
Abstract
Study Design
Retrospective cohort study.
Objective
To evaluate whether spinal cord-canal mismatch (SCCM) affects clinical outcomes following cervical disc replacement (CDR) in patients with cervical myelopathy, using patient-reported outcome measures (PROMs), global rating of change (GRC), and minimal clinically important differences (MCIDs).
Methods
A retrospective review of a prospectively maintained database identified patients who underwent 1- or 2-level CDR at a single institution from 2016 to 2024. SCCM is measured by the spinal cord occupation ratio (SCOR). Patients were categorized into SCCM (SCOR ≥ 0.7) and no-SCCM (SCOR < 0.7) groups. PROMs, including the Neck Disability Index (NDI), Visual Analog Scale for Neck (VAS-Neck), Arm Pain (VAS-Arm), and GRC, were assessed preoperatively and postoperatively. MCID achievement was analyzed at early (6-12 weeks) and late (6 months–2 years) follow-ups. Statistical tests and logistic regression identified predictors of MCID failure.
Results
Ninety-eight patients (55 SCCM, 43 no-SCCM) were included. Both groups demonstrated significant postoperative improvements in PROMs. Early postoperative MCID rates for NDI, VAS-Neck, and VAS-Arm were 61.4%, 61.4%, and 56.8%, respectively, with no significant differences between groups. Similarly, late postoperative MCID rates and GRC outcomes showed no significant differences. SCCM was not a significant predictor of MCID failure, though male sex was associated with higher odds of MCID failure in NDI (P = .032).
Conclusion
Our findings suggest that SCCM may not adversely affect short-to mid-term clinical outcomes after CDR, although further validation is needed.
Keywords
Introduction
Cervical spondylotic myelopathy (CSM) is a progressive degenerative condition caused by spinal cord compression, leading to significant neurological dysfunction if untreated. Timely diagnosis and intervention are crucial to mitigating the risk of irreversible damage. 1 While anterior cervical discectomy and fusion (ACDF) has traditionally been the gold-standard surgical treatment, its association with adjacent segment disease, which affects approximately 3% of patients annually, 2 has prompted the exploration of alternative approaches. Cervical disc replacement (CDR) has emerged as a promising option, offering motion preservation and lower risks of adjacent segment degeneration compared to ACDF.3,4 Recent meta-analyses of randomized clinical trials indicate that CDR not only yields superior long-term outcomes but also reduces the likelihood of reoperations and adjacent segment syndrome. 5
Spinal cord-canal mismatch (SCCM), characterized by an elevated spinal cord occupation ratio (SCOR), is recognized as a predisposing factor for cervical myelopathy and spinal cord injury. 6 Although previous research indicates that SCCM does not adversely affect neurological outcomes following ACDF, 7 its impact on the success of CDR remains unclear. Research on CDR has traditionally focused on surgical techniques, implant design, and patient factors such as age and comorbidities,8-11 with limited attention to spinal cord morphology.
Given that a high SCOR could theoretically exacerbate spinal cord compression, clarifying its influence on recovery after CDR is essential to optimize patient selection and refine surgical decision-making. This study addresses this knowledge gap by investigating the impact of SCCM on functional outcomes following CDR for cervical myelopathy.
By evaluating patient-reported outcome measures (PROMs) and the achievement of minimal clinically important differences (MCIDs), we aim to determine whether SCCM compromises clinical success. The findings of this study may provide valuable insights into anatomical factors influencing CDR outcomes, ultimately guiding personalized surgical strategies and improving care for patients with cervical myelopathy.
Methods
Patient Population
This was an Institutional Review Board-approved retrospective review of a prospectively maintained database of spine surgeries to identify all consecutive patients who underwent primary, 1- or 2-level CDRs for cervical myelopathy by four attending orthopedic spine surgeons at a single academic institution from February 2016 to Augst 2024. The surgical procedures for CDR have been reported in the previous literature. 12 All patients had cervical myelopathy with central canal stenosis at least at one surgical level. Patients with isolated radiculopathy without stenosis were not included. Patients with a minimum follow-up of 6 weeks were included in the study. Patients without preoperative cervical MRI were excluded. Patients who had operation due to infection, tumor, et al. were exclude. Additionally, patients who were missing preoperative patient-reported outcome measures (PROMs) or failed to complete any postoperative PROM by 2 years in any of the 3 PROMs evaluated (NDI, VAS-Neck, VAS-Arm) were excluded from the study.
Demographic and pre- and post-operative data were collected and managed using REDCap (Research Electronic Data Capture),13,14 hosted by the Weill Cornell Medicine Clinical and Translational Science Center. This initiative was supported by the National Center for Advancing Translational Science of the National Institutes of Health under award number UL1 TR002384.
