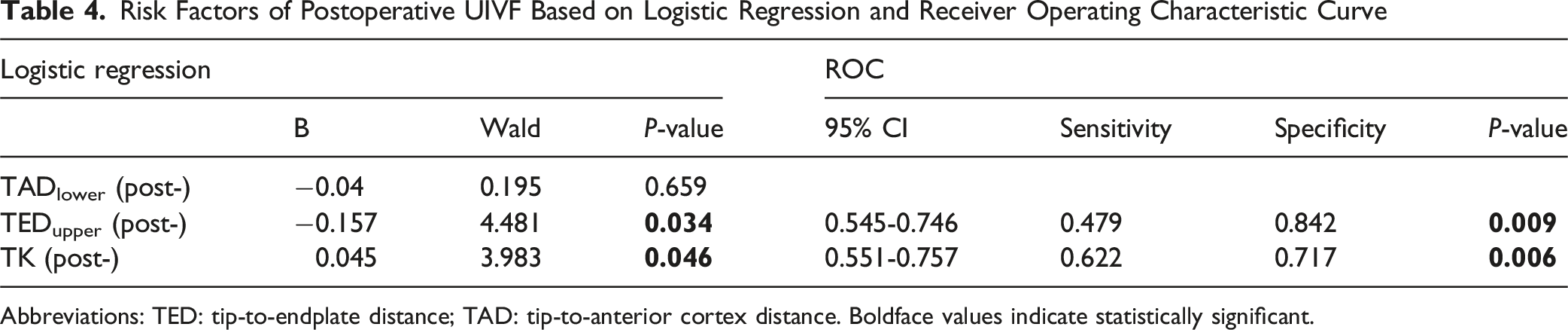
Abbreviations: TED: tip-to-endplate distance; TAD: tip-to-anterior cortex distance. Boldface values indicate statistically significant.
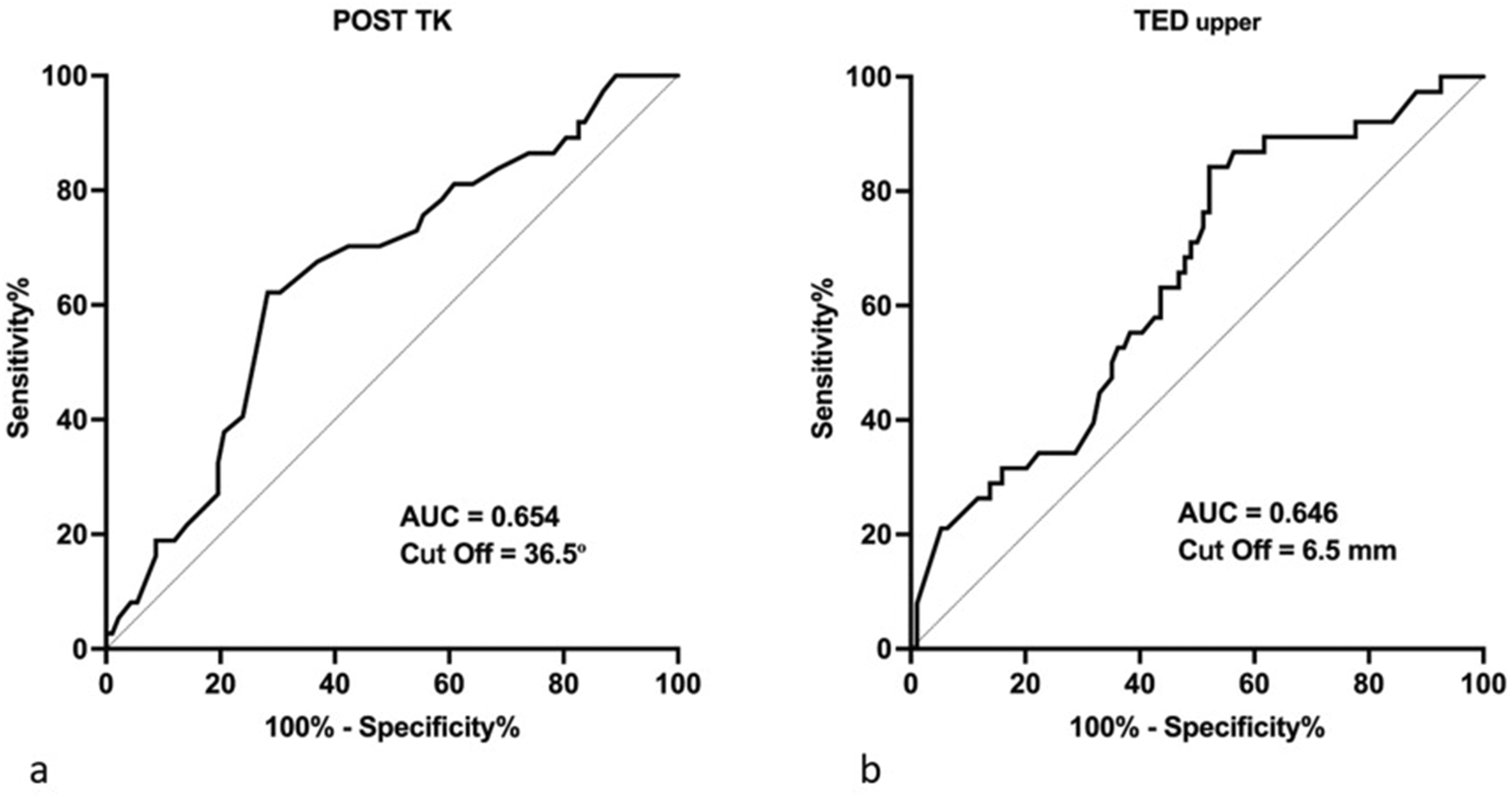
ROC Curve Analysis of Postoperative (b) TEDupper and (a) TK in Predicting the Occurrence of UIVF. (AUC: Area Under the Curve)
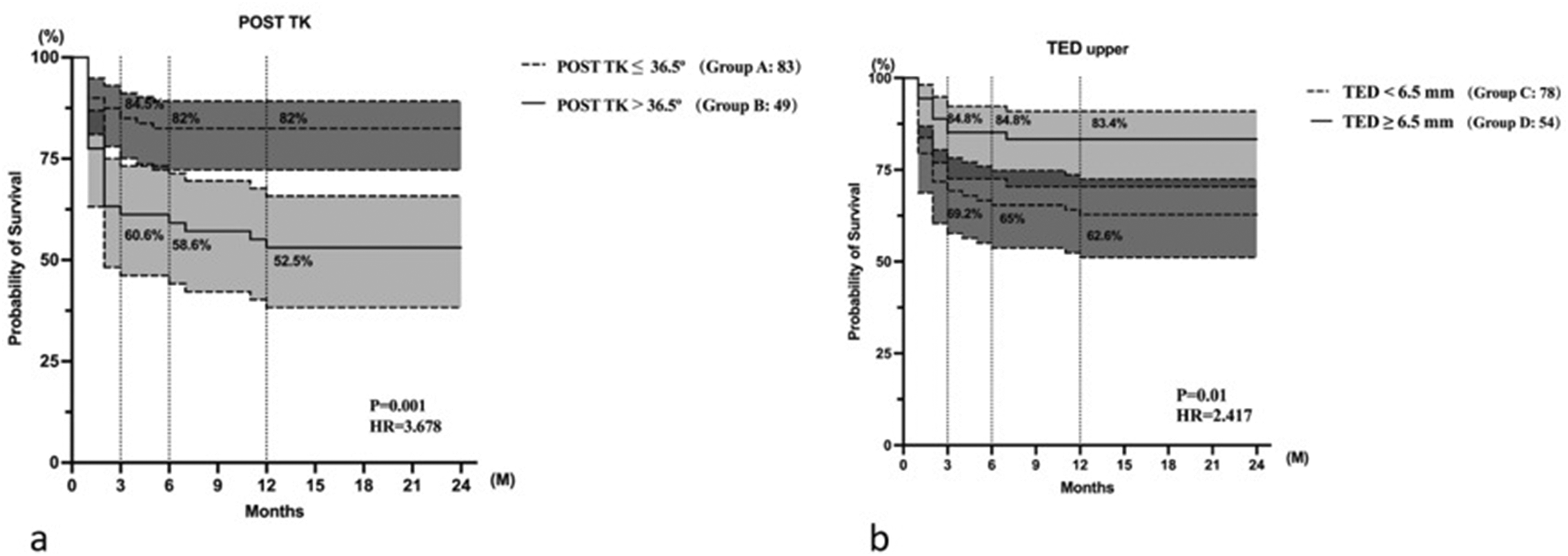
Kaplan–Meier Survivorship Curve Comparing the UIVF-Free Survival Time Among the (A) Group A vs B, for Post-TK; (B) group C vs D, for Post-TEDupper. (UIVF: Upper Instrumented Vertebra Fracture)
Case Illustration
Figure 5A shows the case with Post-TEDupper < 6.5 mm. She was a 75-year-old woman with a spinal kyphoscoliosis deformity. The fusion range was T10 to the pelvis, with TK of 34.1°. The measured TEDupper was 3.05 mm. UIVF occurred 8 months after surgery, and spinal cord injury due to UIVF was also noted. The patient underwent revision surgery for extended fixation. Figure 5B shows the case with Post-TEDupper ≧ 6.5 mm. She was a 73-year-old woman with a spinal kyphoscoliosis deformity. The fusion range was T9 to the pelvis with measured TEDupper was 8.30 mm. The sagittal alignment was well maintained without UIVF after postoperative 6 months and 2 years. (A) A 75-Year-Old Woman had a Spinal Kyphoscoliosis Deformity. (a) Fusion Range was T10 to Pelvis With TK 34.1°. (b) The Measured TEDupper was 3.05 mm. (d) UIVF Occurred 8 Months After Surgery, and (c) The Spinal Cord Injury was Also Noted. (e) Then