
Abstract
Study Design
Systematic review with meta-analysis.
Objective
This study aimed to assess the diagnostic accuracy of USG for detecting PLC injuries.
Methods
A systematic search was conducted in PubMed, EMBASE, and Web of Science. Studies evaluating USG images compared with MRI or intraoperative findings for PLC injuries were included. Pooled sensitivity, specificity, and area under the ROC curve (AUC) were calculated using a bivariate model. Methodological quality was assessed using QUADAS-C, and publication bias was evaluated via Deeks’ test.
Results
Six studies comprising 140 patients were included. The pooled sensitivity and specificity of USG were 0.86 (95% CI: 0.73-0.93) and 0.95 (95% CI: 0.81-0.99), respectively, with an AUC of 0.91 (95% CI: 0.88-0.93). Moderate heterogeneity was observed in specificity (I2 = 51.89%), and publication bias was detected (Deeks’ test, P < 0.001).
Conclusions
Ultrasonography shows good diagnostic performance for detecting thoracolumbar PLC, particularly involving the supraspinous and interspinous ligaments. However, its role in assessing deeper structures such as the ligamentum flavum and facet joint capsules remains inadequately validated. Therefore, USG should be considered a complementary tool, especially where MRI is unavailable or contraindicated, and further studies are required to broaden its clinical applicability.
Keywords
Introduction
The Posterior Ligamentous Complex (PLC) consists of the supraspinous ligament, interspinous ligament, ligamentum flavum, and facet joint capsules. 1 Magnetic resonance imaging (MRI) is widely regarded as the gold standard for diagnosing PLC injuries due to its high sensitivity and ability to visualize soft tissue structures. 2 However, MRI may not always be available or may delay treatment, can be contraindicated in certain patients (eg, those with pacemakers or severe claustrophobia), and may not be feasible in emergency settings.2,3 Ultrasound has emerged as a promising alternative for diagnosing PLC injuries, particularly when MRI is unavailable or contraindicated.
Ultrasound (US) provides a fast, real-time, and dynamic evaluation of musculoskeletal injuries, allowing clinicians to assess joints, and it is particularly valuable in acute trauma settings, where immediate information about the extent and nature of injuries can guide management decisions and interventions.4,5
Studies demonstrate that US is especially effective in detecting injuries to the supraspinous and interspinous ligaments in patients with thoracolumbar fractures. In surgical cases, ultrasound findings have shown excellent correlation with both MRI and intraoperative observations, supporting its diagnostic reliability for these superficial ligamentous structures. 6 Thus, the present meta-analysis aims to evaluate the pooled sensitivity and specificity of ultrasonography (USG).
Methods
Search Strategy and Data Collection
This systematic review was registered in PROSPERO with the following protocol: CRD420251005409. We performed an extensive literature search across PubMed/MEDLINE, Embase, and Web of Science (Clarivate) databases, covering their inception through March 2025. The search terms included: (“ultrasound” OR “ultrasonography” OR “spinal ultrasound”) AND (“posterior ligamentous complex” OR “posterior ligament”)AND (“spinal trauma” OR “spine injury” OR “thoracolumbar spinal fractures” OR “thoracolumbar spinal injuries” OR “injury” OR “PLC injury” OR “traumatic”). No filters were applied during the search. Two reviewers (LGSA and KLA) independently extracted data based on pre-established criteria. A third reviewer (LF) resolved any disagreements. Data were systematically collected, including study design, patient demographics, and diagnostic metrics such as sensitivity, specificity, accuracy, true positives, true negatives, false positives, and false negatives.
Inclusion and Exclusion Criteria
Studies were assessed for eligibility by two reviewers (RFOSM and AN) using the following inclusion criteria: prospective or retrospective studies evaluating the diagnostic performance of USG for PLC injuries, with MRI and/or intraoperative findings as the reference standard, and reporting at least one of the following outcomes: (1) True Positives, (2) True Negatives, (3) False Positives, or (4) False Negatives.
Studies were excluded if they met any of the following: (1) full text was unavailable, (2) involved preclinical or animal research, (3) were duplicate publications (only the most comprehensive version was retained), (4) included fewer than four patients (eg, case reports or small case series), or (5) were abstracts, conference papers, or reviews lacking original data.
Quality Evaluation
One reviewer (IRM) independently assessed the methodological quality of included studies using the Quality Assessment of Diagnostic Accuracy Studies - Comparative (QUADAS-C) tool. Research with a QUADAS-C score evaluates the accuracy of primary studies comparing two or more index tests.
Statistical Analysis
Statistical analyses were conducted using Stata 14.2 with the midas package. A summary receiver operating characteristic (SROC) curve was generated via bivariate binomial regression to assess ultrasonography’s diagnostic accuracy. Forest plots were created to display pooled estimates of the area under the curve (AUC), sensitivity, and specificity, with 95% confidence intervals (CIs). A binormal mixed-effects model was applied to synthesize diagnostic performance across studies.
Scatter plots illustrate the distribution of positive (LR+) and negative likelihood ratios (LR−). A Fagan nomogram was employed to calculate post-test probabilities of PLC injury across various pre-test probabilities, demonstrating the clinical value of USG.
Publication bias was examined using Deeks’ funnel plot asymmetry test, with a P-value <.05 indicating significance. Study heterogeneity was evaluated with the I2 statistic, where values <25% suggested low heterogeneity and >75% showed high heterogeneity.