Spinal Cord Occupying Ratio (SCOR) Assessment
The SCOR was calculated by dividing the average spinal cord diameter (C3 and C7 levels) by the average spinal canal diameter (C3 and C7 levels) on midsagittal T2 MRI (Figure 1). Patients with spinal cord occupation ratio (SCOR) of ≥ 0.7 were classified into the S CCM group, while those with a SCOR of < 0.7 were included in the no-SCCM group. Cutoff value of 0.7 was chosen based on previous studies.6,7,15,16 Radiographic Assessment of the SCOR. The SCOR was Calculated by Dividing the Average Spinal Cord Diameter by the Average Spinal Canal Diameter on Sagittal T2 MRI ([a + c]/2)/([b + d]/2). SCOR Indicates Spinal Cord Occupying Ratio. Reference Sites Above and Below were Measured at C3 and C7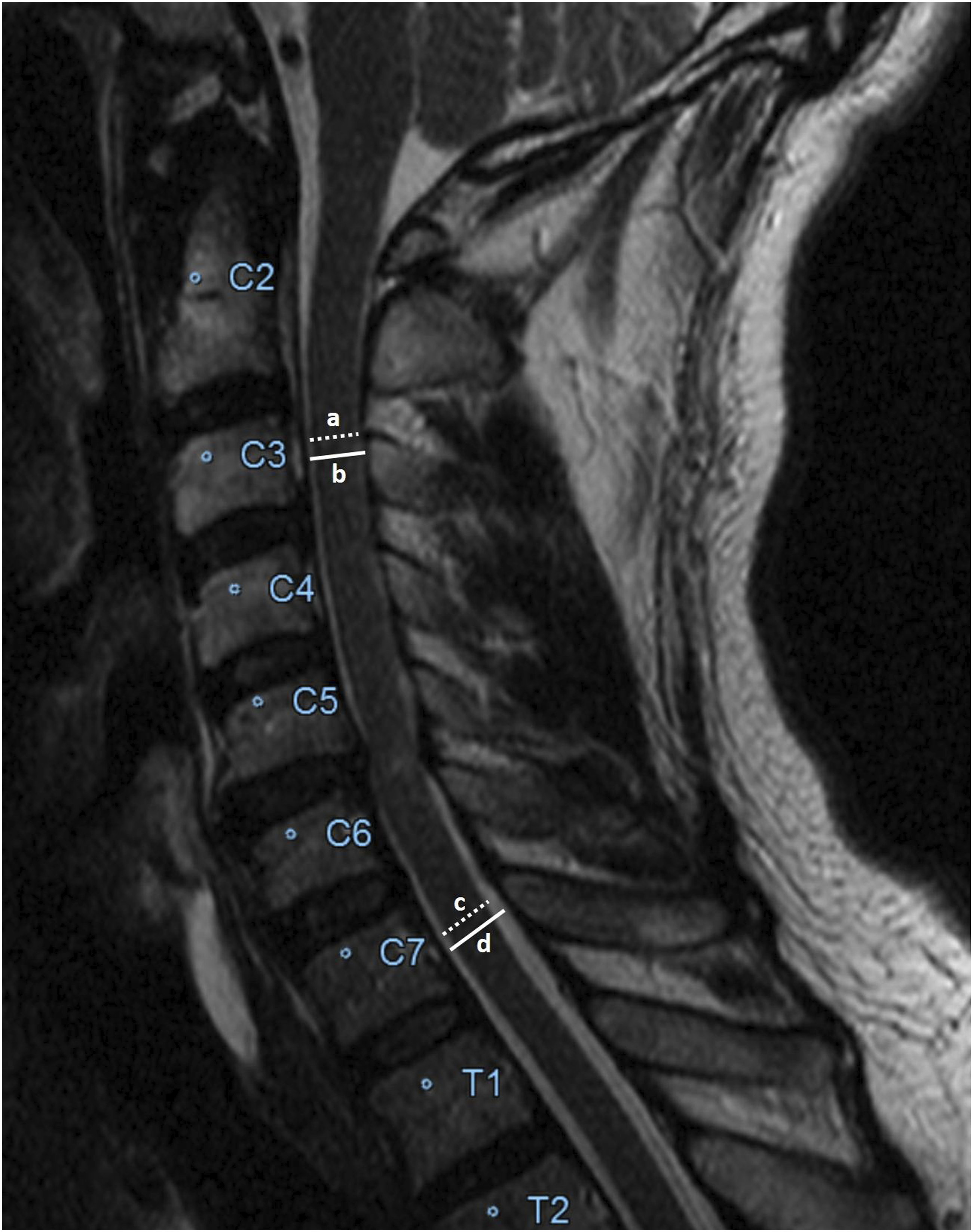
Clinical Outcome Measures
Patient-reported outcome measures (PROMs) evaluated in this study include NDI, VAS-Neck, and VAS-Arm. Questionaries were completed preoperatively and at 6-week, 12-week, 6-month, 1-year, and 2-year timepoints postoperatively. NDI is scored as a percentage (max 100%) with higher scores associated with greater disability, while VAS-Neck and VAS-Arm measure pain on a scale of 0 (no pain) to 10 (maximum pain).