She Underwent Revision Surgery for Extended Fixation; (B) a 73-Year-Old Woman With a Spinal Kyphoscoliosis Deformity. (a) The Fusion Range was T9 to the Pelvis With Measured TEDupper was 8.30 mm. (b) The Sagittal Alignment was Well Maintained Without UIVF After Postoperative 6 Months and (c) 2 Years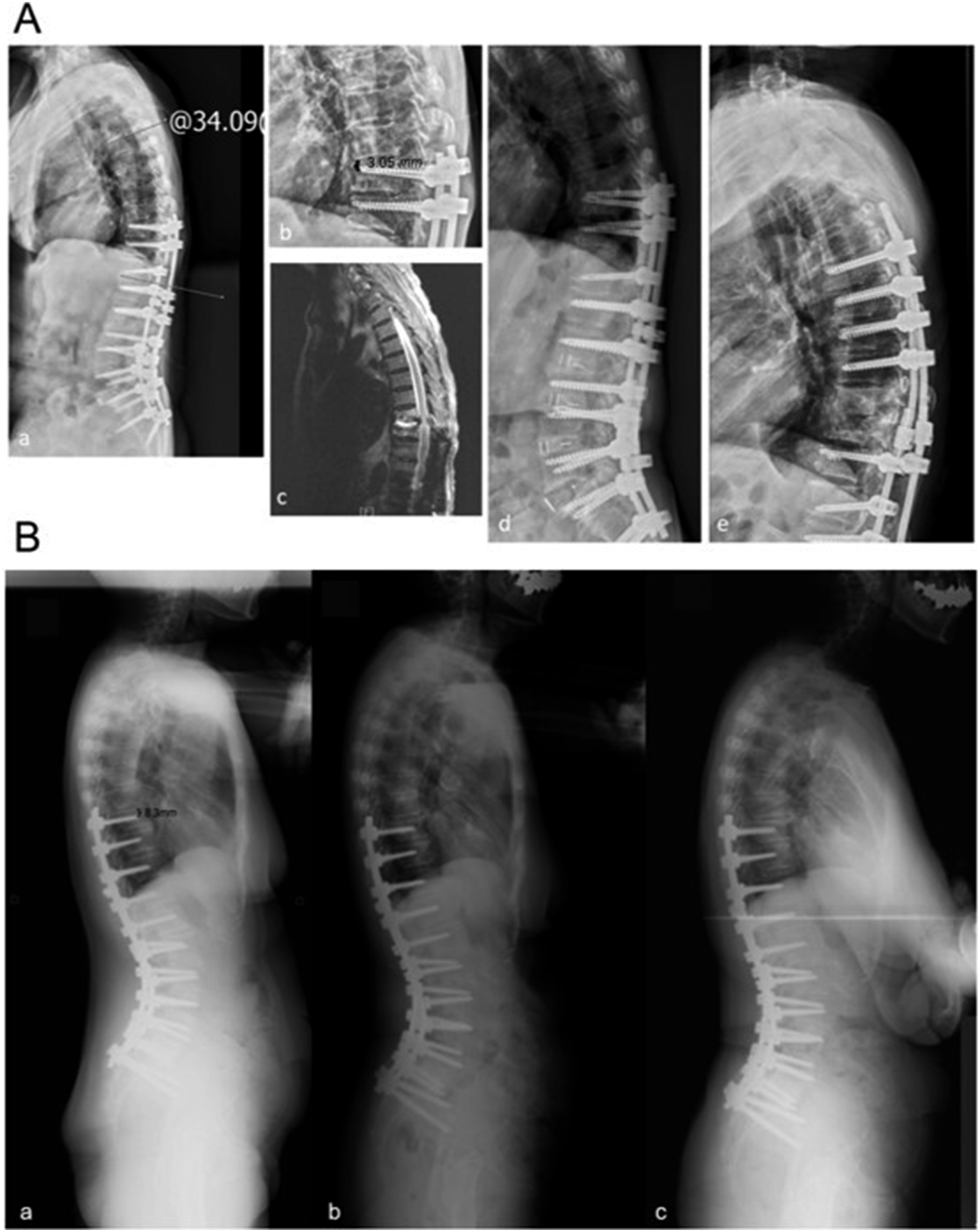
Discussion
Although numerous studies have explored the etiology of PJK/PJF, the underlying causes remain inconclusive and no definitive preventive strategies have been established. In recent years, emerging research has focused on instrumentation placement at the UIV, including factors such as the mismatch between the proximal spinal curve and rod contour, as well as cranially directed UIV screw angles relative to the superior endplate of the UIV.14-16 However, the association between the other characteristics of UIV pedicle screws and the development of UIVF remains inconclusive. Pedicle screws remain the most widely used method of internal fixation in spinal surgery because of their superior mechanical strength, which contributes significantly to deformity correction and fusion stability. Given that surgeons can control both the trajectory and length of pedicle screw placement, investigating the impact of UIV screw characteristics on UIVF has potential clinical relevance. Such insights may inform surgical strategies and aid in preventing postoperative UIVF. In this study, we analyzed the relationship between various UIV screw