Results
The flow diagram in Figure 1 summarizes the study selection process. A total of 2588 records were identified from PubMed (1,265), EMBASE (690), and Web of Science (633). After removing 184 duplicate records, 1339 studies were screened based on title and abstract, resulting in the exclusion of 1332 studies. Of the seven reports assessed for eligibility, one was excluded due to the absence of outcomes. Ultimately, six studies were included in the final review.3,6-10 PRISMA Flow Diagram of Our Search Mechanism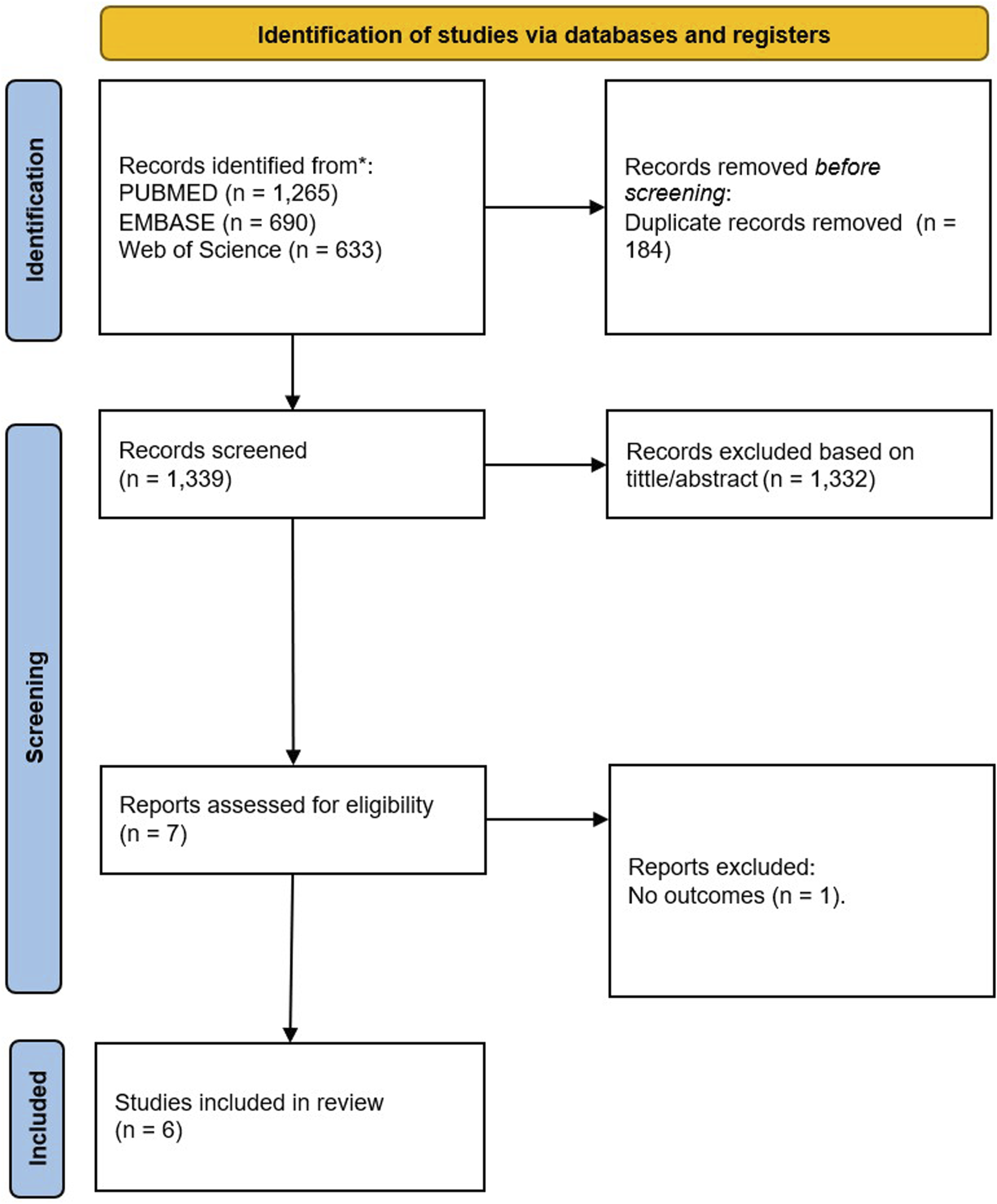
Based on Figure 2, the assessment of methodological quality using the QUADAS-C tool indicates that most studies evaluating USG for PLC injuries presented a low risk of bias across key domains, including patient selection, index test, reference standard, and flow/timing. However, several instances of unclear risk were noted - particularly in patient selection and index test domains - largely due to incomplete reporting regarding blinding procedures and selection criteria. A few studies showed a high risk of bias in patient selection, commonly attributed to retrospective designs or non-consecutive inclusion. Regarding applicability concerns, most studies were aligned with the review question, with only minor issues observed in patient selection and reference standard domains. Quality Assessment of the Six Included Studies Using the QUADAS-C Tool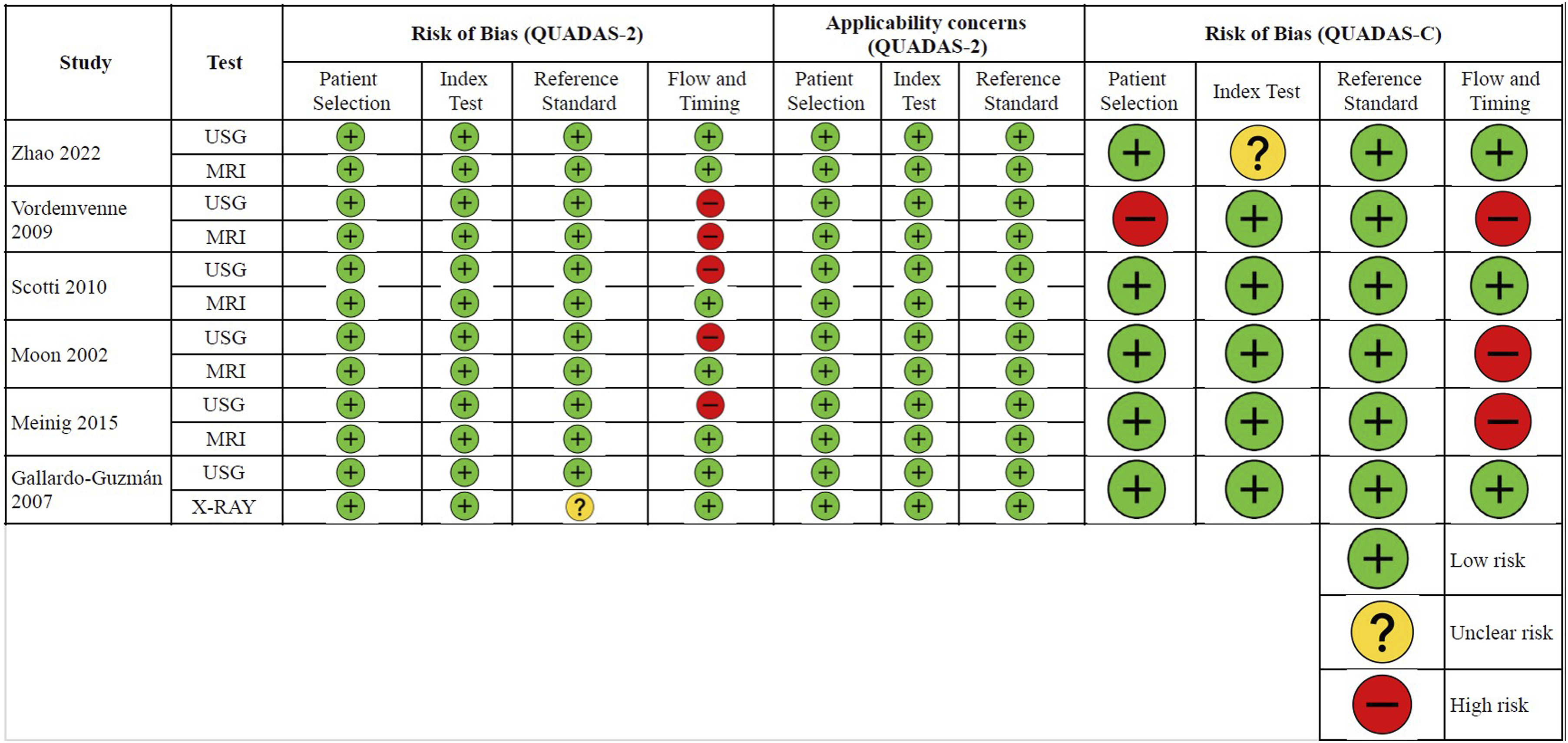