Early postoperative period includes the 2-week, 6-week and 12-week postoperative timepoint, and late postoperative period includes the 6-month, 1-year, and 2-year postoperative timepoints. Self-reported changes in health status were evaluated by global rating of change (GRC).
The minimal clinically important difference (MCID) is defined as the smallest meaningful difference in a score that the patients perceive as beneficial. 17 MCID achievement was assessed by assessing the difference between postoperative PROM values and their respective baseline (preoperative) values. MCID thresholds for NDI, VAS-Neck, and VAS-Arm were set at 15.0, 2.5, and 2.5, respectively, based on previously established values.12,18-22 For each PROM, achievement of MCID was assessed in an early and late postoperative period. Early postoperative period includes the 6-week and 12-week postoperative timepoint, and late postoperative period includes the 6-month, 1-year, and 2-year postoperative timepoints. Most recent available PROM scores for the early and late postoperative periods were used for the MCID calculation and achievement determination.
Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics version 27.0. Frequencies and proportions were reported for categorical variables. Descriptive statistics (mean and SD) were reported for continuous variables. Categorical variables and outcomes were compared between groups using chi-square test or listwise chi-square test when applicable. Variance for continuous variables was assessed using Shapiro–Wilk tests, and comparison between continuous variables were compared using independent samples t tests. Univariable logistic regressions were performed to identify predictors for failure to achieve MCID for PROMs at the latest follow-up time point. P values of <.05 were interpreted as statistically significant.
Results
Demographics
Patient Demographics
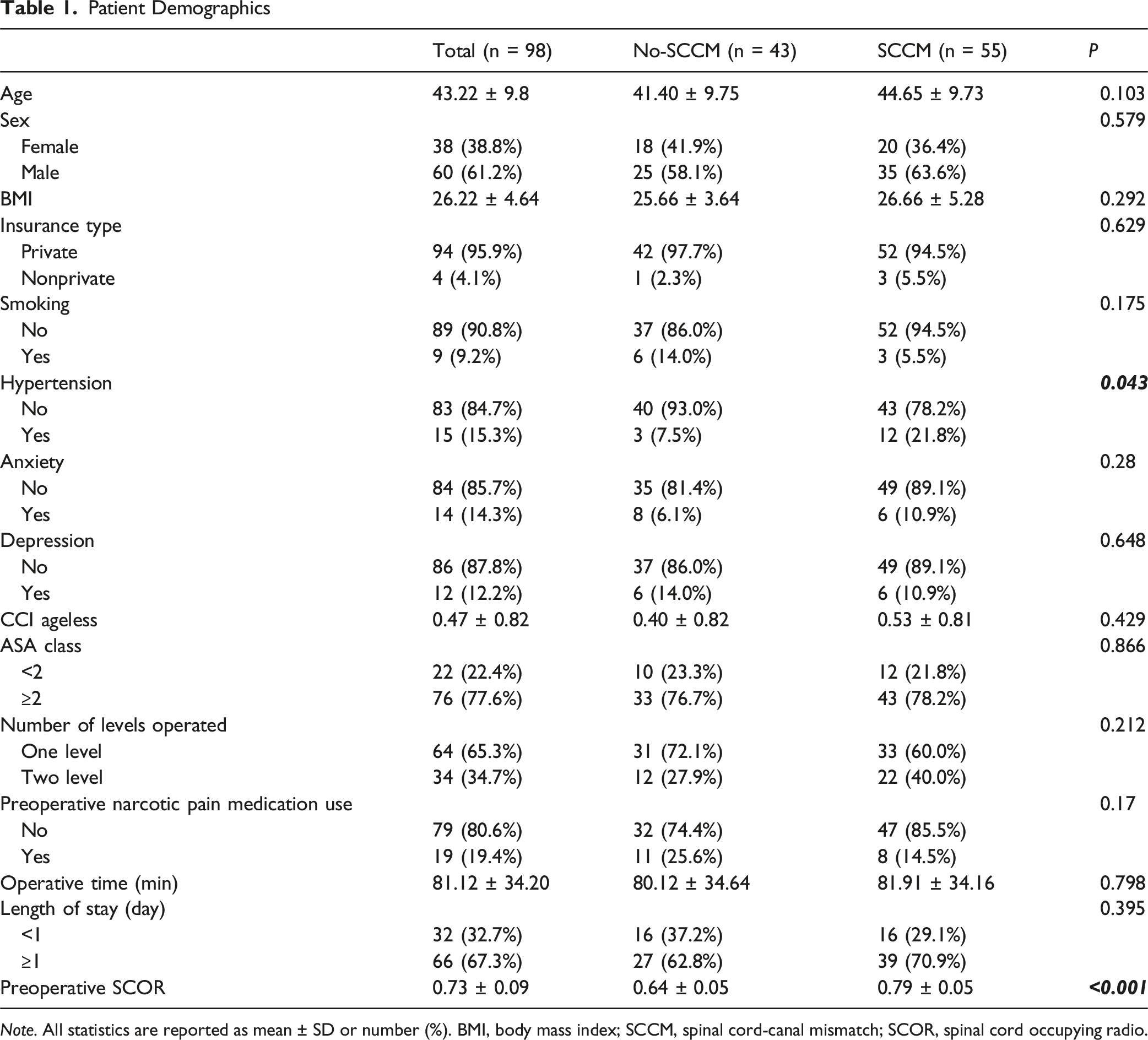
Note. All statistics are reported as mean ± SD or number (%). BMI, body mass index; SCCM, spinal cord-canal mismatch; SCOR, spinal cord occupying radio.