characteristics, including UIV screw slope (UIV SS), tip-to-endplate distance (TED), tip-anterior cortex distance (TAD), and UIVF. Previous biomechanical studies and finite element analyses have typically evaluated pedicle screw insertion angles as categorical variables, which are generally classified into 3 groups: caudally directed, parallel to the endplate, and cranially directed.17-19 In addition to quantifying the UIV SS, the present study also measured UIV TED and UIV TAD to account for potential confounding factors, such as damage to the upper endplate or anterior vertebral wall.
Bivariate logistic regression analysis revealed that both Post-TEDupper and Post-TK were associated with UIVF development. Specifically, increased Post-TK and reduced Post-TEDupper were identified as independent risk factors of UIVF in patients undergoing surgery for ASD. ROC curve analysis further identified that Post-TK >36.5° and Post-TEDupper < 6.5 mm were strong predictors of UIVF. These findings suggest that (1) larger postoperative reciprocal changes in TK and (2) a reduced distance between the pedicle screw tip and the upper endplate correlate with a higher likelihood of postoperative UIVF.
In this study, the impact of Post-TK on UIVF aligns with the findings reported in previous research.20,21 Lo et al 20 observed that significant postoperative alignment changes can occur in unfused thoracic segments following staged corrective surgery for ASD. These reciprocal changes in thoracic kyphosis (TK RCs) have been associated with the development of PJK/PJF and unfavorable clinical outcomes. Similarly, Lafage et al 21 reported that patients in the postoperative “unfavorable reciprocal change” group exhibited a greater increase in TK, with a mean Post-TK angle of 36 ± 13°. Based on these studies, the findings of the present study are consistent with existing literature. We recommend that when Post-TK exceeds the established cutoff values in corrective surgery for ASD, efforts should be directed toward optimizing the sagittal alignment distribution to mitigate the risk of junctional complications.
Possible explanations for the influence of Post-TEDupper on UIVF are as follows. From a biomechanical standpoint, UIVF is believed to result from accelerated degeneration of adjacent segments secondary to increased proximal junctional stress.22,23 A reduced distance between the pedicle screw tip and superior endplate may elevate local stress concentrations at the proximal fixation construct. Moreover, a decreased Post-TEDupper may increase the risk of endplate violation and subsequent adjacent segment degeneration (Figure 6). When the UIV pedicle screw is oriented toward the superior endplate, the reduction in the distance between the screw tip and endplate causes the applied stress to align with the screw axis and act directly on the superior endplate. This may induce cumulative microdamage under compressive forces, ultimately contributing to adjacent segment degeneration.