Most domains demonstrated a low risk of bias, reflecting strong methodological quality in key areas such as patient selection, index test execution, reference standard, and flow and timing. However, Zhao et al 7 study exhibited unclear risk, particularly in the index test domain. A high risk of bias was identified in patient selection in Vordemvenne et al 3 study. Flow and timing showed high risk in Vordemvenne et al, 3 Moon et al 6 and Meinig et al 9 studies. In terms of applicability concerns, most studies were well aligned with the review question, with only minimal issues observed, notably in patient selection for Vordemvenne et al. 3
Our review included six studies with a total of 140 patients. The studies were conducted in Taiwan, Germany, Korea, and Mexico, with four prospective and two retrospective designs. The gold standard for diagnosing PLC injuries was MRI in four studies and intraoperative findings in two studies. The mean age across studies ranged from 30.6 to 47.5 years. The assessed ligaments included the supraspinous ligament (SSL), interspinous ligament (ISL), facet joint capsules (FJC), and ligamentum flavum (LF). MRI imaging primarily involved 1.5 T or 3 T scanners, using conventional T1/T2 or T2 sequences. Image evaluations were performed by spine surgeons, trauma surgeons, musculoskeletal radiologists, and independent observers, most commonly using a blinded assessment approach.
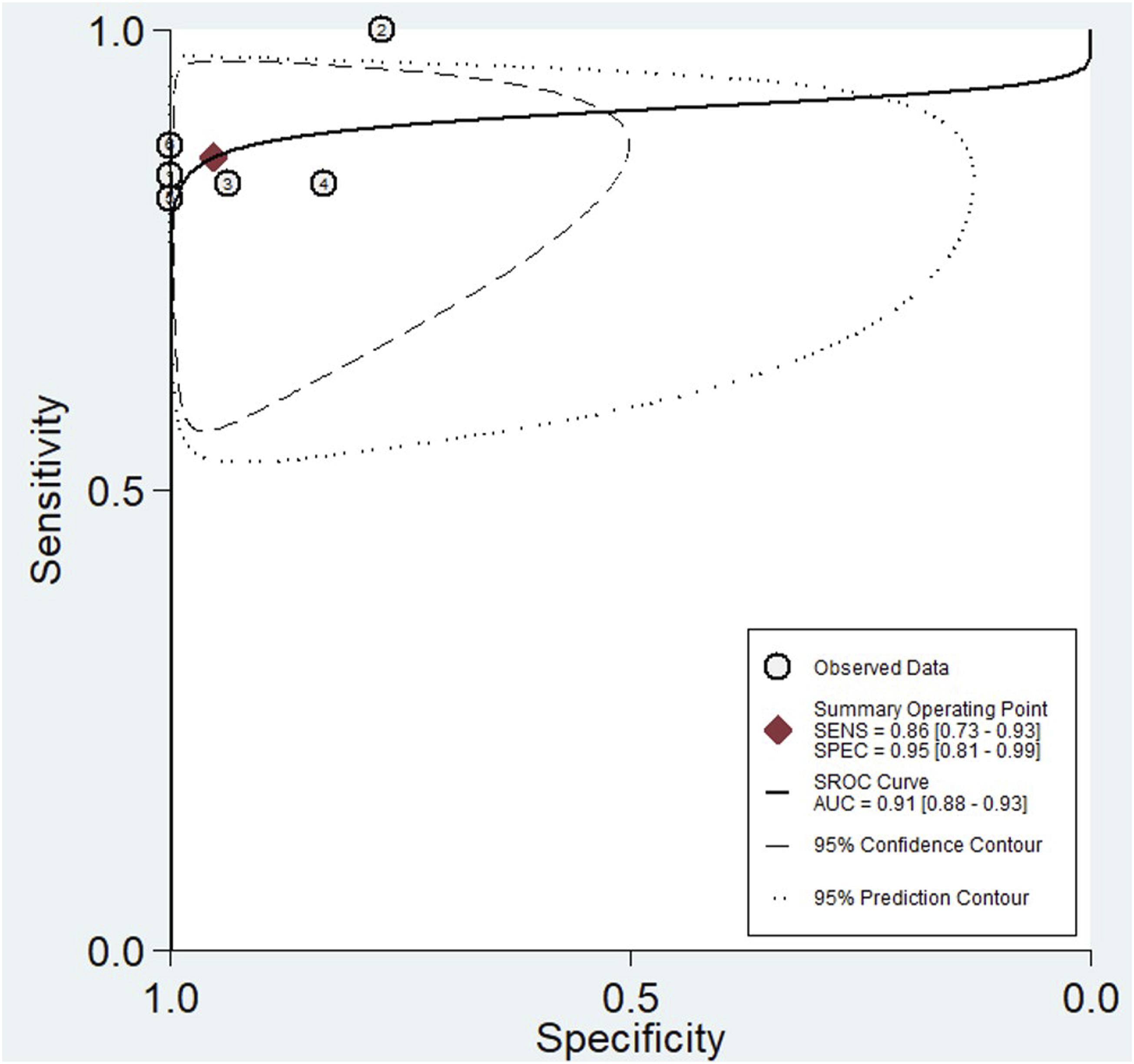
A meta-analysis of USG for detecting PLC injuries in the thoracolumbar spine demonstrated good diagnostic performance. As shown in Figure 3, the pooled sensitivity was 0.86 (95% CI: 0.73 to 0.93; I2 = 0.00), and specificity was 0.95 (95% CI: 0.81 to 0.99; I2 = 51.89), indicating moderate heterogeneity. Based on Figure 4, the AUC from the SROC curve was 0.91 (95% CI: 0.88 to 0.93), reflecting good overall accuracy. These findings suggest that USG may be a reliable imaging modality for identifying PLC injuries, with strong discriminative ability. Plots of Diagnostic Accuracy Measures of Sensitivity and Specificity Summary ROC Plot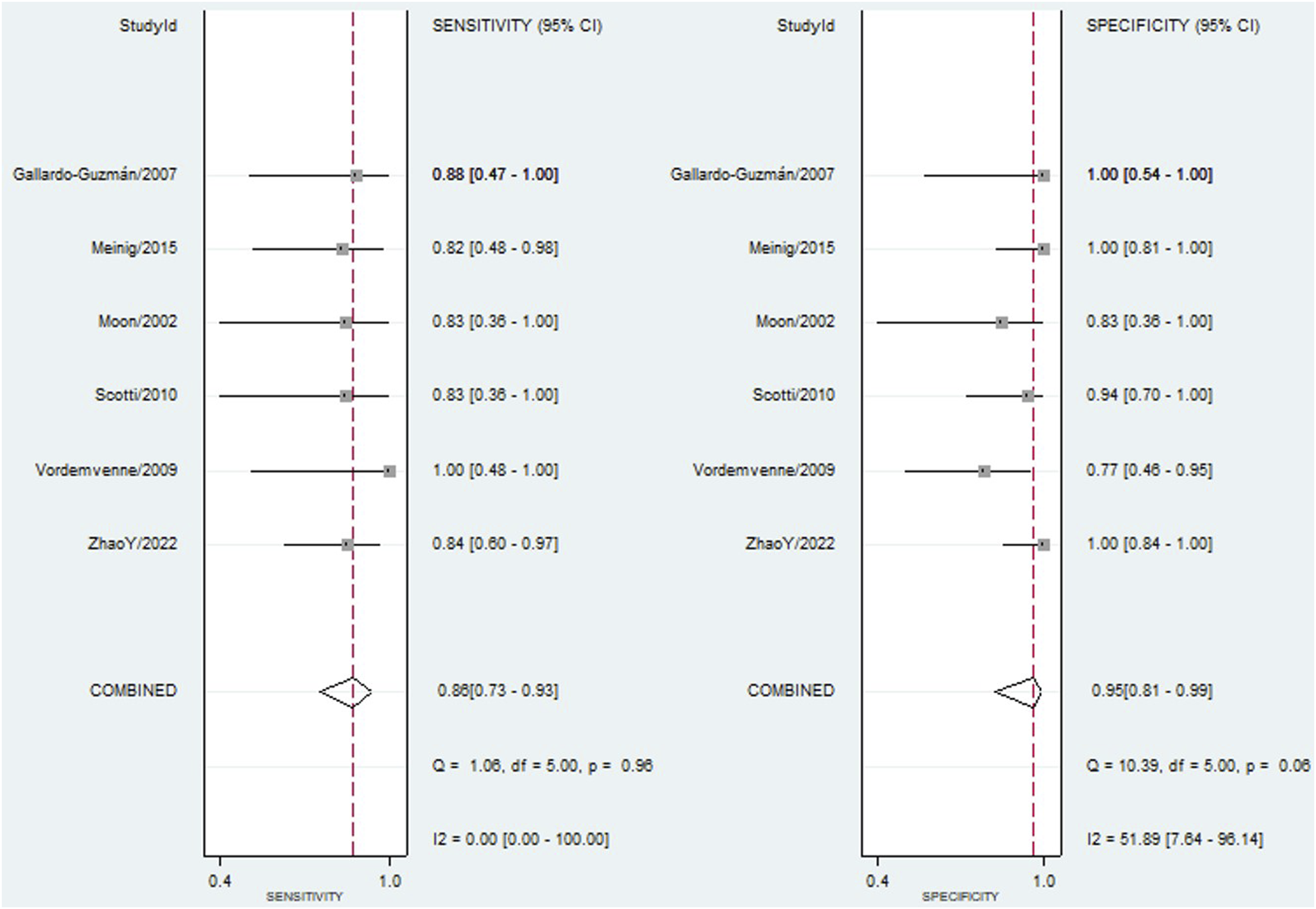
The Fagan nomogram (Figure S1, Supplementary Material) demonstrates the clinical utility of USG in detecting PLC injuries. Given a pre-test probability of 25%, a LR + of 19 increases the post-test probability to 86%, while a LR− of 0.15 reduces the post-test probability to just 5%. Additionally, the posterior probability analysis (Figure S2, Supplementary Material) reinforces the diagnostic performance of USG. Across a prevalence range of 25% to 75%, the test achieved an unconditional negative predictive value (NPV) of 0.86 (95% CI: 0.82 to 0.90) and an unconditional positive predictive value (PPV) of 0.94 (95% CI: 0.90 to 0.98), highlighting its strong predictive capacity in both ruling in and ruling out PLC injuries.