PROMs
PROM Scores and its Change
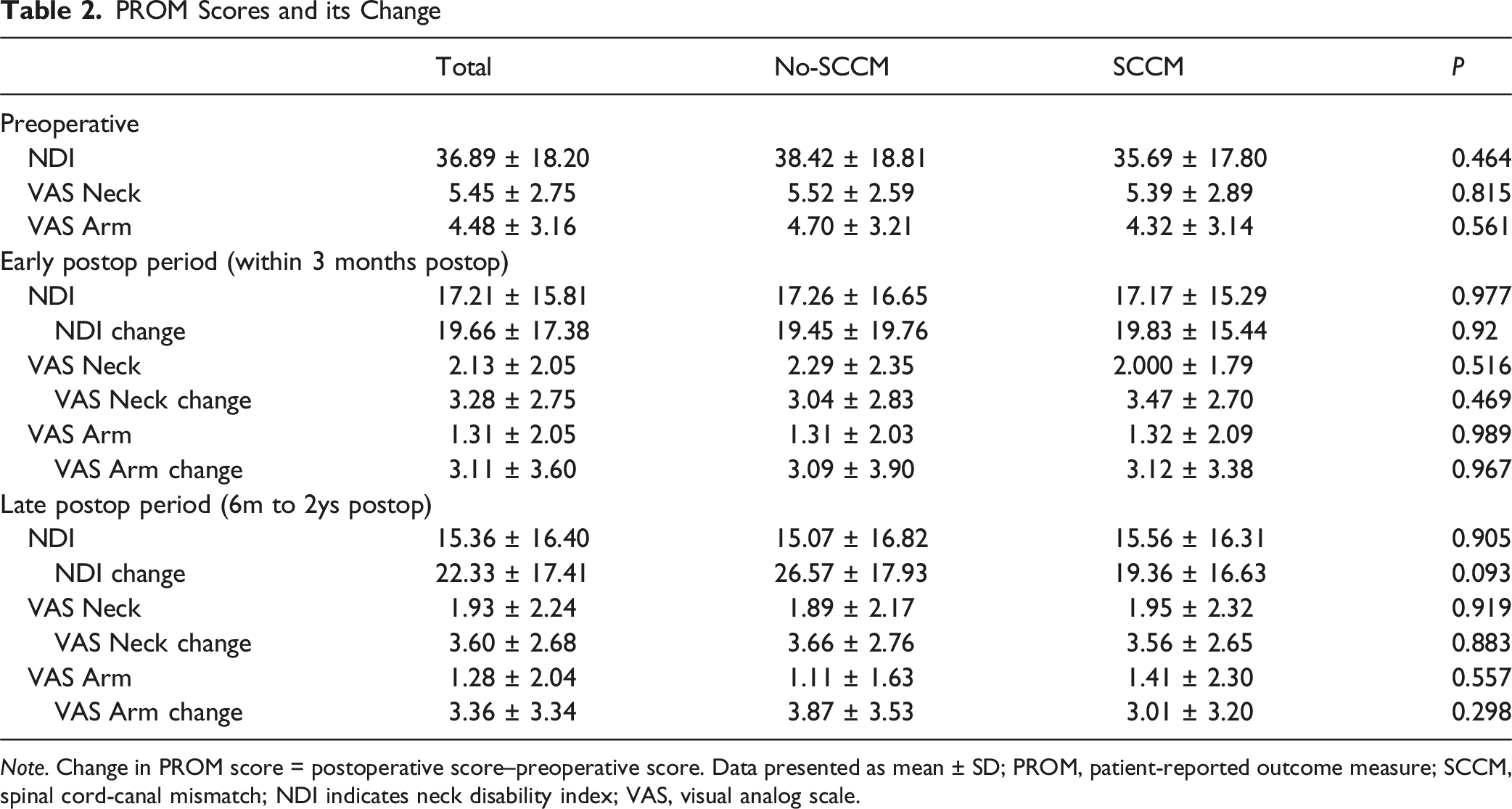
Note. Change in PROM score = postoperative score–preoperative score. Data presented as mean ± SD; PROM, patient-reported outcome measure; SCCM, spinal cord-canal mismatch; NDI indicates neck disability index; VAS, visual analog scale.