24
The Central Region of the Superior Vertebral Endplate is More Depressed Compared to its Periphery. When TED < 6.5 mm, (B) The Screw Tip May Appear Intact on Sagittal View but can (A) Subtly Breach the Centrally Depressed Superior Endplate, Risking Irreversible Structural Damage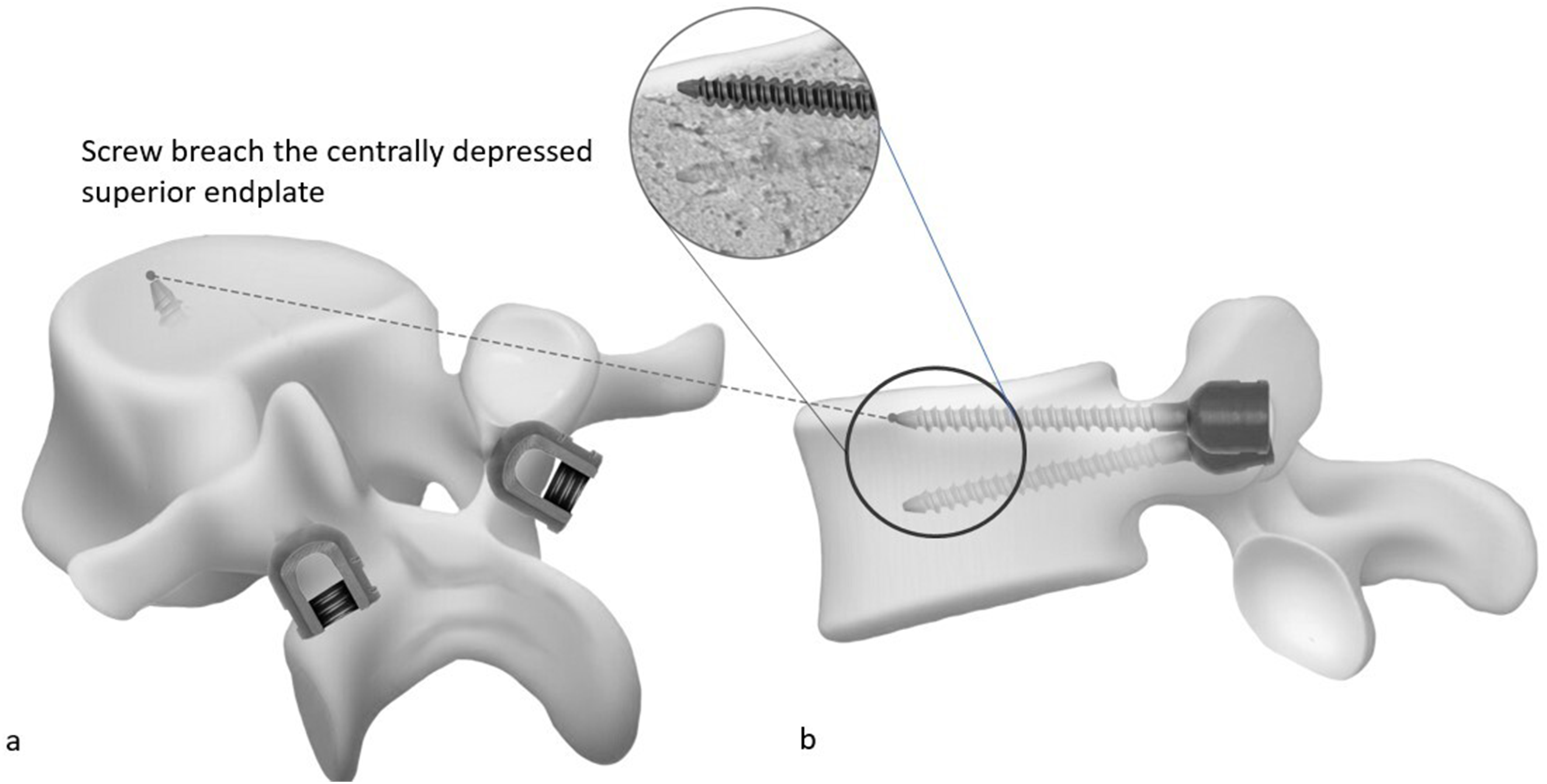
Furthermore, TEDupper and TEDlower may vary over time. Our study demonstrated a significant decrease in both TEDupper and TEDlower at the final follow-up compared to the immediate postoperative period (P < 0.001) in the UIVF group. This suggests a progressive reduction in the distance between the screw tip and endplate, accompanied by a gradual increase in adjacent segment stress. Therefore, maintaining a larger TED for the UIV screw may help prevent adverse events, such as screw cutout and endplate violation during follow-up. It is crucial to avoid an excessively small TED for the UIV screws. However, achieving a TED greater than 6.5 mm for both UIV screws can be technically demanding owing to the narrow anatomical margin. Thus, the use of an intraoperative navigation system may facilitate optimal screw positioning and help ensure adequate TED, potentially reducing the risk of postoperative complications.