The scatter plot (Figure S3) illustrates the distribution of positive and LR + and LR− for USG in the diagnosis of PLC injuries. The summary point, positioned in the upper-left quadrant (LR + > 10 and LR− < 0.1), indicates that USG demonstrates both high confirmatory and exclusionary power. This suggests that USG is a highly effective diagnostic tool, capable of confidently ruling in and ruling out PLC injuries. The clustering of individual study points around the summary estimate supports the consistency and robustness of USG’s diagnostic accuracy across the included studies.
Quality Assessment and Publication Bias
The univariable meta-regression and subgroup analysis (Figure 5) identified several study-level characteristics associated with variations in the diagnostic performance of USG for detecting PLC injuries. Sensitivity and specificity were not significantly statistically influenced by prospective studies, those using MRI as the reference standard, those involving spine surgeons as readers, studies conducted in Europe, and studies with dual independent readers. Meta-Regression Analysis of US Sensitivity and Specificity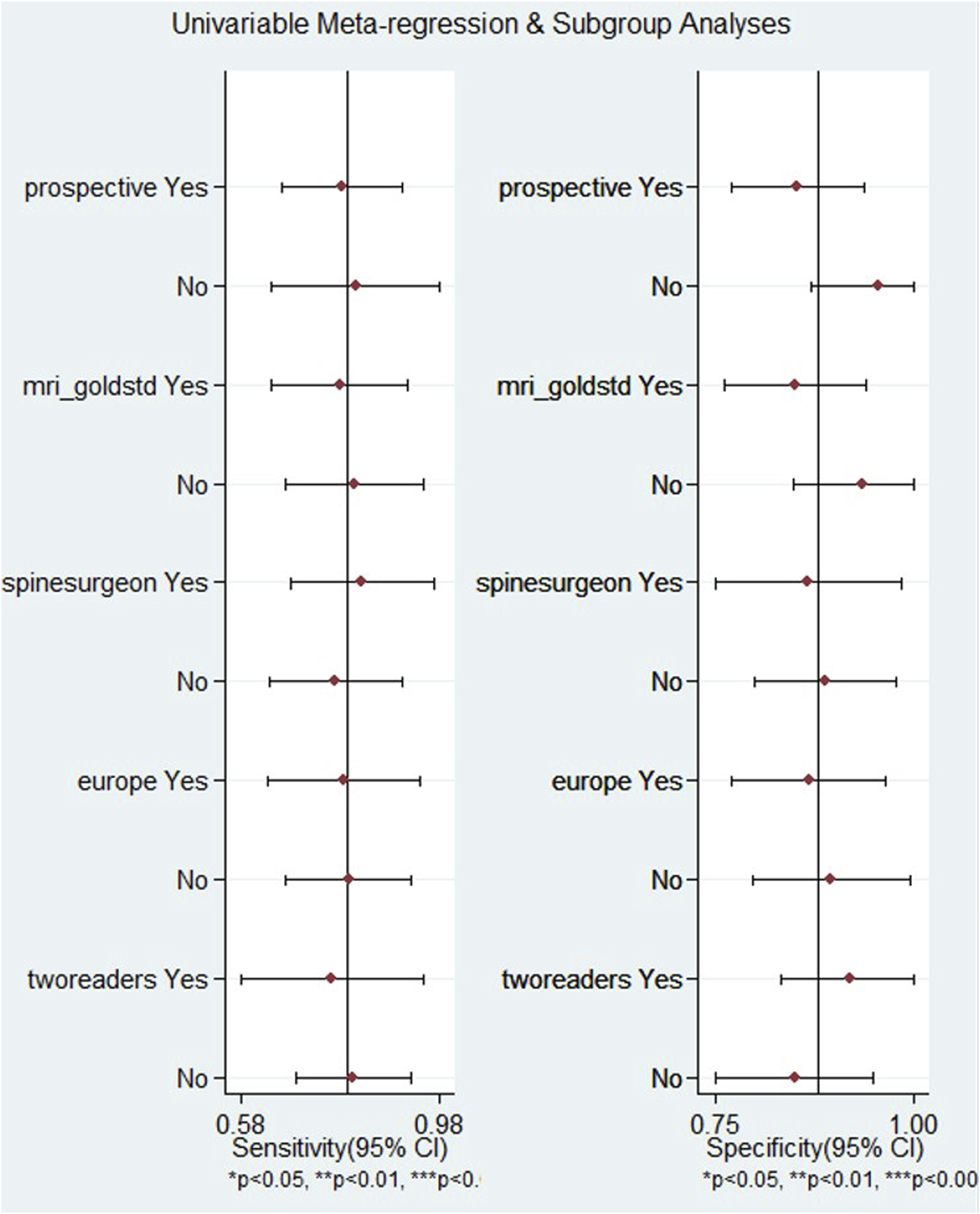
The Deeks’ Funnel Plot analysis (Figure 6) demonstrated a significant deviation from symmetry (P < 0.001), indicating a high likelihood of publication bias. The asymmetric distribution of studies around the regression line suggests that smaller studies with less favorable or non-significant results may be underrepresented, potentially leading to an overestimation of the diagnostic performance of USG in detecting PLC injuries. Deeks’ Funnel Plot Asymmetry Test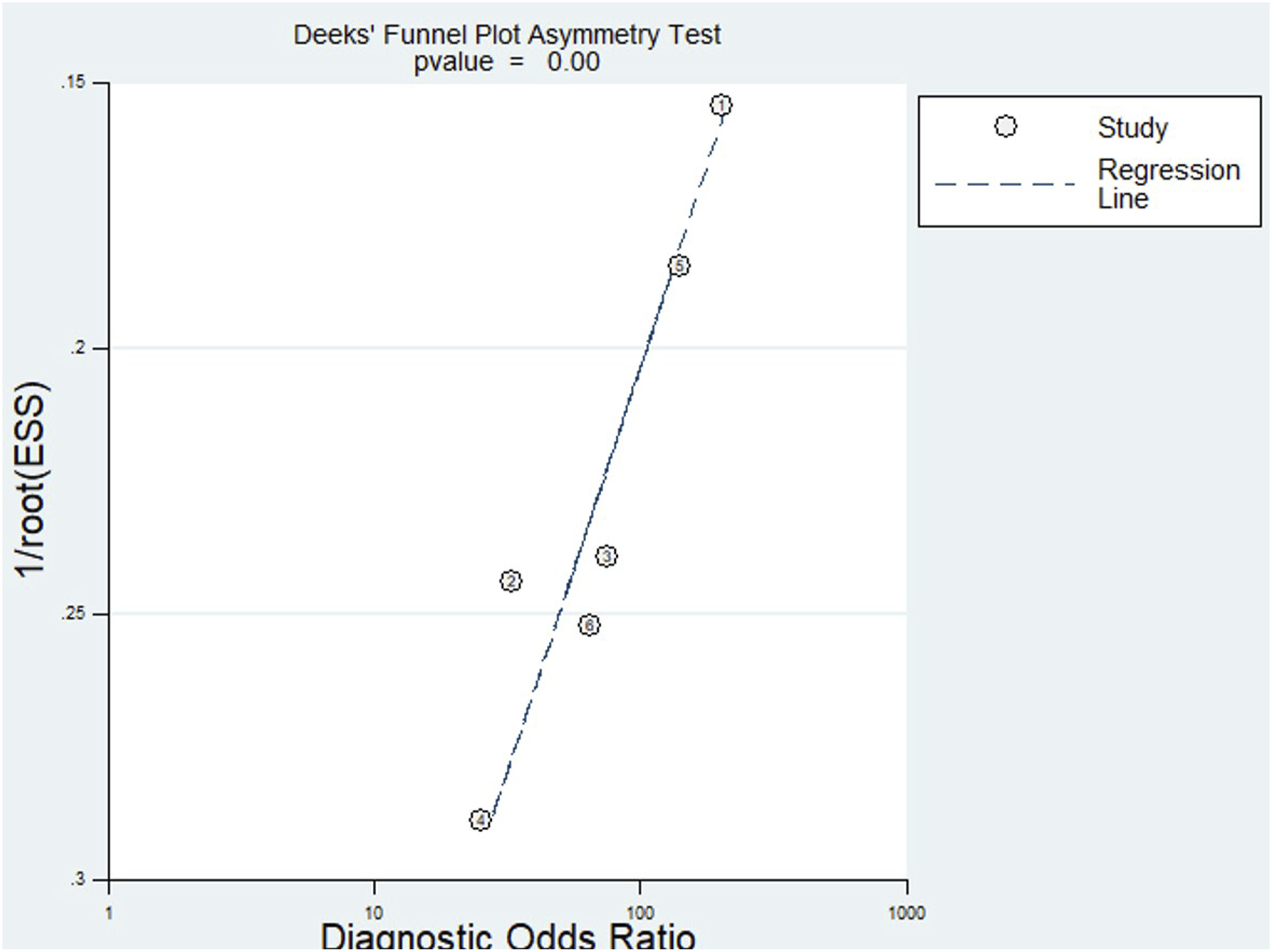
The bivariate boxplot analysis (Figure 7) reveals a strong clustering of studies with moderate logit-transformed sensitivity and specificity, while identifying a few notable outliers with unusually high sensitivity or low specificity. The influence diagnostics (Figure S4, Supplementary Material) support a well-fitting bivariate model for evaluating the diagnostic performance of USG in detecting PLC injuries. The goodness-of-fit and bivariate normality plots confirm that residuals align well with expected distributions. Outlier detection reveals no extreme deviations, and influence analysis identifies a few studies with higher Cook’s distance, suggesting some influence but not undue leverage. Overall, these findings affirm the model’s robustness and the reliability of USG accuracy estimates. Bivariate Boxplot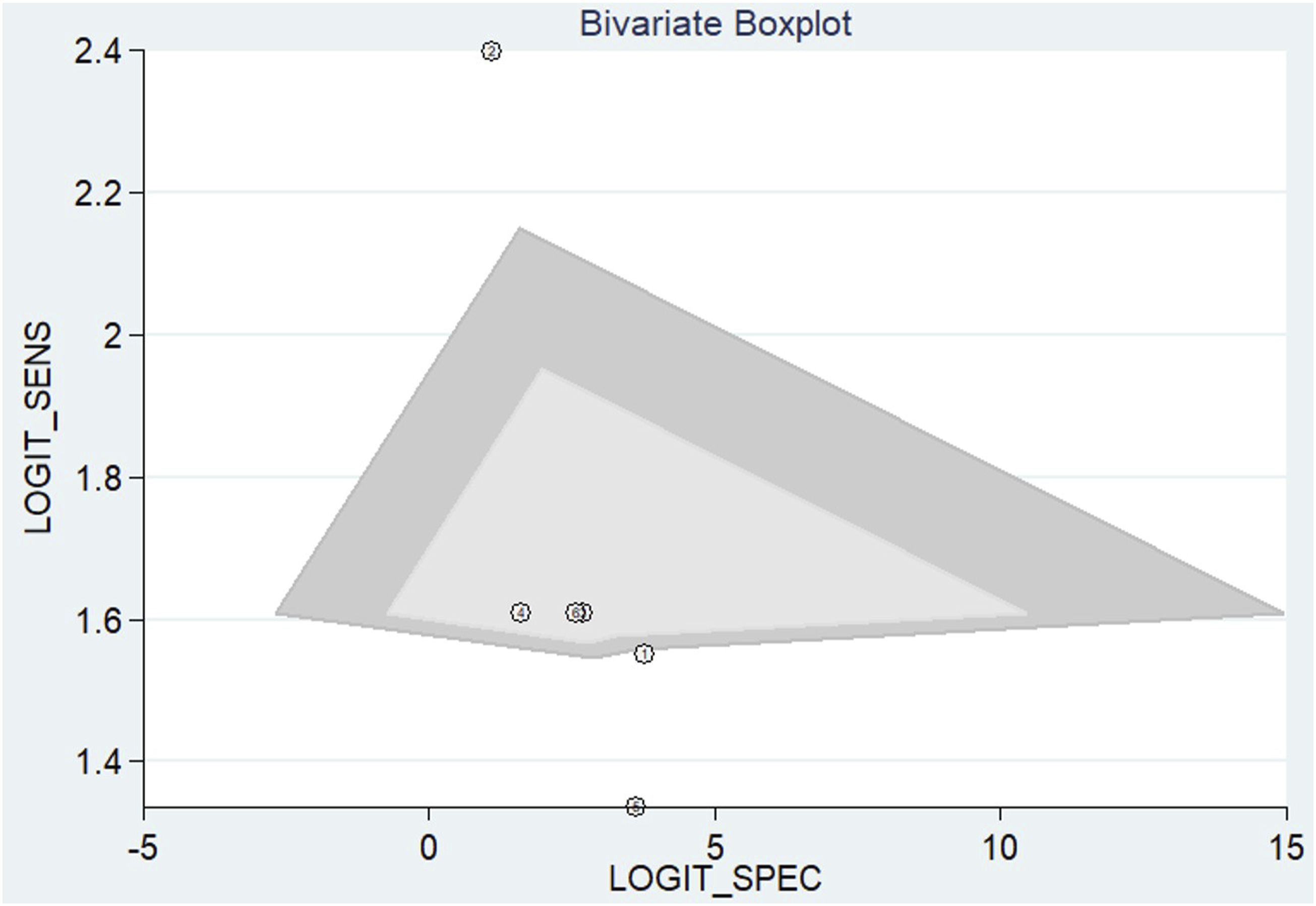