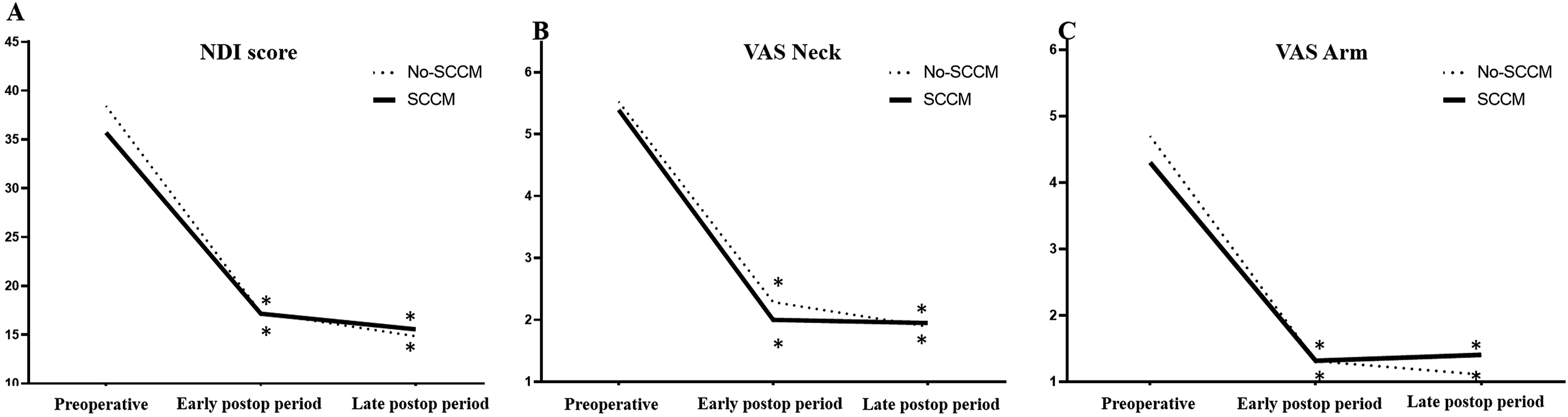
Patient-Reported Outcome Measures. NDI, Neck Disability Index; SCCM, Spinal Cord-Canal Mismatch; VAS, Visual Analog Scale. * Significant Improvement Compared with Preoperative Assessment
GRC
Patients’ Subjective Perceptions of Clinical Change
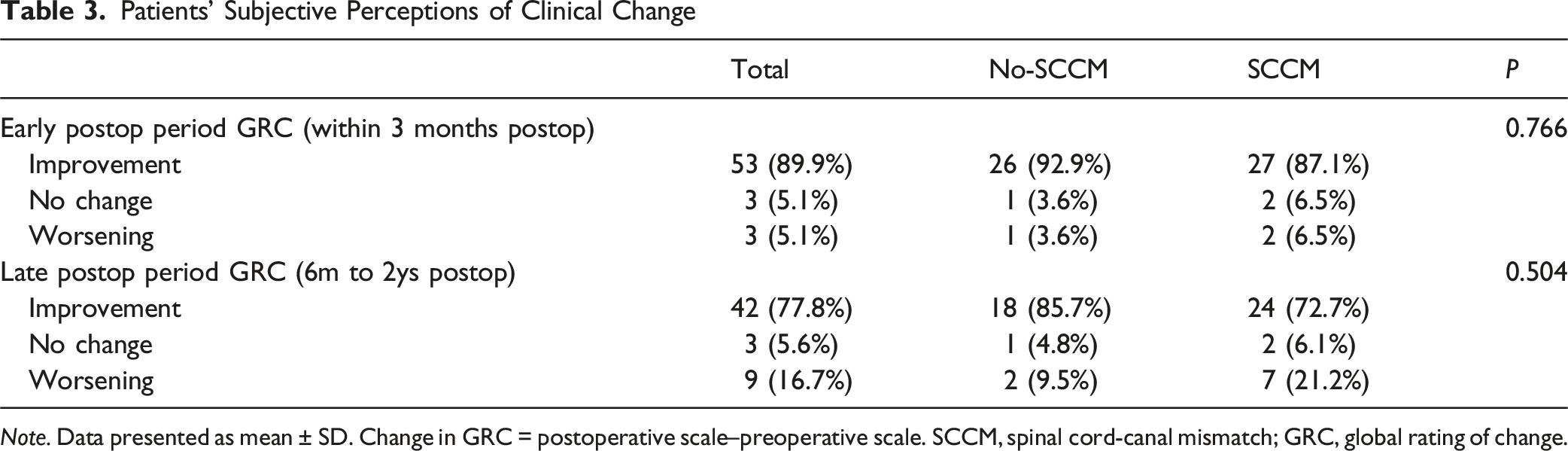
Note. Data presented as mean ± SD. Change in GRC = postoperative scale–preoperative scale. SCCM, spinal cord-canal mismatch; GRC, global rating of change.