At 3 months postoperatively, 39.4% of patients in group B and 30.8% of patients in group C experienced UIVF, which aligns with the findings of previous reports.25,26 As illustrated in Figure 4, the Kaplan–Meier curve showed a marked deceleration in the decline beyond the 3-month postoperative period. Therefore, vigilant surveillance for UIVF is crucial within the first 3 months after surgery. At 12 months postoperatively, the risk of new-onset UIVF was minimal.
Previous literature has reported results that closely align with our study. In the work by Qiu et al, 27 it was observed that the insertion of UIV pedicle screws in a cranial direction significantly increased the likelihood of developing PJK and PJF in adult patients with de novo degenerative lumbar scoliosis. Supporting this, Lu et al 28 reported that a UIV screw angle exceeding 1° served as a strong indicator for the onset of these complications. Based on these findings, angling the UIV screw downward may be a key strategy to reduce adverse outcomes such as screw cutting and junctional failure during long-term follow-up.
However, in the present study, the cutoff values for Post-TEDupper and Post-TK yielded relatively modest sensitivities of 47.9% and 62.2%, respectively. A plausible explanation for these findings is that, as demonstrated in previous studies, UIVF is a multifactorial condition influenced by a variety of risk factors. Yagi et al 29 reported that teriparatide administration significantly improved volumetric BMD and trabecular microarchitecture at the UIV+1 level, thereby reducing the incidence of PJF in patients undergoing surgical correction for ASD. Similarly, Duan et al 30 found that in patients undergoing long-segment fusions from the lower thoracic spine to the sacrum for ASD, UIVF was associated with decreased Hounsfield unit (HU) values on CT at the UIV, UIV+1, and UIV+2 levels, indicating that diminished local bone quality at these segments increases fracture susceptibility. Moreover, Lo et al 20 highlighted that older patients may exhibit insufficient muscular reserve to resist flexion loading of the thoracic spine, likely due to generalized age-related sarcopenia or paraspinal muscle degeneration, which may further contribute to the risk of UIVF.
Limitations
This study had several limitations. First, its retrospective nature inherently limits its ability to establish causation. This introduces the potential for selection bias. Second, the absence of PROMs makes it unclear whether radiographic UIVF translates to meaningful clinical impairment. This limits the clinical applicability of our findings. Third, although this study included a comparison of bone marrow density with T-scores, it did not record the Hounsfield Unit (HU) values of UIV on CT, limiting the ability to provide a more objective assessment of bone quality at the UIV. Fourth, although strict inclusion and exclusion criteria were applied to enhance the methodological rigor of the study design, this also resulted in the exclusion of numerous cases with heterogeneous clinical or perioperative conditions. Consequently, the external validity and generalizability of our findings may be limited.
Conclusions
Post- TK > 36.5° and Post-TEDupper < 6.5 mm are significant predictors of UIVF. Based on the study findings, a postoperative TED of ≥ 6.5 mm may be associated with a reduced risk, and could be considered as a potential target in surgical planning, while acknowledging the limitations of the retrospective design and the model’s moderate predictive accuracy. Otherwise, the screw may penetrate the upper endplate of the vertebral body and the risk of UIVF is greater.
Footnotes
Acknowledgements
The authors wish to acknowledge the help of Professor Hsien-Te Chen and Yen-Jen Chen’s supervision.
Consent to Participate
Consent was obtained from all study participants and approval obtained from the Institutional Review Board at China Medical University Hospital (CMUH111-REC1-128).
Author Contributions
B.-H. W., Y.-S. L. designed and performed experiments, Y.-S. L. developed the algorithm. M.-M. Z. assisted in data analysis and figures, B.-H. W., Y.-S. L., M.-M. Z. prepared the manuscript. All authors have contributed to the manuscript and approved the submitted version. We declare that AI-assisted technologies were not used to generate scientific or interpreted data. AI technologies were only used to perform grammar checks on completed manuscripts to improve linguistic accuracy under the supervision of all authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available upon request from Professor Yuan-Shun Lo.