Discussion
In this systematic review and diagnostic accuracy meta-analysis, USG demonstrated consistent performance in detecting traumatic injuries of the PLC of the thoracolumbar spine. The pooled sensitivity was 0.86 (95% CI 0.73 - 0.93), while the pooled specificity reached 0.95 (95% CI 0.81 - 0.99). The AUC was 0.91 (95% CI 0.88 - 0.93), indicating good discriminative capacity. These findings support the use of USG as an adjunct diagnostic tool in the initial evaluation of patients with thoracolumbar trauma, particularly in settings where MRI is not readily available or contraindicated.
This analysis updates and expands upon the evidence previously synthesized by Alcalá-Cerra et al , who included four studies with only 66 patients and reported a sensitivity of 0.89 (95% CI 0.86 - 0.92), specificity of 1.00 (95% CI 0.98 - 1.00), and an AUC of 0.93. 11 Although the diagnostic estimates in both meta-analyses are similar, the current study incorporates a larger number of studies and participants and applies bivariate statistical models that jointly estimate sensitivity and specificity - an approach not used in the earlier analysis.
Beyond diagnostic estimates, the clinical implications of these findings warrant careful consideration. USG offers several advantages over MRI, including portability, lower cost, absence of ionising radiation, and the feasibility of bedside application. These features make USG particularly valuable in emergency departments, field hospitals, and resource-limited settings, where clinical decisions must often be made rapidly and access to MRI may be restricted or unavailable. 3 The dynamic nature of USG allows for real-time assessment, enabling immediate correlation with localized pain or clinical signs. This is particularly relevant in polytrauma patients, where early identification of vertebral instability may directly influence initial management decisions, including the need for rigid immobilization, early surgical stabilization, or referral to specialized centers.12,13