MCID Achievement
MCID Achievement Rates After CDR
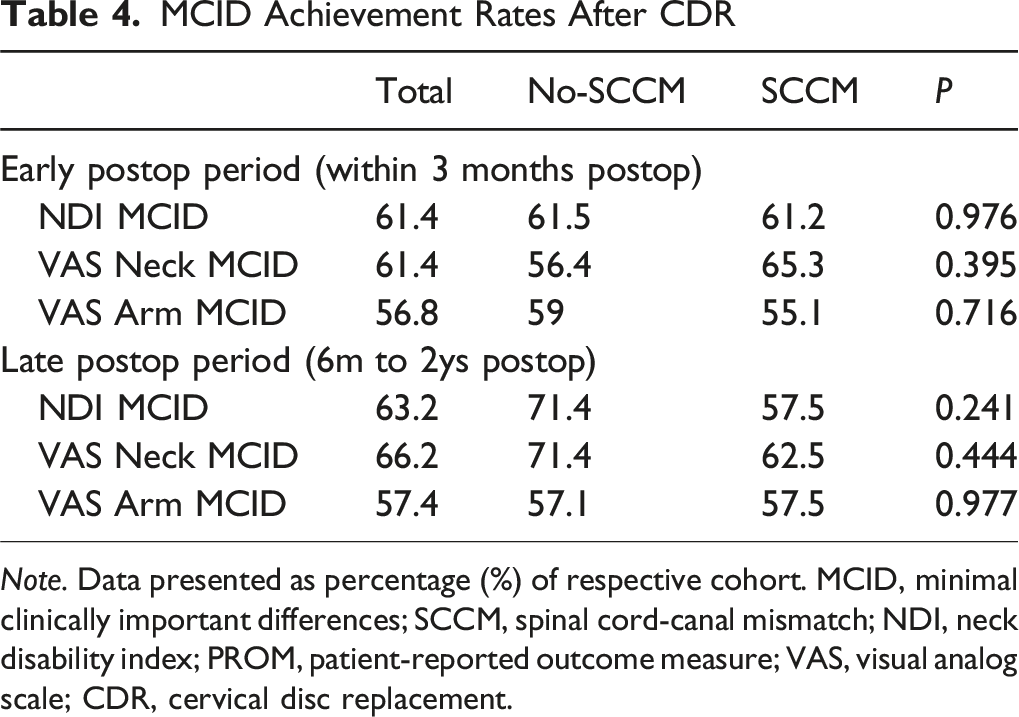
Note. Data presented as percentage (%) of respective cohort. MCID, minimal clinically important differences; SCCM, spinal cord-canal mismatch; NDI, neck disability index; PROM, patient-reported outcome measure; VAS, visual analog scale; CDR, cervical disc replacement.