In the context of rehabilitation, USG may serve as a follow-up tool, enabling non-invasive monitoring of ligamentous integrity throughout the recovery process. 8 Future studies could explore its role in tracking the progression of ligament healing or in predicting functional outcomes following trauma. 14 However, for these applications to be fully implemented, barriers related to protocol standardization, professional training, and the validation of USG across diverse clinical practice settings must be addressed. These needs are consistent with the technical recommendations outlined by the American College of Radiology in the ACR - ASNR - SPR Practice Parameter for the Performance of Spine Ultrasound, which emphasizes the importance of structured scanning protocols, highlights the limitations of USG in visualizing deeper structures such as the ligamentum flavum, and reinforces the role of formal operator training in reducing interobserver variability and enhancing diagnostic reliability. 15
Institutions aiming to implement USG for PLC evaluation should ensure practitioners complete competency-based training programs focused on spine ultrasonography, ideally incorporating supervised hands-on practice, standardized interpretation criteria, and inter-rater reliability assessments, as supported by existing musculoskeletal ultrasound guidelines. The establishment of objective criteria for the interpretation of USG findings, as well as the integration of complementary techniques such as elastography and Doppler imaging, may enhance its diagnostic utility and consolidate its role in the evaluation of spinal trauma.16,17
This meta-analysis presents several strengths. First, it represents the most comprehensive update to date on the diagnostic performance of USG in detecting PLC injuries of the thoracolumbar spine. The analysis included a greater number of studies and patients compared to the previous review, allowing for more robust estimates of sensitivity, specificity, and overall diagnostic accuracy. The application of complementary analyses, such as the Fagan nomogram and the assessment of unconditional predictive values across varying prevalence scenarios, added clinical relevance to the findings and strengthened their applicability across diverse healthcare settings.