Predictors of MCID Failure
Predictors for Failure to Achieve MCID for PROMs at Latest Timepoint Period
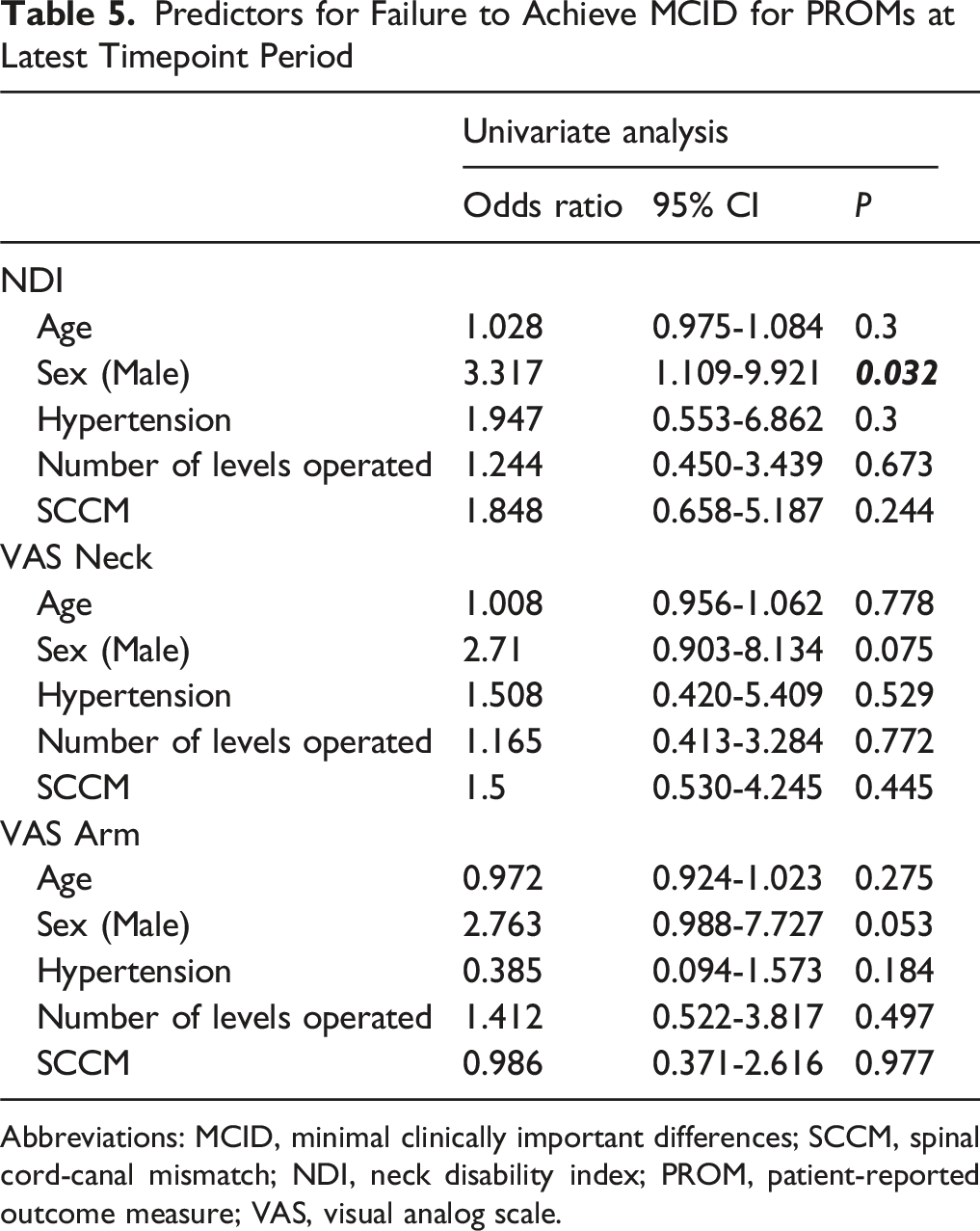
Abbreviations: MCID, minimal clinically important differences; SCCM, spinal cord-canal mismatch; NDI, neck disability index; PROM, patient-reported outcome measure; VAS, visual analog scale.
Discussions
In our study, SCCM was present in 56% of patients who underwent CDR for cervical myelopathy, a proportion higher than that reported in ACDF cohorts (21.0% SCCM). 7 This discrepancy may be attributable to our institutional selection patterns and study design. Despite the relatively high prevalence of SCCM, our findings demonstrate that CDR is effective in managing cervical myelopathy irrespective of SCCM status. Both SCCM and no-SCCM groups demonstrated significant improvements in PROMs, including NDI, VAS-Neck, and VAS-Arm, during early and late postoperative periods. These results are further supported by subjective health status improvements assessed through GRC. Additionally, the similar rates of MCID achievement between the two groups confirm that SCCM, as measured by SCOR, does not adversely affect clinical outcomes following CDR.
Patients with pre-existing cervical spinal canal stenosis face a heightened risk of poor neurological outcomes following minor spinal cord injuries, highlighting the potential need for earlier preventive decompression surgery. 23 Nouri et al. 6 emphasized that spinal cord-canal mismatch (SCCM), rather than simply a narrow spinal canal, increases the likelihood of spinal cord injury and earlier onset of degenerative cervical myelopathy (DCM). Similarly, Nakashima et al. 24 identified a disproportionately large cervical spinal cord relative to the spinal canal as a key risk factor for cervical spinal cord compression. Furthermore, Nouri et al. 15 proposed SCOR ≥ 70% as a reliable diagnostic criterion for congenital spinal stenosis (CSS), finding that CSS patients tend to develop myelopathy at a younger age and experience more severe impairment compared to other DCM patients. In contrast, our study observed that the no-SCCM group was younger, with impairment levels comparable between SCCM and no-SCCM groups. Although the no-SCCM group was younger, the difference was not statistically significant. This discrepancy may reflect our relatively small sample size, the younger age and less severe myelopathy typically seen in cervical disc replacement (CDR) candidates at our institution, as well as other demographic differences between study populations. Multicenter prospective studies with larger and more heterogeneous populations are warranted to clarify these differences.
Recent evidence also indicates that SCCM, as measured by SCOR, does not negatively impact clinical outcomes in ACDF for cervical myelopathy. 7 This study further corroborates that SCCM does not significantly hinder recovery or functional and pain-related improvements after CDR. Additionally, Cho et al. 25 demonstrated that SCCM is not a significant risk factor for adverse outcomes in adults with Klippel-Feil syndrome when compared to matched controls. Although current evidence suggests that SCCM does not significantly impact clinical outcomes following ACDF or CDR, further studies should explore the potential differences in long-term efficacy between various surgical approaches.
Recent studies have investigated the role of MCID in assessing CDR outcomes.12,26,27 MCID reflects the smallest change in PROM scores that patients perceive as meaningful. 28 The similar MCID achievement rates between the SCCM and no-SCCM groups further indicate that SCCM does not compromise clinical outcomes. Both groups showed comparable early postoperative MCID rates for NDI, VAS-Neck, and VAS-Arm, with this pattern continuing into the late postoperative period. Interestingly, univariate analysis revealed that male sex was a significant predictor of MCID failure for NDI, hinting at the influence of gender-specific factors on postoperative recovery. This may be attributable to gender differences in baseline health, pain perception, or psychosocial factors between men and women. This observation highlights the need for further research to explore and address potential gender-related disparities in surgical outcomes.
This study offers valuable insights but has several limitations. Its retrospective design introduces potential biases, and the relatively small sample size may limit the generalizability of the findings. Although the follow-up period was sufficient for evaluating early and mid-term outcomes, it may not fully capture the long-term effects of SCCM on clinical success. Larger, multicenter cohorts with extended follow-up are needed to validate these results and refine patient selection criteria. Another limitation is the reliance on static MRI measurements, which may not fully reflect the dynamic impact of SCCM on cord compression during motion or loading; advanced imaging modalities such as dynamic MRI or CT could provide additional insights. In addition, only a small proportion of patients in this study had mJOA scores available, precluding consistent incorporation of neurological outcome measures. As PROMs alone may not fully capture neurological recovery, future studies should integrate validated neurological scoring systems alongside patient-reported measures. Finally, further research into the interaction between SCCM, spinal cord morphology, and implant design could help clarify the factors influencing CDR outcomes.
Conclusion
CDR may be an effective option for patients with cervical myelopathy, regardless of SCCM status. Our results suggest that SCCM, as assessed by SCOR, does not significantly impact short-to mid-term outcomes. However, given the study’s limitations, these findings should be interpreted cautiously. Further prospective research is needed to confirm these observations and guide surgical decision-making.
Footnotes
ORCID iDs
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: No direct funding was received for this study. However, this study used REDCap (Research Electronic Data Capture) hosted at Weill Cornell Medicine Clinical and Translational Science Center supported by the National Center For Advancing Translational Science of the National Institute of Health under award number: UL1 TR002384.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Sheeraz Qureshi has the following disclosures: AMOpportunities: Other financial or material support; Annals of Translational Medicine: Editorial or governing board; Association of Bone and Joint Surgeons: Board or committee member; Cervical Spine Research Society: Board or committee member; Contemporary Spine Surgery: Editorial or governing board; Globus Medical: IP royalties; Paid consultant; Paid presenter or speaker; Hospital Special Surgery Journal: Editorial or governing board; HS2, LLC: Stock or stock Options; International Society for the Advancement of Spine Surgery (ISASS) - Program Committee member: Board or committee member; Lifelink.com: Other financial or material support; Lumbar Spine Research Society: Board or committee member; Minimally Invasive Spine Study Group: Board or committee member; North American Spine Society: Board or committee member; Simplify Medical, Inc.: Other financial or material support; Society of Minimally Invasive Spine Surgery (SMISS) - Program Committee member: Board or committee member; Spinal Simplicity: Other financial or material support; SpineGuard, Inc.: Paid consultant; Stryker: IP royalties; Paid consultant; Surgalign: Paid consultant; Tissue Differentiation Intelligence: Stock or stock Options; Viseon, Inc.: Paid consultant; Research support.
Sravisht Iyer has the following disclosures: Globus Medical: Paid presenter or speaker; Stryker: Paid presenter or speaker; Vertebral Columns/International Society for the Advancement of Spine Surgery (ISASS): Editorial or governing board.
All other authors have no conflicts of interest to disclose.