Some limitations must be acknowledged. Our analysis identified moderate heterogeneity in specificity (I2 = 51.89%). This variation may be attributed to differences in USG acquisition protocols, the level of operator experience, or the definition of the reference standard used across studies.6,8,9 Nevertheless, the clustering of individual data points around the pooled estimate in the likelihood ratio scatter plot supports the overall consistency of the findings. Another methodological strength of this study was the application of posterior probability analysis across varying prevalence scenarios, allowing for a more refined assessment of the clinical utility of USG in diverse epidemiological settings. 18 USG maintained high positive and NPV even in intermediate prevalence ranges (25%–75%), reinforcing its role as a triage tool or complementary modality to MRI. 19
Baseline Characteristics of Included Studies
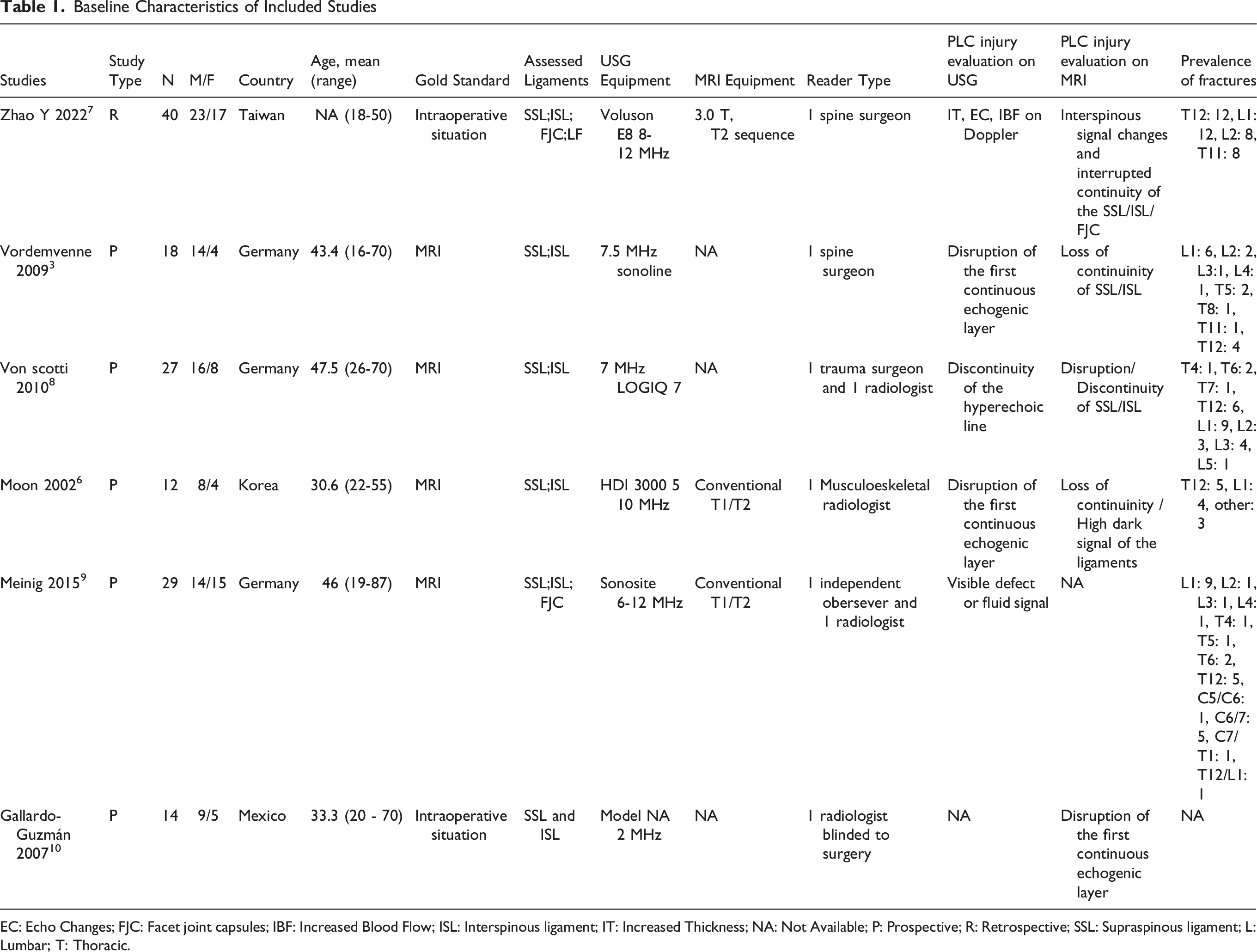
EC: Echo Changes; FJC: Facet joint capsules; IBF: Increased Blood Flow; ISL: Interspinous ligament; IT: Increased Thickness; NA: Not Available; P: Prospective; R: Retrospective; SSL: Supraspinous ligament; L: Lumbar; T: Thoracic.
Taking together, our findings highlight the growing role of USG as a reliable diagnostic tool for detecting PLC injuries in thoracolumbar trauma, particularly when MRI is not accessible. In parallel, computed tomography has also demonstrated acceptable diagnostic performance in this context, as shown in the recent meta-analysis by Falcão et al, with an AUC of 0.81 and specificity of 87%. 21 Considering the widespread availability of both CT and USG, we propose that future research should focus on developing standardized diagnostic protocols that combine these two modalities. Such integration may increase diagnostic accuracy, expedite decision-making in emergency settings, and ultimately reduce the reliance on MRI in the acute evaluation of PLC injuries.
Conclusion
This meta-analysis provides updated evidence supporting the diagnostic utility of USG for detecting traumatic PLC injuries of the thoracolumbar spine, especially for superficial structures such as the supraspinous and interspinous ligaments. With high pooled sensitivity and specificity, USG emerges as a viable adjunct imaging modality. However, the current literature provides limited data on the accuracy of USG for deeper components like the ligamentum flavum and facet joint capsules, which warrants cautious interpretation and restricts generalization. Further standardization of scanning protocols, operator training, and clinical validation across diverse environments are warranted to optimize its implementation. Clinical studies to validate the role of USG in the management of thoracolumbar spinal trauma are necessary.
Supplemental Material
Supplemental Material - Diagnostic Accuracy of Ultrasonography for Detecting Posterior Ligamentous Complex Injuries of Thoracolumbar Trauma: An Updated Systematic Review With Meta-Analysis
Supplemental material for Diagnostic Accuracy of Ultrasonography for Detecting Posterior Ligamentous Complex Injuries of Thoracolumbar Trauma: An Updated Systematic Review With Meta-Analysis by Luciano Falcão, Victor Arthur Ohannesian, Luiz Guilherme Silva Almeida, Karina de Lima Andrade Pereira, Isabelle Rodrigues Menezes, Ricardo Fonseca Oliveira Suruagy Motta, Anderson Matheus Pereira da Silva, André Nishizima, Miguel José Francisco.Neto, Andrei Fernandes Joaquim, Danilo Gomes Quadros in Global Spine Journal
Footnotes
Authors Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.